Embed Size (px)
Citation preview

ORIGINAL ARTICLE
CT-guided needle biopsy performed with modified coaxialtechnique in patients with refractory or recurrent lymphomas
Francesco Gaudio & Pasquale Pedote & Annunziata Ferrante &
Tommasina Perrone & Giuseppe Ingravallo & Amato Antonio Stabile Ianora &
Giuseppe Angelelli & Giorgina Specchia
Received: 17 August 2013 /Accepted: 8 April 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract The aim of this study was to evaluate the role ofcomputed tomography (CT)-guided core needle biopsy(CNB) performed by modified coaxial technique as an alter-native tool to surgical biopsy in patients with refractory orrecurrent lymphomas. Between May 2005 and May 2012, 57CT-guided CNB of deep lesions were performed in patientswith a previous diagnosis of lymphoma and suspected forrefractory or recurrent disease. A modified coaxial techniquewas used in all cases and multiple samples were obtained forhistological and immunohistochemical studies. A diagnosis oflymphoma with specification of subtype according to theWorld Health Organization (WHO) classification wasestablished in 30/57 cases (52.6 %). The previous diagnosisof lymphoma was confirmed in 27/57 patients (47.4 %),whereas histological progression in 3/57 (5.3 %) and othermalignant neoplasms in 17/57 (29.8 %) were found. Lympho-ma without subtype specification was diagnosed in 6/57(10.5 %), and no conclusive diagnosis could be establishedin 4/57 cases (7 %). Overall diagnostic accuracy was 82.5 %.In patients with a final diagnosis of malignant lymphoma,accuracy was 75%. No complications occurred. PercutaneousCT-guided CNB is a safe, effective and reliable tool in themanagement of patients with refractory or recurrent
lymphomas without superficial lymphadenopathy and can beconsidered as alternative to surgical sampling.
Keywords Lymphoma . Core needle biopsy .
Immunohistochemical
Introduction
Lymphomas are curable by chemotherapy, combined modal-ity therapy (chemotherapy plus radiotherapy) or radiotherapyalone. However, even after this treatment, 20–40% of patientseither progress during treatment or relapse following an initialremission [1–3].
Percutaneous computed tomography (CT)-guided fine nee-dle aspiration biopsy (FNAB) is a widely used procedure inthe diagnosis and follow-up of neoplasms, having high accu-racy values ranging from 80 to 93 % and a low complicationrate [4–6]. However, this technique has been shown to be lessaccurate in the diagnosis of lymphomas compared with othermalignancies [4, 7–9]. Correct diagnosis of lymphoma re-quires, in addition to a morphological study, immunohisto-chemical and molecular analyses to define the exact histolog-ical type and, on this basis, establish the best therapeuticapproach and prognostic significance [10]. For this reason,excisional biopsy of the entire lymph node is considered thegold standard [11].
In patients with suspected diagnosis of lymphoma, in theabsence of superficial lesions, CT-guided core needle biopsy(CNB) has been suggested as a viable alternative to surgicalintervention [12]. The aim of our study was to verify theeffectiveness of CT-guided CNB performed with a modifiedcoaxial technique in a group of patients with refractory orrecurrent lymphomas.
F. Gaudio (*) : T. Perrone :G. SpecchiaDepartment of Emergency and Organ Transplantation (D.E.T.O.),Hematology Section, University of Bari Medical School, Bari, Italye-mail: [email protected]
P. Pedote :A. Ferrante :A. A. S. Ianora :G. AngelelliInterdisciplinary Department of Medicine, Section of Radiology,University of Bari Medical School, Bari, Italy
G. IngravalloDepartment Pathology, University of Bari Medical School, Bari, Italy
Ann HematolDOI 10.1007/s00277-014-2078-0

Materials and methods
Between May 2005 and May 2012, 57 patients (25 womenand 32 men, age range 25–87 years, mean 64) with a previousdiagnosis of lymphoma (shown in Table 1), 33 in relapse and24 refractory to chemotherapy, underwent CT-guided CNB ofdeep-seated lesions. Elapsed time from previous diagnosis toCNB ranged 6–239 months (mean 55).
Patients with superficial site localisation (laterocervical,supraclavear, axillary, inguinal) were excluded from the study,because they are routinely subjected to excisional biopsy or, inselected cases with contraindications to surgery, to needlebiopsy with ultrasound guidance rather than CT. A total of57 CNB were performed.
Before the biopsy, written informed consent was obtainedfrom all patients. Prothrombin time (PT), partial thromboplas-tin time (PTT) and platelet count (PLT) were measured. Pa-tients with prolonged PTand PTT values and/or PLT <50,000/microl received appropriate corrective treatment. PET-CT andcontrast-enhanced CT scans were preliminarily assessed todetermine site, presence of necrotic areas and anatomicalrelationships between lesions so as to select lesions to besampled, best patient position, access site and safest needlepath. Immediately before the biopsy, scans were obtained ofthe area of interest, with anatomical landmarks placed on theskin surface using Multi Detector CTscanner to determine thedistance and angle of the needle in relation to the target. Weused semiautomatic guillotine-type cutting needles, rangingfrom 20 to 16 gauge in diameter and 100 to 200 mm in length,depending on lesion location and size. To facilitate multiplesampling, a modified coaxial technique was used that involvesthe introduction of a cutting needle sheathed in a 6-cm plasticcannula after administration of locoregional anaesthesia(10 ml lidocaine hydrochloric acid 2 %). After checkingcorrect needle position with serial CT scans (3-mm thickness,3-mm increment, 1.25 pitch, 0.5-s rotation time, 120 kVp,250 mAs), the plastic cannula was pushed as deep as possibleand left on site after the first biopsy to be used as a guide for
subsequent biopsies [13]. At least three cores at least 1 cmlong were obtained. The procedure was carried out success-fully in all cases (mean duration 30 min). Immediately afterthe biopsies, a CT scan was performed to study possiblecomplications, and all patients were monitored clinically forat least 24 h. Specimens were fixed in formaldehyde (40 g/l),embedded in paraffin. The histological diagnosis wasestablished according to the World Health Organization(WHO) classification of malignant lymphomas [14]. In agree-ment with other authors, we considered as complete successall cases in which the biopsy provided adequate material toestablish a diagnosis of lymphoma, with specification of his-tological subtype or a diagnosis of other disease; partial suc-cess if the material obtained enabled a diagnosis of malignantlymphoma without specification of a definite histologicaltype; and failure if the material sampled was non-diagnostic[10, 12]. To measure diagnostic accuracy, we considered thecases of complete success in relation to the total number ofCNB performed.
Results
Fifty-seven patients with suspected recurrent lymphoma orrefractory to therapy in the absence of superficial localisationsunderwent CT-guided CNB. The 57 sampled lesions had adiameter ranging from 1.8 to 15 cm (mean 4 cm). No compli-cations occurred.
Location of lymphoma was nodal in 27 cases (47.4 %) andextranodal in 30 (52.6 %). The anatomical distribution oflesions is summarised in Table 2. In 47 CNB, we obtained a
Table 1 Previous lymphoma diagnosis
First diagnosis N Percentage
Follicular lymphoma 19 33.3
Diffuse large B cell lymphoma 13 22.8
Marginal cell lymphoma 9 15.7
Lymphocytic lymphoma 5 8.8
Mantle cell lymphoma 4 7
Hodgkin lymphoma 3 5.3
Lymphoplasmocytic lymphoma 2 3.5
Lymphoblastic lymphoma 1 1.7
Peripheral T cell lymphoma 1 1.7
Table 2 Site of lesionsstudied by core biopsy N %
Lumbar nodes 20 35.1
Pelvic bone 4 7
Lung 4 7
Kidney 4 7
Retroperitoneum 4 7
Liver 3 5.3
Pleura 3 5.3
Celiac nodes 2 3.5
Iliac nodes 2 3.5
Obturator nodes 2 3.5
Paravertebral space 2 3.5
Pelvic peritoneal space 2 3.5
Pancreas 1 1.7
Mesenteric nodes 1 1.7
Tibial plateau 1 1.7
Shoulder 1 1.7
Hepatorenal recess 1 1.7
Ann Hematol
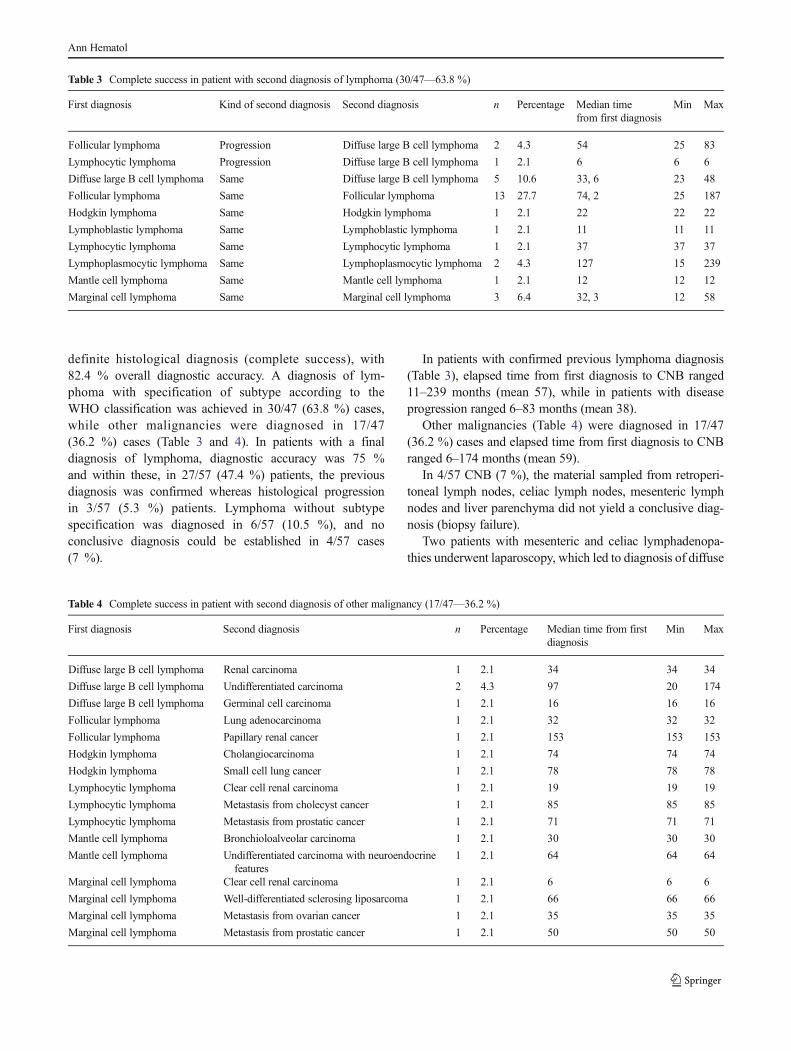
definite histological diagnosis (complete success), with82.4 % overall diagnostic accuracy. A diagnosis of lym-phoma with specification of subtype according to theWHO classification was achieved in 30/47 (63.8 %) cases,while other malignancies were diagnosed in 17/47(36.2 %) cases (Table 3 and 4). In patients with a finaldiagnosis of lymphoma, diagnostic accuracy was 75 %and within these, in 27/57 (47.4 %) patients, the previousdiagnosis was confirmed whereas histological progressionin 3/57 (5.3 %) patients. Lymphoma without subtypespecification was diagnosed in 6/57 (10.5 %), and noconclusive diagnosis could be established in 4/57 cases(7 %).
In patients with confirmed previous lymphoma diagnosis(Table 3), elapsed time from first diagnosis to CNB ranged11–239 months (mean 57), while in patients with diseaseprogression ranged 6–83 months (mean 38).
Other malignancies (Table 4) were diagnosed in 17/47(36.2 %) cases and elapsed time from first diagnosis to CNBranged 6–174 months (mean 59).
In 4/57 CNB (7 %), the material sampled from retroperi-toneal lymph nodes, celiac lymph nodes, mesenteric lymphnodes and liver parenchyma did not yield a conclusive diag-nosis (biopsy failure).
Two patients with mesenteric and celiac lymphadenopa-thies underwent laparoscopy, which led to diagnosis of diffuse
Table 3 Complete success in patient with second diagnosis of lymphoma (30/47—63.8 %)
First diagnosis Kind of second diagnosis Second diagnosis n Percentage Median timefrom first diagnosis
Min Max
Follicular lymphoma Progression Diffuse large B cell lymphoma 2 4.3 54 25 83
Lymphocytic lymphoma Progression Diffuse large B cell lymphoma 1 2.1 6 6 6
Diffuse large B cell lymphoma Same Diffuse large B cell lymphoma 5 10.6 33, 6 23 48
Follicular lymphoma Same Follicular lymphoma 13 27.7 74, 2 25 187
Hodgkin lymphoma Same Hodgkin lymphoma 1 2.1 22 22 22
Lymphoblastic lymphoma Same Lymphoblastic lymphoma 1 2.1 11 11 11
Lymphocytic lymphoma Same Lymphocytic lymphoma 1 2.1 37 37 37
Lymphoplasmocytic lymphoma Same Lymphoplasmocytic lymphoma 2 4.3 127 15 239
Mantle cell lymphoma Same Mantle cell lymphoma 1 2.1 12 12 12
Marginal cell lymphoma Same Marginal cell lymphoma 3 6.4 32, 3 12 58
Table 4 Complete success in patient with second diagnosis of other malignancy (17/47—36.2 %)
First diagnosis Second diagnosis n Percentage Median time from firstdiagnosis
Min Max
Diffuse large B cell lymphoma Renal carcinoma 1 2.1 34 34 34
Diffuse large B cell lymphoma Undifferentiated carcinoma 2 4.3 97 20 174
Diffuse large B cell lymphoma Germinal cell carcinoma 1 2.1 16 16 16
Follicular lymphoma Lung adenocarcinoma 1 2.1 32 32 32
Follicular lymphoma Papillary renal cancer 1 2.1 153 153 153
Hodgkin lymphoma Cholangiocarcinoma 1 2.1 74 74 74
Hodgkin lymphoma Small cell lung cancer 1 2.1 78 78 78
Lymphocytic lymphoma Clear cell renal carcinoma 1 2.1 19 19 19
Lymphocytic lymphoma Metastasis from cholecyst cancer 1 2.1 85 85 85
Lymphocytic lymphoma Metastasis from prostatic cancer 1 2.1 71 71 71
Mantle cell lymphoma Bronchioloalveolar carcinoma 1 2.1 30 30 30
Mantle cell lymphoma Undifferentiated carcinoma with neuroendocrinefeatures
1 2.1 64 64 64
Marginal cell lymphoma Clear cell renal carcinoma 1 2.1 6 6 6
Marginal cell lymphoma Well-differentiated sclerosing liposarcoma 1 2.1 66 66 66
Marginal cell lymphoma Metastasis from ovarian cancer 1 2.1 35 35 35
Marginal cell lymphoma Metastasis from prostatic cancer 1 2.1 50 50 50
Ann Hematol

large B cell and mantle cell lymphoma, while in two otherpatients, the diagnosis was performed by bone marrow biopsy(in all cases previous diagnosis was confirmed) (Table 5).
Discussion
Even though lymphomas are curable, approximately 30 % ofall patients relapse and eventually die of progressive disease orcomplications of therapy [1–3]. Some patients with aproven diagnosis of lymphoma may need to undergo histo-logical revaluation to assess response to therapy, histologicalprogression, presence of concurrent disease or a new malig-nancy [15].
Histological revaluation has traditionally been performedby surgical excision biopsy of an involved node, and thistechnique has represented the gold standard for diagnosis inthis kind of patients, as it provides sufficient material toperform immunophenotypic, cytogenetic and molecular biol-ogy studies required for diagnosis. In those cases where thespecific rearrangement of neoplastic T or B cells is known—also in those cases where the biopsy quality is not optimal—the combination of histomorphological, immunohistochemi-cal and molecular approaches may lead to a clear diagnosis[16–19]. Operative node excision however requires input ofsurgical, nursing and anaesthetic staff, adding considerablecost as well as anaesthetic and surgical risks [20].
In the absence of superficial lymphadenopathy, an alterna-tive to surgery may be provided by CT-guided needle biopsy,characterised by less invasiveness, minimal anaesthetic risk,reduced hospitalisation, lower costs and a reduced incidenceof complications and mortality [21, 22]. However, its role inidentifying lymphoproliferative disease remains controversial[23]. There is considerable doubt as to the effectiveness ofcytology in differentiating reactive lymphoid hyperplasiafrom low-grade lymphoma [16, 23].
CNB performed with 14- to 20-gauge cutting needlesyields enough sampling tissue to perform all immunohisto-chemical studies necessary for accurate diagnosis of lym-phoma [22]. Some authors have emphasised the usefulnessof the coaxial technique for obtaining multiple biopsies in asingle session [10, 24]. The disadvantage of this technique isthe presence of an external cannula that increases the totaldiameter of the biopsy system, leading to a higher risk ofcomplications [5, 25]. In our series, especially in patientswith access points that were difficult to reach and/or in closeproximity to vascular structures, the modified coaxial tech-nique allowed us to easily obtain multiple specimens. Theuse of a soft cannula caused less trauma to the superficialand deep structures, whereas the diameter of the sampledmaterial remained unvaried. Another advantage is the easewith which small changes can be made in the angle of theintroducing cannula to obtain a larger sampling area. CNB T
able5
Partialsuccess
andfailedbiopsy
(10/57—17.5%)
Patients
Firstdiagnosis
CNBsite
CNBdiagnosis
Secondprocedure
Seconddiagnosis
Kindof
second
diagnosis
1Marginalcelllym
phom
aLum
barnodes
Low
gradelymphom
aRefused
a
2Follicular
lymphom
aLum
barnodes
Lym
phom
awith
outsubtype
Laparoscopy
Diffuse
largeBcelllymphom
aProgression
3Marginalcelllym
phom
aLum
barnodes
Lym
phom
awith
outsubtype
Laparoscopy
Diffuse
largeBcelllymphom
aProgression
4Diffuse
largeBcelllymphom
aLum
barnodes
Lym
phom
awith
outsubtype
Laparoscopy
Diffuse
largeBcelllymphom
aSame
5Follicular
lymphom
aCeliacnodes
Lym
phom
awith
outsubtype
Laparoscopy
Follicularlymphom
aSame
6PeripheralT
celllymphom
aPelvicbone
Lym
phom
awith
outsubtype
Intraoperativ
ebiopsy
PeripheralT
celllymphom
aSame
7Diffuse
largeBcelllymphom
aLum
barnodes
Insufficient
material
Bonemarrowbiopsy
Diffuse
largeBcelllymphom
aSame
8Diffuse
largeBcelllymphom
aCeliacnodes
Colliq
uativ
ematerial
Laparoscopy
Diffuse
largeBcelllymphom
aSame
9Mantle
celllymphom
aMesentericnodes
Colliq
uativ
ematerial
Laparoscopy
Mantle
celllymphom
aSame
10Diffuse
largeBcelllymphom
aLiver
Insufficient
material
Bonemarrowbiopsy
Diffuse
largeBcelllymphom
aSame
aTherapy
basedon
previous
diagnosisleadingto
completeremission
Ann Hematol

performed with this technique was well tolerated by mostpatients and was completed according to the establishedprotocol in all cases.
In our study, 57 biopsies on deep-seated lesions wereperformed and diagnostic accuracy was 82.4 %. This valueis in line with the values reported in other series, some ofwhich, however, also included biopsies of superficial lesions[10, 12, 16, 24, 26–30].
After extrapolating from our series the cases with a finaldiagnosis of lymphoma, the diagnostic accuracy of CNB inthese patients was 75%. The previous diagnosis of lymphomawas confirmed in 47.4 %, histological progression of lympho-ma was documented in 5.3 % and a different disease wasdiagnosed in 36.2 %. Lymphoma without subtype specifica-tion was diagnosed in 6/57 (10.5 %), and no conclusivediagnosis could be established in 4/57 cases (7 %).
In 7 % of cases, the procedure failed because the sampledmaterial was insufficient or colliquative and the definite diag-nosis was determined by intraoperative biopsy. CNB can beused as an alternative to surgery also because it does notexclude the possibility of initiating subsequently the patientto surgical biopsy, in the event of failure of the procedure.Furthermore, with the combination of PET-CT and CT-guidedcore needle biopsy, the risk of aspiration of non-diagnosticnecrotic tissue could be reduced. Agid et al. [26] reported thatCT-guided core needle biopsies were sufficient to establish adiagnosis in 83 % of the patients with lymphoproliferativedisorders, and they suggested that it should be used as the firststep in the diagnosis of lymphoma. Stattaus et al. [24] reportedthat the correct lymphoma subtype could be revealed forretroperitoneal masses in 87 % of the patients by using a 16-or 18-gauge core biopsy system with the coaxial techniqueunder CT guidance.
In our study, 20 of 57 (35 %) patients had a defineddiagnosis different from the previous, and the subsequenttreatment was performed on the basis of the results of thebiopsy. It was possible to use a CT-guided biopsy to make thespecific diagnosis of the lymphoma type in most cases, and it
played a very important role in determining the treatmentmodalities. Core biopsy produces a histological prepara-tion which allows cell identification, some assessment oftissue architecture (particularly in larger-gauge biopsies)and immunohistochemistry (Fig. 1). These advantagesgreatly improve the diagnostic yield with conclusive di-agnosis achieved on 84.4 % of needle cores in our series.
Early studies suggested that core biopsy could only fullyclassify lymphoma in 38–51 % of cases. However, some ofthese studies were carried out before the advent of most of thecurrently available monoclonal antibodies [11]. More recentwork has suggested that full subclassification of the diseasewith prompt institution of therapy was possible in 92.3 % ofthe lymphoma patients [31]. In patients with follicular lym-phoma, in 2/15 cases (13 %) was documented a diseaseprogression. By definition, follicular lymphoma is not gradedin biopsies and this fact leads to the problem that the diseaseprogression may be less identified. Our results accord withmore recent studies [28, 31, 32] that achieved subclassifica-tion in 72–96 % of cases. They also correlate with the data ofVandervelde et al. [16] who reported in 2008 with 51 head andneck lymphomas, where 67 % of core biopsies were fullydiagnostic for treatment purposes.
Conclusions
CT-guided CNB is a safe and accurate technique useful inthe management of patients with a previous diagnosis oflymphoma and suspected disease progression or withdeep-seated lesions suggesting a different disease. In theabsence of superficial lymphadenopathies, it represents avaluable alternative to surgical intervention and may radi-cally change treatment decisions.
Conflict of interest The authors declare that they have no conflict ofinterest.
Fig. 1 Cores of tissue at a×40and b×200 magnificationobtained by CNB using an 18-gauge needle. These samples arelarge enough to show tissuearchitecture andimmunohistochemistry to assessthe diagnosis of lymphocytic Bcell lymphoma
Ann Hematol

References
1. Jerkeman M, Anderson H, Dictor M, Kvaløy S, Åkerman M,Cavallin-Ståhl E (2004) Assessment of biological prognostic factorsprovides clinically relevant information in patients with diffuse largeB-cell lymphoma. A Nordic Lymphoma Group study. Ann Hematol83:414–419
2. Swenson WT, Lynch CF, Wooldridge JE, Forman-Hoffman VL,Chrischilles E, Link BK (2005) Improved survival of follicularlymphoma patients in the surveillance, epidemiology, and end-results (SEER) program. J Clin Oncol 23:5019–5026
3. Gaudio F, Giordano A, Pavone V, Perrone T, Curci P, Pastore D,Delia M, de’ Risi C, Spina A, Liso V, Specchia G (2011) Outcome ofvery late relapse in patients with Hodgkin’s lymphomas. AdvHematol 2011:707542
4. Welch TJ, Sheedy PF, Johnson CD, Johnson CM, Stephens DH(1989) CT-guided biopsy: prospective analysis of 1,000 procedures.Radiology 171:493–496
5. Cardella JF, Bakal CW, Bertino RE, Burke DR, Drooz A,Haskal Z, Lewis CA, Malloy PC, Meranze SG, Oglevie SB,Sacks D, Towbin RB (2003) Quality improvement guidelinesfor image-guided percutaneous biopsy in adults. J Vasc IntervRadiol 14:S227–S230
6. Smith EH (1991) Complications of percutaneous abdominal fine-needle biopsy. Rev Radiol 178:253–258
7. Quinn SF, Sheley RC, Nelson HA, Demlow TA, Wienstein RA,Dunkley BL (1995) The role of percutaneous needle biopsies in theoriginal diagnosis of lymphoma: a prospective evaluation. J VascInterv Radiol 6:947–952
8. Yao L, Nelson SD, Seeger LL, Eckardt JJ, Eilber FR (1999) Primarymusculoskeletal neoplasms: effectiveness of core-needle biopsy.Radiology 212:682–686
9. Joensuu H, Alanen K, Klemi PJ (1992) Prognosis of lymphoma froma fine-needle aspirate. Eur J Cancer 29A:29–33
10. De Kerviler E, Guermazi A, Zagdanski AM, Meignin V, Gossot D,Oksenhendler E, Mariette X, Brice P, Frija J (2000) Image-guidedcore-needle biopsy in patients with suspected or recurrent lympho-mas. Cancer 89:647–652
11. Erwin BC, Brynes RK, Chan WC, Keller JW, Phillips VM,Gedgaudas-McClees RK, Torres WE, Bernardino ME (1986)Percutaneous needle biopsy in the diagnosis and classification oflymphoma. Cancer 57:1074–1078
12. Balestreri L, Morassut S, Bernardi D, Tavio M, Talamini R, GloghiniA, Carbone A (2005) Efficacy of CT-guided percutaneous needlebiopsy in the diagnosis of malignant lymphoma at first presentation. JClin Imaging 29:123–127
13. Pedote P, Gaudio F, Moschetta M, Cimmino A, Specchia G,Angelelli G (2010) CT-guided needle biopsy performed with modi-fied coaxial technique in the diagnosis of malignant lymphomas.Radiol Med 115:1292–1303
14. WHO classification of tumours of haematopoietic and lymphoidtissues. IARC 2008, Lyon
15. Goldschmidt N, Libson E, Bloom A, Amir A, Paltiel O (2003)Clinical utility of computed tomography-guided core needle biopsyin the diagnostic re-evaluation of patients with lymphoproliferativedisorders and suspected disease progression. Ann Oncol 14:1438–1441
16. Vandervelde C, Kamani T, Varghese A, Ramesar K, Grace R,Howlett DC (2008) A study to evaluate the efficacy of image-guided core biopsy in the diagnosis and management of lymphoma—results in 103 biopsies. Eur J Radiol 66:107–111
17. Sklair-Levy M, Amir G, Spectre G, Lebensart P, Applbaum Y, AgidR, Lieberman S, Ben-Yehuda D, ShermanY, Libson E (2005) Image-guided cutting-edge-needle biopsy of peripheral lymph nodes andsuperficial masses for the diagnosis of lymphoma. J Comput AssistTomogr 29:369–372
18. Demharter J, Neukirchen S, Wagner T, Schlimok G, Bohndorf K,Kirchhof K (2007) Do ultrasound-guided core needle biopsies oflymph nodes allow for subclassification of malignant lymphomas?RöFo 179:396–400
19. De Kerviler E, de Bazelaire C, Mounier N, Mathieu O, Brethon B,Brière J, Marolleau JP, Brice P, Gisselbrecht C, Frija J (2007) Image-guided core-needle biopsy of peripheral lymph nodes allows thediagnosis of lymphomas. Eur Radiol 17:843–849
20. Shaw JHF, Rumball EM (1990) Complications and local recurrencefollowing lymphadenectomy. Br J Surg 77:760–764
21. Sklair-LevyM, Polliack A, Shaham D, ApplbaumYH, Gillis S, Ben-Yehuda D, Sherman Y, Libson E (2000) CT-guided core-needlebiopsy in the diagnosis of mediastinal lymphoma. Eur J Radiol 10:714–718
22. Priola AM, Priola SM, Cataldi A, Ferrero B, Garofalo G, Errico L,Marci V, Fava C (2008) Biopsia percutanea transtoracica TC-guidatanella diagnosi degli espansi del mediastino: valutazione di 73 proce-dure. Radiol Med 113:3–15
23. Caraway NP (2005) Strategies to diagnose lymphoproliferative dis-orders by fine-needle aspiration by using ancillary studies. Cancer105:432–442
24. Stattaus J, Kalkmann J, Kuehl H, Metz KA, Nowrousian MR,Forsting M, Ladd SC (2008) Diagnostic yield of computedtomography-guided coaxial core biopsy of undetermined masses inthe free retroperitoneal space: single-center experience. CardiovascIntervent Radiol 31:919–925
25. Gazelle GS, Haaga JR, Rowland DY (1992) Effect of needle gauge,level of anticoagulation, and target organ on bleeding associated withaspiration biopsy. Work in progress. Radiology 183:509–513
26. Agid R, Sklair-Levy M, Bloom AI, Lieberman S, Polliack A, Ben-Yehuda D, Sherman Y, Libson E (2003) CT-guided biopsy withcutting-edge needle for the diagnosis of malignant lymphoma: expe-rience of 267 biopsies. Clin Radiol 58:143–147
27. Li L, Wu QL, Liu LZ, Mo YX, Xie CM, Zheng L, Chen L, Wu PH(2005) Value of CT-guided core-needle biopsy in diagnosis andclassification of malignant lymphomas using automated biopsygun. World J Gastroenterol 11:4843–4847
28. Pappa VI, Hussain HK, Reznek RH, Whelan J, Norton AJ, WilsonAM, Love S, Lister TA, Rohatiner AZ (1996) Role of image-guidedcore-needle biopsy in the management of patients with lymphoma. JClin Oncol 14:2427–2430
29. Silverman SG, Lee BY, Mueller PR, Cibas ES, Seltzer SE (1994)Impact of positive findings at image-guided biopsy of lymphoma onpatient care: evaluation of clinical history, needle size, and pathologicfindings on biopsy performance. Radiology 190:759–764
30. Loubeyre P, McKee TA, Copercini M, Rosset A, Dietrich PY (2009)Diagnostic precision of image-guided multisampling core needlebiopsy of suspected lymphomas in a primary care hospital. Br JCancer 100:1771–1776
31. Pfeiffer J, Kayser G, Ridder GJ (2009) Sonography-assisted cuttingneedle biopsy in head and neck for the diagnosis of lymphoma: can itreplace lymph node extirpation? Laryngoscope 119:689–695
32. Zinzani PL, Colecchia A, Festi D, Magagnoli M, Larocca A, AscaniS, Bendandi M, Fraternali Orcioni G, Gherlinzoni F, Albertini P,Pileri SA, Roda E, Tura S (1998) Ultrasound-guided core-needlebiopsy is effective in the initial diagnosis of lymphoma patients.Haematologica 83:989–992
Ann Hematol