Embed Size (px)
Citation preview

CS 2015
Mechanical Properties of Lung and Chest Wall
Christian StrickerAssociate Professor for Systems Physiology
ANUMS/JCSMR - ANU
[email protected]://stricker.jcsmr.anu.edu.au/Mechanics.pptx
THE AUSTRALIAN NATIONAL UNIVERSITY

CS 2015

CS 2015
Aims
At the end of this lecture students should be able to
• explain different types of air flow conditions;
• identify determinants of airway resistance (RAW);
• illustrate the concepts of static and dynamic
compliance and how these are measured;
• demonstrate why a small lung volume is harder to
inflate than a larger; and
• point out how surfactants increase compliance.

CS 2015
Contents
• Airway resistance– Air flow conditions
– Locations and determinants of RAW
– Transmural pressure
• System compliance and its elements– Static & dynamic compliances
– Alveolar surface tension
– Laplace’ law and alveolar pressure
– Surfactants and compliance

CS 2015
Determinants of RAW
• Air flow conditions
• Locations and determinants of RAW
• Transmural pressure
• Modulation of RAW

CS 2015
Air Exchange
• Conducting airways: blood supply via bronchial artery.
• Bronchioles: no skeleton; exposed to transmural pressure.
• Respiratory unit = physiological unit, where O2 and CO2
are exchanged; blood supply via pulmonary artery.
Ber
ne e
t al.,
200
4

CS 2015
Consequences for Air Flow
• Flow over vocal cords is biggest and decays later to small
values in alveolar airways.
• Functional consequence: ~ turbulent flow over vocal cords;
but ~ laminar flow in alveolar airways.
Bor
om &
Bou
lpae
p, 2
003

CS 2015
Flow Conditions in Airways• Since airways are bifurcated, turbulence arises at
bifurcation points.
• Flow in airways is transitional (in between laminar
and turbulent).
• Ohm’s law is used to determine RAW (airway and
tissue deformation):
• Contribution to RAW:
Boron & Boulpaep, 2003

CS 2015
Determinants of RAW
• Under laminar flow conditions,
with η viscosity, l length and r radius.
• Normally, viscosity is constant (air); altered
with pressure (altitude, diving) & gas mixtures.
• Elements of RAW (around TV)
– Rvisc ~ 40% (dynamic parameter; flow dependent).
• Laminar and turbulent conditions (80%)
• Tissue resistance (“friction” between elastic fibres; 20%)
• Inertia (very little)
– Relast ~ 60% (static parameter; volume dependent).

CS 2015
RAW and Lung Volume
• Lung volume affects airway diameter, particularly airways
without skeleton: during E, tension release (alveolar size ↓)
and positive pressure on bronchioli → r ↓; during I, vice
versa.
• It is easier to breath in than out (air trapping…).
• COPD: r↓ → RAW↑. To maintain ventilation, flow↑.
Mod
ified
from
Bor
on &
Bou
lpae
p, 2
003

CS 2015
Transmural Pressures
• Affects bronchioles
• During forced I, positive
transmural pressure keeps
small airways open.
• During forced E, when Ppl >
0, transmural pressure can
become ≤ 0; i.e. airways
collapse.
• Can be seen in flow-volume
loop: airway closure.
Modified from Hlastala & Berger 2001
CS 2015
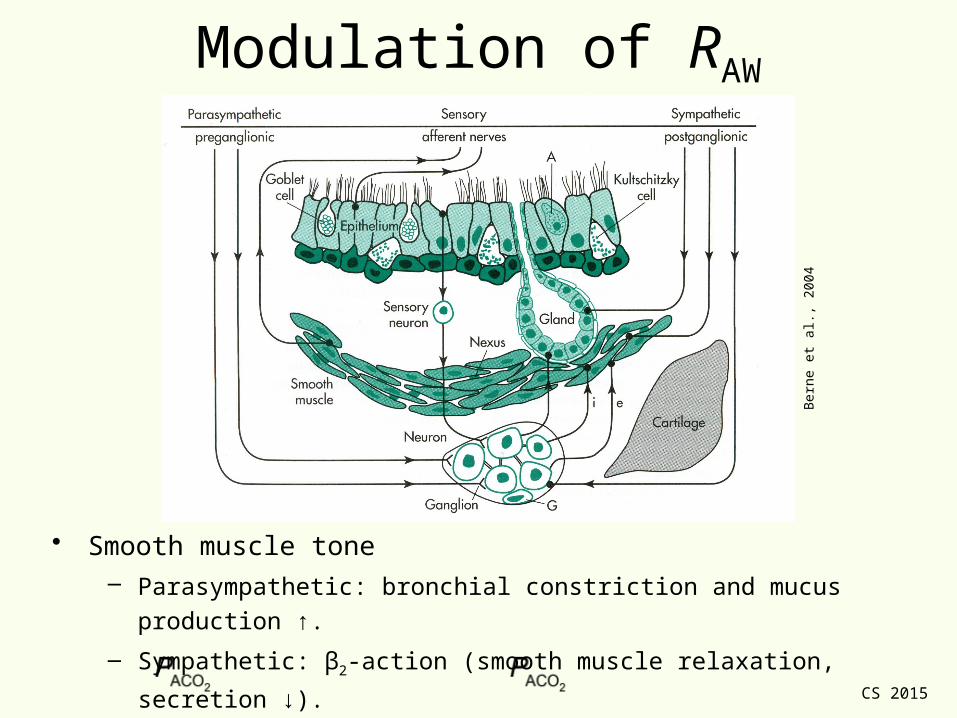
Modulation of RAW
• Smooth muscle tone– Parasympathetic: bronchial constriction and mucus production ↑.
– Sympathetic: β2-action (smooth muscle relaxation, secretion ↓).
• With ↑ → local airway dilation; ↓→ local airway constriction.
Ber
ne e
t al.,
200
4

CS 2015
Compliance of Breathing System
• Static & dynamic compliances
• Alveolar surface tension- Laplace’ law and alveolar pressure
- Surfactants and compliance

CS 2015
Compliance of Breathing System
Static compliance: no flow, volume fixed
Dynamic compliance: both flow, volume change
CT = total compliance (breathing system)
CL = lung compliance
CCW = thorax (chest wall) compliance

CS 2015
How to Measure Compliances• Shown with body
plethysmograph.– Required for Cdyn.
– Not necessary for Cstatic (no
flow…).
• Cstatic with valve and
spirometer only.– Measured during expiration
(see later).
– PA and ΔVL measured
simultaneously after halting
flow (= Poral): at each
volume, PA measured.
Modified from Boron & Boulpaep, 2003

CS 2015
Static Lung Compliance (No Flow)
• Total system compliance (CT) can be
measured after breathing out (“relaxation
curve”); linear within range of TV.
• Both lung (CL; fibrosis – too small;
emphysema – too large) and chest-wall
compliance (CCW; skoliosis) are needed
clinically.
• CT is related to CCW and CL via
• Requires that Ppl be measured with each
volume change.
• Within TV, CL ~ CCW ~ 2 CT, ~ 0.1 L/cm
H2O.Modified from Hlastala & Berger 2001

CS 2015
Static CL and Pathology
• Static CL important in
pathophysiology.
• Emphysema (“overblown”
lung) has large
compliance at FRC: loss
of recoil (elastance; 1/CL).
• Conversely, fibrosis
reduces CL and FRC: too
much recoil …Modified from Boron & Boulpaep, 2003
CS 2015
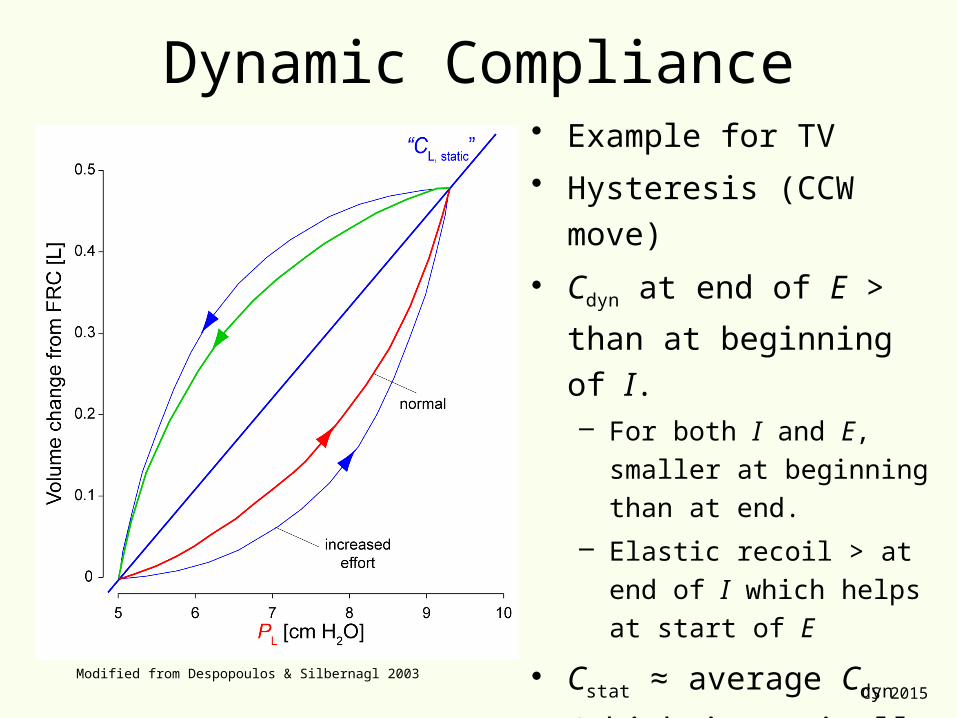
Dynamic Compliance• Example for TV
• Hysteresis (CCW move)
• Cdyn at end of E > than at
beginning of I.– For both I and E, smaller at
beginning than at end.
– Elastic recoil > at end of I
which helps at start of E
• Cstat ≈ average Cdyn (which
is typically a bit smaller).
• Effort sets width of
hysteresis.Modified from Despopoulos & Silbernagl 2003

CS 2015
Compliances in Disease• Emphysema with a high static
compliance and a wide
dynamic hysteresis (work! -
recoil lost).
• Asthma increases
compliance; TV at FRC↑;
large expiratory work
(increased RAW).
• RDS has low static and
dynamic compliance and TV
at high pressures.Modified from Koller, 1979

CS 2015
Alveolar Surface Tension
Laplace’ law
Surfactants

CS 2015
Surface Tension and Compliance
• CL↑ when lung filled with
saline - but finite.
• Surface tension is largest
factor determining CL:
– Laplace’ law.
• How to minimise surface
tension?– Detergents (soap)
– Surfactants …
Modified from Boron & Boulpaep, 2003

CS 2015
What Every Child Knows…
• What is the hardest part to
blowing up a balloon?– Initial volume change…
– Becomes easier as you inflate…
– Ultimately so easy, it can be
blown apart…
CS 2015
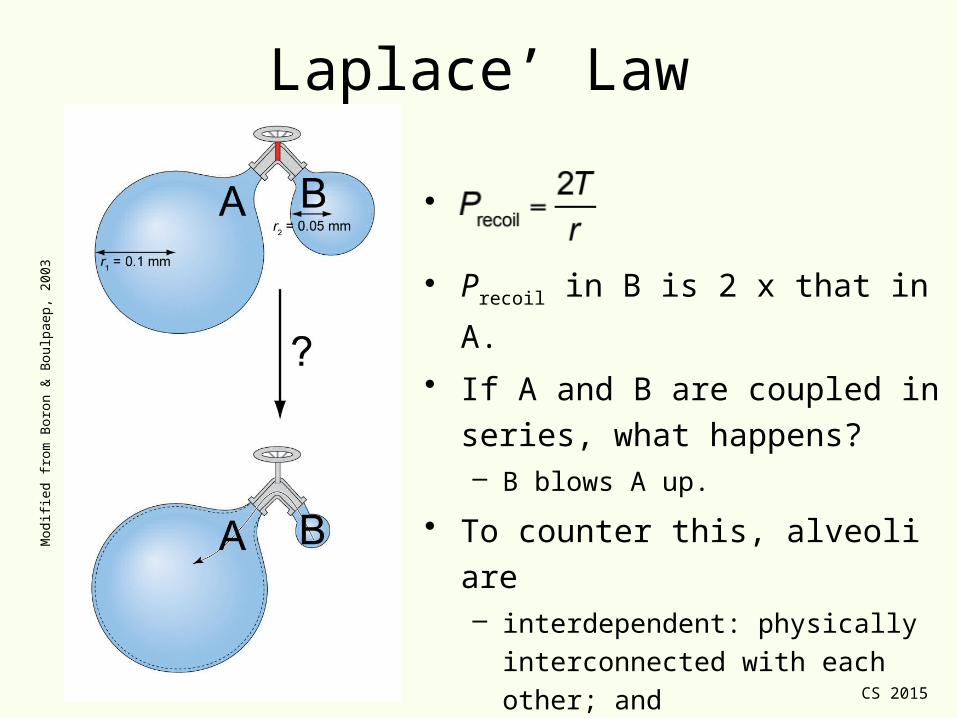
Laplace’ Law
•
• Precoil in B is 2 x that in A.
• If A and B are coupled in series,
what happens?– B blows A up.
• To counter this, alveoli are– interdependent: physically
interconnected with each other; and
– lined with surfactant.
Mod
ified
from
Bor
on &
Bou
lpae
p, 2
003

CS 2015
Surfactants and Surface Tension• Surfactant (surface-active agent)
• Reduces surface H2O and hence
surface tension: it is an attractive force
of surface molecules that tends to
minimise surface area.
• Combination of dipalmitoylphosphatidyl-
choline and apoproteins (SP-A/B/C/D).
• Secreted by alveolar type II cells
• Can easily be destroyed with O2.
• Produced shortly before birth; problem
in premature babies (respiratory
distress syndrome).– Steroid priming for 2-3 d can initiate
surfactant expression.
Modified from Boron & Boulpaep, 2003

CS 2015
Surface Expression• Surfactants form micelles.
• Dynamic system:– During I, as alveolar surface
increases and [surfactant]
decreases, surfactant from
micelles is recruited to surface.
– During E, alveolar surface de-
creases, [surfactant] is higher
and micelles re-form.
• Role:– Reduction in surface tension:
keeps alveoli “open”.
– Keeping alveoli dry.Modified from Hlastala & Berger 2001

CS 2015
Ventilation and Surfactants
• Rapidly expanding alv. →
[surfactant]↓ → CA↓ →
ventilation↓.
• Slowly expanding alv. →
[surfactant]↑ → CA↑ →
ventilation↑.
• Homeostatic principle to
open alveoli to ~ similar volume.
Modified from Boron & Boulpaep, 2003

CS 2015
Take-Home Messages• Flow in bronchi is transitional, in alveoli
laminar.
• RAW is volume dependent; is neurally
modulated.
• CL is ~2 x CT; is linear in range of TV.
• A small alveolus requires a larger pressure to increase its volume than a large one;
• Hysteresis in V-P loop is result of surface tension and Laplace’ law; and
• Surfactants reduce surface tension and ease alveolar ventilation.

CS 2015
MCQAnna May, a 43 year-old female, has an extensive lung
function analysis. As she exhales under static conditions from
FRC + 1 L to FRC, her oesophageal pressure changes from -
10 to -5 cm H2O and the alveolar pressure from 5 to 0 cm
H2O. What is the best estimate of her static lung compliance?
A. 0.5 L / cm H2O
B. 5.0 cm H2O / L
C. 0.1 L / cm H2O
D. 2.0 cm H2O / L
E. 0.2 L / cm H2O

CS 2015
That’s it folks…

CS 2015
MCQAnna May, a 43 year-old female, has an extensive lung
function analysis. As she exhales under static conditions from
FRC + 1 L to FRC, her oesophageal pressure changes from -
10 to -5 cm H2O and the alveolar pressure from 5 to 0 cm
H2O. What is the best estimate of her static lung compliance?
A. 0.5 L / cm H2O
B. 5.0 cm H2O / L
C. 0.1 L / cm H2O
D. 2.0 cm H2O / L
E. 0.2 L / cm H2O