Embed Size (px)
Citation preview

Urol Radiol 10:12-16 (1988) Urologic Radiology
© Springer-Ver[ag New York Inc. 1988
CT and MRI of Adrenal Lesions
N. Reed Dunnick Department of Radiology, Duke University, Durham, North Carolina, USA
Abstract. Adrenal lesions can be divided into those that result in clinical syndromes due to excess hor- mone elaboration and those that are nonhyperfunc- tioning. Computed tomography (CT) is usually ad- equate to assess the adrenal glands in patients with hyperfunctional disease. Occasionally supplemen- tation with radionuclide studies, magnetic reso- nance (MR) or venous sampling, is required. Le- sions which are not hyperfunctioning are often detected as an incidental mass. The CT and MR characteristics often allow a confident diagnosis based on their imaging characteristics. The adrenal glands are a common site of metastatic disease which can be detected by CT and further characterized by MR or biopsy if the stage of disease is uncertain.
Key words: Adrenal, CT -- Adrenal, MR -- Ad- renal, tumor -- Adrenal, metastases -- Adrenal, hy- perplasia -- Pheochromocytoma.
Diseases of the adrenal gland may be classified into functional disease, in which the patient manifests signs and symptoms of hormone excess, and non- functional disease, in which no recognizable hor- mone is being overproduced. Excess production of adrenal hormones may be a result of either an au- tonomous adrenal tumor or bilateral adrenal hy- perplasia, in which the adrenal glands are stimulated by unregulated ACTH.
Nonfunctioning Adrenal Lesions
An incidental adrenal mass may be detected as part of a tumor staging evaluation or when a patient is being evaluated for an unrelated problem. These lesions are not hyperfunctional, in that they do not overproduce a recognizable hormone. Their possi- ble causes include a wide variety of developmental, inflammatory, and neoplastic masses.
Adenoma
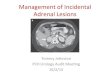
The incidence of nonfunctioning adrenal adenomas in the autopsy population is surprisingly high. Com- mons and Callaway reported a 2.86% incidence of adrenal adenomas greater than 3 mm in diameter among 7,437 autopsies. While these lesions are al- most always an incidental finding, the challenge aris- es in distinguishing them from malignant lesions, such as metastases. Serial computed tomographic (CT) examinations to determine interval growth or percutaneous fine-needle biopsy to detect malignant cells have both been advocated. However, magnetic resonance (MR) may also be used for this purpose. Metastases have a high signal intensity on T2- weighted images while the intensity ofnonfunction- ing adenomas is similar to normal adrenal tissue (Fig. 1). There is overlap, however, in as many as 20-30% of cases, as small metastases do not always have a high signal intensity and areas of hemorrhage may raise the intensity of the signal arising from a benign adenoma.
Address reprint requests to: N. Reed Dunnick, M.D., Department of Radiology, Duke University, Durham, NC 27710, USA
Myelolipoma
An adrenal myelolipoma is a rare tumor comprised of both fat and bone marrow elements. Although

N.R. Dunnick: CT and MRI of Adrenal Lesions 13
A
Fig. 1. Benign adenoma. A A 2 cm left adrenal mass is seen on this T~ (TR 500, TE 25) weighted image. B The signal intensity is similar to normal adrenal tissue on T2 (TR 2500, TE 80) weighted images, indicating its benign nature.
most of these tumors are small and reported in au- topsy series, larger lesions may become symptom- atic and can usually be diagnosed with confidence due to their appreciable fat content (Fig. 2). How- ever, there may be varying amounts o f myeloid or stromal elements, which can increase the density o f these tumors and preclude a confident diagnosis.
Cyst
A homogeneous, rounded mass with a density near water, which does not enhance and has a thin wall, may be regarded as a benign cyst, whether it is renal or adrenal in location. However , adrenal pseudo- cysts are almost as c o m m o n as true endothelial cysts and may be detected more frequently since they tend to be larger. Pseudocysts have a fibrous wall that may contain calcification, and internal septa are common. Pseudocysts are thought to arise f rom hemorrhage into the adrenal gland.
Metastases
The adrenal glands are a rich site of metastatic dis- ease. Abrams and co-workers found adrenal metas- tases in 27% of 1,000 consecutive pos tmor tem ex- aminat ions o f patients with malignant neoplasms o f epithelial origin. Thus, examinat ion o f the adrenal glands by CT is frequently included in the staging evaluation o f a variety o f tumors. An adrenal mass in a patient with an underlying pr imary malignancy is most likely an adrenal metastasis. However , if the adrenal mass is the only evidence of metastatic dis- ease, confirmation is needed and may be obtained from percutaneous fine-needle aspiration.
Fig. 2 Myelolipoma. The obvious fatty density of this 6 cm right adrenal mass (arrow) indicates a myelolipoma.
Adrenal metastases usually demonstra te a high signal intensity on T2-weighted images that differ- entiates them from nonfunctioning adrenal adeno- mas (Fig. 3). However , small metastatic deposits or metastases from a tumor with a low T2 may not show this increased signal intensity.
Fur thermore, an increased signal on T2-weight- ed images is not pathognomonic of a metastasis. Both pheochromocy toma and neuroblas toma have a high intensity on T2-weighted images. Most o f these, however, can be exluded by the clinical setting and absence of endocrinologic abnormali ty. Both adrenal hemorrhage and myelol ipoma also have a high signal intensity on T2-weighted images. How- ever, they can be differentiated from metastases by their increased signal on Tl-weighted images. Ad- renal cysts do not usually present a problem, since

14 N.R. Dunnick: CT and MRI of Adrenal Lesions
Fig. 3. Metastasis. A A large left adrenal mass (M) in this patient with large cell carcinoma of the lung suggests as adrenal metastasis. B The high signal intensity on a T2-weighted image (TR 2500, TE 80) supports its malignant nature.
Fig. 4 Adrenal hemorrhage. Bilateral adrenal enlargement with high-density material on an unenhanced CT scan suggests adrenal hemorrhage.
they are usually recognized on either CT or ultra- sound.
Lymphomatous involvement of the adrenal glands is more common with non-Hodgkin's lym- phoma than with Hodgkin's disease. It is frequently bilateral and almost always accompanied by tumor in other locations. The CT appearance is that of a soft tissue mass with no characteristic features that might differentiate it from other adrenal masses.
Hemorrhage
Adrenal hemorrhage in the perinatal period is a common event and frequently assumed to be the cause of adrenal calcification. Adrenal hemorrhage, either spontaneous or as the result of trauma or antieoagulation results in a mass of soft tissue den-
sity. If the hemorrhage is recent, the density may be high (Fig. 4), while old hematomas undergo liqui- fication and have a low attenuation coefficient.
Recently the association of adrenal hemorrhage and Addison's disease has been emphasized. Pa- tients with this condition are frequently ill, and the signs and symptoms of adrenal insufficiency are rel- atively subtle. Serial CT examination will reveal evolution and usually resorption of adrenal hem- orrhage.
Functional Adrenal Lesions
Primary Aldosteronism
Patients with primary aldosteronism (Conn's syn- drome) present with hypertension and hypokalemia. The serum and urinary aldosterone levels are ele- vated, but the serum renin level is low. Since these tumors are small, averaging less than 2 cm in di- ameter, the CT examination must be done with nar- row (1.5-5 mm) collimation. A minority of these patients have bilateral adrenal hyperplasia rather than an adrenal adenoma as the cause. When pri- mary aldosteronism has been confirmed biochem- ically, the role of radiology is to identify and localize an adrenal tumor. This can usually be done with CT; however, as many as one-third of aldosteron- omas cannot be identified by CT due to their small size, and adrenal venous sampling may be needed.
Cushing's syndrome
The clinical presentation of patients with Cushing's syndrome includes truncal obesity, hirsutism, ab- dominal striae, muscle wasting, and hypertension.

N.R. Dunnick: CT and MRI of Adrenal Lesions 15
Fig. 5. Adrenal carcinoma. A This huge mass (3//) with hepatic invasion is most likely a primary adrenocortlcal carcinoma. B The high signal intensity on T2-weighted images is typical.
Fig. 6. Pheochromocytoma. A Adrenal pheochromocytomas (P) are usually readily detected with CT. B The high signal intensity on T_,-weighted images (TR 2500, TE 80) makes MR useful in problem cases, such as patients who have undergone previous retroperitoneal surgery with disruption of tissue planes.
The most c o m m o n cause is bilateral adrenal hy- perplasia due to st imulation by A C T H from a pi- tuitary adenoma. The adrenal glands are not always recognizably enlarged, but may be normal in size and hyperfunctioning. The abundant fat produced by these patients usually results in excellent delin- eation by CT of the adrenal glands within the peri- renal fat. Adrenal adenomas causing Cushing's syn- d rome are almost always detected, since they are usually more than 2 cm in diameter.
Carcinoma
Adrenal carcinomas frequently outgrow their blood supply and demonstra te central necrosis. Calcifi-
cation is another c o m m o n feature that may be de- tected by CT. The tumor may extend along the ad- renal vein into the renal vein or inferior vena cava. The CT scan has been useful in detecting venous extension, although vena cavography via the su- perior vena cava and right atr ium may be needed to delineate the cephalad extent o f the tumor. A CT scan is also useful in assessing other staging param- eters o f pr imary adrenal carcinoma, such as exten- sion outside Gerota 's fascia, involvement of region- al lymph nodes, or hepatic metastases.
The ability o f MRI to differentiate benign from malignant adrenal masses is not usually helpful in adrenal carcinoma, since the large size o f these tu- mors indicates a malignant etiology (Fig. 5). An MR

16
image m a y be useful, however , in defining extension into the inferior vena cava.
P h e o c h r o m o c y t o m a
Episodic hypertension, tachycardia, sweating, and headache are c o m m o n presenting s y m p t o m s o f pa- tients with a pheoch romocy toma . Approx imate ly 90 percent o f p h e o c h r o m o c y t o m a s lie in the adrenal medul la and 10 percent are bilateral. Those patients with mult iple endocrine neoplasia syndrome (MEN) have associated medul lary ca rc inoma o f the thyroid and para thyroid hyperplasia. They frequently have a family history of endocrine disorders, which are inheri ted as an au~osomal dominan t trait. The pheo- c h r o m o c y t o m a s among these M E N patients are usu- ally bilateral but rarely extraadrenal. Pheochrom- ocytomas average 5 cm in d iamete r and are readily detected by CT. I f careful s tudy o f the adrenal glands fails to identify the tumor , the examina t ion should be cont inued through the lower a b d o m e n to include the paraaort ic region.
The accuracy o f CT for localizing pheoch romo- cy tomas is greater than 90% in identifying intraab- domina l tumors . Since ex t raabdomina l pheochro- m o c y t o m a s are rare, further CT examinat ion , such as o f the chest or neck, is not usually warranted. In the few cases in which CT cannot identify the pheo- ch romocy toma , radionuclide scanning or M R I m a y be used.
Where available, radionuclide scanning with 1311 M I B G m a y be very useful. This technique is capable of examining any por t ion o f the body without re- quiring an addit ional injection. Thus, ectopic or metas ta t ic lesions can be readily detected. Asymp- tomat ic p h e o c h r o m o c y t o m a s m a y also be diag- nosed with M I B G scans.
Since p h e o c h r o m o c y t o m a s are relatively large, they can usually be detected by M R I (Fig. 6). The high signal intensity on T2-weighted images aids fur- ther in their identification. This m a y be particularly valuable in patients who have had previous surgery
N.R. Dunnick: CT and MRI of Adrenal Lesions
with p lacement of surgical clips or disrupt ion o f the retroperi toneal fat planes, since they are often dif- ficult to examine with CT.
Suggested Readings
Abrams HL, Spiro R, Goldstein N: Metastases in carcinoma. Cancer 3:74-85, 1950
Baker ME, Spritzer C, Blinder R, Herfkens R J, Leight GS, Dun- nick NR: Benign adrenal lesions mimicking malignancy by MRI: a report of two cases. Radiology 163:669-671, 1987
Cho KJ, Freier DJ, McCormick TL, et al: Adrenal medullary disease in multiple endocrine neoplasia type II. A JR 134:23- 29, 1980
Commons RR, Callaway CP: Adenomas of the adrenal cortex. Arch Intern Med 81:37-41, 1948
Dunnick NR: The adrenal gland, In Taveras JM, Ferrucci JT (eds): Radiology." Diagnosis, Imaging, Intervention. Philadel- phia: JB Lippincott, 1986
Dunnick NR, Doppman JL, Gill JR Jr, et al: Localization of functional adrenal tumors by computed tomography and ve- nous sampling. Radiology 142:429-433, 1982
Dunnick NR, Doppman JL, Mills SR, el al: Preoperative diag- nosis and localization of aldosteronomas by measurement of corticosteroids in adrenal venous blood. Radiology 133:331- 333, 1979
Falke THM, te Strake L, Shaft MI, Sandier MP, Kulkarni MV, Partain CL, Nieuwenhuizen-Kruseman AC, James AE Jr: MR imaging of the adrenals: correlation with computed tomogra- phy. J Comput Assist Tomogr 10(2):242-253, 1986
Francis IR, Glazer GM, Shapiro G, et al: Complementary roles of CT and ~3q-MIBG scintigraphy in diagnosing pheochro- mocytoma. A JR 141:719-725, 1983
Hamper VM, Fishman EK, Hartman DS, Roberts JL, Sanders RC: Primary adrenocortical carcinoma: sonographic evalua- tion with clinical and pathologic correlation in 26 patients. A JR 148:915-919, 1987
Johnson CD, Baker ME, Dunnick NR: CT demonstration of an adrenal pseudocyst. J Comput Assist Tomogr 9:817-819, 1985
Quint LE, Glazer GM, Francis IR, Shapiro B, Chenevert TL: Pheochromocytoma and paraganglioma: comparison of MR imaging with CT and I- 131 MIBG scintigraphy. Radiology 165: 89-93, 1987
Welch TJ, Sheedy PF, van Heerden JA, et al: Pheochromocy- toma: value of computed tomography. Radiology 148:501- 503, 1983
Zornoza J, Ordonez N, Bernardino ME, et al: Percutaneous bi- opsy of adrenal tumors. Urology 18:412-416, 1981









![The diagnostic value of MRI multi-parameter combination ... · hancement (internal enhancement pattern) [1-3] of breast lesions on dynamic contrast-enhanced MRI (DCE-MRI) indicates](https://img.pdfslide.net/doc/110x75/5fa73044450d904265457571/the-diagnostic-value-of-mri-multi-parameter-combination-hancement-internal.jpg)