Embed Size (px)
Citation preview

Introduction
In 1986, Cumming et al. first described a fetus with anunusual pattern of multiple congenital anomalies in-cluding campomelia, cervical lymphocele, polysplenia,short gut, and polycystic kidneys, pancreas, and liver[1]. Urioste et al. subsequently reported two additionalfetuses with similar findings [2]. Ming et al. recentlyreported another fetus with Cumming syndrome, alsoªexpanding the phenotypeº [3]. Based on parental con-sanguinity and occurrence in siblings, an autosomal re-cessive pattern of inheritance has been proposed.
We report two unrelated cases with a similar patternof multiple congenital anomalies consisting of limb
shortening, long bone angulation, and cervical lympho-cele. Case 1 had the additional finding of cystic renaldysplasia; multiple cardiac defects were found in case2. We believe that these two cases possibly representfurther examples of Cumming syndrome.
Case reports
Case 1
A female fetus was delivered at 28 weeks' gestation to a 35-year-oldG1P0 woman. Prenatal ultrasound had revealed polyhydramnios,severe micromelia, foot deformities, cystic kidneys, and a smallbell-shaped chest. The pregnancy was electively terminated. At au-
Kurt M. DibbernJohn M. GrahamRalph S. LachmanWilliam R.Wilcox
Cumming Syndrome:report of two additional cases
Received/accepted: 6 May 1998
This study was supported in part bya USPHS NIH program project grant(HD 22657)
K.M. Dibbern × J. M. Graham ×R. S. Lachman × W.R. WilcoxDepartment of Medical Genetics andPediatrics, Cedars-Sinai Medical Center,University of California, Los Angeles,Los Angeles, California, USA
K.M. Dibbern × R. S. LachmanDepartment of Radiology,Harbor-UCLA Medical Center,Torrance, California, USA
R.S. Lachman ())International Skeletal Dysplasia Registry,444 South San Vicente Blvd., Suite 1001,Los Angeles, CA 90048, USA
Abstract We present two unrelat-ed cases with a similar pattern ofmultiple congenital anomalies in-cluding limb shortening, long boneangulation, and cervical lympho-cele. We believe these cases to rep-resent additional examples of asyndrome first described by Cum-ming et al. (1986), and by Uriosteet al. (1991) and Ming et al. (1997).
Pediatr Radiol (1998) 28: 798±801Ó Springer-Verlag 1998
topsy, the fetus weighed 1030 g (50%) and measured 30 cm (±2 SD)in length. There was a large cervical lymphocele, multiple renal pa-renchymal cysts, and cystic dilatation of the calyceal system and pel-vis of the right kidney. No other visceral abnormalities were noted.
Case 2
A female fetus was delivered at 21 weeks' gestation to a 30-year-old G2P1 Filipino woman in good health. An ultrasound examina-tion performed at 17 weeks' gestation demonstrated a large cystichygroma, mild hydrocephalus, marked limb shortening, and severe
799
a
b c
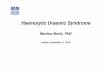
Fig.1a±c Case 1. a Lateral skull radiograph reveals midface hypo-plasia and slightly decreased skull ossification, with a large soft-tis-sue nuchal mass. b AP film of torso and extremities showselongated handlebar clavicles with a small thorax, 12 ribs, hypo-plastic scapulae, small vertebral bodies, tall hypoplastic iliac wings,no ischial or pubic ossification, femoral, tibial and ulnar bending,Bowdler-like spurs of the ulnae and generalized long-bone short-ening. c Lateral film of the spine and extremities reveals hypoplas-tic slightly flat vertebral bodies with coronal clefts at the thoraco-lumbar junctional area, short ribs, posteriorly angled femoral dia-physes, and significant fibular hypoplasia
Table 1 Summary of findings in 6 cases of Cumming syndrome
Cumming [1] Urioste case 1 [2] Urioste case 2 [2] Present case 1 Present case 2 Ming [3]
Sex M F F F F FGestational age 27 weeks Term 37 weeks 30 weeks 20 weeks 23weeksCystic hygroma + + + + + ?Cleft palate + ± ± + ± ±Cleft lip ± ± + ± ± +Short limbs + + + + + +Bowed femurs + ? + + + +Hypoplastic fibulae + ? ? + + ±Posteriorly angulated femurs ? ? ? + + +Small thorax + + + + + +Hypoplastic scapulae ± ± ± + + ±Syndactyly ± + + ± ± ±Polycystic liver + + + ± ± ±Polycystic/multicystic kidneys + + + + ± +Polycystic pancreas + ± + ± ± ±Intestinal anomalies + ± ± ± ± +Polysplenia + ± ± ± ± +Arrhinencephaly + ± ± ? ± ±Cardiac anomalies ± ± ± ± + +
hydrops. Amniocentesis revealed a normal 46,XY karyotype. Thepregnancy was terminated electively.
The fetus weighed 301 g and had a crown-heel measurement of20 cm. There was midface hypoplasia, micrognathia, cleft palate,short limbs with campomelia, upper and lower extremity pterygia,and a small, tapered thorax. At autopsy, multiple cardiac abnor-malities, including a ventricular septal defect, double-outlet rightventricle, and coarctation of the aorta, were noted.
Results
Radiologic findings
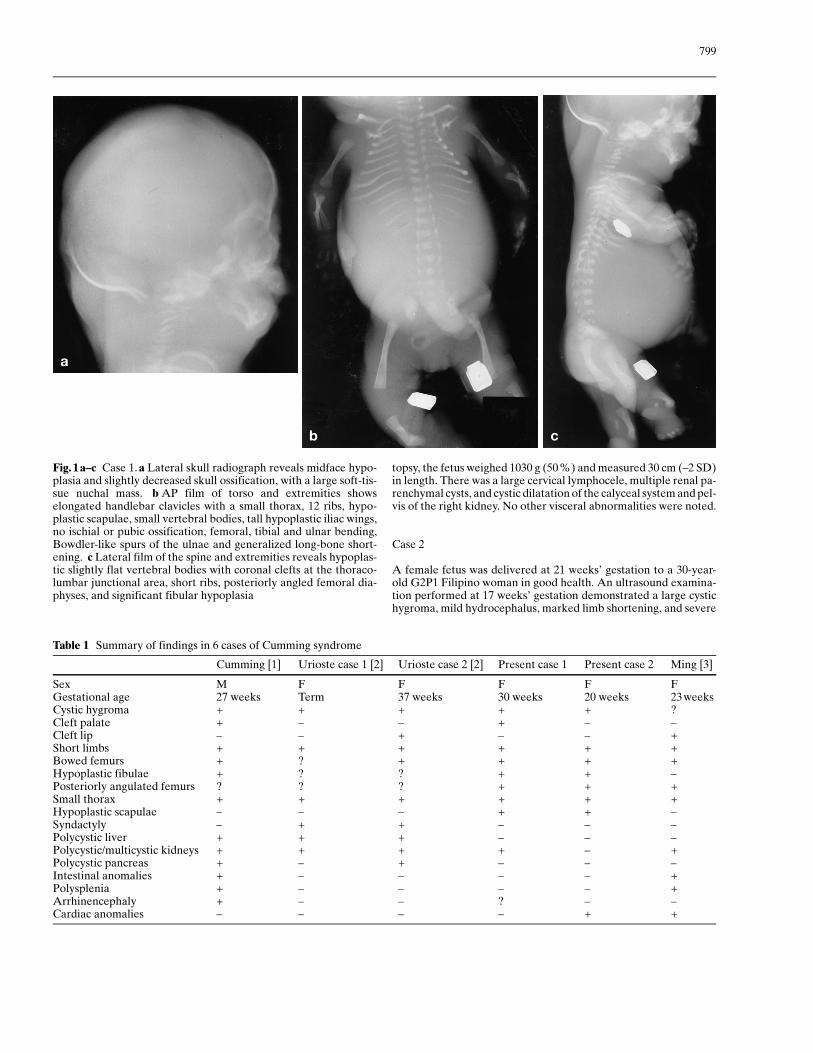
Radiographs of case 1 (Fig. 1) showed generalized ex-tremity shortening with upper- and lower-extremitymesomelia, hypoplastic scapulae, Bowdler-like spur ab-normality of the ulnae (and perhaps the tibiae), hypo-plastic vertebral bodies with coronal clefts, midfacehypoplasia, a bell-shaped chest, elongated handlebarclavicles, tall hypoplastic iliac wings, unusual posteriorangulation of the femurs, and fibular hypoplasia. Radio-graphs of case 2 (Fig.2) revealed micromelia, campom-elia, a small, tapered thorax, microcephaly, midfacehypoplasia with micrognathia, hypoplastic vertebrae
(without coronal clefts), tall hypoplastic iliac wings,tiny fibulae, and posteriorly angulated femurs. Radio-graphically, both cases are quite similar.
Chondro-osseous morphology
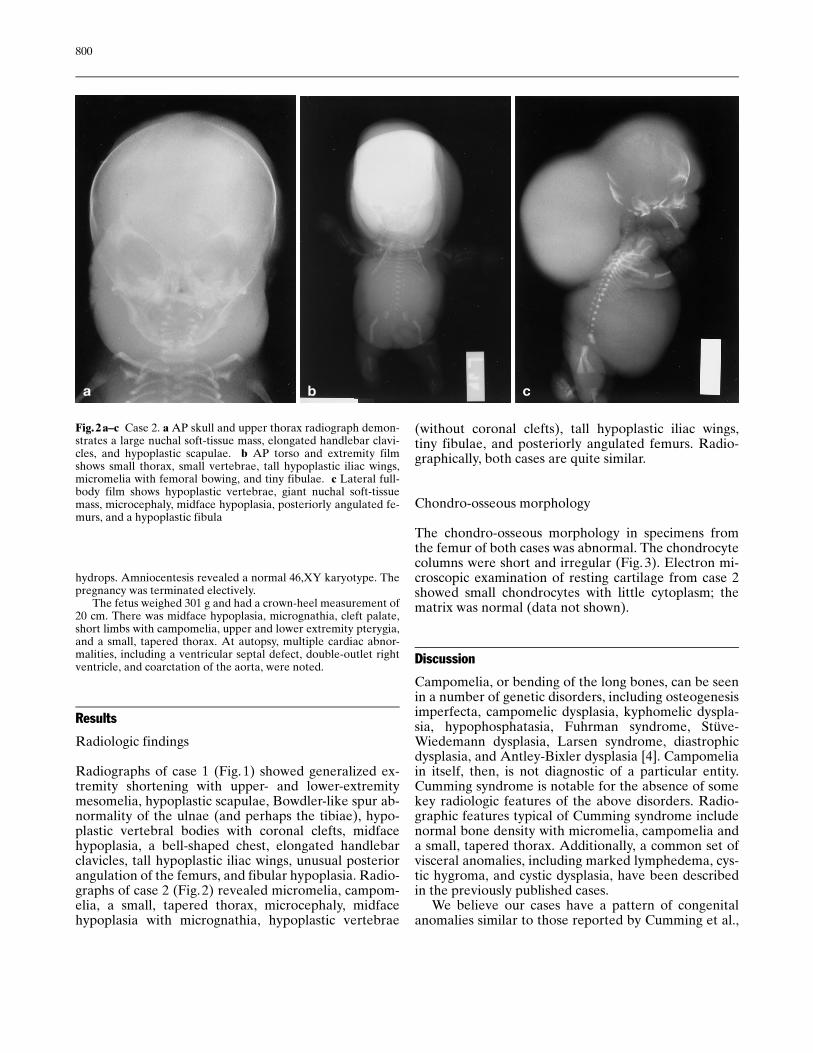
The chondro-osseous morphology in specimens fromthe femur of both cases was abnormal. The chondrocytecolumns were short and irregular (Fig. 3). Electron mi-croscopic examination of resting cartilage from case 2showed small chondrocytes with little cytoplasm; thematrix was normal (data not shown).
Discussion
Campomelia, or bending of the long bones, can be seenin a number of genetic disorders, including osteogenesisimperfecta, campomelic dysplasia, kyphomelic dyspla-sia, hypophosphatasia, Fuhrman syndrome, Stüve-Wiedemann dysplasia, Larsen syndrome, diastrophicdysplasia, and Antley-Bixler dysplasia [4]. Campomeliain itself, then, is not diagnostic of a particular entity.Cumming syndrome is notable for the absence of somekey radiologic features of the above disorders. Radio-graphic features typical of Cumming syndrome includenormal bone density with micromelia, campomelia anda small, tapered thorax. Additionally, a common set ofvisceral anomalies, including marked lymphedema, cys-tic hygroma, and cystic dysplasia, have been describedin the previously published cases.
We believe our cases have a pattern of congenitalanomalies similar to those reported by Cumming et al.,
800
a b c
Fig.2a±c Case 2. a AP skull and upper thorax radiograph demon-strates a large nuchal soft-tissue mass, elongated handlebar clavi-cles, and hypoplastic scapulae. b AP torso and extremity filmshows small thorax, small vertebrae, tall hypoplastic iliac wings,micromelia with femoral bowing, and tiny fibulae. c Lateral full-body film shows hypoplastic vertebrae, giant nuchal soft-tissuemass, microcephaly, midface hypoplasia, posteriorly angulated fe-murs, and a hypoplastic fibula
Urioste et al.,and Ming et al. In addition to the previous-ly described radiographic features of Cumming syn-drome, our cases had the additional skeletal findings ofmidface hypoplasia, hypoplastic scapulae, Bowdler-likespur abnormality of the ulnae (and perhaps the tibiae),small fibulae, and hypoplastic vertebral bodies with afew coronal clefts. Our second case had very similar ra-diographic findings and a cleft palate, but no coronalclefts nor Bowdler-like spurs (Table 1).
In spite of the Bowdler-like spurs, case 1 had no otherfeatures of perinatal lethal or infantile hypophosphata-sia. Renal cystic dysplasia, described previously [1±3],was also noted in our first patient. Only one of the previ-ously reported patients had a cardiac malformation, aswas seen in our second patient. Neither of our patientshad polycystic dysplasia of the liver or pancreas, poly-splenia, cecal atresia, arrhinencephaly, shortening of thesmall and large bowel [1], or accessory thyroid tissue [2].Given the small number of reported cases, the absence
of these anomalies and the finding of significant congeni-tal heart disease in our second patient may represent vari-ability in the clinical phenotype of Cumming syndrome.
Although the hypoplastic scapulae, iliac wing chan-ges, and midface hypoplasia are features of campomelicdysplasia, the large cystic hygroma, and cystic renal dis-ease are not features of that disorder. Hydronephrosisalone has been described in campomelic dysplasia [4].The femoral angulation in campomelic dysplasia is notposterior. Therefore, this combination of defects doesnot suggest campomelic dysplasia, but the possibility ofanother SOX-9 molecular defect in our cases of Cum-ming syndrome. A determination of SOX-9 gene abnor-mality was performed in the patient reported by Minget al., with a negative result.
Acknowledgements We would like to thank David Rimoin, M.D,Ph.D for his valuable comments and MaryAnne Priore for her helpin organizing the data on these cases.
801
a b
Fig.3 Chondro-osseous mor-phology. a Case 1 Femur, vonKossa trichrome stain, 10X.(Note the short and irregularchondrocyte columns). b Case2 Femur, von Kossa trichromestain, 10X. (Note the short andirregular chondrocyte columns)
References
1. Cumming W, Ohlsson A, Ali A (1986)Campomelia, cervical lymphocele,polycystic dysplasia, short gut, poly-splenia. Am J Med Gen 25: 783±790
2. Urioste M, Arroyo A, Martinez-FriasM (1991) Campomelia, polycystic dys-plasia, and cervical lymphoceles in twosibs. Am J Med Gen 41: 475±477
3. Ming JE, McDonald-McGinn DM,Markowitz RI, Ruchelli E, Zackai EH(1997) Heterotaxia in a fetus with cam-pomelia, cervical lymphocele, polysple-nia, and multicystic dysplastic kidneys:expanding the phenotype of Cummingsyndrome. Am J Med Gen 73: 419±424
4. Taybi H, Lachman RS (1996) Radiolo-gy of syndromes, metabolic disorders,and skeletal dysplasias, 4th edn. Mosby,St. Louis