Embed Size (px)
Citation preview

CTO Crossing Based on Cap Morphology
J.A. Mustapha, MD, FACC, FSCAI Director of Cardiovascular Catheterization Laboratories
Director of Endovascular Interventions Director of Cardiovascular Research Metro Health Hospital, Wyoming, MI
Clinical Assistant Professor of Medicine Michigan State University COM, E. Lansing, MI

Disclosure • Abbott Vascular - Consultant, Speaker, Medical Advisory Board • Bard Peripheral Vascular - Research, Consultant, Medical Advisory Board,
Speaker, Trainer • Bayer - Medical Advisory Board • Biotronik - Research • Boston Scientific - Speaker, Consultant • Cardiovascular Systems, Inc. - Research, Consultant, Speaker, Trainer • Cook Medical - Research, Consulting, Speaker, Trainer • Cordis - Consultant, Trainer • Medtronic - Consulting, Speaker, Trainer • Terumo - Consulting, Speaker, Trainer • Trireme – Research • Spectranetics – Research, Consulting

Variation in the Use of Lower Extremity Vascular Procedures forCritical Limb Ischemia
Philip P. Goodney, MD, MS1,2, Lori L. Travis, MS6, Brahmajee K. Nallamothu, MD, MPH3,Kerianne Holman, MD, MPH3, Bjoern Suckow, MD5, Peter K. Henke, MD4, F. Lee Lucas,PhD6, David C. Goodman, MS, MD2, John D. Birkmeyer, MD4, and Elliott S. Fisher, MD,MPH2
1Section of Vascular Surgery, Dartmouth-Hitchcock Medical Center, Lebanon2Dartmouth-Hitchcock Medical Center, The Dartmouth Institute for Health Policy and ClinicalPractice, Hanover NH3Center for Health Outcomes and Policy, The University of Michigan, Ann Arbor, MI4The Section of Vascular Surgery, The University of Michigan, Ann Arbor, MI5The Section of Vascular Surgery, University of Utah, Salt Lake City, UT6Center for Outcomes Research and Evaluation, Maine Medical Center, Portland, ME
AbstractBackground—Many believe that variation in vascular practice may affect limb salvage rates inpatients with severe PAD. However, the extent of variation in procedural vascular care obtainedby patients with critical limb ischemia (CLI) remains unknown.
Methods and Results—Using Medicare 2003–2006, we identified all patients with CLI whounderwent major lower extremity amputation in the 306 hospital referral regions (HRRs)described in the Dartmouth Atlas of Healthcare. For each patient, we studied the use of lowerextremity vascular procedures (open surgery or endovascular intervention) in the year prior toamputation. Our main outcome measure was the intensity of vascular care, defined as theproportion of patients in the HRR undergoing vascular procedure in the year before amputation.Overall, 20,464 patients with CLI underwent major lower extremity amputations during the studyperiod, and collectively underwent 25,800 vascular procedures in the year prior to undergoingamputation. However, these procedures were not distributed evenly − 54% of patients had novascular procedures performed in the year prior to amputation, 14% underwent 1 vascularprocedure, and 21% underwent more than one vascular procedure. In the regions in the lowestquintile of vascular intensity, vascular procedures were performed in 32% of patients. Conversely,in the regions in the highest quintile of vascular intensity, revascularization was performed in 58%of patients in the year prior to amputation (p<0.0001). In analyses accounting for differences inage, sex, race, and comorbidities, patients in high intensity regions were 2.4 times as likely toundergo revascularization in the year prior to amputation than patients in low intensity regions(adjusted OR=2.4, 95% CI 2.1–2.6, p<0.001).
Conclusions—Significant variation exists in the intensity of vascular care provided to patientsin the year prior to major amputation. In some regions, patients receive intensive care, while in
Correspondence: Philip P. Goodney, MD, Dartmouth-Hitchcock Medical Center, 1 Medical Center Drive, Lebanon, NH 03766.,Telephone 603-650-4682, Fax 603-650-4973, [email protected] at the Society for Vascular Surgery’s Annual Meeting, June 15th, 2011.Conflict of Interest Disclosures: None
NIH Public AccessAuthor ManuscriptCirc Cardiovasc Qual Outcomes. Author manuscript; available in PMC 2013 January 1.
Published in final edited form as:Circ Cardiovasc Qual Outcomes. 2012 January 1; 5(1): 94–102. doi:10.1161/CIRCOUTCOMES.111.962233.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH-PA Author ManuscriptNIH-PA Author ManuscriptNIH-PA Author Manuscript
Goodney et al.
Page 18
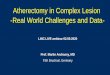
Table 3
Ten most common open and endovascular CPT codes performed in the year prior to amputation
Endovascular Interventions
CPT Code Description n*percent of all CPTs
(n=25,800)
36200 Catheter placement aorta, from groin or arm 3791 14.7
36246 Abdominal, pelvic, or lower extremity arteriography, 2nd order selective 3469 13.5
36247 Abdominal, pelvic, or lower extremity arteriography, 3nd order selective 3271 12.7
36245 Abdominal, pelvic, or lower extremity arteriography, 1st order selective 2055 8.0
35474 Transluminal balloon angioplasty, percutaneous;femoral-popliteal 2015 7.8
37205 Transcatheter placement of an intravascular stent(s), (except coronary, carotid, and vertebral vessel), percutaneous; initial vessel 1850 7.2
35470 Transluminal balloon angioplasty, percutaneous; tibioperoneal trunk or branches, each vessel 894 3.5
35473 Transluminal balloon angioplasty, percutaneous;iliac 532 2.1
37206 Transcatheter placement of an intravascular stent(s), (except coronary, carotid, and vertebral vessel), percutaneous;each additionalvessel
473 1.8
36248 Abdominal, pelvic, or lower extremity arteriography, Additional order selective 444 1.7
Open Surgical Procedures
CPT Code Description n* percent of all CPTs
35656 Bypass graft, with other than vein;femoral-popliteal 854 3.3
35566 Bypass graft, with vein;femoral-anterior tibial, posterior tibial, peroneal artery 762 3.0
35666 Bypass graft, with other than vein;femoral-anterior tibial, posterior tibial, or peroneal artery 526 2.0
35571 Bypass graft, with vein;popliteal-tibial, -peroneal artery or other distal vessels 454 1.8
35585 In-situ vein bypass;femoral-anterior tibial, posterior tibial, or peroneal artery 443 1.7
35371 Thromboendarterectomy, including patch graft, if performed;common femoral 408 1.6
35556 Bypass graft, with vein;femoral-popliteal 405 1.6
35372 Thromboendarterectomy, including patch graft, if performed;deep (profunda) femoral 232 0.9
35661 Bypass graft, with other than vein;femoral-femoral 196 0.8
35681 Bypass graft; composite, prosthetic and vein 180 0.7
*The “n” represented here is the total number of procedures performed, which is greater than the total number of unique patients undergoing vascular procedures (n=9,349). Further details regarding
patients who underwent more than one (or more than one type) of vascular procedure number are shown in Figures 1 and 2.
Circ C
ardiovasc Qual O
utcomes. A
uthor manuscript; available in PM
C 2013 January 1.

Current Evidence
• The Peripheral Registry of Endovascular Clinical Outcomes (PRIME Registry) is an ongoing multi-center CLI registry
• Started enrolling patients in 2013. • Target to obtain data from 15 centers in the US and
international, evaluating patients with advanced PVD and CLI
• The registry covers all aspects of patient care including patient evaluation, treatment modality and clinical follow up

Tibio-Pedal Access Outcomes
• N = 300 patients • Ultrasound utilized 100% for access

Cook Tibio-Pedal Registry Planned Enrollment
– 200 patients at up to 12 US and European sites Patient population
– Patient has an infrainguinal artery occlusion – Previous attempts to cross the occlusion from an antegrade approach have been
unsuccessful (unless institutional standard of care permits primary retrograde access)
– All techniques to be used for access, lesion crossing, lesion treatment, and vessel closure are at the investigator’s discretion according to institutional standard of care
Data collected include: – Procedural information, access site and lesion characteristics, procedural times,
treatments used, and closure methods – Procedural complications and complications occurring within 30 days following
the procedure
Walker et al. NCVH 2014

Cook Tibio-Pedal Registry • Enrollment period May 2012 - July 2013
• Final enrollment: 199 patients from 8 US and 3 European sites
PI (Site) Patients Enrolled Jihad Mustapha (Metro Heart & Vascular Institute) 50
George L. Adams (Rex Health) 31
Nelson Bernardo (Washington Hospital Center) 26
Andrej Schmidt (Park Hospital Leipzig) 24
Aravinda Nanjundappa (West Virginia University) 16
Robert Beasley (Mount Sinai) 11
Craig Walker (Cardiovascular Institute of the South) 11
Yazan Khatib (First Coast Cardiovascular Institute) 11
Thomas Zeller (Universitäts-Herzzentrum Bad Krozingen) 9
Marco Manzi (Casa Di Cura Abano Terme) 7
Luis Leon (Tucson Medical Center) 3
Total 199
Walker et al. NCVH 2014

Adverse Outcomes
Event Type
Local pain at access site 2.5% (5/199)
Infection at access site 1.0% (2/199)
Bruising at access site 1.0% (2/199)*
Bleeding at access site 1.0% (2/199)
Acute vessel dissection 0.5% (1/199)
Acute vessel thrombosis 0% (0/199)
Compartment syndrome 0% (0/199)
Urgent surgical revascularization 0% (0/199)
• Low (< 3%) complication rate for all events associated with vascular access site
Walker et al. NCVH 2014

Advantage of Retrograde Tibial Access
Increase success rate of crossing
Shorten treated segment
Preserve options of therapy: surgery, atherectomy
Utilize hibernating lumen
Preserve tibial vessels flow

Tibio-Pedal Access Clinical Consideration
• Critical Limb Ischemia patients • Patients with Long CTOs • Patients with CTO reconstitution
with the P2/3 segment of the popliteal artery
• Patients with CTO reconstitution within the tibial vessels
• Patients with hostile groin access (fibrotic, obese, prior surgery)
• Patients unable to lay flat (back pain, COPD, CHF)
Anatomical Consideration
• Adequate tibial reconstitution (usually distal third)
• Patients with adequate anterior and posterior communicating circulation
• Patients with distal CTO caps that are concave in retrograde fashion

Tibio- Pedal Access
Relative Contraindications
• Claudication with single vessel runoff • Patients with complete occlusion of tibial vessels. White stop sign • Inability to insert a sheath • Indolence to anticoagulation or vasodilators

CTO Cap Morphology PRIME Analysis
• Concave • Convex • Acoustic shadowing • Branching and collaterals

Chronic Total Occlusion Crossing Approach based on the
Plaque Cap Appearance. The C-TOP Trial • Retrospective analysis evaluating CTO
CAP morphology. • Interim analysis of patients enrolled in the
PRIME registry with CTOs • Prevalence of different CTO caps • Access selection, technique and success
rate of crossing

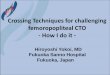
Proposed C-TOP Classification



!
!
CTO!
CTO!!Lenghth!
Intermed!iate!
5K10!cm!
Start!with!CTO!crossing!device!
Consider!catheter!and!wire!
Long!>!10!cm!
CTO!Cap!analysis!
Type!I!
CFA!access!
High!likelihood!of!crossing!
Start!CTO!crossing!Device!
Change!to!catheter!/wire!if!difSicult!to!cross!
Type!II!
SFA!Reconstiution!proximal!P1!
CFA!access!Consider!Popliteal/
Tibial!
less!likely!to!cross!in!antegrade!or!
retrograde!fashion!
CTO!Crossing!device!
Catheter/Wire!if!failed,!reKentry!device!
Popliteal/Tibial!reconstitution!
Combined!antegrade/Retrograde!Access!
CTO!crossing!device!!from!antegrade!and!
retrograde!(Tunneling)!
Catheter!and!wire,!antegrade/retrograde!
(Tunneling)!
Type!III! !!
Antegrade/Retrograde!access!
High!likelohood!of!subKintimal!croosing!
Consider!CTO!crossing!device!!
catheter/Wire!technique!
Advanced!techniques!CART!ReKback!
Type!IV!
Consider!starting!with!Tibial/popliteal!access!Priority!for!retrograde!
crossing!
Low!proSile!CTO!crossing!device!
Cather/Wire!technique!(0.018!
catheter)!
Short!<5!cm!
Catheter!and!wire!technique!
Pending publication

CTO Crossing tools….


Clinical Scenario
• 67 year old male presented with a 2 week hx rest pain. Ulcer involving the tip of R toe.
• Risk factors include HTN, DM, HLP and smoking
• Non compressible ABIs

Cap Analysis – Planning an Intervention


C-TOP Classification

Proximal Cap Analysis

Distal CTO Cap

Options of Therapy
1. Retrograde or Antegrade Access, attempt Crossing to the tibials
2. Antegrade and Retrograde Access? 3. Retrograde Access Only?

Antegrade US Guided Access

Antegrade Crossing Attempt




US Guided Pedal Access


Retrograde Access



Final Result

Clinical Scenario
• 53 year old male that presented with a non healing ulcer of the Left foot, involves AT and PT distribution
• Applying the C-TOP algorithm…..

Retrograde Access

Distal CTO Cap

Choose Appropriate access
Low profile CTO crossing device
Mechanical activation, less
operator dependency
Less concern with retrograde dissection and perforation

Confirm Position After Crossing

Final Result

Advanced Techniques
• Re-constitution of the CTO within the popliteal artery will require the operator experience in guiding re-entry
• Retrograde access in long CTO will guarantee no loss of relatively healthy conduits

Re-Back Technique
• Re-entry using ante grade outback and retrograde balloon
• Utilized if antegrade and retrograde wires/catheters are in two different sub-intimal planes

Case Demonstration
• 72 year old male • Rutherford Class III - advanced
claudication • 2 attempts for revascularization 1 year
prior • Hx CABG • No adequate venous conduits


Superior control with antegrade
access

- Type III CTO - Longer than 10 cm - High likelihood of subintimal crossing - Re-entry may occur beyond re-
constitution - Retrograde access will preserve
relatively normal segments



Wire advanced into the balloon
Balloon pulled distally
Wire advanced from one sub-intimal space to another
Deliver treatment from true
lumen to true lumen

Operator can switch from CTO device to wire and catheter, but not the opposite
Wire and catheter technique in experienced hands
CTO crossing device for antegrade access, low profile
CTO Crossing Device if CTO cap is favorable
Determine Access Points
Define CTO Caps CTO length

Conclusion
• CTOs remain a challenging and difficult arena to treat
• Operators should be comfortable with a device to utilize in crossing CTOs especially with tibial disease
• Crossing a CTO requires a detailed analysis to determine access point, strategy and device required

Thank You
J.A. Mustapha, MD, FACC, FSCAI Director of Cardiovascular Catheterization Laboratories
Director of Endovascular Interventions Director of Cardiovascular Research Metro Health Hospital, Wyoming, MI
Clinical Assistant Professor of Medicine Michigan State University, E. Lansing, MI