Embed Size (px)
Citation preview

Current Concepts in
Assessment, Management, and Prevention CE Broker Provider #50-1997
CE Broker Course Tracking #20-6744
NCBTMB Approved Provider #154019-00
The Institute for Advanced Therapeutics, Inc.
PO Box 848152
Pembroke Pines, Florida 33084 1-954-441-9553

Consultants: Stephen Silver, M.D.
Research and Development: Charles Cook, L.M.T. Editor: Mark Blum, D.D.S.
By: Renee J. Demmery
Copyright @ 1999 All Rights Reserved
NOTE: The images used herein were obtained from IMSI’s MasterClips® and MasterPhotos™ Premium Image Collection, 1895 Francisco Blvd. East, San Rafael, CA 94901-5506, USA unless otherwise noted.
TABLE OF CONTENTS
COURSE DIRECTIONS
MAILING INSTRUCTIONS
COURSE OBJECTIVES
INTRODUCTION
CHAPTER 1
HISTORY OF THE PATIENT
CHAPTER 2 THE PHYSICAL EXAMINATION
CHAPTER 3 DIAGNOSTIC TESTING
CHAPTER 4 SOME COMMON CAUSES OF NECK PAIN
CHAPTER 5 TREATMENT OF NECK PAIN
CHAPTER 6 PREVENTION OF NECK PAIN FOR HEALTH CARE PROFESSIONALS
ANSWERS TO PRE-TESTS
NECK PAIN POST-TEST
GLOSSARY OF MEDICAL TERMS
REFERENCE LIST

HOW TO BEST PROCEED WITH THIS COURSE Each chapter should be approached systematically in a careful and objective manner.
The pre-test questions at the end of each chapter will help you determine the mastery of the material. It is important to master each chapter before going on to the next. Relax, take your time, and go at your own pace. Only after you have successfully mastered all the material in the course and completed all the pre-test questions correctly in each chapter should you proceed to the post-test questions.
COMPLETING THE POST-TEST Read each question carefully before answering. Keep in mind that each question has
only one correct answer. The post-test consists of 100 questions. For a passing grade, you must correctly answer 80 questions. We encourage your input and would welcome any suggestions to improve our course or test questions. Please feel free to note your suggestions or comments on the evaluation form.
INFORMATION FOR CERTIFICATION In order to receive continuing education credit, you must be a registered purchaser of
this course. Only one person per purchase of this course is eligible to receive credit. Please notify us of any address or name changes as we keep permanent records for certification and licensure.
*The information in this course has been carefully researched and is generally accepted as factual at the time of publication. The Institute for Advanced Therapeutics, Inc. disclaims responsibility for any contradictory data prior to the publication of the next revision of this course.
The Institute for Advanced Therapeutics, Inc. P.O. Box 848152 Pembroke Pines, Florida 33084
If you have any questions regarding this course, please contact our Customer Service Department at 1-954-441-9553, fax us at 1-954-432-1824 or email us [email protected] .
COURSE OBJECTIVES
Upon completion of this course, you will be able to:
1. Recognize red flags for cancer in patients with neck pain. 2. List common diagnostic tests to elucidate neck pain etiology and describe their indications and limitations. 3. Identify the signs and symptoms of acute cervical sprain/strain. 4. Describe which activities may predispose a person to cervical intervertebral disc herniation. 5. Analyze the effectiveness of many common cervical pain treatments being utilized by a variety of health care practitioners today. 6. Discuss measures to reduce the risk of neck injury in the workplace and educate others in proper posture and lifting techniques.
NOTE: This course was developed to help expand the knowledge and skills of massage therapists and bodyworkers with respect to the subject of neck pain. It is the physician’s responsibility to diagnose and order treatment for patients with neck pain.

INTRODUCTION
Although it has been reported that 80 to 90 percent of the adult population will experience some form of low back pain at some time in their lives, only 35 to 40 percent will experience neck and arm pain. Those who will become disabled due to chronic neck symptomatology represent less than 5% of patients with neck problems.
The two stages of neck pain:
1. Acute - episodes of acute neck pain present for less than three months.
2. Chronic - continuous pain persisting for greater than three months unrelieved with three months of relevant medical treatment for acute neck pain.
Neck pain can sometimes be referred to the head, the shoulders, the arms, the chest,
and the back. The most common cause of acute neck injury is motor vehicle accidents. Other possible etiologies for neck pain include occupational injuries, trauma, disease,
congenital anomalies, and poor posture.
DEMOGRAPHICS OF NECK PAIN*
AGE 25-44 years 6.6%
45-64 years 10.1%
65-74 years 9.3%
SEX Male 7.0%
Female 9.4%
RACE White 8.6%
Black 5.6%
Other 7.2%
*Defined by pain in the neck on most days for at least 2 weeks.
* Source: Praemer A, Furner S, Rice DP: Musculoskeletal Conditions in the United States. Illinois: American Academy of Orthopaedic Surgeons 1992, pages 23-33.
Proper evaluation of neck pain requires a multi-disciplinary team approach. The team begins with a treating physician, usually a general physician, and can also include a physical therapist, occupational therapist, massage therapist, or psychologist. Patients should be referred, however, to a neuro-musculo-skeletal specialist i.e. orthopedist, neurologist/neurosurgeon, physiatrist, or rheumatologist with eight years of professional education in medicine or osteopathy and no less than 4 years of study of the neuro-musculo-

skeletal system under the following circumstances:
1. The patient is experiencing pain that is both severe and disabling.
2. The patient experiences persistent pain without improvement or worsening pain.
3. The patient exhibits clinical evidence of nerve root compromise.
It is of utmost importance that patients with neck pain have an efficient, cost effective, and accurate evaluation, as the wrong diagnosis and/or treatment can make a simple case of neck pain a complex one.
It is reported that neck pain represents less than 2% of all injuries in the workplace. The most common diagnosis given as a result of work-related neck injuries is sprain/strain. Certain occupations are at higher risk than most for neck symptoms. Risk factors may include a history of frequent bending and twisting at work.
OCCUPATIONS AT INCREASED RISK OF NECK PAIN
1. Machine operators
2. Carpenters
3. Office workers and keyboard operators
4. Dentists
5. Farmers
6. Meat carriers
7. Miners
Source: Hagberg M, Wegman, DH: Prevalence rates and odds ratios of shoulder-neck diseases in different occupational groups. Br J Ind Med 44:602, 1987.
The purpose of this course is to educate massage therapists and/or bodyworkers, who may be part of the multi-disciplinary team, in the complexities of neck pain including diagnosis and current treatment options available today. Specific attention will be given to the many etiologies of neck pain, diagnostic testing, and therapeutic options.
CHAPTER SUMMARY
It is reported that 35 to 40% of the adult population will experience neck and arm pain.
Those who will become disabled due to chronic neck symptomatology represent less than 5% of patients with neck problems.
The most common cause of acute neck injury is motor vehicle accidents.
Risk factors of work-related neck pain may include a history of frequent bending and twisting at work.

CHAPTER ONE HISTORY OF THE PATIENT
The taking of a thorough medical history plays an important role in the diagnosis of neck pain disorders. Answers the patient provides may help lead the general physician or specialist to an accurate diagnosis and, more importantly, may rule out potentially life-threatening causes of neck pain such as cancer or serious infection.
Although most patients with neck pain will have non-emergent conditions, it is
important to exclude the following conditions:
1. Tumor or metastatic disease. 2. Acute fracture. 3. Infection. 4. Serious neurological deficit. 5. Potentially life-threatening disease. 6. Degenerative or rheumatoid arthritis. 7. Herniated disc. 8. Cervical stenosis. 9. Cervical osteomyelitis. 10. Internal disease unrelated to the cervical spine.
RED FLAGS FOR CANCER IN PATIENTS WITH NECK PAIN
1. An elderly patient presenting to the office for the first time with neck pain. 2. A past medical history of cancer. 3. Recent unexplained weight loss. 4. Recent unexplained fever. 5. Chronic neck pain or increasing neck pain refractory to standard treatment.
Source: Universe of Florida Patients with Neck Pain or Injury. Medical Practice Guidelines. Published by The Agency for Health Care Administration. March 1996: 1-2.
IMPORTANT QUESTIONS TO ASK WHEN TAKING THE MEDICAL HISTORY
1. Where is the location of your pain and what is the intensity? (see illustration 1). 2. What is the duration of your symptoms? (Less than three months or greater than three months?) 3. Was the onset of your neck pain spontaneous or related to a specific trauma? Please detail.

4. Does your neck pain radiating into your head, shoulders, arms, chest, or back? If so, please detail. 5. Is your pain associated with any weakness, stiffness, numbness, tingling, or peculiar sensations? Please describe. 6. Are there any limitations as to what you can do as a result of your neck pain? Please detail. 7. Have you been treated previously for your neck pain? If so, how were you treated and what was the response. 8. Have you experienced a recent fever or unexplained weight loss? 9. Do you have a past medical history of cancer?
Source: Universe of Florida Patients with Neck Pain or Injury. Medical Practice Guidelines. Published by The Agency for Health Care Administration. March 1996: 1.
It may also be helpful to ask patients to circle the area or areas of pain using a written visual diagram. (see illustration 1). A pain analog scale may be used as well to illustrate the intensity of pain.
ILLUSTRATION 1
Circle the area/areas where you are experiencing pain. Next to the area/areas circled, document the intensity of pain using the analog scale below.
1 2 3 4 5 6 7 8 9 10

LESS PAIN MORE PAIN
CHAPTER SUMMARY
Potentially life-threatening causes of neck pain include cancer and serious infection.
It is important to exclude acute fracture in patients presenting with neck pain.
Recent unexplained weight loss is considered a red flag for cancer in patients with neck pain.
When taking the medical history, patients should be asked if they have a past medical history of cancer.

CHAPTER TWO
THE PHYSICAL EXAMINATION
Following completion of a thorough medical history, a physical examination must be performed.
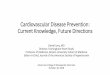
POSTURE
Poor posture can contribute to neck pain by subjecting the cervical spine to abnormal mechanical stresses. The musculature of the neck and back function to hold the spinal column in proper place and provide for movement. Poor posture is highlighted by a forward head carriage, hunched shoulders, a protruding abdomen, and hyperextended knees. (see illustration 2). This type of behavior can result in myofascial pain in both the cervical and lumbar regions.
ILLUSTRATION 2
EXAMPLE OF GOOD POSTURE
EXAMPLE OF BAD POSTURE
RANGE OF MOTION
The cervical spine is an extremely flexible structure comprised of 37 separate joints and 7 vertebrae. The neck is the most active part of the human musculoskeletal system moving over 600 times per hour whether awake or asleep. Range of motion is an important indicator of cervical spine health and active range of motion should be tested in all the basic planes.

ILLUSTRATION 3
Extension/Flexion Rotation Lateral Bending
*Illustration by Renee J. Demmery
Active range of motion involves observing the patient carry out range of motion from instructions. The difference between the endpoint of motion in one direction and the endpoint of motion in the opposite direction is referred to as range of motion. The limits of motion are when movement stops or when the patient experiences pain or an unusual sensation. During range of motion testing, the physician should document any restriction of movement and note any jerky or halting movements. Jerky movements could indicate soft tissue inflammation around the cervical spine.
NEUROLOGICAL ASSESSMENT
The neurological evaluation is divided into three parts: motor strength testing, sensory testing, and reflex testing.
Motor strength testing involves testing the muscles of the neck and upper extremities in an effort to determine the integrity of the cervical nerve supply. This is accomplished by asking the patient to carry out certain motions of the neck and upper extremities against resistance. Deficits can point to the precise level of cervical nerve root involvement. The physician should also look for evidence of muscle wasting which can be a sign of neurological compromise.
Sensory testing is performed by eliciting the patient’s response to modalities such as light touch, pinprick, position sense, or vibration sense. The cervical nerve root levels refer sensation to areas on the skin in patterns called dermatomes. (see illustration 3). When a sensory deficit is noted over a specific dermatomal area, it can be correlated to nerve root involvement at that level.
ILLUSTRATION 4

*Illustration by Renee J. Demmery
Reflex testing including the biceps, triceps, and brachioradialis should be carried out to help locate possible nerve root involvement.
The biceps reflex can be assessed by tapping over the biceps tendon with a reflex
hammer. Contractions indicate neurological integrity of the C5 nerve root.
The triceps reflex is tested by tapping on the triceps tendon with the reflex hammer where it crosses the olecranon fossa on the posterior aspect of the arm. Contractions indicate neurological integrity of the C7 nerve root.
The brachioradialis reflex is evaluated by tapping on the lower end of the radius with the reflex hammer. Flexion of the forearm indicates neurological integrity of the C6 nerve root.
C8 and T1 have no reflex and motor and sensory testing should be performed to test
the integrity of their nerve roots.
The presence of upper motor neuron lesions can be detected by carrying out two additional tests. The Hoffmann’s reflex is tested by placing the patient’s long finger of the dominant hand over the DIP joint of the physician’s long finger palm side down. Next, as the patient’s long finger is slightly extended, the DIP joint of the patient’s long finger is flicked downward by the physician’s thumb. The Hoffmann’s reflex is positive if involuntary flexion of the DIP joints of the patient’s thumb and little finger are simultaneously elicited.
The jaw jerk reflex is tested by tapping downward on the chin with the reflex hammer as
the jaw is relaxed and slightly open. The reflex is normal if the jaw closes. However, brisk closure of the jaw may indicate an upper motor neuron lesion.
OTHER TESTS
Distraction Test: The physician applies upward traction on the neck. Relief of radicular symptoms may indicate nerve root compression.
Compression test: The physician applies downward pressure on the cervical spine. If the patient experiences pain, this may indicate narrowing of the neural foramen, increased pressure on the facets, or muscle spasm. If the pain is referred to the extremities, the physician should note whether it corresponds to a specific dermatomal pattern which may help point to the neurological level of pathologic involvement.

Spurling’s maneuver: This can be performed by hyperextending the neck and rotating the head to each side. If radicular pain is reproduced, this may indicate nerve root compression or irritation.
Lhermitte’s sign: Severe shock-like shooting pains spreading down to the legs after flexion of the neck would indicate a positive Lhermitte’s sign. A positive test could indicate cervical spinal cord compression possibly caused by a large disc herniation or a spinal cord lesion. This test may also be positive in patients with multiple sclerosis affecting the spinal cord.
CHAPTER SUMMARY
The musculature of the neck and back function to hold the spinal column in proper place and provide for movement.
Range of motion is an important indicator of cervical spine health.
Motor strength testing involves testing the muscles of the neck and upper extremities in an effort to determine the integrity of the cervical nerve supply.
A positive Hoffmann’s reflex and jaw jerk reflex may indicate an upper motor neuron lesion.

CHAPTER 3 DIAGNOSTIC TESTING
LABORATORY TESTING:
Blood tests are rarely indicated in the diagnosis of neck pain. Some patients may warrant blood testing if they fail to respond to neck pain therapy or the character of the neck pain changes significantly. The elderly may warrant blood testing if they develop a sudden onset of neck pain without a history of trauma since tumors and infection occur more commonly in the elderly and can be detected through blood screening. An increased erythrocyte sedimentation rate or ESR may indicate infection, rheumatoid arthritis, or other inflammatory condition as a cause for neck pain. A positive rheumatoid factor in the face of neck pain may point to rheumatoid arthritis involving the cervical spine. An elevated serum calcium level may indicate malignancy.
X-RAYS
X-rays can be extremely useful in locating the source of neck pain due to fracture, tumor, or osteoarthritis. Plain radiographs are excellent in demonstrating bony structures but are unable to demonstrate soft tissue structures clearly.
In patients not exhibiting any signs of tumor, infection, fracture, or other serious red flag
conditions, the Agency for Health Care Administration (AHCA) neck pain and injury guideline advises delaying all imaging studies including x-rays for one month. Plain radiographs within this period in the absence of such findings will usually be of low yield. If x-rays are obtained too soon in the diagnostic course or are incorrectly interpreted, the patient may not receive a proper diagnosis thus delaying effective treatment. Furthermore, the patient will be unnecessarily exposed to radiation.
It is important to remember that plain radiographs as well as other studies such as MRI
and CT scans may show abnormalities, however, cannot prove that those abnormalities are actually producing the patient’s neck pain symptoms. Research shows that 50 percent of patients will have degenerative changes on plain radiographs after the age of 40 and, by the age of 65, 90 percent of these patients will have degenerative changes. It is also important to note that it is difficult to rule out infection using plain radiographs. If within the initial month of treatment, the symptoms do not progress, then imaging is usually not suggested and conservative management of the neck pain is indicated.
Patients presenting for initial evaluation following trauma to the cervical spine do not necessarily need x-rays if they meet the following criteria:

1. The patient does not complain of neck pain. 2. There is no tenderness on palpation of the cervical region. 3. The patient does not complain of weakness or paresthesias. 4. The patient has no motor or sensory deficits. 5. The patient is reliable and appropriately responding. 6. The patient has a sprain or strain of the neck or soft tissue injury.
X-rays should be performed immediately at the time of initial examination if the following red flags are present:
1. A history of recent significant trauma. 2. A history of recent unexplained weight loss. 3. Immunosuppression. 4. A history of intravenous drug use. 5. Recent fever of unknown origin. 6. A past medical history of cancer. 7. A history of steroid use of prolonged duration.
X-rays should also be performed if the patient’s symptoms are unresolved or worsened following four weeks of conservative management. When x- rays of the cervical spine are warranted, a maximum of five views is recommended. The patient’s neck should be immobilized and lateral films showing all seven cervical vertebrae are advised including the C7-T1 interspace. The radiographer can then proceed to AP and odontoid views. If the films are negative and cervical spine pathology is still suspected, additional films may be indicated and/or referral to a neuro-musculo-skeletal specialist for CT scanning or MRI scanning would be appropriate.
Because of exposure to radiation, x-rays are contradicted in pregnancy.
BONE SCAN
Bone scan or radionuclide imaging is a valuable screening tool in patients where suspicion of tumor or metastatic involvement is high. A bone scan may detect abnormalities not seen on plain radiographs and may help to confirm early osseous lesions or inflammatory processes.
The sensitivity of a bone scan for the presence of malignancy is approximately 99
percent. Bone scans are also useful in detecting occult fractures, compression fractures, arthritis, discitis, metabolic bone disease, and osteomyelitis. A bone scan should be performed however only in patients in which plain radiographs, laboratory tests, or physical findings indicate one of the above conditions. Because a bone scan requires exposing the patient to radiation, it is contraindicated in pregnancy.
It should be noted that a bone scan may not always distinguish between a fracture, osteoarthritis, or malignancy. A bone scan may even show normal in patients with diffuse bony involvement demonstrated on CT scan or MRI, as in osteoclastic disease such as multiple myeloma.

MAGNETIC RESONANCE (MR) IMAGING
Available since the mid 1980’s, MR imaging or MRI produces detailed images of the
soft tissues of the neck, spinal cord, and nerve roots. MR imaging is non-invasive and clear images are produced without the use of radiation or contrast material. MRI has been the procedure of choice for diagnosing herniated discs, infection, spinal cord tumors, or progressive neurological disease.
In patients with severe radiculopathy unresponsive to conservative measures, an MRI
may be indicated. MRI scanning is also indicated in patients presenting with progressive weakness or patients suspected of having spinal stenosis.
It is important to remember, however, that many asymptomatic people will have
abnormalities found on MRI scans that represent normal degenerative changes of the spine as well as asymptomatic herniated or bulging discs. Approximately one-third of asymptomatic individuals will show abnormalities on MRI. Therefore, interpretation should be performed cautiously.
MRI should not be performed in patients with cardiac pacemakers, metallic foreign bodies, or ferromagnetic implants. Also, patients with severe pain who are not able to lay completely still may not be ideal candidates for MRI scanning as movement may create suboptimal images. Severe claustrophobia may rule out successful MRI scanning in some patients as well.
COMPUTED TOMOGRAPHY (CT) SCAN
In patients where MRI scanning is not indicated, CT scan may provide excellent evaluation of the osseous structures of the spine. CT scanning uses x-rays to produce cross-sectional images and can define the spatial relationships of the bony and soft tissue structures.
CT combined with myelography can provide superior bony detail of the spinal canal,
spinal column, subarachnoid space, and extraspinal soft tissues. CT/myelography

involves the instillation of contrast media followed by CT scanning.
CT is useful in assessment of spinal stenosis or disc prolapse, paraspinal abscess, epidural scarring, spinal tumors, and bony fragments due to trauma.
ELECTROMYOGRAPHY (EMG) AND NERVE CONDUCTION STUDIES
Electromyography (EMG) and nerve conduction studies can be used to identify the severity and location of nerve root compression in patients with radiculopathy or myelopathy and can help identify nerve and muscle pathology contributing to the patient’s symptoms.
EMG can help distinguish neck pain due to cervical radiculopathy from neck pain due to acute or chronic peripheral entrapment neuropathies such as carpal tunnel syndrome.
EMG records the action potentials of muscle fibers by the use of needle electrodes
inserted at various depths into the muscles to be studied. Each muscle is examined at multiple locations and in multiple directions for more accurate results.
Nerve conduction studies may also be performed in conjunction with EMG to study
motor and sensory nerves. Nerve conduction studies are performed by placing surface electrodes over the hand muscles and introducing electrical current.
CHAPTER SUMMARY
Blood tests are rarely indicated in the diagnosis of neck pain.
A positive rheumatoid factor in the face of neck pain may point to rheumatoid arthritis involving the cervical spine.
X-rays can be extremely useful in locating the source of neck pain due to fracture, tumor, or osteoarthritis.
A bone scan may detect abnormalities not seen on plain radiographs.

CHAPTER FOUR
SOME COMMON CAUSES OF NECK PAIN
ACUTE CERVICAL STRAIN/SPRAIN
Acute cervical strain refers to an injury to the muscles of the cervical region. Acute cervical sprain refers to an injury to the ligaments of the cervical region. Signs and symptoms may include headache, decreased range of motion, and pain on motion of the neck. These two conditions can occur separately or in conjunction with each other. Acute cervical strain/sprain is usually brought on by precipitating trauma, although the symptoms may occur sometime after the event. Patients usually hold the neck in a stiff manner and the muscles affected can usually be palpated. If x- rays are taken, straightening of the normal cervical curve may be noticed. Patients may exhibit the following:
1. Neck pain which may or may not refer to the arms or shoulders.
2. Decreased range of motion of the cervical spine.
3. Muscle spasm.
4. Point tenderness.
Treatment for acute cervical strain/sprain is almost always conservative. In most cases,
symptoms will resolve within four to six weeks. Treatment options may include one or more of the following:
1. Limiting activity known to increase symptoms.
2. Medications which may include non-steroidal antiinflammatories,
analgesics including ointments, and muscle relaxants.
2. Self-administered treatment with heat or ice packs.
3. At-home cervical traction.
4. An at-home exercise program as instructed by the physician.
5. Spinal manipulation.

7. Licensed physical or occupational therapy as prescribed by the
physician.
X-rays are indicated in patients who are unresponsive to four weeks of conservative treatment. If the x-rays are normal, further diagnostic testing utilizing EMG and nerve conduction studies may be indicated.
TREATMENTS NOT RECOMMENDED FOR ACUTE CERVICAL SPRAIN/SPRAIN
Oral steroids Colchicine
Muscle relaxants beyond one-week Transcutaneous nerve stimulation (TENS) Cervical traction applied in the office setting Biofeedback
Trigger point or ligamentous injections Neck collar of long duration Acupuncture
More than three sessions of epidural steroids
The above table discusses treatments not recommended for acute cervical strain/sprain as per the AHCA neck pain and injury guideline, however, many physicians currently find these treatments to be effective and continue to utilize them in their practice.
ACUTE DISC HERNIATION
Caused by either trauma, heavy lifting, or degenerative changes, a herniated disc is when the nucleus pulposus protrudes through the fibers of the annulus fibrosus. Most cervical disc herniations occur posterolaterally. Symptoms of a cervical herniated disc depend on the size and location of the disc as well as other factors and may include neck pain with radiculopathy, which may be accompanied by weakness in the arms or hands. The patient may also exhibit positive neurological signs and asymmetric reflexes. Cervical disc herniations at multiple levels can occur in up to 12% of patients over 30 years old. The most common cervical disc affected is C6-7 (60%). The second most common cervical disc affected is C5-6 (30%).
Some people may have a cervical herniated disc and report no symptoms. It is
estimated that an average of 8% of people have an asymptomatic cervical herniated disc.
MRI is the imaging modality of choice in detecting acute cervical disc herniation. However, MRI cannot usually distinguish between symptomatic and asymptomatic herniations. CT is also sensitive in detecting cervical herniated disc herniation. Although plain

x-rays can detect loss of disc height and cervical canal stenosis, they cannot directly image neural compression and thus are not recommended in evaluating for cervical disc herniation. EMG may be useful in detecting nerve root impingement and can help correlate the level of cervical disc herniation. Blood tests are not useful in detecting cervical disc herniation.
Treatment for acute cervical disc herniation is initially conservative. Treatment options may include one or more of the following:
1. Limiting activity known to increase symptoms.
2. Medications which may include non-steroidal antiinflammatories and analgesics.
3. Self-administered treatment with heat or ice packs.
4. Gentle spinal manipulation depending on the degree of herniation.
5. An at-home exercise program as instructed by the physician.
6. Epidural steroid injections.
7. Cervical collar (brief duration).
8. Referral for surgical evaluation if necessary.
Conservative measures should continue for a minimum of four weeks. If symptoms are
not relieved with conservative therapy, epidural steroid injections can be considered in patients with radiculopathy. Surgery should be considered as a last resort and only when there are progressive neurologic symptoms, nerve root compression, and conservative treatment has failed.
CERVICAL SPONDYLOSIS
Cervical spondylosis, sometimes referred to as cervical degenerative disc disease, is an age-related process occurring in over 90% of adults over the age of 50 and nearly 100% by 70 years of age. The most common levels affected are C5-6, C6-7, and C4-5 respectively. Patients may or may not be symptomatic. Previous injury to the cervical region can predispose patients to cervical spondylosis. Diagnostic indicators may include:
1. Loss of disc height at multiple levels with or without disc protrusion or acute herniation.
2. The presence of osteophytes (bony outgrowths from vertebral bodies).
3. Degenerative arthritis of the cervical spine.
4. Intersegmental displacement.
5. End-plate sclerosis.

6. The presence of vacuum phenomenon.
Symptomatic patients with cervical spondylosis may complain of one or more of the
following:
1. Neck ache or pain increased with activity or rotation of the neck.
2. Neck stiffness.
3. Pain referring to the shoulder or interscapular regions.
4. Dizziness.
Treatment for cervical spondylosis is almost always conservative. In most cases, symptoms are chronic. Treatment options may include one or more of the following:
1. Limiting activity known to increase symptoms.
2. Medications which may include non-steroidal anti-inflammatories and analgesics.
3. Self-administered treatment with heat or ice packs.
4. At-home gentle cervical traction as prescribed bythe physician.
5. Gentle spinal manipulation depending upon the degree of degenerative changes.
6. Cervical collar to restrict motion of the neck when symptoms are acute.
7. Referral for surgical evaluation if necessary.
Surgical options should be considered only after conservative measures have failed and
there is significant functional disability and evidence of spinal cord compression.
OTHER CAUSES OF NECK PAIN
There are numerous conditions that can contribute to neck pain. Below is a table of some of these conditions.
SOME CAUSES OF NECK PAIN
Sprain/strain Disc
herniation
Spondylosis (degenerative disc disease)
Rheumatoid arthritis or psoriatic arthritis
Polymyalgia rheumatica

Fibromyalgia
Meningitis
Ankylosing spondylitis
Diffuse idiopathic skeletal hyperostosis Vertebral
osteomyelitis
Infection of the intervertebral disc Herpes
zoster
Spinal tumors
CHAPTER SUMMARY
Acute cervical strain and acute cervical sprain can occur separately or in conjunction with each other.
Acute cervical strain/sprain is usually brought on by precipitating trauma.
Cervical disc herniations at multiple levels can occur in up to 12% of patients over 30 years old.
Previous injury to the cervical region can predispose patients to cervical spondylosis.

CHAPTER FIVE
TREATMENT OF NECK PAIN
Treatment measures vary greatly depending on the cause of the neck pain.
BED REST
Recent thinking has shifted away from bed rest as a viable treatment for neck pain. Many studies have concluded that bed rest longer than two or three days may actually be detrimental to recovery of acute episodes of neck pain. Bed rest promotes muscle atrophy, stiffness, and depression. Experts agree that, instead of bed rest, patients should be encouraged to continue daily activities as tolerated except in cases of severe neurologic compromise requiring surgery.
NECK SUPPORT
Neck support of brief duration can be beneficial to some patients suffering from neck pain. The main reasons neck support is used include the following:
1. To decrease pain by limiting motion of the cervical spine. 2. To limit further damage and protect the unstable spine following trauma.
There are four types of cervical support systems used today.
1. Soft, rigid - the most commonly used and recommended for mild neck pain. 2. Head-cervical - restrictive device molded around the posterior head and cervical regions. 3. Head-cervical-thoracic - restrictive device molded around the posterior head, cervical, and thoracic regions. 4. Halo - the most restrictive device used when any movement of the cervical spine would be harmful.
The AHCA neck pain and injury guideline does not recommend prolonged neck support
except in cases of spinal cord compromise. Use of a neck supportive device beyond two or

three days may cause detrimental effects such as muscle wasting and atrophy, contracture of soft tissue structures, and psychological dependence.
MEDICATION
Many types of drugs have been found useful in controlling neck pain on both a short-term and long-term basis. Nonsteroidal anti-inflammatory drugs, non-narcotic analgesics, narcotic analgesics, and muscle relaxants have been found to relieve neck pain symptoms. Narcotic analgesics are more effective in relieving neck pain than non-narcotic analgesics or nonsteroidal anti-inflammatory drugs, however, should be prescribed with caution and on a limited basis due to potential complications such as dependence, drowsiness, and clouded judgement.
SPINAL MANIPULATION
Spinal manipulation or the use of external force on parts of the axial skeleton is performed by a variety of health care practitioners including MDs, DOs, chiropractors, and physical therapists. Although research-based evidence is limited, many practitioners have found spinal manipulation to be effective in relieving symptoms of mechanical neck pain.
Patients should be assessed for contraindications to spinal manipulation before treatment including the following:
1. Fracture. 2. Osteoporosis. 3. Malignancy. 4. Osteomyelitis. 5. Torn ligaments. 6. Herniated disc. 7. Acute arthritis. 8. Neurologic dysfunction. 9. Bleeding disorders or patients on anticoagulant therapy. 10. Vertebral artery stenosis. 11. Carotid artery stenosis.

12. Congenital anomalies.
MASSAGE THERAPY
Massage therapy is becoming increasingly accepted as an effective treatment modality for patients suffering from neck pain. Massage techniques can be performed by chiropractors, osteopathic physicians, physiatrists, nurses, and qualified massage therapists. Massage is believed to help decrease muscle spasm and restore normal range of motion to the cervical spine. Massage therapy has been found to be most effective in the treatment of acute cervical pain. Massage may, in some cases, reduce the need for drug treatment. Contraindications are similar to that of spinal manipulation.
CERVICAL TRACTION
Traction is applied to the cervical spine in an effort to stretch muscles, ligaments, and spinal components. Proponents believe traction to relieve nerve root compression, prevent lysis of adhesions, decrease pressure within the intervertebral discs, ease muscle spasm, and improve vascular status.
There are at least ten different types of traction. Traction may be applied manually or by
use of a mechanical device. The weight and duration of the traction are adjusted according to the patient’s tolerance.
Contraindications to cervical traction are numerous and include the following:
1. Osteomyelitis. 2. Osteoporosis. 3. Spinal cord compression. 4. Rheumatoid arthritis. 5. Malignancy. 6. Torticollis and structural scoliosis. 7. Spondyloarthropathies. 8. Myelopathy. 9. Hypermobility. 10. Temporomandibular joint (TMJ) dysfunction.

BIOFEEDBACK
Although the efficacy of biofeedback in neck pain is yet to be determined, it is a modality employed to teach patients to relieve tension and anxiety whenever they feel pain. Biofeedback requires multiple treatment sessions and is indicated in patients with chronic neck pain. A series of electrodes are attached to the patient that measure one or more physiologic variables such as blood pressure, skin temperature, and heart rate. Patients are taught to control these variables while observing images or listening to prerecorded tapes.
The AHCA neck pain and injury guideline does not recommend biofeedback for the
treatment of patients with neck problems.
TRANSCUTANEOUS NERVE STIMULATION (TENS)
A TENS unit is a small battery-operated device that involves the careful placement of electrodes over painful areas delivering a vibratory electrical current. The transcutaneous electrical stimulation is thought to relieve pain by working on the patient’s nerves and stimulating the body’s natural pain killing endorphins. There is much conflicting data regarding the effectiveness of this device, thus the AHCA neck pain and injury guideline does not recommend transcutaneous nerve stimulation for the extremities of patients with neck problems.
THERAPEUTIC ULTRASOUND
Therapeutic ultrasound employs high-energy sound waves to relieve painful muscle

spasms and joint pain. It is believed that the ultrasonic waves increase blood flow by producing heat deep into the joints, muscle, and bone. Ultrasound is believed to hasten repair of the tissues and produce temporary relief of pain by increasing the threshold for pain perception.
Due to conflicting studies on the efficacy of therapeutic ultrasound, the AHCA neck pain
and injury guideline has determined that the use of therapeutic ultrasound in the treatment of neck problems is of “insufficiently proven benefit” to justify its cost.
EXERCISE
Exercise is of tremendous value in the management of neck pain. Used primarily to increase strength in a specific muscle or group of muscles, exercise can also be used to decrease pain by means of increasing range of movement. Most patients with neck problems can benefit from walking, swimming, or biking. Low-impact aerobic exercise can also be beneficial during the first month of symptoms by helping patients return to their optimal level of function. Conditioning exercises may be started in patients with persistent symptoms of neck pain. Exercise can be continued if the patient notes decreased pain and increased range of movement. Exercise should be discontinued if the patient notes severity of pain beyond that expected with normal exercise or if the patient notes radiation of pain into the extremities.
Machines directed specifically at improving neck function provide no increased benefit over traditional exercise in patients with neck problems.
INJECTION THERAPY
Epidural corticosteroid injections are a viable treatment option in patients with cervical radiculopathy when conservative treatment has failed to provide relief and as a means of avoiding surgery. Other types of injections such as trigger point, ligamentous, and sclerosant injections are considered invasive and not recommended in patients with neck problems. Some physicians believe that these injections help relieve neck pain, however research regarding the effectiveness of these injections is lacking.

PHYSICAL THERAPY
Patients can benefit from a good structured exercise program supervised by a licensed professional physical therapist. Physical therapy is preferred over other modalities such as TENS, ultrasound, and heat and cold, which have yet to be proven efficacious in the treatment of acute neck pain. Exercises should be focused to meet specific goals such as to condition the neck muscles and regain normal movement of the cervical spine. An adjunct home exercise program should be implemented as well for maximal benefit.
According to the AHCA neck pain and injury guidelines, a maximum of 12 sessions of
physical therapy should be performed for patients with functional disability.
ACUPUNCTURE
Acupuncture is the ancient Chinese practice of careful insertion of tiny needles into the skin. Acupuncture is believed to:
1. Relieve pain by stimulating the release of endorphins. 2. Produce an anesthesia effect by stimulating a location distant to the painful site.
As acupuncture is an invasive procedure yet to be proven effective in reducing neck pain, the AHCA neck pain and injury guideline does not recommend acupuncture for treatment of neck problems.
HEAT AND COLD THERAPY
Heat therapy can come in many forms including hot packs, diathermy, hydrotherapy, paraffin bath, or heat lamps. These modalities are meant to induce muscle relaxation, increase blood circulation, and decrease inflammation and spasm. Superficial heat is believed to produce an analgesic-type effect when applied, although the exact mechanism

of this is unknown.
Cold therapy or cryotherapy is utilized to treat acute injuries to reduce swelling and minimize tissue damage by reducing blood flow and decreasing metabolic activity. Therapeutic cold in the form of ice packs, ice massage, or vapo-coolant sprays can also be used to produce a temporary analgesic effects, as long as the source of cold is applied. Once removed, however, the analgesic effect quickly wears off.
According to the AHCA neck pain and injury guideline, heat and cold therapy have not
been proven to be of benefit to justify their cost.
SURGERY
Although only a small percentage of patients suffering from chronic neck pain will be referred for surgery, it is important to carefully select patients based on certain criteria in relation to their diagnosis. Inappropriate patient selection accounts for most cases of poor surgical outcome.
Generally, chronic neck pain sufferers can be considered for surgery if the following
circumstances are met:
1. The patient has failed to achieve acceptable results from a variety of conservative therapy measures and has intractable pain that interferes with his/her ability to perform daily activities.
2. The patient does not display signs of exaggeration and has demonstrated a good faith effort towards rehabilitation.
3. A distinct surgical lesion has been identified and believed to be the cause of the patient’s pain symptomatology.
The decision to operate ultimately lies in the hands of the physician, however some
basic guidelines apply and are as follows:
CERVICAL SURGERY GUIDELINES
TYPES OF CERVICAL SURGERY
1. Laminectomy.
2. Laminotomy. 3. Laminoplasty. 4. Foraminotomy. 5. Discectomy. 6. Corpectomy.

PATIENT SYMPTOMS 1. Radicular pain, numbness, weakness, burning, or tingling in a dermatomal distribution indicating nerve root compromise.
2. Weakness or sensory loss in an extremity. 3. Uncontrolled severe pain.
FINDINGS ON CLINICAL EXAMINATION
Nerve root compromise in the distribution of a particular spinal nerve may cause the following:
1. Motor or sensory deficit. 2. Changes on reflex testing. 3. Positive findings on EMG testing. 4. Positive Spurling’s maneuver. 5. Intractable pain in a pattern consistent with a nerve root distribution.
DIAGNOSTIC EVIDENCE
For surgery to be considered, one of the following diagnostic tests must show evidence of nerve root compression:
1. MRI scan. 2. CT scan. 3. Myelogram with CT scan.
Source: Universe of Florida Patients with Neck Pain or Injury. Medical Practice Guidelines. Published by The Agency for Health Care Administration. March 1996: 9.
Surgical success can be measured by assessing the following in relation to pre-surgical status:
1. Pain. 2. Range of motion. 3. Functional ability. 4. Psychologic well-being. 5. Structural and neurologic status.
POST CERVICAL SURGERY TREATMENT OPTIONS
1. The application of heat or ice to the neck to relieve discomfort. 2. Medication:
a. Non-narcotic analgesics.
b. Muscle relaxants but not longer than one week.
c. NSAIDS if not contraindicated.
d. Narcotic analgesics on a short-term basis.
e. Antidepressants for chronic neck pain.

3. A home exercise program. 4. Patients exhibiting loss of functional ability may be prescribed physical therapy with a licensed professional physical or occupational therapist.
CHAPTER SUMMARY
Recent thinking has shifted away from bed rest as a viable treatment for neck pain.
Neck support of brief duration can be beneficial to some patients suffering from neck pain.
Non-steroidal anti-inflammatory drugs, non-narcotic analgesics, narcotic analgesics, and muscle relaxants have been found to relieve neck pain symptoms.
Traction is applied to the cervical spine in an effort to stretch muscles, ligaments, and spinal components.

CHAPTER SIX PREVENTION OF NECK PAIN FOR HEALTH CARE PROFESSIONALS
Programs designed to educate and prevent neck problems should be instituted in every
workplace. Suggested measures to reduce the risk of neck injury include following basic ergonomic strategy in the workplace and education of management and employees.
POSTURE
Good posture plays a significant role in the prevention of neck problems. Chronic poor posture greatly increases neck strain which, in turn, can induce myofascial pain. The following postural guidelines can help prevent worker injury.
POSTURAL GUIDELINES FOR THE PREVENTION OF CERVICAL PAIN
1. The cervical spine should be kept as straight as possible.
2. The head should be positioned directly above the shoulders; not protruded forward.
3. Cradling the telephone between the ear and shoulder should be avoided. A telephone receiver cradle should be used to maintain proper cervical spine alignment. If both hands are required for desk work, a telephone headset should be used.
4. The computer screen should be placed directly in front of the body to avoid chronic
rotation of the neck.
5. Office machines should be placed within comfortable reaching distances to reduce strain.
6. Physicians, massage therapists, and other health care workers should avoid hunching the shoulders when administering care to patients. Furthermore, prolonged lateral neck flexion and rotation should be avoided.
7. An ergonomically appropriate chair that allows for proper posture should be utilized.
8. Seat height should be adjusted allowing the elbows to rest comfortably to reduce

fatigue. Work activity should be at the same level as the elbows.
LIFTING SAFETY
Nurses, massage therapists, physical therapists, radiologic technicians, and other health care professionals who tend to lift patients on a frequent basis are at most risk for developing cervical and lumbar spine problems. Adherence to some basic safe lifting techniques can help prevent most injuries.
Some facilities institute a “no lifting policy.” This means that the manual lifting of
patients is prohibited, except in cases of emergency. Patients are encouraged to become more independent by helping to transfer themselves whenever possible. The rolling of patients can also be an alternative to lifting whenever possible and patients can be moved from bed to bed or bed to gurney using sliding aids.
There are four aspects of lifting that play a role in spinal stress. They include:
1. The amount and shape of the weight lifted. 2. The distance of the load from the torso. 3. Lifting of the load from ground level. 4. The speed in which the load is lifted.
ILLUSTRATION 5
EXAMPLE OF BAD LIFTING TECHNIQUE EXAMPLE OF GOOD LIFTING TECHNIQUE
Spinal stress can be lessened with simple lifting techniques.
1. When picking up an object from ground level, the knees should be bent and the

neck and back should be kept as straight as possible. 2. Keep the object close to the body to prevent undue strain on the discs. 3. Lift the object as quickly as possible to reduce strain on the annulus and ligaments. 4. Use common sense when deciding whether or not an object is safe weight-wise to lift. 5. When lifting, do not rotate the neck or twist the lumbar spine.
CHAPTER SIX SUMMARY
Programs designed to educate and prevent neck problems should be instituted in every workplace.
Good posture plays a significant role in the prevention of neck problems.
Nurses, massage therapists, physical therapists, radiologic technicians, and other health care professionals who tend to lift patients on a frequent basis are at most risk for developing cervical and lumbar spine problems.
Use common sense when deciding whether or not an object is safe weight- wise to lift.

GLOSSARY OF MEDICAL TERMS
ACUPUNCTURE - The ancient Chinese practice of inserting needles into specific body regions in an effort to relieve pain.
ANEMIA - A below normal reduction in erythrocytes (red blood cells) on hemoglobin (the oxygen carrier) in the blood.
ANNULUS FIBROSUS - A ring of the intervertebral disc composed of fibrous tissue and fibrocartilage.
ARTHRITIS – An inflammation of the joints caused by a variety of problems.
BIOFEEDBACK – Training technique which enables an individual to gain voluntary control over automatic body functions.
BONE SCAN - A test utilizing an intravenous injection and radiation helpful in detecting malignancy or infection involving any part of the skeleton.
BULGING DISC – When the nucleus pulposus presses against the annulus fibrosus producing an indentation as noted on spinal imaging.
CAUDA EQUINA - A group of spinal roots descending from the lower part of the spinal cord.
CHYMOPAPAIN – A papaya fruit-derived enzyme used as an injectable to dissolve herniated discs by chemonucleolysis.
COLCHICINE - An alkaloid commonly used to treat gouty arthritis.
COMPRESSION FRACTURES – Wedge-shaped broken bones caused by compression such as seen in the lumbar spine
CONTRAST MEDIA - A substance commonly used to emphasize the difference between light and dark on x-rays or scans to better visualize the organs and tissue.
CORTICOSTEROID - A steroid used clinically in many settings including hormone replacement therapy, antineoplastic, antiallergic, anti-inflammatory, and to suppress the immune system.
CHEMONUCLEOLYSIS – Dissolution of the nucleus pulposus of an intervertebral disc by injection of an agent such as chymopapain.
CRYOTHERAPY - Cold used for relief in treatment.
CT SCAN - Three-dimensional diagnostic test providing accurate density detail of internal organs.
DECOMPRESSIVE SURGERY – Excision of disc and bone to decrease anatomical irritation on the spinal cord or nerve roots.
DEEP TENDON REFLEXES - Involuntary muscle contraction following brief stretching caused by percussion of its tendon.

DEGENERATIVE ARTHRITIS - (Osteoarthritis) A noninflammatory degenerative joint disease most commonly found in the elderly causing pain and stiffness.
DERMATOMAL DISTRIBUTION - The extent of a nerve and its branches.
DIATHERMY - Warming of different parts of the body using high frequency electromagnetic radiation.
ELECTRODES - An object used between an electric source and the position to which the electric stimulus will be applied.
ELECTROMYOGRAM (EMG) - An electrodiagnostic test to detect neuromuscular disorders.
ENDORPHINS - Chemicals located in the brain and, when present, produce analgesic effects.
EPIDURAL INJECTION - Injection into or around the dura mater used for diagnostic or anesthetic purposes.
ERYTHROCYE SEDIMENTATION RATE (ESR) - Test using whole blood for detection of infection.
FIBROMYALGIA - Pain in fibrous tissue around a muscle.
FORAMINOTOMY – An operation performed to relieve nerve root compression by removing the roof of the intervertebral foramina.
HERNIATED DISC - A protrusion of the nucleus pulposus extending into or tearing part of the annulus fibrosus.
HYDROTHERAPY - The use of water therapeutically.
INFLAMMATORY ARTHRITIS - Also known as degenerative arthritis.
IMMUNOSUPPRESSION - Suppression of the immune system.
LAMINECTOMY – Surgical removal of the posterior arch of a vertebra.
LAMINOTOMY – Splitting of the lamina of a vertebra.
LIGAMENT - A band of tissue that connects bones to joints.
METASTATIC DISEASE - Disease that is transferred from one part of the body to another not connected to the original part of the body.
MRI SCAN - (Magnetic resonance imaging) - A diagnostic test, when directed at the lumbar spine, can detect herniation, lumbar canal stenosis, infection, tumor, or other pathology affecting the lumbar spine.
MUSCLE ATROPHY - Wasting away of a muscle.
MULTIPLE MYELOMA - A plasma cell cancer characterized by multiple bone marrow tumors, fractures, hypercalcemia, and anemia.

MYELOGRAPHY - Testing used to visualize the spinal cord by injecting contrast media into the subarachnoid space via spinal needle.
MYELOPATHY - A general term denoting pathology in the spinal cord or bone marrow.
MYOFASCIAL PAIN– Pain due to muscle and surrounding connective tissue irritation.
NONSTEROIDAL ANTIINFLAMMATORY DRUG (NSAID) - Medication that counteracts inflammation.
OSSEOUS– Relating to bone.
OSTEOARTHRITIS – Arthritis from aging, trauma, wear, and tear. Also known as degenerative arthritis.
OSTEOCLASTIC - Destruction of bone by cellular activity.
OSTEOPOROSIS - A significant reduction in bone mass which can result in fractures.
RADICULOPATHY - An abnormality with the base of a nerve.
REFLEXES – Involuntary muscle contraction following brief stretching caused by percussion of a tendon.
SERUM CALCIUM - A blood test used to detect conditions such as hyperparathyroidism and malignancy.
SPINAL MANIPULATION - Passive movement of the bones of the vertebrae by hand used to increase flexibility and decrease pain.
SPINAL STENOSIS - Narrowing of the vertebral openings.
SPINAL TRACTION - The pulling by force of the vertebrae.
TRIGGER POINT INJECTION – Injection of local anesthetic with or without corticosteroid to digitally palpable tissue texture abnormality.
ULTRASOUND – High frequency crystal-induced sound waves to induce heat below the skin surface.

REFERENCE LIST
1. Gam, Arne Nyholm and Johannsen, Finn. “Ultrasound Therapy in Musculoskeletal Disorders: A Meta-Analysis.” Pain. 63 (1995): 85-91.
2. Nachemson, AL. “Lumbar Disc Herniation: Conclusions.” (University of Gothenburg, Sweden: Acta Orthop Scand 64:59S-50S, 1993.
3. Rydevik, B. “Spinal Stenosis: Conclusions.” Acta Orthop Scand 64- 81S-82S, 1993.
4. Assendelft, WJ and Bouter, LM and Knipschild, PG. “Complications of Spinal Manipulation: A Comprehensive Review of the Literature.” The Journal of Family Practice. Vol. 42, No. 5 (May 1996): 475-480.
5. Barker, ME. “Spinal Manipulation: A General Practice Study.” The Journal of Orthopaedic Medicine. Vol. 16, No. 2. (1994): 42-44.
6. Broadhurst, NA and Wilk, VJ. “Vertebral Mid-Line Pain: Pain Arising from The Interspinous Spaces.” The Journal of Orthopaedic Medicine. 18(1) 1996: 2-4.
7. Kroll, Dorothy. “Alternative Therapies for Chronic Pain Management.” Alternative & Complementary Therapies. (January/February 1996): 5- 8.
8. Jensen, MC and Brant-Zawadzki, MN and Obuchowski, N and Modic, MT and Malkasian D and Ross, JS. “Magnetic Resonance Imaging of the Lumbar Spine in People Without Back Pain.” (Hoag Mem Hosp, Newport Beach, Calif; Cleveland Clinic, Ohio) New England Journal of Medicine. (1994) 331:69-73.
9. Schneck, Carson D. “Functional and Clinical Anatomy of the Spine.” Physical Medicine and Rehabilitation: State of the Art Reviews. Vol. 9, No. 3. (October 1995): 571-603.
10. Garfin, Steven R. “Conservative Management for Spondylolysis and Spondylolisthesis.” The Journal of Musculoskeletal Medicine. (June 1996): 11-12.
11. Hanley, Edward N. “Low Back Pain: Help from Corticosteroids, but not Prolotherapy or Colchicine.” The Journal of Musculoskeletal Medicine. (March 1996): 15.
12. Borenstein, David and Wiesel, Sam and Boden, Scott. Neck Pain: Medical Diagnosis and Comprehensive Management. 1st Edition.
W.B. Saunders and Company, 1996.
13. Giles, LGF and Singer, KP Editors. Volume 3: Clinical Anatomy and Management of Cervical Spine Pain. Reed Educational and Professional Publishing Ltd, 1998.
14. Panjabi, MAMMOGRAM and Vasavada, A and White, AA III. Biomechanics of Cervical Spine and Whiplash Injuries. Seminars in Spine Surgery, Vol 10, No 2 (June), 1998: pp 141-149.

15. Blackburn, Dennis. Neck Pain: It Could Be Cervical Osteomyelitis. Journal of the American Osteopathic Academy of Orthopedics, Vol 35, No 2, 1998: p 36.
16. Barnsley, L and Lord, S and Bogduk, N. The Pathophysiology of Whiplash. SPINE: State of the Art Reviews. Vol 12, No2, 1998: pp 209-242.
17. Rogers, Carcinoma and Joshi, A and Dreyfuss, P. Cervical Intrinsic Disc Pain and Radiculopathy. SPINE: State of the Art Reviews. Vol 12, No 2, 1998: pp 323-356.
18. O’Malley, Thomas and Kamkar, Abdulazeem. Manual Examination and Treatment of the Cervicothoracic Region. Orthopaedic Physical Therapy Clinics of North America. 7:4 December 1998: pp 499-503.
19. Vaccaro, A and Cook, C, and McCullen, G and Garfin, S. Cervical Trauma: Rationale for Selecting the Appropriate Fusion Technique. The Orthopedic Clinics of North America. Vol 29, No 4, 1998: pp 745- 754.
20. Czervionke, Leo and Berquist, Thomas. Imaging of the Spine: Techniques of MR, Imaging. The Orthopedic Clinics of North America. Vol 28, No 4, 1997: pp 583-616.
21. Garfin, Steven. Editorial: Spine Focus – Cervical Spine. SPINE. Vol 23, No 24, 1998: pp 2661-2662.
22. Grob, Dieter. Surgery in the Degenerative Cervical Spine. SPINE. Vol 23, No 24, 1998: pp 2674-2683.
23. Kaiser, Jay and Holland, Betsy. Imaging of the Cervical Spine. SPINE. Vol 23, No 24, 1998: pp 2701-2712.
24. Dreyer, Susan and Boden, Scott. Nonoperative Treatment of Neck and Arm Pain. SPINE. Vol 23, No 24, 1998: pp 2746-2754.
25. Abdu, William and Provencher, Lt. Matthew. Primary Bone and Metastatic Tumors of the Cervical Spine. SPINE. Vol 23, No 24, 1998: pp 2767-2777.
26. I. Jeffreys, Eurig, Editor. Disorders of the Cervical Spine – 2Rev. ed. Butterworth-Heinemann Ltd. 1993.
27. Praemer A, Furner S, Rice DP: Musculoskeletal Conditions in the United States. Illinois: American Academy of Orthopaedic Surgeons 1992, pages 23-33.
28. Hagberg M, Wegman DH: Prevalence rates and odds ratios of shoulder-neck diseases in different occupational groups. Br J Ind Med 44-602, 1987.
29. University of Florida Patients with Neck Pain or Injury. Medical Practice Guidelines. Published by The Agency for Health Care Administration. March 1996: 1-10.
30. Florida Neck Pain and Injury Guideline. Quality Effectiveness/Cost Saving Measures. Published by The Agency for Health Care Administration. March 1996: 1-4.