Embed Size (px)
Citation preview

Current State of Blindness in Ghana and SiB
Boateng Wiafe,
Regional Director for Africa
Oscar Debrah
Head, Eye Care Unit, Ghana Health Service
KATH
KUMASI
FEBRUARY 2014

Causes of Blindness
Cataract 45 – 50% Glaucoma 15 – 20% Trachoma 5% Onchocerciasis 5% Childhood Blindness 5 -10% Refractive Errors & Low Vision 5% Others 10 –
15%
Human Resource Development
Ophthalmologists – Trained by Ghana Postgraduate College
Optometrists – Doctors in Optometry (OD). Trained in Kumasi and Cape Coast
Ophthalmic Nurses – Trained at Ophthalmic Nursing School in Korle Bu
Optical Technicians – Trained at Oyoko

Human Resource Ophthalmologists 74 Optometrists 150 Ophthalmic Nurses 420 Low Vision Specialist 1
Distribution of personnel (especially ophthalmologists and optometrists) skewed towards Accra and Kumasi.
No ophthalmologist in Upper West Region. One each in Volta, BA and Upper East Regions

HR in Eye Health in Ghana
Skewed Distribution of Eye Health workforce

Disease Control Cataract
Trachoma Control Programme
Childhood Blindness
Refractive Error & Low Vision Services

Cataract Services
Provided at both static and outreach centres
Cataract surgery covered under the National Health insurance Scheme (NHIS) which started in 2005
CSR in 2012 was 819
Total cataract surgeries in 2012 = 19860

5-Year CSR Trend

2012 CSR
Trachoma Control Programme
Trachoma was endemic in two regions, Northern and Upper West
Using ‘SAFE’ strategy for control, which started in 2000
Targeted 2010 for the elimination of blinding trachoma
Trachoma Control Programme
Trachoma was endemic in two regions, Northern and Upper West
Using ‘SAFE’ strategy for control, which started in 2000
Targeted 2010 for the elimination of blinding trachoma

Prevalence of Active Trachoma (Baseline & After Intervention)
2.8
2.8
3.2
3.5
3.6
3.7
3.8
4.4
5
5.7
6.7
6.8
8.2
9.7
11.5
11.7
12.4
16.1
0 2 4 6 8 10 12 14 16 18
Lawra
E Mamprusi
Sab Cherep
Yendi
Nadowli
E Gonja
Nanumba
Gushiegu K
J/Lambussie
Tamale
Zab/Tat
West Mamp
Bole
Savelugu/Nanton
Sissala
West Gonja
Tolon/Kunbumgu
Wa
Prevalence (%)

Trachoma Control Programme
3rd year of Trachoma Surveillance in the 2 Regions.
Epidemiological Prevalence Survey to be conducted next year, which will lead to applying for declaration of Ghana being free from Blinding Trachoma

Childhood Blindness Prevention
Paediatric Ophthalmology Units in Korle Bu and Komfo Anokye Teaching Hospitals
Trained ophthalmic nurses in Childhood Blindness prevention
Lions Club International/WHO supporting Korle Bu Paediatric Unit to set up a satellite centre at Weija

Refractive Error & Low Vision Services
Refractive Error Services mostly in the private sectors. Teaching and some Regional Hospitals also render service
2 Low Vision Centres set up in 2 regions (Greater Accra and Eastern).
National Low Vision Coordinator in the office of Eye Care Unit. Used to be supported by CBM but support ended in 2010

Challenges No National Prevalence of Blindness Survey
done Integration of PEC into Regional and District
Health Service delivery Inadequate and inequity in distribution of eye
care personnel especially ophthalmologists and optometrists
Sub-specialty for ophthalmologists Low National Cataract Surgical Rate (CSR) Inadequate resource for eye health activities Data collection

No National Prevalence Survey done
Data we use are extrapolated A RAAB conducted in the Eastern Region in
2009 funded by Sightsavers revealed a prevalence of blindness of 0.7
The Faculty of Public Health, Swiss Red Cross and OE are planning on a National Survey but the funds are not adequate so we will sample from each of the 3 ecological zones and have a snap shot of the prevalence and causes of blindness in Ghana
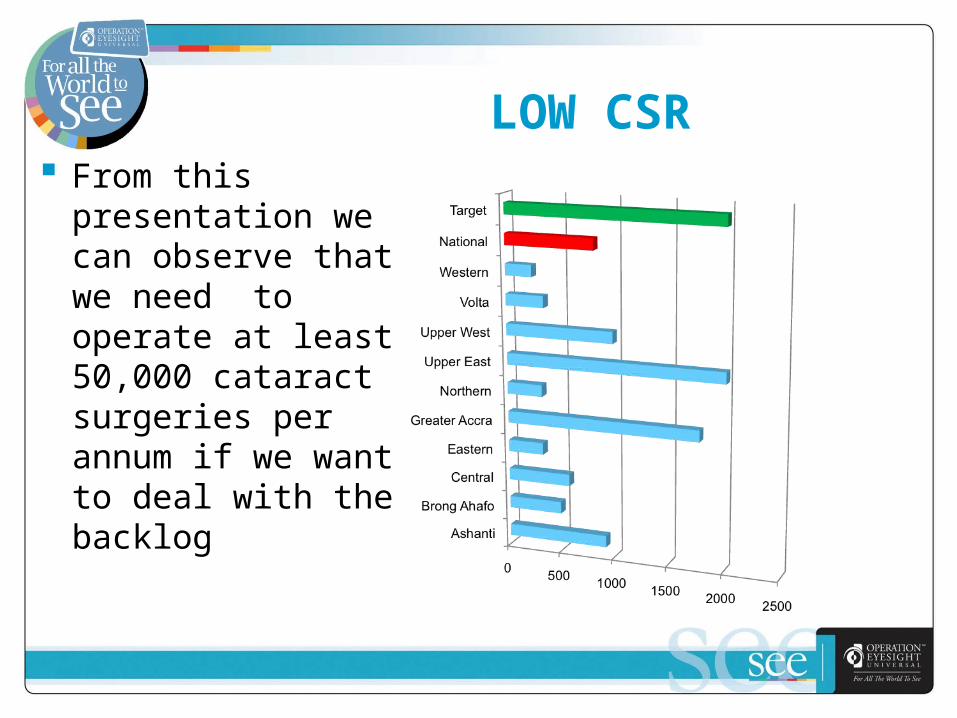
LOW CSR From this
presentation we can observe that we need to operate at least 50,000 cataract surgeries per annum if we want to deal with the backlog
OUR APPROACH In Partnership with the Standard Chartered
Bank, Seeing is Believing we decided to
REMOVE BARRIERS TO QUALITY EYE CARE IN GHANA BY
a) Strengthening the district level eye care, making it robust enough to take referrals from the community
b) Empower the frontline health workers and volunteers through capacity building

Strengthening the District Level Eye Services
Infrastructure Development – • Constructed and Renovated Eye Clinics
Equipment provision – • Equipped 24 District Hospitals with Diagnostic
Equipment to make them functional
• Provision of 7 Surgical Sets to 7 regions - Operating Microscopes, Biometry Equipment, Surgical Instruments
Capacity Building - • Retraining of the Ophthalmic Nurses on how to use
the equipment provided

Capacity building – • Training of instruments technicians and
equipping them with tool kits
• Training the Ophthalmic Nurses to be trainers of others
Service Delivery enhancement:• SiB offered consumables for cataract services
for as many surgeries as would be required for the first year and then decline as the year goes by , an attempt to assist in sustainability

Outcome of the intervention Infrastructure Development:
• 2 new eye clinics were constructed - Bibiani and Weija
• 3 Eye Clinics refurbished – Takoradi Government Hospital, Worawora district Hospital and Tokurano Clinic
Human Resource Development• 42 Ophthalmic Nurses
• 10 Optometrists
• 12 Equipment Technicians
• 1361 PEC workers trained

Service Delivery
1. 240,664 patients screened and treated
2. Community Awareness program through the mass media
3. Surgeries – low productivity (27%)a) Only 31% of the 10,969 cataract surgeries have
been delivered
b) Only 11% of the 4388 major surgeries have been delivered
c) Only 40% of the 6581 minor surgeries have been delivered

Discussion
Several of the partners have never delivered any surgery at all
Those who do something are grossly underperforming
Only about 7 or so partners are delivering There is surgical instruments available,
consumables are available, patients are available
The blind patients are not converted to seeing

Recommendations
Districts should be adopted by Ophthalmic Teams from the teaching hospitals• Surgical Visits should be once a month and if a
regular visit is made and a target is set at not less than 20 cases per day in a year we can reach at least 200 – 250 cases.
• If it becomes busy, then the frequency can be increased.
• We should not treat this as a part time work outside our normal duties, activities done over the weekends.

Recommendations
Districts that have been equipped and not generating any surgeries may have to surrender their equipment to district hospitals that are prepared to deliver.• It is unethical to tell someone that he has a
problem and not do anything about it.

Any suggestions?
1. …….
2. …….
3. ……….

Partners in Eye Care
Sightsavers CBM SRC OEU HCP GEF
Rotary Club Lions Club Standard
Chartered Bank (“Seeing is Believing”)
Orbis

Thank you