Embed Size (px)
Citation preview
ORIGINAL ARTICLE – HEPATOBILIARY TUMORS
Cure Model Survival Analysis After Hepatic Resectionfor Colorectal Liver Metastases
Alessando Cucchetti, MD1, Alessandro Ferrero, MD, PhD2, Matteo Cescon, MD, PhD1, Matteo Donadon, MD3,
Nadia Russolillo, MD2, Giorgio Ercolani, MD1, Giacomo Stacchini, MD1, Federico Mazzotti, MD1, Guido Torzilli,
MD, PhD3, and Antonio Daniele Pinna, MD, PhD1
1Department of Medical and Surgical Sciences, S. Orsola-Malpighi Hospital, Alma Mater Studiorum - University of
Bologna, Bologna, Italy; 2Department of General and Oncological Surgery, Ospedale Mauriziano Umberto I, Turin, Italy;3Department of Hepatobiliary Surgery, Humanitas Research Hospital, School of Medicine - University of Milan, Milan,
Italy
ABSTRACT
Background. Statistical cure is achieved when a patient
population has the same mortality as cancer-free individ-
uals; however, data regarding the probability of cure after
hepatectomy of colorectal liver metastases (CLM) have
never been provided. We aimed to assess the probability of
being statistically cured from CLM by hepatic resection.
Methods. Data from 1,012 consecutive patients undergo-
ing curative resection for CLM (2001–2012) were used to
fit a nonmixture cure model to compare mortality after
surgery to that expected for the general population matched
by sex and age.
Results. The 5- and 10-year disease-free survival was 18.9
and 15.8 %; the corresponding overall survival was 44.3
and 32.7 %. In the entire study population, the probability
of being cured from CLM was 20 % (95 % confidence
interval 16.5–23.5). After the first year, the mortality
excess of resected patients, in comparison to the general
population, starts to decline until it approaches zero 6 years
after surgery. After 6.48 years, patients alive without tumor
recurrence can be considered cured with 99 % certainty.
Multivariate analysis showed that cure probabilities range
from 40.9 % in patients with node-negative primary tumors
and metachronous presentation of a single lesion \3 cm, to
1.5 % in patients with node positivity, and synchronous
presentation of multiple, large CLMs. A model for the
calculation of a cure fraction for each possible clinical
scenario is provided.
Conclusions. Using a cure model, the present results
indicate that statistical cure of CLM is possible after hep-
atectomy; providing this information can help clinicians
give more precise answer to patients’ questions.
Colorectal cancer is a major cause of mortality
throughout the world.1, 2 At the time of the initial diag-
nosis, 20–25 % of patients will have clinically detectable
colorectal liver metastases (CLM), and an additional
40–50 % of patients will develop liver metastases after
resection of the primary tumor; approximately 20–30 % of
these patients will have the liver as the exclusive site of
disease.3,4 These latter patients could be considered as
having an organ-specific confined disease, so that hepatic
resection can be viewed as a potentially curative treat-
ment.4 Recently published literature suggests that long-
term survival can be achieved, with a 10-year survival rate
ranging from 17 to 28 %, but whether resected patients can
be considered cured is currently unknown.4,5 In epidemi-
ology, and as endorsed by the United States National
Cancer Institute, cure is said to occur when the mortality of
patients, treated for a specific disease, returns to the same
level as that of the general population; these patients can be
considered statistically cured from the specific disease
because they are just as likely to die as a member of the
general population.6–8 Cure rate models represent survival
models incorporating a cure fraction. They assume that a
proportion of subjects exists who will never die as a
Electronic supplementary material The online version of thisarticle (doi:10.1245/s10434-014-4234-0) contains supplementarymaterial, which is available to authorized users.
� Society of Surgical Oncology 2014
First Received: 30 July 2014
M. Cescon, MD, PhD
e-mail: [email protected]
Ann Surg Oncol
DOI 10.1245/s10434-014-4234-0
consequence of the specific disease that has been treated.
Survival after specific treatment can be considered as the
sum of a fraction of patients who have mortality similar to
that expected in the general population and who can be
considered cured of their disease, and that of patients who
are bound to die after being treated.6–8 The cure fraction
can provide a useful measure of the probability of success
of a therapeutic approach; however, this aspect, that is
survival incorporating a cure fraction, has never been
properly investigated in the setting of CLM. The main aim
of the present study was to assess the probability of being
cured from CLM by hepatic resection using a cure-rate
model.
METHODS
Study Population
Between January 2001 and December 2012, 1130 con-
secutive patients undergoing first curative resection (R0)
for CLM without extrahepatic disease were identified at
three Italian tertiary referral hospitals; 118 patients were
excluded because of incomplete clinical data. The study
population finally consisted of 1,012 patients: 507 were
from the Ospedale Mauriziano Umberto I, Turin; 348 were
from the S. Orsola-Malpighi Hospital, Bologna; and 157
were from the Istituto Clinico Humanitas, Rozzano, Milan.
Patients were deemed to have resectable disease in the
presence of an adequate performance status if the metas-
tases could be completely resected and if the future
remnant liver volume would be adequate. Standard
demographic and clinical data were collected for each
patient. The number, size, and distribution of the hepatic
metastases were recorded as well as the extension of the
hepatectomy, according to the International Hepato-Biliary
Association nomenclature.9 Primary tumor stage, presen-
tation of CLM (synchronous vs. metachronous), time
elapsed from the resection of the primary tumor to clinical
evidence of metastases [disease-free survival (DFS) from
colon surgery], and the adoption of adjuvant therapy, with
respect to the hepatic surgery, were also detailed. The
chemotherapy strategy was prescribed by the oncologist in
charge. The follow-up included clinical examination, esti-
mation of serum carcinoembryonic antigen level, and
computed tomography or magnetic resonance imaging at 3,
6, and/or every 12 months, as indicated by the oncologist
in charge and on the basis of the clinical course. The fol-
low-up was carried out by assessing the records of the
respective institutions regarding laboratory, interventional,
and pathologic data, and by telephone contact directly with
the patient, or alternatively with the referring clinician for
patients residing in regions distant from hospitals.
Cure Fraction Model
Mathematical details of the cure model are provided in
the Supplementary Materials. The first requirement for the
application of the cure model is the statistical plausibility
of cure.10 This means that cure time should occur within a
reasonable time frame so as to ensure that a cure is plau-
sible within the patient’s lifetime. If a proportion of
patients who are not expected to die of disease exists in the
study population, the Kaplan–Meier survival curve will
tend to a plateau on the y-axis (Fig. 1).7 In the present
analysis, we used DFS after hepatic resection as the pri-
mary survival measure for the cure model. We decided to
use DFS instead of disease-specific survival (which is
calculated from the time of surgery until cancer-related
death) because this latter measure does not take into
account, as events, patients who are alive with recurrence,
and it is not correct to define these patients as cured of their
disease.4,5,11 For the same reason, overall survival was used
as secondary survival measure for completeness of results.
DFS was calculated from the time of the hepatectomy until
clinical evidence of recurrence or patient death. The
mathematical model applied here is the nonmixture cure
fraction model that was chosen because it has a background
in modeling of tumor recurrence.12,13,17 The estimations of
expected survival of the general population (the compara-
tor used for cure fraction calculation) at the time of patient
event (death or recurrence) were derived from population
survival tables obtained from the Italian National Institute
of Statistics, matched by age and sex.14 Details regarding
statistical analysis are reported in the Supplementary
Materials.
0
0.2
.4.6
.81
2 4
Disease-free Overall
6
Years
Surv
ival
8 10 12
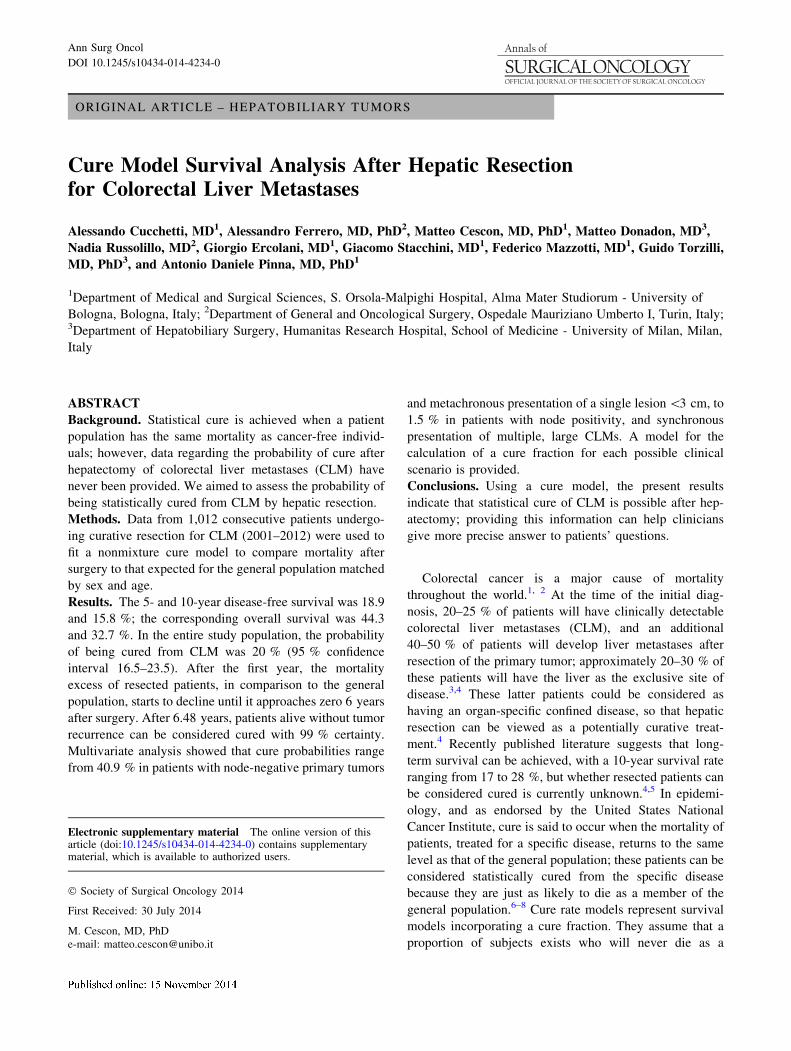
FIG. 1 Overall and disease-free survival (DFS) of 1,012 consecutive
patients who underwent resection for colorectal liver metastases
(CLM) (gray areas represent 95 % confidence intervals). As can be
noted, DFS curve tends to flatten at end of fourth year after resection,
confirming that the cure hypothesis can be accepted 7
N. A. Cucchetti et al.
RESULTS
Baseline characteristics of the study population (1,012
patients) are detailed in Table 1. Within a median follow-
up of 47.8 months (range, 1 day to 12 years), 618 patients
(61.1 %) experienced tumor recurrence, and 374 patients
(37.0 %) died. The 30- and 90-day postoperative death
rates were 0.3 and 1.0 %, respectively. The 3-, 5-, and
10-year DFS rates were 26.0, 18.9, and 15.8 %, respec-
tively, and the corresponding overall survival rates were
62.1, 44.3, and 32.7 % (Fig. 1). Tumor recurrence was
only intrahepatic in 284 patients, both intra- and extrahe-
patic in 121, and extrahepatic only in 195 patients (data not
available for 18 patients). Tumor progression accounted for
77.2 % of the causes of death. Relationships between
clinical variables are detailed in the Supplementary
Materials.
The cure model converged for the entire study popula-
tion and for each subgroup analyzed (p \ 0.001 in all
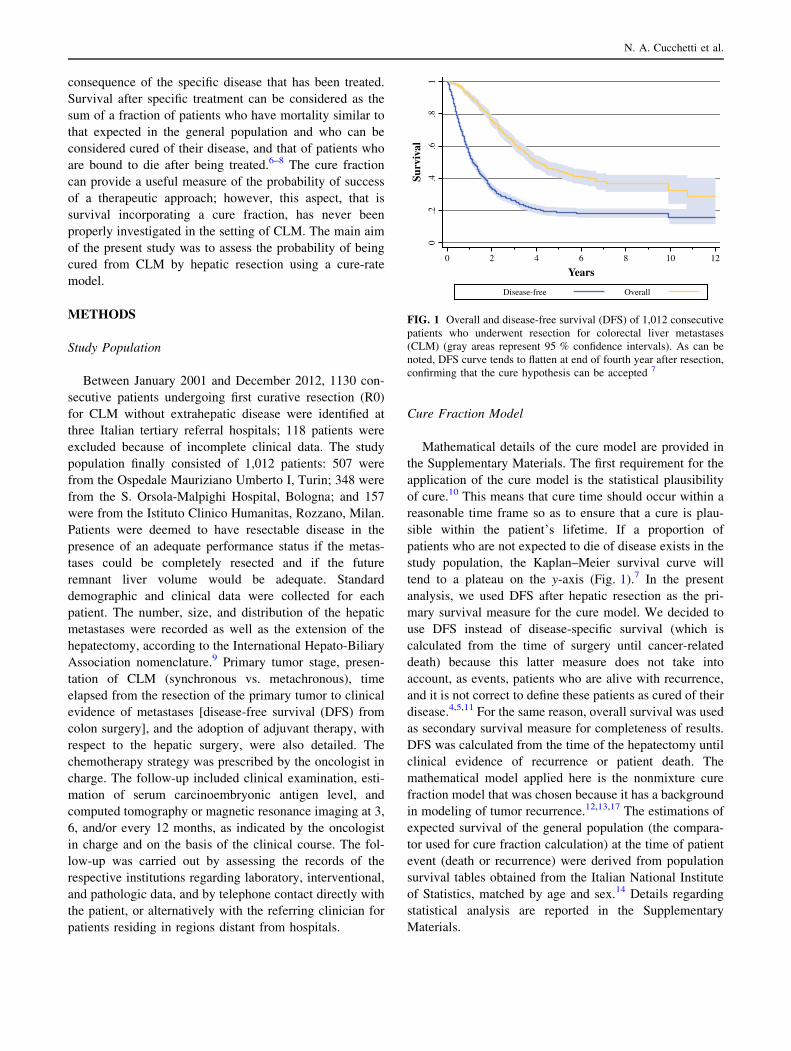
cases). In the entire study population, the probability of
being cured from CLM by hepatic resection was 20 %
(95 % confidence interval 16.5–23.5), and the median
survival of uncured patients was 0.9 years (Fig. 2a). The
excess of hazard after surgery is plotted in Fig. 2b and
starts from a 25 % increased risk of death early after
resection with respect to the general population. In the first
postoperative year, the excess of hazard increased to
approximately 60 % in the entire group and up to 90 % in
uncured patients. At the end of the first year after surgery,
the hazard of uncured patients progressively increased over
TABLE 1 Baseline characteristics of the study population used for
cure fraction estimation
Variable All patients
(n = 1,012)
Age, year, median (IQR) 63 (56–70)
Age C 60 year 650 (64.2 %)
Male sex 619 (61.2 %)
Primary tumor T stage
T1 12 (1.2 %)
T2 91 (9.0 %)
T3 763 (75.4 %)
T4 146 (14.4 %)
Primary tumor nodal status
N0 312 (30.8 %)
N1 444 (43.9 %)
N2 256 (25.3 %)
Synchronous presentation 537 (53.1 %)
Disease-free interval from colon surgery C 24 month 226 (22.3 %)
Largest tumor size, median (IQR) 3.2 (2.0–5.0)
\3 cm 413 (40.8 %)
3–5 cm 386 (38.1 %)
[5 cm 213 (21.1 %)
No. of liver metastases
1 408 (40.3 %)
2 195 (19.3 %)
3 125 (12.4 %)
C4 284 (28.1 %)
Adjuvant chemotherapy (n = 830) 641 (77.2 %)
Extension of hepatectomy
Single or multiple wedges 443 (43.8 %)
Segmentectomy with or without wedges 103 (10.2 %)
Bisegmentectomy with or without wedges 168 (16.6 %)
Major hepatectomy with or without wedges 298 (29.4 %)
Any postoperative complications (Dindo [ 1) 330 (32.6 %)
IQR interquartile range (25th–75th percentiles)
0
0.5
11.
50
.2.4
.6.8
1
2 4
Whole group Uncured patients
6
Years
Exc
ess
haza
rd r
ate
Rel
ativ
e su
rviv
al
8 10 12
0 2 4 6
Years
A
B
8 10 12
FIG. 2 Cure model results. a Relative survival of entire group of
patients and uncured patients. In entire group, from sixth year after
surgery onward, survival curve reaches plateau at 20 %, which
represents cure fraction. b Excess hazard rate of entire study group
and of uncured patients. At end of the first year after surgery, excess
of hazard starts to decrease until it approaches zero at end of 6 years
after surgery. Conversely, in uncured patients, excess of hazard
progressively increases over time
Statistical Cure for Colorectal Liver Metastases
time, whereas the entire group showed a progressive
reduction until it approached zero. The excess of hazard in
the entire group decreased until a 99 % level of confidence
in the general population at 6.48 years after hepatic
resection, indicating that after this time point, a patient
alive without tumor recurrence could be considered cured
with 99 % certainty. Considering overall survival, instead
of DFS, as a survival measure, the death rate after surgery
for CLM equals the death rate of the general population in
41.8 % of cases (95 % confidence interval 35.4–48.2) with
a median survival of remaining patients of 2.5 years.
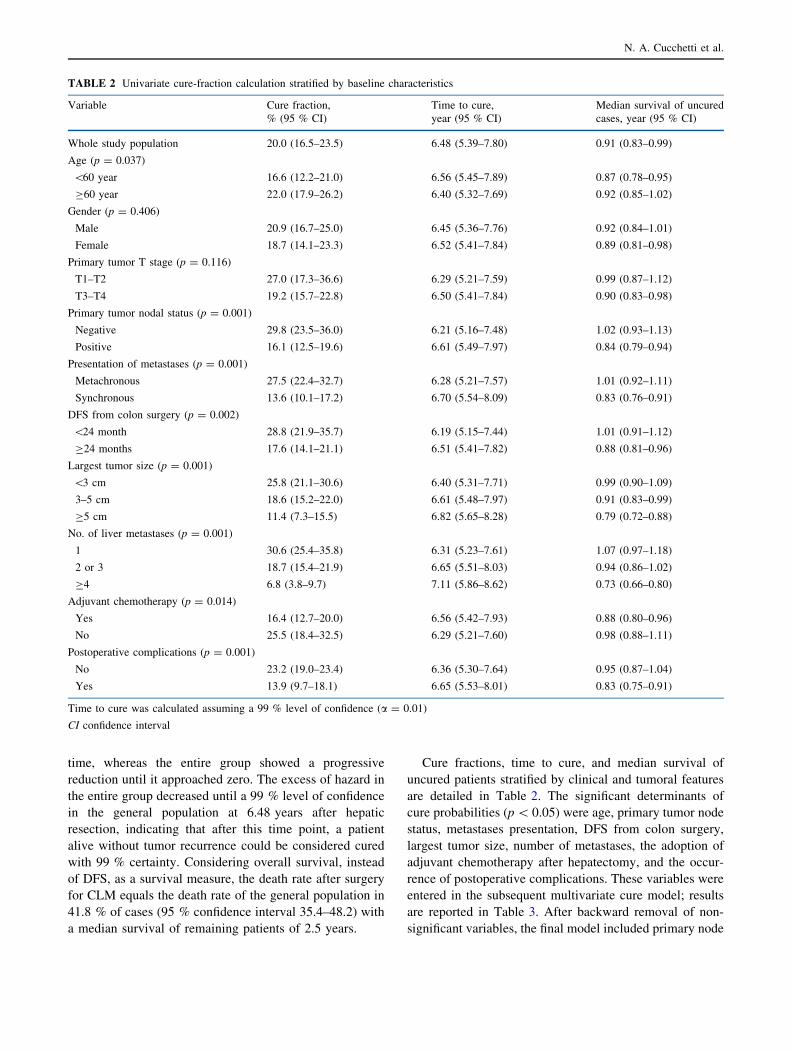
Cure fractions, time to cure, and median survival of
uncured patients stratified by clinical and tumoral features
are detailed in Table 2. The significant determinants of
cure probabilities (p \ 0.05) were age, primary tumor node
status, metastases presentation, DFS from colon surgery,
largest tumor size, number of metastases, the adoption of
adjuvant chemotherapy after hepatectomy, and the occur-
rence of postoperative complications. These variables were
entered in the subsequent multivariate cure model; results
are reported in Table 3. After backward removal of non-
significant variables, the final model included primary node
TABLE 2 Univariate cure-fraction calculation stratified by baseline characteristics
Variable Cure fraction,
% (95 % CI)
Time to cure,
year (95 % CI)
Median survival of uncured
cases, year (95 % CI)
Whole study population 20.0 (16.5–23.5) 6.48 (5.39–7.80) 0.91 (0.83–0.99)
Age (p = 0.037)
\60 year 16.6 (12.2–21.0) 6.56 (5.45–7.89) 0.87 (0.78–0.95)
C60 year 22.0 (17.9–26.2) 6.40 (5.32–7.69) 0.92 (0.85–1.02)
Gender (p = 0.406)
Male 20.9 (16.7–25.0) 6.45 (5.36–7.76) 0.92 (0.84–1.01)
Female 18.7 (14.1–23.3) 6.52 (5.41–7.84) 0.89 (0.81–0.98)
Primary tumor T stage (p = 0.116)
T1–T2 27.0 (17.3–36.6) 6.29 (5.21–7.59) 0.99 (0.87–1.12)
T3–T4 19.2 (15.7–22.8) 6.50 (5.41–7.84) 0.90 (0.83–0.98)
Primary tumor nodal status (p = 0.001)
Negative 29.8 (23.5–36.0) 6.21 (5.16–7.48) 1.02 (0.93–1.13)
Positive 16.1 (12.5–19.6) 6.61 (5.49–7.97) 0.84 (0.79–0.94)
Presentation of metastases (p = 0.001)
Metachronous 27.5 (22.4–32.7) 6.28 (5.21–7.57) 1.01 (0.92–1.11)
Synchronous 13.6 (10.1–17.2) 6.70 (5.54–8.09) 0.83 (0.76–0.91)
DFS from colon surgery (p = 0.002)
\24 month 28.8 (21.9–35.7) 6.19 (5.15–7.44) 1.01 (0.91–1.12)
C24 months 17.6 (14.1–21.1) 6.51 (5.41–7.82) 0.88 (0.81–0.96)
Largest tumor size (p = 0.001)
\3 cm 25.8 (21.1–30.6) 6.40 (5.31–7.71) 0.99 (0.90–1.09)
3–5 cm 18.6 (15.2–22.0) 6.61 (5.48–7.97) 0.91 (0.83–0.99)
C5 cm 11.4 (7.3–15.5) 6.82 (5.65–8.28) 0.79 (0.72–0.88)
No. of liver metastases (p = 0.001)
1 30.6 (25.4–35.8) 6.31 (5.23–7.61) 1.07 (0.97–1.18)
2 or 3 18.7 (15.4–21.9) 6.65 (5.51–8.03) 0.94 (0.86–1.02)
C4 6.8 (3.8–9.7) 7.11 (5.86–8.62) 0.73 (0.66–0.80)
Adjuvant chemotherapy (p = 0.014)
Yes 16.4 (12.7–20.0) 6.56 (5.42–7.93) 0.88 (0.80–0.96)
No 25.5 (18.4–32.5) 6.29 (5.21–7.60) 0.98 (0.88–1.11)
Postoperative complications (p = 0.001)
No 23.2 (19.0–23.4) 6.36 (5.30–7.64) 0.95 (0.87–1.04)
Yes 13.9 (9.7–18.1) 6.65 (5.53–8.01) 0.83 (0.75–0.91)
Time to cure was calculated assuming a 99 % level of confidence (a = 0.01)
CI confidence interval
N. A. Cucchetti et al.
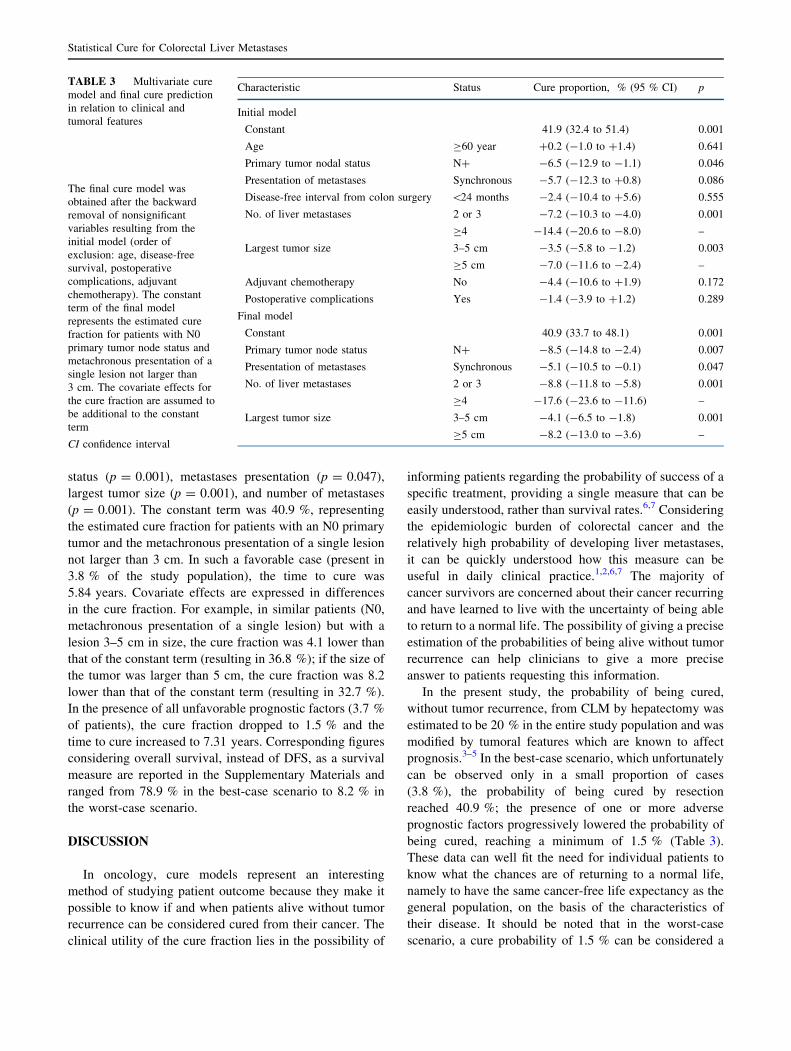
status (p = 0.001), metastases presentation (p = 0.047),
largest tumor size (p = 0.001), and number of metastases
(p = 0.001). The constant term was 40.9 %, representing
the estimated cure fraction for patients with an N0 primary
tumor and the metachronous presentation of a single lesion
not larger than 3 cm. In such a favorable case (present in
3.8 % of the study population), the time to cure was
5.84 years. Covariate effects are expressed in differences
in the cure fraction. For example, in similar patients (N0,
metachronous presentation of a single lesion) but with a
lesion 3–5 cm in size, the cure fraction was 4.1 lower than
that of the constant term (resulting in 36.8 %); if the size of
the tumor was larger than 5 cm, the cure fraction was 8.2
lower than that of the constant term (resulting in 32.7 %).
In the presence of all unfavorable prognostic factors (3.7 %
of patients), the cure fraction dropped to 1.5 % and the
time to cure increased to 7.31 years. Corresponding figures
considering overall survival, instead of DFS, as a survival
measure are reported in the Supplementary Materials and
ranged from 78.9 % in the best-case scenario to 8.2 % in
the worst-case scenario.
DISCUSSION
In oncology, cure models represent an interesting
method of studying patient outcome because they make it
possible to know if and when patients alive without tumor
recurrence can be considered cured from their cancer. The
clinical utility of the cure fraction lies in the possibility of
informing patients regarding the probability of success of a
specific treatment, providing a single measure that can be
easily understood, rather than survival rates.6,7 Considering
the epidemiologic burden of colorectal cancer and the
relatively high probability of developing liver metastases,
it can be quickly understood how this measure can be
useful in daily clinical practice.1,2,6,7 The majority of
cancer survivors are concerned about their cancer recurring
and have learned to live with the uncertainty of being able
to return to a normal life. The possibility of giving a precise
estimation of the probabilities of being alive without tumor
recurrence can help clinicians to give a more precise
answer to patients requesting this information.
In the present study, the probability of being cured,
without tumor recurrence, from CLM by hepatectomy was
estimated to be 20 % in the entire study population and was
modified by tumoral features which are known to affect
prognosis.3–5 In the best-case scenario, which unfortunately
can be observed only in a small proportion of cases
(3.8 %), the probability of being cured by resection
reached 40.9 %; the presence of one or more adverse
prognostic factors progressively lowered the probability of
being cured, reaching a minimum of 1.5 % (Table 3).
These data can well fit the need for individual patients to
know what the chances are of returning to a normal life,
namely to have the same cancer-free life expectancy as the
general population, on the basis of the characteristics of
their disease. It should be noted that in the worst-case
scenario, a cure probability of 1.5 % can be considered a
TABLE 3 Multivariate cure
model and final cure prediction
in relation to clinical and
tumoral features
The final cure model was
obtained after the backward
removal of nonsignificant
variables resulting from the
initial model (order of
exclusion: age, disease-free
survival, postoperative
complications, adjuvant
chemotherapy). The constant
term of the final model
represents the estimated cure
fraction for patients with N0
primary tumor node status and
metachronous presentation of a
single lesion not larger than
3 cm. The covariate effects for
the cure fraction are assumed to
be additional to the constant
term
CI confidence interval
Characteristic Status Cure proportion, % (95 % CI) p
Initial model
Constant 41.9 (32.4 to 51.4) 0.001
Age C60 year ?0.2 (-1.0 to ?1.4) 0.641
Primary tumor nodal status N? -6.5 (-12.9 to -1.1) 0.046
Presentation of metastases Synchronous -5.7 (-12.3 to ?0.8) 0.086
Disease-free interval from colon surgery \24 months -2.4 (-10.4 to ?5.6) 0.555
No. of liver metastases 2 or 3 -7.2 (-10.3 to -4.0) 0.001
C4 -14.4 (-20.6 to -8.0) –
Largest tumor size 3–5 cm -3.5 (-5.8 to -1.2) 0.003
C5 cm -7.0 (-11.6 to -2.4) –
Adjuvant chemotherapy No -4.4 (-10.6 to ?1.9) 0.172
Postoperative complications Yes -1.4 (-3.9 to ?1.2) 0.289
Final model
Constant 40.9 (33.7 to 48.1) 0.001
Primary tumor node status N? -8.5 (-14.8 to -2.4) 0.007
Presentation of metastases Synchronous -5.1 (-10.5 to -0.1) 0.047
No. of liver metastases 2 or 3 -8.8 (-11.8 to -5.8) 0.001
C4 -17.6 (-23.6 to -11.6) –
Largest tumor size 3–5 cm -4.1 (-6.5 to -1.8) 0.001
C5 cm -8.2 (-13.0 to -3.6) –
Statistical Cure for Colorectal Liver Metastases

poor outcome; nevertheless, even in this infrequent unfa-
vorable scenario (3.7 %), surgery probably remains the
only chance for radical treatment. In addition, the consid-
erable difference observed between DFS and overall
survival (Fig. 1) and the observed equipoise of the death
rate after CLM surgery to the death rate of the general
population of 41.8 %, support the possibility of long-term
survival even in the case of tumor recurrence after hepa-
tectomy by both repeated hepatic surgery and the adoption
of efficient chemotherapeutic strategies, thus providing
further hope to patients in search of a return to a normal
life.15,16
The present results can give a clearer idea of the like-
lihood of the success of the surgery to oncologists and can
better define the appropriate therapeutic strategy. To our
knowledge, few reports have analyzed the cure rate of liver
cancers, and they do not distinguish among specific histo-
logic types or type of therapy adopted. From population-
based estimations, the cure fraction for liver cancer was
found to be about 10 %.17,18 The difference between pre-
vious results and the results presented here is probably the
consequence of the proportion of patients with other liver
cancers (such as hepatocellular carcinoma) that have an
unfavorable outcome with respect to resectable CLMs in
the population-based estimations. The present report is thus
the first to give an estimation of the cure fraction of CLM.
On the basis of a large multicenter experience involving
three high-volume hospitals with low postoperative mor-
tality, an up-to-date chemotherapy approach, and good
long-term survival, the present results seem reliable.
Together with the probability of being cured, patients
may also want to know when they will be considered cured.
In the past, some attempts have been made to answer this
question. Surgical series have suggested that patients who
survive 10 years after surgery appear to be cured of their
disease on the basis of a disease-specific probability of
death of approximately 1 %, but these results only indi-
rectly support the possibility of achieving a cure.4,5 To be
fair, the cure fraction should be determined by comparing
the DFS of treated people against a matched control group
who have never had the disease.11 Considering disease-
specific survival as an outcome measure, as in previous
reports, patients who are alive with recurrence are con-
sidered to be cured just the same. This observation is also
pertinent if overall survival is considered as a temporal end
point. From a formal statistical point of view, the term of
comparison can be survival of the general population that is
inevitably affected by age-specific causes of death
(including, for example, other cancer types). However, we
chose to use DFS to provide unequivocal information for
patients. In fact, it can be difficult for patients to understand
that they can be considered cured, even with tumor
recurrence after surgery, only because there are other
persons in the general population that are currently dying
from other diseases. In the present study, these aspects
were considered and accomplished by considering DFS as
an end point and by analyzing relative survival using the
cure model. Results from the present analysis suggest that
if there is a cure, it will be achieved earlier than 10 years
after hepatic surgery. In fact, the excess hazard rate
increases quickly in the first year after surgery (Fig. 2b) as
a consequence of both postoperative and early recurrence,
which leads to a very unfavorable outcome, but after the
first year, it starts to decline until it approaches zero from
the sixth year after surgery onward.19 More precisely, in
the entire study group, a patient alive without tumor
recurrence will be considered cured, with 99 % certainty,
between 5.84 and 7.31 years, depending on tumoral fea-
tures. That is, the more advanced the tumor stage, the
longer the time needed to achieve the cure. This is an
important aspect to consider when communicating with
patients who have been free of recurrence for a long time
and who would like to know when they will be able to
breathe a sigh of relief. Regarding this temporal aspect, it
can be pointed out that a not negligible proportion of
patients, in the present analysis, would be censored before
reaching this temporal end point. This aspect has already
been evaluated in specific modeling studies, suggesting that
a certain threshold is required before the statistical cure
rate can be estimated.20 For liver cancer, this threshold was
estimated to be 3.7 years. As can be noted from Fig. 1, at
this temporal end point, confidence intervals of curves are
quite narrow, supporting the fact that most patient survivals
were still not right censored. Thus, assumptions at the basis
of the cure model application can be reasonably considered
to be fulfilled.
Some other results from the present study deserve more
discussion. In particular, no benefit from adjuvant chemo-
therapy after hepatectomy was observed; instead, it seems
that adjuvant chemotherapy provided a lower cure fraction
(Table 2). This paradoxical aspect is explained by the more
advanced tumor sizes at the time of the colonic and hepatic
surgery of the patients who received adjuvant chemother-
apy (Supplementary Materials). This observation is
reinforced by the multivariate cure model, which excluded
adjuvant chemotherapy as an independent prognostic factor
in reaching a cure. The pivotal role of adjuvant chemo-
therapy is not under examination in the present analysis,
especially in view of the rapid progress observed in the
field over the past decade; however, to correctly estimate
its benefit in achieving a statistical cure, dedicated, well-
matched studies are needed.3,16
In conclusion, the present study provides a statistical
measure useful in the assessment of the success that can be
expected from the hepatic resection of CLM. The cure
fraction can be of interest for clinicians and, in particular,
N. A. Cucchetti et al.

for patients who would like to be fully informed regarding
what awaits them after hepatic surgery.
ACKNOWLEDGMENT This work is dedicated to the memory of
Prof. Lorenzo Capussotti.
DISCLOSURE The authors declare no conflict of interest.
REFERENCES
1. Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA
Cancer J Clin. 2011;61:69–90.
2. US Cancer Statistics Working Group. United States cancer sta-
tistics: 1999–2010 incidence and mortality Web-based report.
Atlanta, GA: US Department of Health and Human Services,
Centers for Disease Control and Prevention and National Cancer
Institute; 2013. Available at: http://www.cdc.gov/uscs. Accessed
1 Feb 2014.
3. Garden OJ, Rees M, Poston GJ, et al. Guidelines for resection of
colorectal cancer liver metastases. Gut. 2006;55(Suppl 3):iii1–8.
4. Tomlinson JS, Jarnagin WR, DeMatteo RP, et al. Actual 10-year
survival after resection of colorectal liver metastases defines cure.
J Clin Oncol. 2007;25:4575–80.
5. Pulitano C, Castillo F, Aldrighetti L, et al. What defines ‘‘cure’’
after liver resection for colorectal metastases? Results after
10 years of follow-up. HPB (Oxford). 2010;12:244–9.
6. Statistical Methodology and Applications Branch, Data Modeling
Branch, National Cancer Institute. Cansurv, version 1.1. Available at:
http://surveillance.cancer.gov/cansurv/index.html. Accessed 1 Feb
2014.
7. Othus M, Barlogie B, Leblanc ML, et al. Cure models as a useful
statistical tool for analyzing survival. Clin Cancer Res. 2012;18:
3731–6.
8. Lambert PC, Thompson JR, Weston CL, et al. Estimating and
modeling the cure fraction in population-based cancer survival
analysis. Biostatistics. 2007;8:576–94.
9. Terminology Committee of the IHPBA. The Brisbane 2000 ter-
minology of liver anatomy and resections. Abingdon: Taylor &
Francis; 2000. p. 333–9.
10. Smoll NR, Schaller K, Gautschi OP. The cure fraction of glio-
blastoma multiforme. Neuroepidemiology. 2012;39:63–9.
11. Fuller AF, Griffiths CT. Gynecologic oncology. Amsterdam:
Wolters Kluwer; 1983.
12. Lambert PC. Modeling of the cure fraction in survival studies.
Stata J. 2007;3:1–25.
13. Tsodikov AD, Ibrahim JG, Yakovlev AY. Estimating cure rates
from survival data: an alternative to two-component mixture
models. J Am Stat Assoc. 2003;98:1063–78.
14. Italian population life tables. Available at: http://demo.istat.it/.
Accessed 1 Dec 2013.
15. Adam R, Bismuth H, Castaing D, et al. Repeat hepatectomy for
colorectal liver metastases. Ann Surg. 1997;225:51–60.
16. Adam R, De Gramont A, Figueras J, et al. The oncosurgery
approach to managing liver metastases from colorectal cancer: a
multidisciplinary international consensus. Oncologist. 2012;
17:1225–39.
17. Cvancarova M, Aagnes B, Fossa SD, et al. Proportion cured
models applied to 23 cancer sites in Norway. Int J Cancer.
2013;132:1700–10.
18. Dal Maso L, Guzzinati S, Buzzoni C, et al. Long-term survival,
prevalence, and cure of cancer: a population-based estimation for
818,902 Italian patients and 26 cancer types. Ann Oncol. 2014;
25:2251-60.
19. Vigano L, Capussotti L, Lapointe R, et al. Early recurrence after
liver resection for colorectal metastases: risk factors, prognosis,
and treatment. A LiverMetSurvey-based study of 6,025 patients.
Ann Surg Oncol. 2014;21(4):1276–1286.
20. Tai P, Yu E, Cserni G, et al. Minimum follow-up time required
for the estimation of statistical cure of cancer patients: verifica-
tion using data from 42 cancer sites in the SEER database. BMC
Cancer. 2005;5:48.
Statistical Cure for Colorectal Liver Metastases