Embed Size (px)
Citation preview

Current and Future Trends inCurrent and Future Trends in HIV Therapy HIV Therapy
Hail M. Al-AbdelyHail M. Al-AbdelyConsultant, Infectious DiseasesConsultant, Infectious Diseases

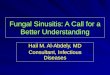
CD4 Cell Count
Virus in Plasma
Symptoms
Detectable VIRUS IN PLASMA Detectable
> 500 cells CD4 COUNTS < 200 cells
Seroconversion Asymptomatic AIDSTime 0 12 Years
Infection Death
Clinical, Virological and Immunological Course of HIV Infection
0
200
400
600
800
1000
RNA in Plasma

HIVinfection
J. Coffin, XI International Conf. on AIDS, Vancouver, 1996
Development of AIDS is like an Development of AIDS is like an impending train wreckimpending train wreck
Viral Load = Speed of the train Viral Load = Speed of the train CD4 count = Distance from cliffCD4 count = Distance from cliff

T1/2 ~5.7 hrs
Productively infectedCD4 lymphocytes
Latently infectedCD4 lymphocytes
HIV
Uninfected CD4 lymphocytes
Uninfected activatedCD4 lymphocytes
Long-lived cell populations
2.6 daysper generation
99%T 1/2 ~1.6d
<1%
Viral Dynamics of HIV-1 Infection
Perelson et.al. Science 271:1582 (1996)Perelson et.al. Science 271:1582 (1996)
CD4 lymphocytes infected with defective virus
1%

Latency TheoryLatency Theory

261
15

Nucleoside Reverse Transcriptase Nucleoside Reverse Transcriptase Inhibitors (NRTIs)Inhibitors (NRTIs)
Abacavir (Ziagen)
Abacavir + Lamivudine (Epzicom)
Abacavir+Lamivudine+Zidovudine (Trizivir)
Didanosine (Videx, ddI)
Emtricitabine (Emtriva, FTC)
Emtricitabine + Tenofovir DF (Truvada)
Lamivudine (Epivir, 3TC)
Lamivudine+Zidovudine (Combivir)
Stavudine (Zerit, d4T)
Tenofovir DF (Viread)
Zalcitabine (Hivid, ddC)
Zidovudine (Retrovir, AZT, ZDV)
Nonnucleoside Reverse Transcriptase Nonnucleoside Reverse Transcriptase InhibitorsInhibitors (NNRTIs)(NNRTIs)
Delavirdine (Rescriptor)
Efavirenz (Sustiva)
Nevirapine (Viramune)
Protease Inhibitors (PIs)Protease Inhibitors (PIs)
Amprenavir (Agenerase)
Atazanavir (Reyataz)
Fosamprenavir (Lexiva, 908)
Indinavir (Crixivan)
Lopinavir+Ritonavir (Kaletra)
Nelfinavir (Viracept)
Ritonavir (Norvir)
Saquinavir (Fortovase, Invirase)
Tipranavir
Fusion InhibitorsFusion Inhibitors
Enfuvirtide (Fuzeon, T-20)
Total = 25 drug or Total = 25 drug or drug combinationsdrug combinations

RT
Provirus
ProteinsRNA
RNA
RT
Viral protease
Reversetranscriptase
RNA
RNA
DNA
DNA
DNA
Current antiretroviral targets
ZDV, ddI,ddC, d4T,3TC, ABC,
DLV, NVP,EFV
SQVRTVIDVNFVAPVLPV

50
60
70
80
90
Monot herapy
50
60
70
80
90
Mon
othe
rapy
20
40
60
80
100
Mon
othe
rapy
MonotherapyMonotherapy Dual therapyDual therapy Triple therapyTriple therapy
Viral Suppression with Monotherapy Viral Suppression with Monotherapy versus Multiple Drugsversus Multiple Drugs




Hospitalization Days for AIDS Patients
Ho
spit
aliz
atio
n d
ays
(n)
2,000
1,500
1,000
500
0
1993
/2
1994
/1
1994
/2
1995
/1
1995
/2
1996
/1
1996
/2
1997
/1
1997
/2
1998
/1
1998
/2
1999
/1
1999
/2
2000
/1
2000
/2
2001
/1

Highly active antiretroviral therapy has Highly active antiretroviral therapy has Changed our view toward HIV from Changed our view toward HIV from inevitably fatalinevitably fatal (Cancer) (Cancer)to a to a manageable disease manageable disease (Diabetes, HTN)(Diabetes, HTN)
Good News

1.1. Incomplete responseIncomplete response
2.2. Adherence & Complexity of treatmentAdherence & Complexity of treatment
3.3. Short and long term side effectsShort and long term side effects
4.4. ResistanceResistance
5.5. Drug-drug interactionsDrug-drug interactions
Bad News

Bad News
1.1. Incomplete responseIncomplete response• Complete RNA suppression and sustained CD4
increase happens only in 60-80%.• Effectiveness is even lower in patients with high
replication rates and extensive antiretroviral experience.
2. Adherence & Complexity of treatmentAdherence & Complexity of treatment3. Short and long term side effectsShort and long term side effects4. ResistanceResistance5. Drug-drug interactionsDrug-drug interactions

50
60
70
80
90
Monot herapy
50
60
70
80
90
Mon
othe
rapy 20
40
60
80
100
Monot herapy
MonotherapyMonotherapy Dual therapyDual therapy Triple therapyTriple therapy
Viral Suppression with Monotherapy Viral Suppression with Monotherapy versus Multiple Drugsversus Multiple Drugs

1. Incomplete responseIncomplete response
2.2. Adherence & Complexity of treatmentAdherence & Complexity of treatment• Too many tablets.Too many tablets.
• Difficult schedule.Difficult schedule.
• Food factorFood factor
3. Short and long term side effectsShort and long term side effects
4. ResistanceResistance
5. Drug-drug interactionsDrug-drug interactions
Bad News

Predictors of Inadequate Adherence
• Regimen complexity and pill burden• Poor clinician-patient relationship• Active drug use or alcoholism • Unstable housing• Mental illness (especially depression)• Lack of patient education • Medication adverse effects• Fear of medication adverse effects

1. Incomplete responseIncomplete response
2. Complexity of treatmentComplexity of treatment
3.3. Short and long term side effectsShort and long term side effects4. Drug-drug interactions Drug-drug interactions
5. ResistanceResistance
Bad News

Metabolic Complications of PIs
• Hyperbilirubinemia
• Hyperlipidemia– Coronary artery disease
• Insulin resistance
• Abnormal fat distribution.
• Lipodystrophy

From NEJM

Risk: Benefit Analysis ofRisk: Benefit Analysis of Coronary Heart Disease and HAART Coronary Heart Disease and HAART
Average Average calculated calculated increase in increase in
CHD events = CHD events = 0.14% per year0.14% per year
RisksRisks
BenefitsBenefits
Mortality Mortality rates in HIV-rates in HIV-
infected infected patients by patients by
50%50%
Adapted from Grunfeld. 6th CROI; 1999; Chicago. Palella. NEJM 1998;338:853.

1. Incomplete responseIncomplete response
2. Complexity of treatmentComplexity of treatment
3. Short and long term side effectsShort and long term side effects
4.4. Drug-drug interactionsDrug-drug interactions
5. ResistanceResistance
Bad News

Drug Category Indinavir Ritonavir Saquinavir Nelfinavir Amprenavir Nevirapine Delavirdine Efavirenz
Ca++ channel blocker
(none) bepridil (none) (none) bepridil (none) (none) (none)
Cardiac (none) amioderoneflecainidepropafenonequinidine
(none) (none) (none) (none) (none) (none)
Lipid LoweringAgents
simvastatinlovastatin
simvastatinlovastatin
simvastatinlovastatin
simvastatinlovastatin
simvastatinlovastatin
(none) simvastatinlovastatin
(none)
Anti-Mycobacterial
rifampin none rifampinrifabutin
rifampin rifampin (none) rifampinrifabutin
(none)
Antihistamine astemizoleterfenadine
astemizoleterfenadine
astemizoleterfenadine
astemizoleterfenadine
astemizoleterfenadine
(none) astemizoleterfenadine
astemizoleterfenadine
GastrointestinalDrugs
cisapride cisapride cisapride cisapride cisapride (none) cisaprideH-2 blockersProton pumpinhibitors
cisapride
Neuroleptic (none) clozapine pimozide
(none) (none) (none) (none) (none) (none)
Psychotropic midazolamtriazolam
midazolamtriazolam
midazolamtriazolam
midazolamtriazolam
midazolamtriazolam
(none) midazolamtriazolam
midazolamtriazolam
Drugs That Should Not Be Used With Antiretrovirals

1. Incomplete responseIncomplete response
2. Complexity of treatmentComplexity of treatment
3. Short and long term side effectsShort and long term side effects
4. Drug-drug interactionsDrug-drug interactions
5.5. ResistanceResistance
Bad News

ResistanceResistance
Agent Resistance mutationsZDV 41 67 69* 70 151 210 215 219 333
3TC 69* 151 184 333
ddI 65 69* 74 151 184
ddC 65 69 69* 74 151 184
d4T 50 69* 75 151 178
ABC 65 69* 74 115 151 184
Agent Resistance mutations
DLV 103 181 236
EFV 100 103 108 179 181 188 190 225
NV 100 103 106 108 181 188 190
Genotypic Mutations Associated With Resistance to NRTI & NNRTIs

ResistanceResistance
Genotypic Mutations Associated With Resistance to PIs
Agent Resistance mutations
APV 10 36 46 47 48 50 54 63 71 82 84
IDV 10 20 24 32 36 46 48 54 63 71 73 82 84 90
NFV 10 30 36 46 48 71 82 84 88 90
RTV 10 20 32 33 36 46 54 63 71 82 84 90
SQV 10 20 24 30 36 46 48 54 63 71 73 82 84 90
LPV 10 32 46 47 50 84

Overcoming Drug ResistanceOvercoming Drug Resistance
Change to a drug to which virus shows greater susceptibility
Increase exposure to drug
RESISTANCE
Drug

Change to a drug to which virus shows greater susceptibility
Overcoming Drug ResistanceOvercoming Drug Resistance
Guided by Genotypic resistance testing

Goals of Antiretroviral Goals of Antiretroviral Therapy (ART)Therapy (ART)
• Eradication of HIV? Not possible with currently available antiretroviral medications.

GOALS OF THERAPYGOALS OF THERAPY
Clinical goals
Prolongation of life and improved quality of life
Immunologic goals: Achieve immune reconstitution that is quantitative (CD4 to normal range) and qualitative (pathogen-specific immune response)
Virologic goalsReduction in viral load to:
1) halt disease progression 2) prevent/reduce resistant variants
Therapeutic goalsRational use of drugs that achieves virologic goals, but also: 1) maintains therapeutic options 2) relatively free of side effects 3) realistic in terms of probability of adherence
Epidemiologic goals
Reduce HIV transmission

Importance of Initial Therapy
Success Failure Success Failure Success Failure
Naïve patientExperienced
patient
Highly-experienced
patient

HAART: Randomized Comparative Trials*: HIV RNA <400 Copies/mL at Week 48 (ITT)
*All trials have 100 patients/arm
Study 863: LPV/r + d4T + 3TC
DuPont 006: EFV + AZT + 3TC
Study 863: NFV + d4T + 3TC
Agouron 542: NFV BID + d4T + 3TC
Atlantic: IDV + d4T + ddI
Agouron 542: NFV TID + d4T + 3TC
Atlantic: 3TC + d4T + ddI
Atlantic: NVP + d4T + ddI
DuPont 006: EFV + IDV
Patients (%)
DuPont 006: IDV + AZT + 3TC
CNAAB 3005: IDV + AZT + 3TC
CNAAB 3005: ABC + AZT + 3TC
0 10 20 30 40 50 60 70 80 90
Gilead 903: TDF + 3TC + EFV
Adapted from Bartlett J et al. 7th CROI, 2000

Correlation Between Nonadherence and Virologic Failure
Paterson DL et al. Ann Intern Med, 2000
Pat
ien
ts w
ith
vir
olo
gic
fai
lure
* (%
)
Adherence (%)
100
80
60
40
20
0 >95 90–95 80–90 70–80 <70
P<0.001, r=–0.554*Virologic failure defined as HIV RNA >400 copies/mL at last study visit

Duration of initial HAART100
80
60
40
20
0
Pat
ien
ts w
ith
ou
t ch
ang
ein
th
erap
y (%
)
0 120 240 360 480 600 720
Days
197 patients, Cologne 1997–1999 Fätkenheuer G et al. 8th ECCATH, 2001

Reasons for Modification of Initial HAART
197 patients, Cologne 1997–1999113/197 (57%) modified therapy
35
30
25
20
15
10
5
0Adverse Virologic Lost to Otherevents failure follow-up
Fätkenheuer G et al. 8th ECCATH, 2001
Pat
ien
ts (
%)

Considerations in Initiating ART: Asymptomatic HIV
• Willingness of patient to begin and the likelihood of adherence
• Degree of immunodeficiency (CD4+ T cell count)
• Plasma HIV RNA• Risk of disease progression• Potential benefits and risks of therapy

Considerations in Initiating ART: Chronically HIV-Infected Patient,
Asymptomatic
• Strong evidence of decreased mortality and morbidity with ART if CD4 <200 cells/µL or symptomatic
• Theoretical benefit of treatment at higher CD4• Few data establish clinical benefit for treatment if
CD4 >200 cells/µL; optimal point to initiate ART is unknown
• Individualize treatment decisions

Indications for ART in the Chronically HIV-Infected Patient
Treat all (regardless of viral load):
• Symptomatic (AIDS, severe symptoms)
• Asymptomatic, CD4 count <200 cells/µL

Indications for ART in the Chronically HIV-Infected Patient
Offer treatment, after discussion of pros and cons:
• Asymptomatic, CD4 count 200-350 cells/µL

Indications for ART in the Chronically HIV-Infected Patient
Defer Treatment:
Asymptomatic, CD4 count >350 cells/µL
– If HIV RNA >100,000 copies/mL, may consider treatment

Initial Treatment for Previously Untreated Patients: Choosing
Regimens
• Three categories:– 1 NNRTI + 2 NRTIs– 1 PI + 2 NRTIs– 3 NRTIs
• Few clinical endpoints to guide choices• Advantages and disadvantages to each type of
regimen• Individualize regimen choice

GUIDELINES
1987 AZT
1992 AZT/ddI
1995 2 NRTIs
1997 2 NRTIs + PI
1999 2 NRTI + PI/NNRTI
2002 2 NRTI + NNRTI or
PI or 3d NRTI
2004 2 NRTIs + PI/r or NNRTI

Initial Treatment: Preferred Regimens
*Avoid in pregnant women and women with pregnancy potential.
Efavirenz*
+ (lamivudine or emtricitabine)
+ (zidovudine or tenofovir)
2-5
# pills/day
Lopinavir/ritonavir (Kaletra)
+ (lamivudine or emtricitabine)
+ zidovudine
8-10
NNRTI-Based
PI-Based

Future Trends

New agents in the pipeline
New agents should:1. Exhibit high potency.2. Adequate drug levels.3. Activity against resistant isolates.4. Penetration into all cellular and bodily compartments
(eg, central nervous system, genital tract). 5. Favorable drug interaction profile.6. Minimal side effects. 7. Convenient to take, with no food restrictions and
minimal dosing requirements; preferably once daily.

Class Target Example Compounds
AttachmentInhibitors
gp120, CD4 specific Mab, PRO 542 soluble CD4 and CD4-Ig
Co-receptorInhibitors
CXCR-4 AMD-3100
CCR-5 SCH-C, specific Mab,
FusionInhibitors gp41 T-1249, D-peptides
Entry inhibitors under developmentEntry inhibitors under development

Barriers to the Development of an Barriers to the Development of an Effective AIDS VaccineEffective AIDS Vaccine
• Sequence variation• Protective immunity in natural infection not clearly
established• Lack of adequate animal model to study vaccine protection
with HIV• Latency and integration of HIV into host genome• Transmission by cell-associated virus• Limited knowledge about mucosal transmission and
immune responses• Financial disincentives• Ethical issues

Conclusion• HIV/AIDS is no longer a “death sentence” for infected
individuals• Cure is beyond reach at this stage, but patients can survive
years to decades longer. • Better understanding of the HIV has allowed better
treatment modalities.• More drugs and drug problems are on the horizon.• Control of HIV replication by the host immune system may
be the best outlook for future research.• Intense vaccine research is ongoing and ultimately will be
the major preventive measure against HIV infection