Embed Size (px)
Citation preview

Curriculum for the Hospitalized Aging Medical Curriculum for the Hospitalized Aging Medical PatientPatient
CHAMPCHAMP Drugs and Aging Drugs and Aging
Paula M. Podrazik, MDPaula M. Podrazik, MD
University of ChicagoUniversity of Chicago

Case of Mrs. T…..Case of Mrs. T…..
• • 85 y/o with h/o DM, CHF, lumbar spinal stenosis admitted with increasing 85 y/o with h/o DM, CHF, lumbar spinal stenosis admitted with increasing confusion and falls. Lives alone, daughter involved. Daughter notes patient confusion and falls. Lives alone, daughter involved. Daughter notes patient h/o anxiety but c/o insomnia and phoning her continuously throughout the h/o anxiety but c/o insomnia and phoning her continuously throughout the night for the past 3 nights.night for the past 3 nights.
• • Brought to U of C ER by daughter after a witnessed fall. New patient to Brought to U of C ER by daughter after a witnessed fall. New patient to the U of C system. Admitted at 3AM to telemetry. the U of C system. Admitted at 3AM to telemetry.
• • On exam, alternately agitated and somnolent, oriented to person only.On exam, alternately agitated and somnolent, oriented to person only. VS: T99, P54, RR20, BP110/50 lying supine wt. 100lbs. 5’1”VS: T99, P54, RR20, BP110/50 lying supine wt. 100lbs. 5’1” Cor: RRR, +SCor: RRR, +S33 Lungs: dry crackles in basesLungs: dry crackles in bases Abd: soft, nontender, nondistended, firm stool felt throughout colonAbd: soft, nontender, nondistended, firm stool felt throughout colon
• • ER data:CT head neg., dirty urine, CXR with ER data:CT head neg., dirty urine, CXR with cor, KUB FOS, BUN 48/CR cor, KUB FOS, BUN 48/CR 2.7, glc= 74, K2.7, glc= 74, K++ hemolyzed at 6.3 F/U pending,INR=3.0, EKG SB-rate 58, no hemolyzed at 6.3 F/U pending,INR=3.0, EKG SB-rate 58, no peaked t waves. Given dose IV antibiotics in ER.peaked t waves. Given dose IV antibiotics in ER.

Case of Mrs. T…..Case of Mrs. T…..
Meds:Meds:Lisinopril 40mg q dailyLisinopril 40mg q dailyGlipizide ER 20mg BIDGlipizide ER 20mg BIDLasix 40 mg q dailyLasix 40 mg q dailyKCL 20 meq q dailyKCL 20 meq q dailyPaxil 20 mg q dailyPaxil 20 mg q dailyAmiodarone 200mg q dailyAmiodarone 200mg q dailyDigoxin 0.25 mg q dailyDigoxin 0.25 mg q dailyCoumadin 5mg q dailyCoumadin 5mg q dailyT#3 prnT#3 prnAtivan 1mg prnAtivan 1mg prnUnsom (OTC) prn sleepUnsom (OTC) prn sleepLomotil (OTC) prnLomotil (OTC) prnSenna and colace prnSenna and colace prn

Questions Raised….Questions Raised….
• Why is this patient on so many meds?Why is this patient on so many meds?• Could some of these meds be causing Could some of these meds be causing
her decline?her decline?• What is involved in medication What is involved in medication
management in the aging population?management in the aging population?• Why is medication management so Why is medication management so
difficult in this population?difficult in this population?• Are there principles help guide Are there principles help guide
medication management?medication management?

Drugs and Aging: Topics for Drugs and Aging: Topics for ReviewReview
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• PolypharmacyPolypharmacy
• Drugs to Avoid Drugs to Avoid
• Adverse Drug Reactions Adverse Drug Reactions
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• PolypharmacyPolypharmacy
• Drugs to Avoid Drugs to Avoid
• Adverse Drug Reactions Adverse Drug Reactions
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

Older patients under-represented in drug Older patients under-represented in drug trialstrials
• Statins: 47 RCTsStatins: 47 RCTs– Only 1/3 reported proportion of Only 1/3 reported proportion of
patients >65 yearspatients >65 years– Median % of patients >65 in US trials Median % of patients >65 in US trials
was 21.1%was 21.1%• Acute Coronary SyndromesAcute Coronary Syndromes
– Of patients hospitalized for ACS in Of patients hospitalized for ACS in 1995, 37% were >75 years1995, 37% were >75 years
– Only 9% of patients in ACS trials 1991 Only 9% of patients in ACS trials 1991 to 2000 were >75 yearsto 2000 were >75 years
Bartlett, et al. Heart 2003; 89: 327-328.

Adverse Drug Events, Research Adverse Drug Events, Research and Agingand Aging
• Elderly excluded from investigational trials• small sample sizes Phase III trials• exclusion criteria=vulnerable elder•“in vivo” no look at drugs in combo
• Under-reporting of drug safety problems Schmucker DL, et al:J Clin Pharmacol 1999;39:1103-8 Avorn J: Br Med J 1997;315:1033-1034

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• Adverse Drug Reactions Adverse Drug Reactions
• Drugs to AvoidDrugs to Avoid
• PolypharmacyPolypharmacy
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

Aging Pharmacology:Aging Pharmacology:ObjectivesObjectives
• DefinitionsDefinitions• PharmacokineticsPharmacokinetics
– Aging & drug absorptionAging & drug absorption– Aging drug distributionAging drug distribution– Aging & Drug ClearanceAging & Drug Clearance
• Renal MetabolismRenal Metabolism• Hepatic BiotransformationHepatic Biotransformation
• PharmacodynamicsPharmacodynamics

Drug Absorption with Normal AgingDrug Absorption with Normal Aging
in gastric pH, motility, absorptive surfacein gastric pH, motility, absorptive surface gastric emptying timegastric emptying time• May see slower absorption, May see slower absorption, time to effect time to effect
Bottom line: No clinically sign. age-related Bottom line: No clinically sign. age-related change in drug absorption with normal change in drug absorption with normal aging.aging.

Drug Distribution with AgingDrug Distribution with Aging
body fat to age 60-70body fat to age 60-70 antipsychotics, antipsychotics, TCAsTCAs
in lean body mass and fat after 70in lean body mass and fat after 70 digoxin conc.digoxin conc.
protein-binding can effect Vd protein-binding can effect Vd warfain + warfain + amiodarone, phenytoin, ketaconazoleamiodarone, phenytoin, ketaconazole
Bottom Line: Drug dosing is a dynamic Bottom Line: Drug dosing is a dynamic process with aging.process with aging.

Hepatic Biotransformation and Hepatic Biotransformation and Aging Aging
• Age- related declineAge- related decline– Reduction in liver blood flowReduction in liver blood flow
• High-clearance drugs affected: propanolol, High-clearance drugs affected: propanolol, labetolol, esmolol, lidocainelabetolol, esmolol, lidocaine
– Reduction in hepatic oxidation: CYP450Reduction in hepatic oxidation: CYP450
• No age-related changesNo age-related changes– Hepatic acetylationHepatic acetylation– Hepatic conjugationHepatic conjugation

Cytochrome P450 SystemsCytochrome P450 Systems
• CYP3ACYP3A– Metabolizes >60% of prescribed drugs Metabolizes >60% of prescribed drugs
including: Calcium channel blockers, certain including: Calcium channel blockers, certain beta-blockers, most “statins”, warfarin, beta-blockers, most “statins”, warfarin, amiodaroneamiodarone
• CYP2D6CYP2D6– Metabolizes: metoprolol, propranolol, tramadol, Metabolizes: metoprolol, propranolol, tramadol,
codeine,oxycodone,TCAs, SSRIscodeine,oxycodone,TCAs, SSRIs

Cytochrome P450 InhibitorsCytochrome P450 Inhibitors
• CYP3A InhibitorsCYP3A Inhibitors– Amiodarone, cimetadine, cyclosporin, Amiodarone, cimetadine, cyclosporin,
erythromycin, erythromycin, itra-/ketoconazole,grapefruit juiceitra-/ketoconazole,grapefruit juice
• CYP2D6 InhibitorsCYP2D6 Inhibitors– Cimetidine, SSRIs, quinidineCimetidine, SSRIs, quinidine

Renal Clearance and AgingRenal Clearance and Aging
• ~ age 40~ age 40, renal func. declines 1% per year, renal func. declines 1% per year• Normal serum Cr Normal serum Cr normal GFR normal GFR• Estimate using Cockcroft-Gault equationEstimate using Cockcroft-Gault equationCreatinine clearance =Creatinine clearance =
((140-age) * Wt (kg) 140-age) * Wt (kg) ( ( 0.85 in women) 0.85 in women)
72 * serum Cr72 * serum Cr
• Modified MDRDModified MDRD
GFR estimate=GFR estimate= 186x(Cr)186x(Cr)-1.154-1.154x (Age)x (Age)-0.203-0.203x (0.742, if female) x (1.21, if x (0.742, if female) x (1.21, if
African American)African American)

Aging PharmacodynamicsAging Pharmacodynamics
With aging:With aging:• Beta-adrenergic responsiveness Beta-adrenergic responsiveness • Anticholinergic drugs Anticholinergic drugs CNS effects CNS effects• Baroreceptor reflex bluntedBaroreceptor reflex blunted

Medication use based on aging Medication use based on aging pharmacology principlespharmacology principles
• Start low, go slow, dose to effectStart low, go slow, dose to effect• Adjust for decrease in renal clearance Adjust for decrease in renal clearance • ID drugs w/narrow toxic/therapeutic ID drugs w/narrow toxic/therapeutic
indexindex• ID drugs that effect CPY450 system e.g., ID drugs that effect CPY450 system e.g.,
inhibitors/inducersinhibitors/inducers• Adjust for anticholinergic properties of Adjust for anticholinergic properties of
drugsdrugs• Remember the blunted barorecepter Remember the blunted barorecepter
reflexreflex

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• PolypharmacyPolypharmacy
• Adverse Drug ReactionsAdverse Drug Reactions
• Drugs to AvoidDrugs to Avoid
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

Case of Mrs. K…..Case of Mrs. K…..
75 y o F with CAD, HTN, OP, LBP75 y o F with CAD, HTN, OP, LBPWalks 1 mile 3x per week & Tai Chi 2x per week & water Walks 1 mile 3x per week & Tai Chi 2x per week & water
aerobics class 1x per weekaerobics class 1x per weekMed list:Med list: asa 81 q dayasa 81 q day lisinopril 20 q daylisinopril 20 q day atenolol 25 q dayatenolol 25 q day hctz 25 q dayhctz 25 q day lipitor (atorvastatin) 10 q daylipitor (atorvastatin) 10 q day fosamax (alendronate) 70 mg q weekfosamax (alendronate) 70 mg q week MVI q dayMVI q day tums 3 q daytums 3 q day vicodin (hydrocodone/acetaminophen) prnvicodin (hydrocodone/acetaminophen) prn

What is the prevalence of drug What is the prevalence of drug use in the elderly? use in the elderly?
• Ambulatory adults Ambulatory adults >> 65 surveyed 65 surveyed– 12% take > 10 meds12% take > 10 meds– 50% take 5 or > meds50% take 5 or > meds
Kaufman DW, et al The Slone survey. JAMA 2002;287:337..

2040 projections 2040 projections >> 65 = 65 = 20% of population & 20% of population & consume 50% prescribed medsconsume 50% prescribed meds

Will polypharmacy continue to Will polypharmacy continue to escalate?escalate?

Factors that influence Factors that influence prescribing in the elderlyprescribing in the elderly
– More chronic conditions w/advancing More chronic conditions w/advancing ageage
– Newer Rx for diseases (e.g., Newer Rx for diseases (e.g., Alzheimer’s)Alzheimer’s)
– Wider indications for CV drugsWider indications for CV drugs– Lower thresholds @ which diseases Rx’d Lower thresholds @ which diseases Rx’d
(e.g., hypercholesterolemia)(e.g., hypercholesterolemia)– Increased use of primary/secondary Increased use of primary/secondary
preventionpreventionKaufman DW, et al. JAMA. 2002;287:337.

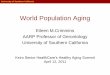
Drug Interactions Drug Interactions with 5 or > with 5 or > drugsdrugs
Hazzard, Principles of Geriatric Medicine and Gerontology

Polypharmacy definitions?Polypharmacy definitions?
• > > 5 medications used5 medications used• Concurrent use of multiple prescriptions & Concurrent use of multiple prescriptions &
over-the-counter medsover-the-counter meds• Definitions w/measure of Definitions w/measure of
""appropriatenessappropriateness""– Use of one med to treat adverse effects of Use of one med to treat adverse effects of
anotheranother– Medical regimen includes Medical regimen includes >> one one unnecessary unnecessary
medmed– Use of more meds than clinically indicatedUse of more meds than clinically indicated

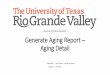
Polypharmacy & Adverse Drug Polypharmacy & Adverse Drug ReactionsReactions
Rochon PA, Gurwitz JH BMJ 1997;315:1097

What is the risk of What is the risk of polypharmacy?polypharmacy?
• Risk of drug-drug interactions Risk of drug-drug interactions increases with increasing # of medsincreases with increasing # of meds
• Up to 73% of ADRs involved Up to 73% of ADRs involved unnecessary medsunnecessary meds
• 10-17% of hospital admissions due to 10-17% of hospital admissions due to ADEsADEs
Bergendal L, et al. Pharm World Sci. 1995;17:152.Lindley CM. et al. Age Ageing. 1992;21:294.Beard K. Drugs Ageing. 1992;2:356.

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• PolypharmacyPolypharmacy
• Drugs to AvoidDrugs to Avoid
• Adverse Drug ReactionsAdverse Drug Reactions
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

Explicit Criteria --BeersExplicit Criteria --Beers
• List of medications to avoid in elderly List of medications to avoid in elderly nursing home patients nursing home patients
• Developed by consensus panel in Developed by consensus panel in 19911991
• Updated in 1997 and 2002Updated in 1997 and 2002
Beers, et al. Arch Intern Med 1991; 151: 1825-1832.
Beers MH. Arch Intern Med 1997; 157(14): 1531-1536.
Fick DM, et al. Arch Int Med 2003; 163: 2716-24.

Drugs to Avoid in the ElderlyDrugs to Avoid in the Elderly
Drug Classes/DrugsDrug Classes/Drugs• antihistaminesantihistamines• antispasmodicsantispasmodics• certain CV medscertain CV meds
– methyldopa, (Aldometmethyldopa, (AldometTMTM), reserpine), reserpine– disopyramide (Norpacedisopyramide (NorpaceTMTM))– dipyridamole (Persantinedipyridamole (PersantineTMTM))
• certain psychotropicscertain psychotropics– amitriptyline( Elavilamitriptyline( ElavilTMTM), doxepin (Sinequan), doxepin (SinequanTMTM))– meprobamate(Miltownmeprobamate(MiltownTMTM), diazepam, ), diazepam, flurazepam (Dalmaneflurazepam (DalmaneTMTM), barbs), barbs
Beers MH Arch Intern Med 1997;157:1531-1536Beers MH Arch Intern Med 1997;157:1531-1536

Drugs to Avoid in the ElderlyDrugs to Avoid in the Elderly
Drug Classes/DrugsDrug Classes/Drugs• certain analgesicscertain analgesics
– propoxyphene (Darvonpropoxyphene (DarvonTMTM))– merperidine (Demerolmerperidine (DemerolTMTM))– pentazocine (Talwinpentazocine (TalwinTMTM))
• chlorpropamide (Diabenasechlorpropamide (DiabenaseTMTM))• trimethobenzamide (Tigantrimethobenzamide (TiganTMTM))• certain anti-inflammatory agentscertain anti-inflammatory agents
– indomethacin (Indocinindomethacin (IndocinTMTM),ketorolac (Toradol),ketorolac (ToradolTMTM), ), piroxicam(Feldenepiroxicam(FeldeneTMTM))
Beers MH Arch Intern Med 1997;157:1531-Beers MH Arch Intern Med 1997;157:1531-15361536

Interactions to BewareInteractions to Beware
Drug-Disease Interactions to AvoidDrug-Disease Interactions to Avoid dementia, falls + benzodiazepinesdementia, falls + benzodiazepines BPH, constipation + antihistamines, BPH, constipation + antihistamines, antispasmodics, TCAsantispasmodics, TCAs CRF, CHF, PUD + NSAIDSCRF, CHF, PUD + NSAIDS DM + steroidsDM + steroids asthma, COPD, PVD, HB + beta blockersasthma, COPD, PVD, HB + beta blockers
Beers MH Arch Intern Med Beers MH Arch Intern Med 1997;157:1531-15361997;157:1531-1536

Limitations of Explicit Limitations of Explicit CriteriaCriteria
• Clinical relevanceClinical relevance– Many medications outdated or not used Many medications outdated or not used – Requires update by consensus panel Requires update by consensus panel
• Validity of dataValidity of data– Criteria developed from nursing home Criteria developed from nursing home
datadata– Applied in many unvalidated settingsApplied in many unvalidated settings
• Room for clinical judgement?Room for clinical judgement?
Buetow SA, et al. Soc Sci Med 1997; 45(2): 261-271.

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• PolypharmacyPolypharmacy
• Drugs to AvoidDrugs to Avoid
• Adverse Drug ReactionsAdverse Drug Reactions
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

ADR/ADE--definedADR/ADE--defined
• Adverse Drug Reaction (ADR)Adverse Drug Reaction (ADR)any undesirable or noxious drug effect at any undesirable or noxious drug effect at
standard drug treatment dosesstandard drug treatment doses WHO;1996 Technical Report Series No. 425WHO;1996 Technical Report Series No. 425
• Adverse Drug Event (ADE)Adverse Drug Event (ADE)ADRs + errors in drug administrationADRs + errors in drug administration

ADRsADRs
ADRs
Amplified drug effects
Drug-nutrient interaction
Drug-drug interaction
Drug-disease interaction
Side-effects
*not therapeutic failures*not ADWEs

ADR Risk FactorsADR Risk Factors
Carbonin P, et al JAGS 1991;39:1093-1099

ADR Risk FactorsADR Risk Factors
? prior ADRs
high risk drugs
# of drugs
# medical problems
? aging pharm
? fragmented care
AdverseDrug
Reaction

ADEs and HospitalizationADEs and Hospitalization
Recent inhospital studies look at ADEsRecent inhospital studies look at ADEs How big a problem?How big a problem?
• 4th-6th leading cause of hospital death 4th-6th leading cause of hospital death (serious ADRs 6.2%, fatal ADRs 0.32%)(serious ADRs 6.2%, fatal ADRs 0.32%)
• Increased length of stayIncreased length of stay• Increased costIncreased cost
Lazarou J, et al JAMA 1998; 280(20):1741-44Lazarou J, et al JAMA 1998; 280(20):1741-44 Classen D, et al JAMA 1997; 277(4): 301-6Classen D, et al JAMA 1997; 277(4): 301-6

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• Adverse Drug Reactions Adverse Drug Reactions
• Drugs to AvoidDrugs to Avoid
• PolypharmacyPolypharmacy
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

Drugs and Aging:Drugs and Aging: Cost Cost
• Important to ask: “How do you pay for Important to ask: “How do you pay for your medications?”your medications?”
• Federal poverty level: $10,400 for Federal poverty level: $10,400 for individual, $14,000 for coupleindividual, $14,000 for couple
• Potential sources of aid: Medicare Part D, Potential sources of aid: Medicare Part D, Medicaid, Circuit Breaker, Illinois Care Medicaid, Circuit Breaker, Illinois Care Rx, Rx buying club, manufacturer-Rx, Rx buying club, manufacturer-sponsored programssponsored programs

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• Adverse Drug Reactions Adverse Drug Reactions
• Drugs to AvoidDrugs to Avoid
• PolypharmacyPolypharmacy
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

ComplianceCompliance
• Compliance Adherence ConcordanceCompliance Adherence Concordance• Non-adherence 25 to 59% in the elderlyNon-adherence 25 to 59% in the elderly• Factors associated with non-adherenceFactors associated with non-adherence
– Physical impairmentPhysical impairment– Psychosocial risksPsychosocial risks– Medication related factorsMedication related factors
• Higher risk of re-hospitalization Higher risk of re-hospitalization • Risk of noncompliance after dischargeRisk of noncompliance after discharge
Ryan AA. Int’l J Nursing Studies 1999; 36: 153-62.
Van Eijken M, et al. Drugs & Aging 2003; 20: 229-40.

Drugs and AgingDrugs and Aging
• Information GapInformation Gap
• Aging PharmacologyAging Pharmacology
• Adverse Drug Reactions Adverse Drug Reactions
• Drugs to AvoidDrugs to Avoid
• PolypharmacyPolypharmacy
• CostCost
• ComplianceCompliance
• Medication ReviewMedication Review

Strategies for improving quality Strategies for improving quality of medication use in the elderlyof medication use in the elderly
• Medication ReviewMedication Review– Implicit criteria vs. explicit criteriaImplicit criteria vs. explicit criteria
• Enlisting the pharmacistEnlisting the pharmacist• Use of the CPOEUse of the CPOE• Enlisting the patient Enlisting the patient • Simplifying administrationSimplifying administration
– PolypillPolypill– Single daily dosingSingle daily dosing– Pill organizersPill organizers

Medication ReviewMedication Review• Explicit criteriaExplicit criteria
– Drugs/classes of drugs w/high risk/ low Drugs/classes of drugs w/high risk/ low benefitbenefit
– U.S. example: Beers drugs-to-avoid criteriaU.S. example: Beers drugs-to-avoid criteria• Requires updatingRequires updating• Validity of data in other settings?Validity of data in other settings?• ? Room for clinical judgment/ ? Room for clinical judgment/ ""patient-patient-
centeredcentered"" care care
• Implicit criteriaImplicit criteria– IDs individual elements of prescribing as IDs individual elements of prescribing as
inappropriate e.g., MAIinappropriate e.g., MAI– Time consuming, pharmacist drivenTime consuming, pharmacist driven
Fick DM, et al. Arch Int Med. 2003;163:2716.Hanlon JT, et al. J Clin Epidemiol 1992;45:1045.Samsa GP, et al. J Clin Epidemiol 1994;47:891.

Hanlon JT, et al J Clin Epidemiology 1992;45:1045.
The Medication Appropriateness Index

Balancing the polypharmacy Balancing the polypharmacy tension with a view to tension with a view to improving qualityimproving quality
Every drug listed ……Every drug listed ……• has clinical indicationhas clinical indication• is actually being takenis actually being taken• has a risk/benefit analysis that is has a risk/benefit analysis that is
recognized/understood/acceptedrecognized/understood/accepted• is at the lowest effective doseis at the lowest effective dose• is evaluated for costis evaluated for cost

Key to med review in the elderly Key to med review in the elderly is the clinical contextis the clinical context
• Takes into account unique patient needs Takes into account unique patient needs guided byguided by goals of caregoals of care– patient preferencespatient preferences– estimated remaining life expectancy (RLE)estimated remaining life expectancy (RLE)– best medical evidence including time until best medical evidence including time until
benefitbenefit
• Need a “Need a “captain of the shipcaptain of the ship” for med review” for med review– Need to prioritize meds for patients with Need to prioritize meds for patients with
multiple conditionsmultiple conditions– Address new symptoms by including med Address new symptoms by including med
review as part of the processreview as part of the process
Holmes HM, et al. Arch Intern Med 2006; 166:605.

Enlist the pharmacistEnlist the pharmacist
• Use in the clinical care teamUse in the clinical care team• ExamplesExamples
– Coumadin clinicsCoumadin clinics– Multidisciplinary interventions Multidisciplinary interventions
• ICUICU• COPDCOPD• CHFCHF
Holland R, et al. Homer trial BMJ 2005;330:293.Lenaghan E, et al. Age & Ageing 2007;36:292.Chiquette E, et al. Arch Intern Med 1998;158:1641.Leape LL, et al. JAMA 1999;282:267.Strom BL, et al JAMA 2002;288:1642.Rich MW, et al N Engl J Med 1995;333:1190.

Use of Computerized Physician Order Entry Use of Computerized Physician Order Entry (CPOE)(CPOE)
Bates DW, et al JAMA 1998;1311-16.Classen DC, et al J Am Med Infromat Assoc 2006 14:48.
Leapfrog CPOE Evaluation Test Clinical Decision Support CategoriesLeapfrog CPOE Evaluation Test Clinical Decision Support Categories
* Therapeutic Duplication* Therapeutic Duplication
*Single & Cumulative Dose Limits*Single & Cumulative Dose Limits
*Allergies & Cross Allergies*Allergies & Cross Allergies
*Contraindicated Route of Administration*Contraindicated Route of Administration
*Drug-Drug & Drug-Disease Interactions*Drug-Drug & Drug-Disease Interactions
* Contraindications/Dose Limits Based on Patient Diagnosis* Contraindications/Dose Limits Based on Patient Diagnosis
*Contraindications/ Dose Limits Based in Patient Age or Weight*Contraindications/ Dose Limits Based in Patient Age or Weight
*Contraindications/Dose Limits Based on Laboratory Studies*Contraindications/Dose Limits Based on Laboratory Studies
*Contraindications/Dose Limits Based on Radiology Studies*Contraindications/Dose Limits Based on Radiology Studies
*Corollary*Corollary
*Cost of Care*Cost of Care
* Nuisance* Nuisance

Case of Mrs. T…..Case of Mrs. T…..
• • 85 y/o with h/o DM, CHF, lumbar spinal stenosis admitted with increasing 85 y/o with h/o DM, CHF, lumbar spinal stenosis admitted with increasing confusion and falls. Lives alone, daughter involved. Daughter notes patient confusion and falls. Lives alone, daughter involved. Daughter notes patient h/o anxiety but c/o insomnia and phoning her continuously throughout the h/o anxiety but c/o insomnia and phoning her continuously throughout the night for the past 3 nights.night for the past 3 nights.
• • Brought to U of C ER by daughter after a witnessed fall. New patient to Brought to U of C ER by daughter after a witnessed fall. New patient to the U of C system. Admitted at 3AM to telemetry. the U of C system. Admitted at 3AM to telemetry.
• • On exam, alternately agitated and somnolent, oriented to person only.On exam, alternately agitated and somnolent, oriented to person only. VS: T99, P54, RR20, BP110/50 lying supine wt. 100lbs. 5’1”VS: T99, P54, RR20, BP110/50 lying supine wt. 100lbs. 5’1” Cor: RRR, +SCor: RRR, +S33 Lungs: dry crackles in basesLungs: dry crackles in bases Abd: soft, nontender, nondistended, firm stool felt throughout colonAbd: soft, nontender, nondistended, firm stool felt throughout colon
• • ER data:CT head neg., dirty urine, CXR with ER data:CT head neg., dirty urine, CXR with cor, KUB FOS, BUN 48/CR cor, KUB FOS, BUN 48/CR 2.7, glc= 74, K2.7, glc= 74, K++ hemolyzed at 6.3 F/U pending,INR=3.0, EKG SB-rate 58, no hemolyzed at 6.3 F/U pending,INR=3.0, EKG SB-rate 58, no peaked t waves. Given dose IV antibiotics in ER.peaked t waves. Given dose IV antibiotics in ER.

Case of Mrs. T…..hospital day Case of Mrs. T…..hospital day #5#5
Lisinopril 40mg q dailyLisinopril 40mg q daily
Glipizide ER 20mg BIDGlipizide ER 20mg BID
Lasix 40 mg q dailyLasix 40 mg q daily
KCL 20 meq q dailyKCL 20 meq q daily
Paxil 20 mg q dailyPaxil 20 mg q daily
Amiodarone 200mg q dailyAmiodarone 200mg q daily
Digoxin 0.25 mg q dailyDigoxin 0.25 mg q daily
Coumadin 5mg q hsCoumadin 5mg q hs
T#3 prnT#3 prn
Ativan 1mg prnAtivan 1mg prn
Unsom (OTC) prn sleepUnsom (OTC) prn sleep
Lomotil (OTC) prnLomotil (OTC) prn
Senna and colace prnSenna and colace prn
Lisinopril Lisinopril 20mg20mg q daily q daily
Glipizide ER 20 mg Glipizide ER 20 mg dailydaily
Lasix 40 mg q dailyLasix 40 mg q daily
Amiodarone 200mg q dailyAmiodarone 200mg q daily
Digoxin Digoxin 0.125 mg q M,W,Fri0.125 mg q M,W,Fri
Coumadin Coumadin 3mg 3mg q hsq hs
Tylenol 1000mg TIDTylenol 1000mg TID
Cipro 250 mg BIDCipro 250 mg BID

Medication use based on aging Medication use based on aging pharmacology principlespharmacology principles
• Start low, go slow, dose to effectStart low, go slow, dose to effect• Adjust for decrease in renal clearance Adjust for decrease in renal clearance • ID drugs w/narrow toxic/therapeutic ID drugs w/narrow toxic/therapeutic
indexindex• ID drugs that effect CPY450 system e.g., ID drugs that effect CPY450 system e.g.,
inhibitors/inducersinhibitors/inducers• Adjust for anticholinergic properties of Adjust for anticholinergic properties of
drugsdrugs• Remember the blunted barorecepter Remember the blunted barorecepter
reflexreflex

Med Review: Intersecting Med Review: Intersecting SafetiesSafeties
• PCP plays key role in med review (prioritize & individualize)PCP plays key role in med review (prioritize & individualize)• New symptom consider a medication in the D/DxNew symptom consider a medication in the D/Dx• Meds on list guided by goals of careMeds on list guided by goals of care• Review meds on list for Review meds on list for
– IndicationIndication– DoseDose– Interactions—drug/drug & drug/diseaseInteractions—drug/drug & drug/disease– DuplicationsDuplications– AdherenceAdherence– CostCost
• Enlist the pharmacistEnlist the pharmacist• Enlist a CPOE systemEnlist a CPOE system• Review for medication underuseReview for medication underuse

Into the future……Into the future……
• Increase knowledge base on drugs in Increase knowledge base on drugs in the elderlythe elderly– Clinical trials vs. post marketing Clinical trials vs. post marketing
surveillancesurveillance
• Broaden testing/implementation of Broaden testing/implementation of technologies e.g., CPOEtechnologies e.g., CPOE
• Multidisciplinary monitoringMultidisciplinary monitoring• Support continued affordable drug Support continued affordable drug
coveragecoverage

Special ThanksSpecial Thanks
• CHAMP core facultyCHAMP core faculty• Holly Holmes, MDHolly Holmes, MD• Visit our website Visit our website
@http://champ.bsd.uchicago.edu@http://champ.bsd.uchicago.edu

CHAMP: Drugs and AgingCHAMP: Drugs and AgingBibliographyBibliography
1.1. Bates DW, et al: The cost of adverse drug events in hospitalized Bates DW, et al: The cost of adverse drug events in hospitalized patients. JAMA 1997;277:307-11.patients. JAMA 1997;277:307-11.
2.2. Bates DW, et al: Incidence of adverse drug events and potential Bates DW, et al: Incidence of adverse drug events and potential adverse drug events: implications for prevention. JAMA adverse drug events: implications for prevention. JAMA 1995;274:29-34.1995;274:29-34.
3.3. Beers, MH, Ouslander JG, Rollingher I, Reuben DB, Brooks, J, Beers, MH, Ouslander JG, Rollingher I, Reuben DB, Brooks, J, Beck JC.: Beck JC.: Explicit criteria for determining inappropriate medication use Explicit criteria for determining inappropriate medication use in nursing home residents. Arch Intern Med 1991; 151: 1825-in nursing home residents. Arch Intern Med 1991; 151: 1825-1832..1832..
4.4. Beers MH: Explicit criteria for determining potentially Beers MH: Explicit criteria for determining potentially inappropriate medication use by the elderly: an update Arch inappropriate medication use by the elderly: an update Arch Intern Med 1997;157(14):1531-36.Intern Med 1997;157(14):1531-36.
5.5. Beers MH. :Inappropriate medication prescribing in skilled-Beers MH. :Inappropriate medication prescribing in skilled-nursing facilities. Ann Intern Med. 1992 Oct15; 117(8): 684-nursing facilities. Ann Intern Med. 1992 Oct15; 117(8): 684-689.689.
6.6. Buetow SA, Sibbald B, Cantrill JA, Halliwell S.: Appropriateness Buetow SA, Sibbald B, Cantrill JA, Halliwell S.: Appropriateness in health care: application to prescribing. Soc Sci Med 1997; in health care: application to prescribing. Soc Sci Med 1997; 45(2): 261-271.45(2): 261-271.
7. 7. Beyth RJ, et al: Principles of drug therapy in older Beyth RJ, et al: Principles of drug therapy in older adults:rational adults:rational drug prescribing. Clin Ger med 2002;18:577-92.drug prescribing. Clin Ger med 2002;18:577-92.

CHAMP: Drugs and AgingCHAMP: Drugs and AgingBibliographyBibliography
8. 8. Chrischilles EA, et al: Use of medications by persons 65 and Chrischilles EA, et al: Use of medications by persons 65 and over: data from the established populations for the over: data from the established populations for the epidemiologic studies of the elderly. J Gerontol 1992; M137-epidemiologic studies of the elderly. J Gerontol 1992; M137-M144.M144.
9. 9. Chin MH, Wang LC, Jin L, Mulliken R, Walter J, Hayley DC, Chin MH, Wang LC, Jin L, Mulliken R, Walter J, Hayley DC, Karrison TG, Nerney MP, Miller A, Friedmann PD.: Karrison TG, Nerney MP, Miller A, Friedmann PD.: Appropriateness of medication selection for older Appropriateness of medication selection for older
persons in an persons in an urban academic emergency department. Academic Emergency urban academic emergency department. Academic Emergency Medicine 1999; 6: 1232-1242.Medicine 1999; 6: 1232-1242.10. 10. Classen DC, et al: Adverse drug events in hospitalized Classen DC, et al: Adverse drug events in hospitalized
patients: patients: excess length of stay, extra costs, and attributable mortality. excess length of stay, extra costs, and attributable mortality. JAMA 1997;277: 301-6.JAMA 1997;277: 301-6.
11. 11. Doucet J, et al: Drug-drug interactions related to hospital Doucet J, et al: Drug-drug interactions related to hospital admissions in older adults: a prospective study of 1000 admissions in older adults: a prospective study of 1000 patients. J Am Geriatr Soc 1996;44:944-48.patients. J Am Geriatr Soc 1996;44:944-48.

CHAMP: Drugs and AgingCHAMP: Drugs and AgingBibliographyBibliography
12. 12. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean R, Beers MH. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean R, Beers MH. Updating the Beers Criteria for potentially inappropriate Updating the Beers Criteria for potentially inappropriate medication use in older adults. Arch Int Med 2003; 163: 2716-24.medication use in older adults. Arch Int Med 2003; 163: 2716-24.
13. 13. Gurwitz JH, Field TS, Avorn J, McCormick D, Jain S, Eckler M, Gurwitz JH, Field TS, Avorn J, McCormick D, Jain S, Eckler M, Benser M, Edmondson AC, Bates DW. Incidence and Benser M, Edmondson AC, Bates DW. Incidence and preventability of adverse drug events in nursing homes. Am J preventability of adverse drug events in nursing homes. Am J Med 2000; 109: 87-94.Med 2000; 109: 87-94.
14. 14. Hanlon JT, et al: A method for assssing drug therapy Hanlon JT, et al: A method for assssing drug therapy appropriateness. J Clin Epidemiol 1992; 45: 1045-51.appropriateness. J Clin Epidemiol 1992; 45: 1045-51. 15. 15. Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication
use among frail elderly inpatients. Ann Pharmacother 2004; 38: use among frail elderly inpatients. Ann Pharmacother 2004; 38: 9-14. 9-14.
16. 16. Inouye SK, et al: Precipitating factors for delirium in hospitalized Inouye SK, et al: Precipitating factors for delirium in hospitalized elderly persons: predictive model and interrelationship with elderly persons: predictive model and interrelationship with baseline vulnerability. JAMA 1996;275: 852-57.baseline vulnerability. JAMA 1996;275: 852-57.
17. 17. Kroenke K: Polypharmacy : causes, consequences, and cure. Kroenke K: Polypharmacy : causes, consequences, and cure. Am J Med 1985;79:149-52.Am J Med 1985;79:149-52.

CHAMP: Drugs and AgingCHAMP: Drugs and AgingBibliographyBibliography
18. 18. Kaiser Family Foundation. Views of the new Medicare drug Kaiser Family Foundation. Views of the new Medicare drug law: a survey of people on Medicare. August 2004.law: a survey of people on Medicare. August 2004.
19. 19. Lazarou J, et al: Incidence of adverse drug reactions Lazarou J, et al: Incidence of adverse drug reactions inhospitalized patients: a meta-analysis of prospective inhospitalized patients: a meta-analysis of prospective studies. JAMA 1998; 279: 1200-5.studies. JAMA 1998; 279: 1200-5.
20. 20. Leape L: Reporting of adverse events. NEJM 2002;347: 1633-Leape L: Reporting of adverse events. NEJM 2002;347: 1633-38.38.
21. 21. Lipton HL, et al: The impact of clinical pharmacists’ Lipton HL, et al: The impact of clinical pharmacists’ consultations on physicians geriatric drug prescribing: a consultations on physicians geriatric drug prescribing: a randomized controlled trial. Med Care 1992; 30: 646-58.randomized controlled trial. Med Care 1992; 30: 646-58.
22. 22. Ryan AA. Medication compliance and older people: a review Ryan AA. Medication compliance and older people: a review of the literature. Int’l J Nursing Studies 1999; 36: 153-162.of the literature. Int’l J Nursing Studies 1999; 36: 153-162.
23. 23. Samsa GP, Hanlon JT, Schmader KE, Weinberger M, Clipp EC, Samsa GP, Hanlon JT, Schmader KE, Weinberger M, Clipp EC, Uttech KM, Lewis IK, Landsman PB, Cohen HJ. A summated Uttech KM, Lewis IK, Landsman PB, Cohen HJ. A summated score for the medication appropriateness index: score for the medication appropriateness index: development and assessment of clinimetric properties development and assessment of clinimetric properties including content validity. J Clin Epidemiol 1994; 47(8):891-including content validity. J Clin Epidemiol 1994; 47(8):891-896.896.
24. 24. Schmader K, et al: Appropriateness of medication Schmader K, et al: Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994; 42: 1241-47.1994; 42: 1241-47.

CHAMP: Drugs and AgingCHAMP: Drugs and AgingBibliographyBibliography
25. 25. Stuck AE, Beers MH, Steiner A, Aronow HU, Stuck AE, Beers MH, Steiner A, Aronow HU, Rubenstein LZ, Beck JC. Inappropriate medication use Rubenstein LZ, Beck JC. Inappropriate medication use in community-residing older persons. Arch Intern in community-residing older persons. Arch Intern Med 1994; 154: 2195-2200.Med 1994; 154: 2195-2200.
26. 26. Van Eijken M, Tsang S, Wensing M, de Smet PAGM, Van Eijken M, Tsang S, Wensing M, de Smet PAGM, Grol RPTM.Grol RPTM.
Interventions to improve medication compliance in Interventions to improve medication compliance in older patients older patients
living in the community: a systematic review of the living in the community: a systematic review of the literature. Drugs & Aging 2003; 20: 229-240. literature. Drugs & Aging 2003; 20: 229-240.
27. 27. Illinois Department of Public Aid website, Illinois Department of Public Aid website, ©©2004.2004.