Embed Size (px)
Citation preview
www.appliedradiology.com APPLIED RADIOLOGY©� 15July 2002
The nontraumatic acute abdomenis one of the most common pre-sentations to the emergency
room, with appendicitis being one ofthe most common causes of the acuteabdomen. Up to 30% of patients sus-pected of having acute appendicitiswill present with atypical signs andsymptoms.1 There are many conditionsthat mimic acute appendicitis.2 Thepercentage of unnecessary appendec-tomies that result from a clinical false-positive diagnosis of appendicitis isreported to be 8% to 43%, with a meanof approximately 20%.3
The use of computed tomography(CT) before planned surgery hasdecreased the negative appendicec-tomy rate for patients with suspectedacute appendicitis. Recognition of thetypical and atypical CT signs of appen-dicitis is important to optimize thediagnosis yield of the examination.Visualization of an appendix with nor-mal characteristics is the most impor-tant finding to exclude appendicitis.
To determine the individual fre-quency of CT signs of acute appendici-tis and common features of the normalappendix, CT results obtained in 113patients examined at the author’s hos-pital for suspected appendicitis wereevaluated retrospectively.
Subjects and methods A total of 113 patients with sus-
pected acute appendicitis were referredfor thin-section helical CT from thedepartments of surgery and emergencymedicine. Patients ranged in age from8 to 80 years (5 patients were youngerthan 15 years of age) and included 71males and 42 females. CT diagnoseswere recorded retrospectively. Thestudies were performed on an Advan-tage HI speed helical CT scanner (GEMedical Systems, Milwaukee, WI)using 3-, 5-, or 7-mm slice thickness.Some patients received oral entericcontrast. Intravenous contrast wasadministered to 29 of 57 (51%) ofpatients with acute appendicitis.
Cases were reviewed for the followingCT findings: maximum transverse diam-eter of the appendix, the “target” sign,calcified appendicolith, periappendicealinflammation, appendiceal tip stranding,the “comet-tail” sign, the psoas sign, the“arrowhead sign,” the presence of appen-diceal air (intraluminal, intramural, andperiappendiceal), the position of theappendix (retrocecal or right hemipelvisand low abdomen), and the presence offree intraperitoneal fluid.
Final diagnoses were establishedbased on pathologic findings of surgicalspecimens, clinical follow-up, or both.All cases of appendicitis were confirmedby surgical and pathologic findings.Negative diagnoses were confirmed sur-gically or through chart review untilpatient discharge. The variation and fre-
quency of various CT signs of theinflamed appendix and characteristics ofthe normal appendix were noted.
ResultsAmong the 113 patients studied by
preoperative helical CT, 57 patients hadsurgically and pathologically provenappendicitis. The other 56 patients did not have either surgical or clinicalevidence of appendicitis at discharge.
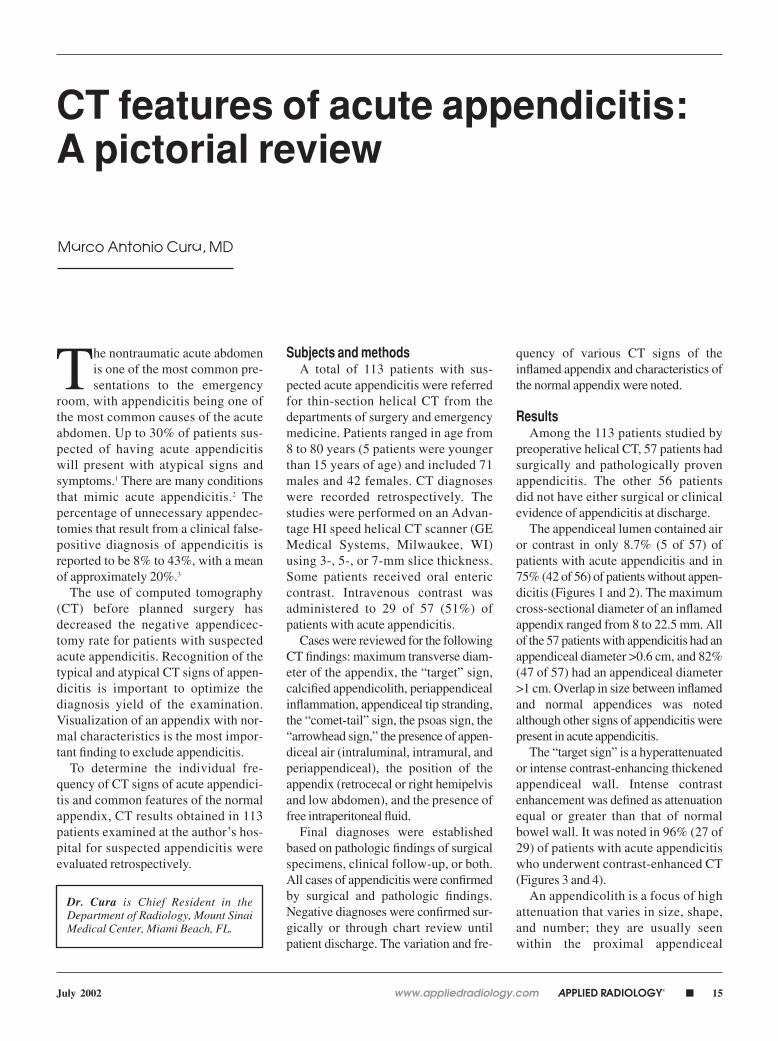
The appendiceal lumen contained airor contrast in only 8.7% (5 of 57) ofpatients with acute appendicitis and in75% (42 of 56) of patients without appen-dicitis (Figures 1 and 2). The maximumcross-sectional diameter of an inflamedappendix ranged from 8 to 22.5 mm. Allof the 57 patients with appendicitis had anappendiceal diameter >0.6 cm, and 82%(47 of 57) had an appendiceal diameter>1 cm. Overlap in size between inflamedand normal appendices was notedalthough other signs of appendicitis werepresent in acute appendicitis.
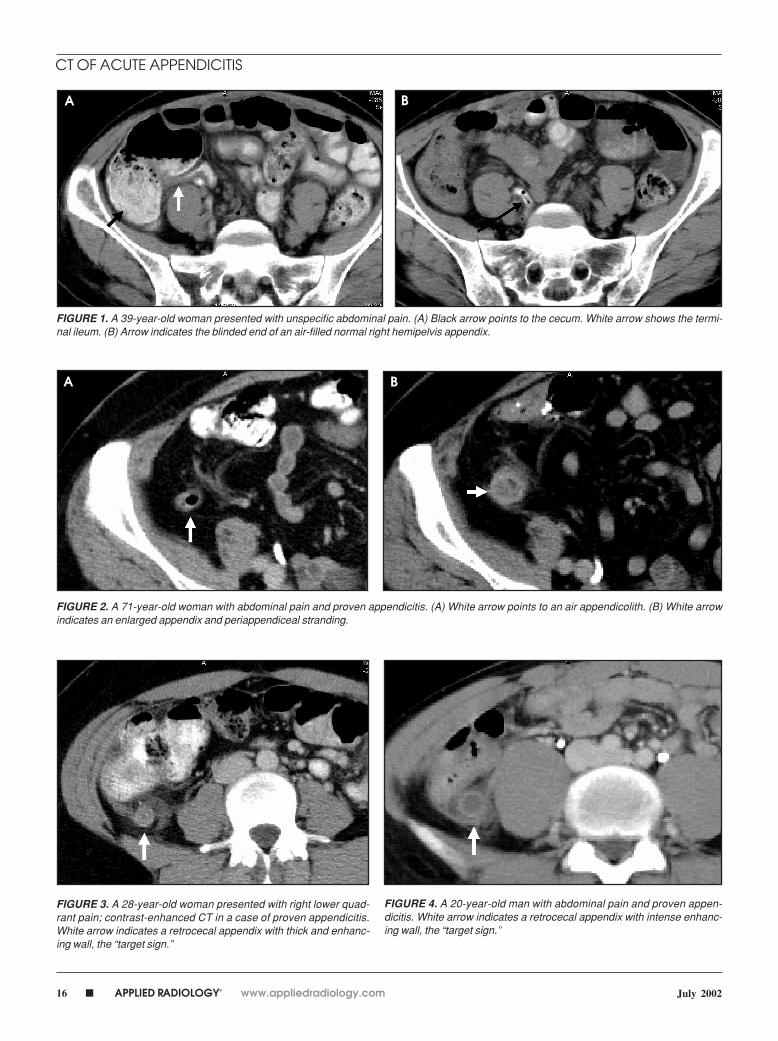
The “target sign” is a hyperattenuatedor intense contrast-enhancing thickenedappendiceal wall. Intense contrastenhancement was defined as attenuationequal or greater than that of normalbowel wall. It was noted in 96% (27 of29) of patients with acute appendicitiswho underwent contrast-enhanced CT(Figures 3 and 4).
An appendicolith is a focus of highattenuation that varies in size, shape,and number; they are usually seenwithin the proximal appendiceal
Marco Antonio Cura, MD
CT features of acute appendicitis:A pictorial review
Dr. Cura is Chief Resident in theDepartment of Radiology, Mount SinaiMedical Center, Miami Beach, FL.
16 � APPLIED RADIOLOGY© www.appliedradiology.com July 2002
FIGURE 1. A 39-year-old woman presented with unspecific abdominal pain. (A) Black arrow points to the cecum. White arrow shows the termi-nal ileum. (B) Arrow indicates the blinded end of an air-filled normal right hemipelvis appendix.
FIGURE 2. A 71-year-old woman with abdominal pain and proven appendicitis. (A) White arrow points to an air appendicolith. (B) White arrowindicates an enlarged appendix and periappendiceal stranding.
FIGURE 3. A 28-year-old woman presented with right lower quad-rant pain; contrast-enhanced CT in a case of proven appendicitis.White arrow indicates a retrocecal appendix with thick and enhanc-ing wall, the “target sign.”
FIGURE 4. A 20-year-old man with abdominal pain and proven appen-dicitis. White arrow indicates a retrocecal appendix with intense enhanc-ing wall, the “target sign.”
A B
A B
CT OF ACUTE APPENDICITIS
www.appliedradiology.com APPLIED RADIOLOGY©� 17July 2002
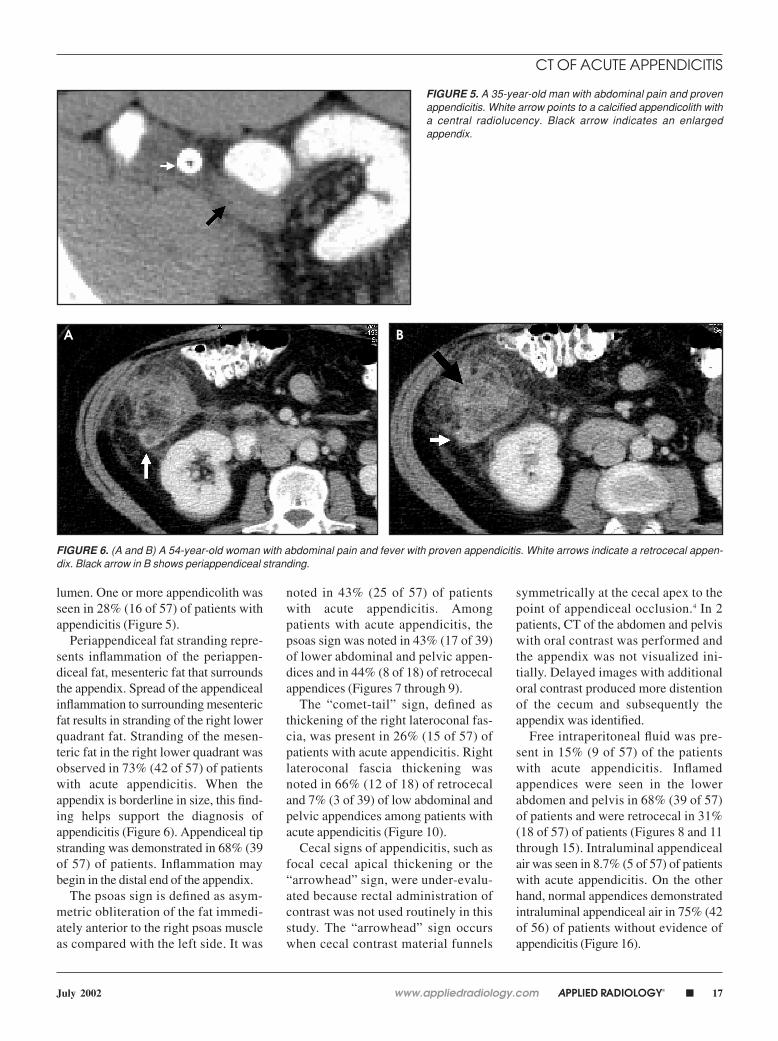
lumen. One or more appendicolith wasseen in 28% (16 of 57) of patients withappendicitis (Figure 5).
Periappendiceal fat stranding repre-sents inflammation of the periappen-diceal fat, mesenteric fat that surroundsthe appendix. Spread of the appendicealinflammation to surrounding mesentericfat results in stranding of the right lowerquadrant fat. Stranding of the mesen-teric fat in the right lower quadrant wasobserved in 73% (42 of 57) of patientswith acute appendicitis. When theappendix is borderline in size, this find-ing helps support the diagnosis ofappendicitis (Figure 6). Appendiceal tipstranding was demonstrated in 68% (39of 57) of patients. Inflammation maybegin in the distal end of the appendix.
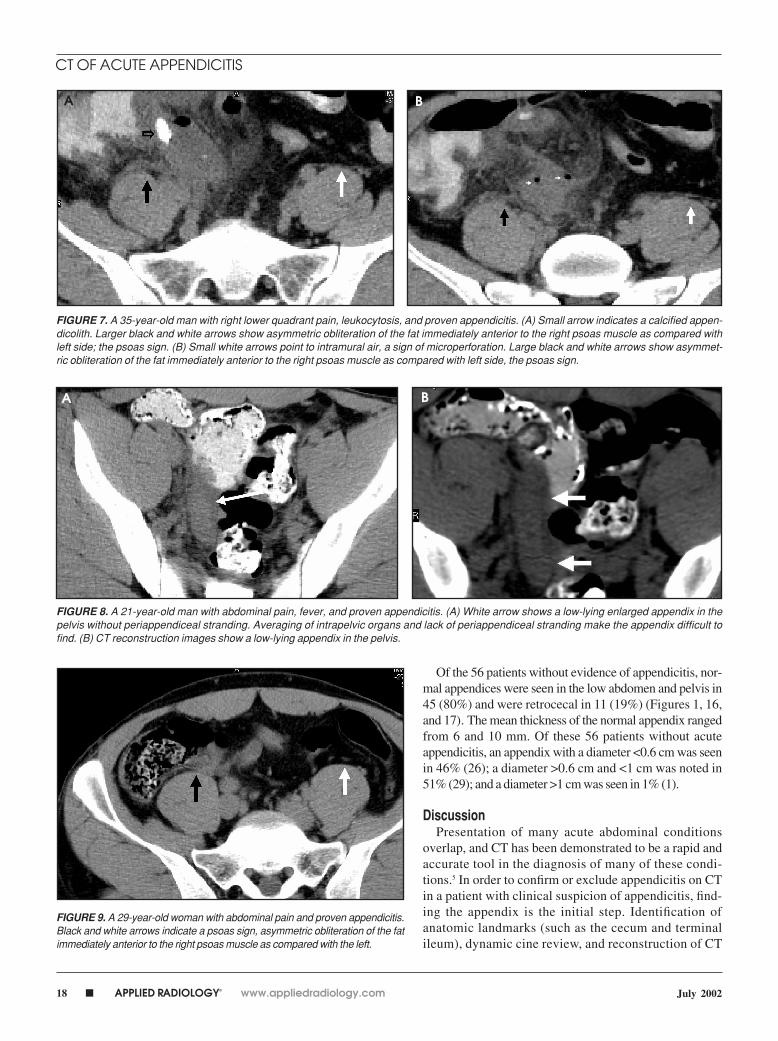
The psoas sign is defined as asym-metric obliteration of the fat immedi-ately anterior to the right psoas muscleas compared with the left side. It was
noted in 43% (25 of 57) of patientswith acute appendicitis. Amongpatients with acute appendicitis, thepsoas sign was noted in 43% (17 of 39)of lower abdominal and pelvic appen-dices and in 44% (8 of 18) of retrocecalappendices (Figures 7 through 9).
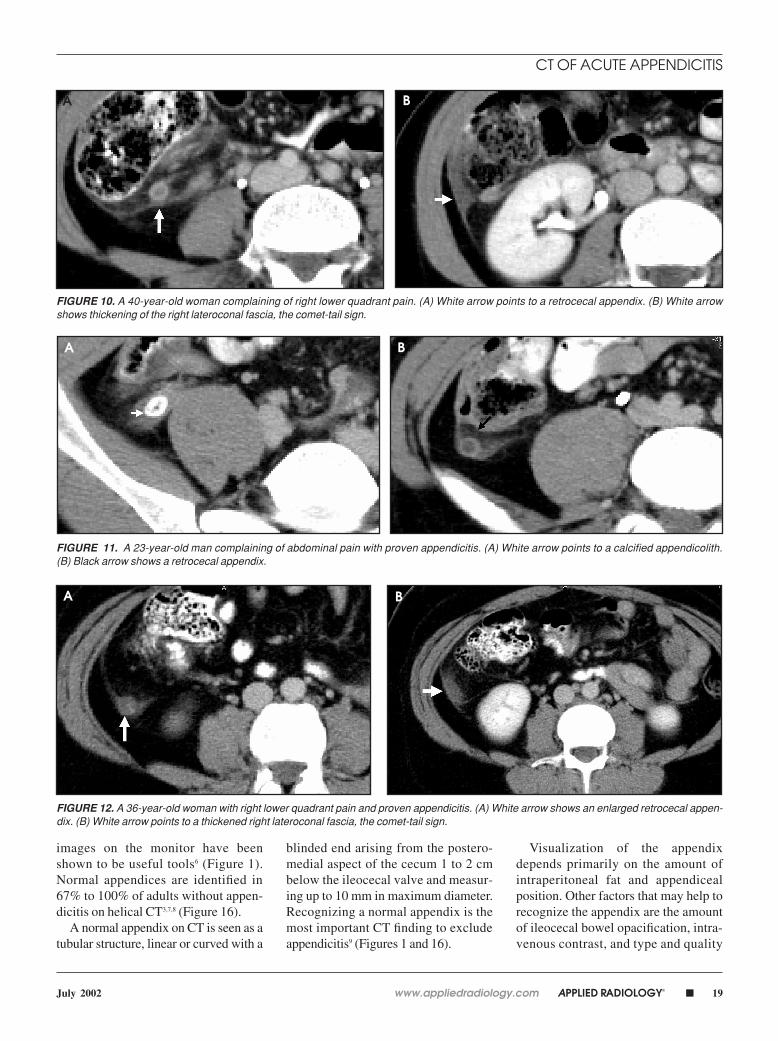
The “comet-tail” sign, defined asthickening of the right lateroconal fas-cia, was present in 26% (15 of 57) ofpatients with acute appendicitis. Rightlateroconal fascia thickening wasnoted in 66% (12 of 18) of retrocecaland 7% (3 of 39) of low abdominal andpelvic appendices among patients withacute appendicitis (Figure 10).
Cecal signs of appendicitis, such asfocal cecal apical thickening or the“arrowhead” sign, were under-evalu-ated because rectal administration ofcontrast was not used routinely in thisstudy. The “arrowhead” sign occurswhen cecal contrast material funnels
symmetrically at the cecal apex to thepoint of appendiceal occlusion.4 In 2patients, CT of the abdomen and pelviswith oral contrast was performed andthe appendix was not visualized ini-tially. Delayed images with additionaloral contrast produced more distentionof the cecum and subsequently theappendix was identified.
Free intraperitoneal fluid was pre-sent in 15% (9 of 57) of the patientswith acute appendicitis. Inflamedappendices were seen in the lowerabdomen and pelvis in 68% (39 of 57)of patients and were retrocecal in 31%(18 of 57) of patients (Figures 8 and 11through 15). Intraluminal appendicealair was seen in 8.7% (5 of 57) of patientswith acute appendicitis. On the otherhand, normal appendices demonstratedintraluminal appendiceal air in 75% (42of 56) of patients without evidence ofappendicitis (Figure 16).
FIGURE 5. A 35-year-old man with abdominal pain and provenappendicitis. White arrow points to a calcified appendicolith witha central radiolucency. Black arrow indicates an enlargedappendix.
FIGURE 6. (A and B) A 54-year-old woman with abdominal pain and fever with proven appendicitis. White arrows indicate a retrocecal appen-dix. Black arrow in B shows periappendiceal stranding.
A B
CT OF ACUTE APPENDICITIS
18 � APPLIED RADIOLOGY© www.appliedradiology.com July 2002
FIGURE 7. A 35-year-old man with right lower quadrant pain, leukocytosis, and proven appendicitis. (A) Small arrow indicates a calcified appen-dicolith. Larger black and white arrows show asymmetric obliteration of the fat immediately anterior to the right psoas muscle as compared withleft side; the psoas sign. (B) Small white arrows point to intramural air, a sign of microperforation. Large black and white arrows show asymmet-ric obliteration of the fat immediately anterior to the right psoas muscle as compared with left side, the psoas sign.
FIGURE 8. A 21-year-old man with abdominal pain, fever, and proven appendicitis. (A) White arrow shows a low-lying enlarged appendix in thepelvis without periappendiceal stranding. Averaging of intrapelvic organs and lack of periappendiceal stranding make the appendix difficult tofind. (B) CT reconstruction images show a low-lying appendix in the pelvis.
FIGURE 9. A 29-year-old woman with abdominal pain and proven appendicitis.Black and white arrows indicate a psoas sign, asymmetric obliteration of the fatimmediately anterior to the right psoas muscle as compared with the left.
Of the 56 patients without evidence of appendicitis, nor-mal appendices were seen in the low abdomen and pelvis in45 (80%) and were retrocecal in 11 (19%) (Figures 1, 16,and 17). The mean thickness of the normal appendix rangedfrom 6 and 10 mm. Of these 56 patients without acuteappendicitis, an appendix with a diameter <0.6 cm was seenin 46% (26); a diameter >0.6 cm and <1 cm was noted in51% (29); and a diameter >1 cm was seen in 1% (1).
DiscussionPresentation of many acute abdominal conditions
overlap, and CT has been demonstrated to be a rapid andaccurate tool in the diagnosis of many of these condi-tions.5 In order to confirm or exclude appendicitis on CTin a patient with clinical suspicion of appendicitis, find-ing the appendix is the initial step. Identification ofanatomic landmarks (such as the cecum and terminalileum), dynamic cine review, and reconstruction of CT
A B
A B
CT OF ACUTE APPENDICITIS
www.appliedradiology.com APPLIED RADIOLOGY©� 19July 2002
FIGURE 10. A 40-year-old woman complaining of right lower quadrant pain. (A) White arrow points to a retrocecal appendix. (B) White arrowshows thickening of the right lateroconal fascia, the comet-tail sign.
FIGURE 11. A 23-year-old man complaining of abdominal pain with proven appendicitis. (A) White arrow points to a calcified appendicolith. (B) Black arrow shows a retrocecal appendix.
FIGURE 12. A 36-year-old woman with right lower quadrant pain and proven appendicitis. (A) White arrow shows an enlarged retrocecal appen-dix. (B) White arrow points to a thickened right lateroconal fascia, the comet-tail sign.
images on the monitor have beenshown to be useful tools6 (Figure 1).Normal appendices are identified in67% to 100% of adults without appen-dicitis on helical CT3,7,8 (Figure 16).
A normal appendix on CT is seen as atubular structure, linear or curved with a
blinded end arising from the postero-medial aspect of the cecum 1 to 2 cmbelow the ileocecal valve and measur-ing up to 10 mm in maximum diameter.Recognizing a normal appendix is themost important CT finding to excludeappendicitis9 (Figures 1 and 16).
Visualization of the appendixdepends primarily on the amount ofintraperitoneal fat and appendicealposition. Other factors that may help torecognize the appendix are the amountof ileocecal bowel opacification, intra-venous contrast, and type and quality
A B
A B
A B
CT OF ACUTE APPENDICITIS
20 � APPLIED RADIOLOGY© www.appliedradiology.com July 2002
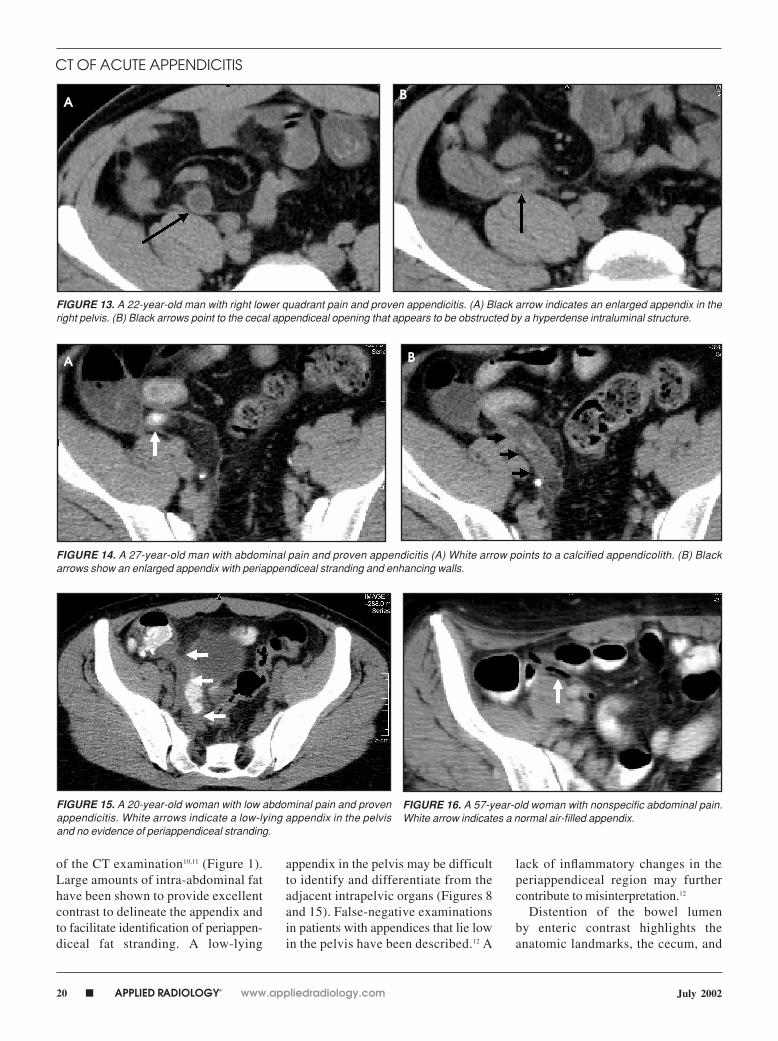
FIGURE 13. A 22-year-old man with right lower quadrant pain and proven appendicitis. (A) Black arrow indicates an enlarged appendix in theright pelvis. (B) Black arrows point to the cecal appendiceal opening that appears to be obstructed by a hyperdense intraluminal structure.
FIGURE 14. A 27-year-old man with abdominal pain and proven appendicitis (A) White arrow points to a calcified appendicolith. (B) Blackarrows show an enlarged appendix with periappendiceal stranding and enhancing walls.
FIGURE 15. A 20-year-old woman with low abdominal pain and provenappendicitis. White arrows indicate a low-lying appendix in the pelvisand no evidence of periappendiceal stranding.
FIGURE 16. A 57-year-old woman with nonspecific abdominal pain.White arrow indicates a normal air-filled appendix.
of the CT examination10,11 (Figure 1).Large amounts of intra-abdominal fathave been shown to provide excellentcontrast to delineate the appendix andto facilitate identification of periappen-diceal fat stranding. A low-lying
appendix in the pelvis may be difficultto identify and differentiate from theadjacent intrapelvic organs (Figures 8and 15). False-negative examinationsin patients with appendices that lie lowin the pelvis have been described.12 A
lack of inflammatory changes in theperiappendiceal region may furthercontribute to misinterpretation.12
Distention of the bowel lumen by enteric contrast highlights theanatomic landmarks, the cecum, and
B
B
CT OF ACUTE APPENDICITIS
A
A
www.appliedradiology.com APPLIED RADIOLOGY©� 21July 2002
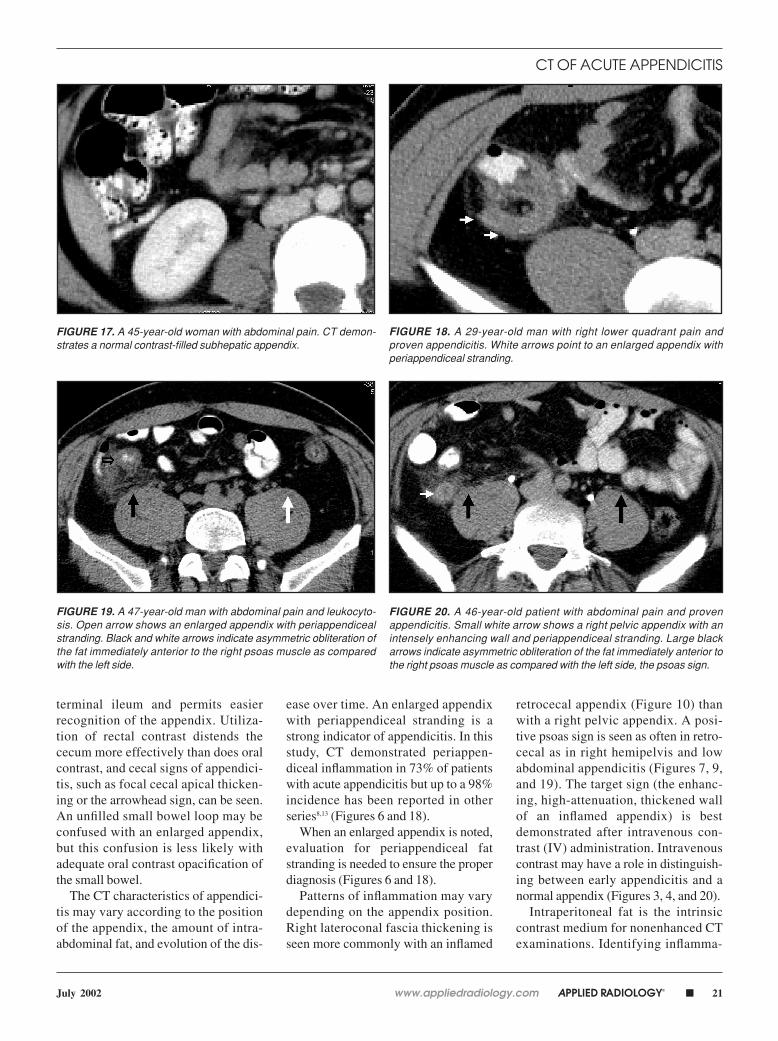
FIGURE 18. A 29-year-old man with right lower quadrant pain andproven appendicitis. White arrows point to an enlarged appendix withperiappendiceal stranding.
FIGURE 19. A 47-year-old man with abdominal pain and leukocyto-sis. Open arrow shows an enlarged appendix with periappendicealstranding. Black and white arrows indicate asymmetric obliteration ofthe fat immediately anterior to the right psoas muscle as comparedwith the left side.
FIGURE 20. A 46-year-old patient with abdominal pain and provenappendicitis. Small white arrow shows a right pelvic appendix with anintensely enhancing wall and periappendiceal stranding. Large blackarrows indicate asymmetric obliteration of the fat immediately anterior tothe right psoas muscle as compared with the left side, the psoas sign.
terminal ileum and permits easierrecognition of the appendix. Utiliza-tion of rectal contrast distends thececum more effectively than does oralcontrast, and cecal signs of appendici-tis, such as focal cecal apical thicken-ing or the arrowhead sign, can be seen.An unfilled small bowel loop may beconfused with an enlarged appendix,but this confusion is less likely withadequate oral contrast opacification ofthe small bowel.
The CT characteristics of appendici-tis may vary according to the positionof the appendix, the amount of intra-abdominal fat, and evolution of the dis-
ease over time. An enlarged appendixwith periappendiceal stranding is astrong indicator of appendicitis. In thisstudy, CT demonstrated periappen-diceal inflammation in 73% of patientswith acute appendicitis but up to a 98%incidence has been reported in otherseries8,13 (Figures 6 and 18).
When an enlarged appendix is noted,evaluation for periappendiceal fatstranding is needed to ensure the properdiagnosis (Figures 6 and 18).
Patterns of inflammation may varydepending on the appendix position.Right lateroconal fascia thickening isseen more commonly with an inflamed
retrocecal appendix (Figure 10) thanwith a right pelvic appendix. A posi-tive psoas sign is seen as often in retro-cecal as in right hemipelvis and lowabdominal appendicitis (Figures 7, 9,and 19). The target sign (the enhanc-ing, high-attenuation, thickened wallof an inflamed appendix) is bestdemonstrated after intravenous con-trast (IV) administration. Intravenouscontrast may have a role in distinguish-ing between early appendicitis and anormal appendix (Figures 3, 4, and 20).
Intraperitoneal fat is the intrinsiccontrast medium for nonenhanced CTexaminations. Identifying inflamma-
FIGURE 17. A 45-year-old woman with abdominal pain. CT demon-strates a normal contrast-filled subhepatic appendix.
CT OF ACUTE APPENDICITIS

22 � APPLIED RADIOLOGY© www.appliedradiology.com July 2002
tory changes in slender patients withlittle periappendiceal and pericecal fatmay be difficult; therefore, false-nega-tive interpretations have been reportedin pediatric patients and young women.14
An appendicolith has a high speci-ficity for the diagnosis of acute appen-dicitis (Figures 5, 11, 21, and 22). Theinitial event in acute appendicitis islikely the appendicolith obstruction of the appendiceal lumen.15,16 Theobstructed lumen leads to increasedintraluminal pressures, causing venouscongestion, arterial compromise, andtissue ischemia. Subsequently, there isepithelial mucosal barrier interruption,bacterial invasion, and transmuralappendiceal wall inflammation.17
Finally, appendiceal wall infarctionand perforation occur, which allowsthe inflammatory process to extend tothe periappendiceal mesenteric fat,parietal peritoneum, and adjacentstructures.17
Intraluminal appendiceal air is afinding on CT in both normal andinflamed appendices. However, intra-luminal air is seen more commonly innormal appendices than in inflamedappendices. The appendix is connectedto the cecum, a gas-filled viscus, andair probably regurgitates from the
cecum into the nonobstructed appen-diceal lumen.15 Intraluminal air can beseen in early appendicitis but is anuncommon finding in the late stages ofthe disease; appendiceal luminal air isprobably resorbed after obstruction.15
Intramural, extraluminal or periappen-diceal air is more characteristic ofadvanced inflammation and indicates aperforated appendix15 (Figure 7).
Summary Intraluminal gas and an appendiceal
diameter measuring up to 10 mm onCT are common findings of a normalappendix. Recognition of a normalappendix is required to exclude appen-dicitis. An enlarged appendix withperiappendiceal inflammation is themost common finding of acute appen-dicitis. Fat stranding may present indifferent patterns depending on loca-tion of the appendix. AR
REFERENCES1. Lewis FR, Holcroft JW, Boey J, Dunphy JE. Appen-dicitis: A critical review of diagnosis and treatment in100 cases. Arch Surg. 1975;110:677-684.2. Lau WY, Fan ST, Yiu TF, et al. Negative findingsat appendectomy. Am J Surg. 1984;148:375-378.3. Schuler JG, Shortsleeve MJ, Goldenson RS, et al.Is there a role for abdominal computed tomographicscans in appendicitis? Arch Surg. 1998;133:373-376.4. Rao PM, Wittenberg J, McDowell RK, et al.
Appendicitis: Use of arrowhead sign for diagnosisat CT. Radiology. 1997:202:363-366. 5. Lane MJ, Katz DS, Ross BA, et al. Unenhancedhelical CT for suspected acute appendicitis. AJRAm J Roentgenol. 1997;168:405-409. 6. Birnbaum BA, Wilson SR. Appendicitis at themillennium. Radiology. 2000;215:337-348.7. Lane MJ, Katz DS, Ross BA, et al. Unenhancedhelical CT for suspected acute appendicitis. AJRAm J Roentgenol. 1997;168:405-409.8. Weltman DI, Yu J, Krumenacker J Jr, et al. Diag-nosis of acute appendicitis: Comparison of 5- and10-mm CT sections in the same patient. Radiol-ogy. 2000;216:172-177. 9. Rao PM, Rhea JT, Novelline RA. Sensitivity andspecificity of the individual CT signs of appendicitis:Experience with 200 helical appendiceal CT exami-nations. J Comput Assist Tomogr. 1997;21:686-692.10. Birnbaum BA, Jeffrey RB, Jr. CT and sono-graphic evaluation of acute right lower quadrantpain. AJR Am J Roentgenol. 1998;170:361-371. 11. Birnbaum BA, Balthazar EJ. CT of appendicitis anddiverticulitis. Radiol Clin North Am. 1994;32:885-898.12. Lane MJ, Liu DM, Huynh MD, et al. Suspectedacute appendicitis: Nonenhanced helical CT in 300consecutive patients. Radiology. 1999;213:341-346.13. Rao PM, Rhea JT, Novelline RA, et al. Helical CTcombined with contrast material administered onlythrough the colon for imaging of suspected appen-dicitis. AJR Am J Roentgenol. 1997;169:1275-1280.14. Malone AJ, Wolf CR, Malmed AS, Melliere BF.Diagnosis of acute appendicitis: Value of unenhancedCT. AJR Am J Roentgenol. 1993;160:763-766. 15. Rettenbacher T, Hollerweger A, Macheiner P,et al. Presence or absence of gas in the appendix:Additional criteria to rule out or confirm acuteappendicitis-evaluation with US. Radiology.2000;214:183-187.16. Poljak A, Jeffrey RB, Kernberg ME. The gas-containing appendix: Potential sonographic pitfallin the diagnosis of acute appendicitis. J UltrasoundMed. 1991;10:625-628.
FIGURE 22. A 5-year-old boy with abdominal pain and proven appen-dicitis. White arrow points to a calcified appendicolith and black arrowpoints to an enlarged appendix.
FIGURE 21. A 26-year-old man with right flank pain and provenappendicitis. Black arrow indicates a calcified appendicolith.
CT OF ACUTE APPENDICITIS




























