Embed Size (px)
Citation preview

110 Copyright © 2017 Asian Society of Cardiovascular Imaging
INTRODUCTION
Contrast-enhanced cardiovascular magnetic resonance (CMR) is considered the gold standard for the non-invasive detection
of focal myocardial fibrosis [1,2]. Over the past decade, more in-depth tissue characterization has become possible using T1 mapping CMR [3]. This technique allows the non-invasive de-tection of diffuse interstitial myocardial fibrosis [4-6], amyloid deposits [7-9], edema [10-12], intramyocardial fat [13,14], and iron deposits [15]. In pathologies such as amyloidosis and An-derson-Fabry’s disease, where the changes in myocardial T1
cc This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduc-tion in any medium, provided the original work is properly cited.
CVIA 2017;1(2):110-115
pISSN 2508-707X / eISSN 2508-7088
ORIGINAL ARTICLE
CVIAhttps://doi.org/10.22468/cvia.2016.00129
Gender Differences in Native Myocardial T1 in a Healthy Chinese Volunteer CohortHeerajnarain Bulluck1,2*, Jennifer A Bryant1*, Jonan Zhien Tan1, Yun Yun Go1, Thu-Thao Le1, Ru San Tan1, Tiong Keng Lim1, Hak Chiaw Tang1, Narayan Lath1, Adrian Shoen Low1, Calvin Woon-Loong Chin1, Stuart A Cook1,3, Derek J Hausenloy1,2,3,4,5,6
1 National Heart Research Institute Singapore, National Heart Centre Singapore, Singapore, Singapore 2 The Hatter Cardiovascular Institute, Institute of Cardiovascular Science, University College London, London, UK
3 Cardiovascular and Metabolic Disorders Program, Duke-National University of Singapore, Singapore, Singapore
4 The National Institute of Health Research, University College London Hospitals, Biomedical Research Centre, London, UK
5Yong Loo Lin School of Medicine, National University Singapore, Singapore, Singapore6Barts Heart Centre, St Bartholomew’s Hospital, London, UK
Objective: T1 mapping cardiovascular magnetic resonance (CMR) is emerging as a promis-ing imaging biomarker. However, there are conflicting reports on whether myocardial T1 is affected by age, gender, heart rate, and blood T1. Therefore, the aim of this study was to as-sess the influence of these parameters on myocardial T1 at 1.5T in a healthy Chinese cohort.
Materials and Methods: 101 healthy Chinese volunteers underwent CMR (Siemens Aera 1.5T scanner). A mid-ventricular short axis modified Look-Locker inversion recovery T1 map was acquired. The images were analyzed on CVI42. Manual regions of interest were drawn in the inferior septum and in the blood pool.
Results: Participants’ mean age was 46±13 (range 21 to 68) years and 51 out of 101 pa-tients (51%) were males. Females in this study had significantly higher myocardial T1 and blood T1 values than males (1025±26 ms vs. 1001±23 ms, p<0.001; and 1659±60 ms vs. 1577±54 ms, p<0.001 respectively). There was no correlation between myocardial T1 and age. Blood T1 and heart rate correlated with myocardial T1 in females, but not in males and both were significantly associated with myocardial T1 in a multivariate analysis. After adjust-ing myocardial T1 for heart rate and blood T1 in females, the standard deviation reduced by 12% but the gender difference was still present.
Conclusion: Gender-specific T1 values should be established by each center, and heart rate and blood T1 should be taken into account in female participants. This would be important in order to reliably detect small changes in native T1 in pathologies with diffuse interstitial fibrosis.
Key words Magnetic resonance imaging ∙ Myocardium ∙ Reference values ∙ Sex ∙ Healthy volunteers.
Received: November 22, 2016Revised: December 25, 2016Accepted: January 3, 2017
Corresponding authorDerek J Hausenloy, PhDCardiovascular and Metabolic Diseases Program, Duke-National University of Singapore, 8 College Road, Singapore 169857, SingaporeTel: 65-6516-6719 Fax: 65-6224-8790E-mail: [email protected]
*These authors contributed equally to this work.

www.e-cvia.org 111
Heerajnarain Bulluck, et al CVIAvalues are large, T1 mapping is already being used in the clini-cal setting [16]. However, in conditions with diffuse interstitial myocardial fibrosis such as hypertensive heart disease [17], di-abetic cardiomyopathy [18], and aortic stenosis [19], where the changes in myocardial T1 values are relatively small, more work needs to be done before this technique can be used for diagno-sis, prognosis, disease surveillance, and assessment of response to therapies.
Initial methods of T1 measurement involved multiple breath-holds to obtain the recovery curve at different time points. The Look–Locker sequence was then introduced [20] to measure the T1 relaxation time at multiple time points after an initial ex-citation pulse and then subsequently adapted as the modified Look–Locker inversion recovery (MOLLI) [21] sequence. Col-ored, pixel-wise T1 maps are generated automatically by the scanner, whereby each pixel carries the measured T1 value [3].
In order for native T1 mapping CMR to be established as a robust marker, the influence of the physiological changes on myocardial T1 due to age [22,23], gender [22-26], and heart rate [22,27] need to be addressed. There have been conflicting re-ports on whether a gender difference exists [22,28]. In a small study of 40 healthy individuals, the gender difference in myo-cardial T1 was eliminated after normalizing for blood T1 [26]. There are also conflicting reports on whether T1 increases [24,29] or decreases with age [22]. Other factors such as blood T1 (either due to the intravascular compartment or partial vol-ume effects) [30] and heart rate have also been shown to influ-ence myocardial T1 values [27]. Furthermore, T1 mapping values in an Asian cohort have not yet been reported and the Society for CMR and CMR Working Group of the European Society of Cardiology consensus statement [31] highlighted the need for site and vendor-specific reference values.
Therefore, the aim of this study was to assess the influence of age, gender, heart rate, and blood T1 on myocardial T1 at 1.5T in a healthy Chinese volunteer cohort.
MATERIALS AND METHODS
The study was approved by the Singhealth Centralized Insti-tutional Review Board and all participants provided written informed consent. Healthy Chinese Singaporean volunteers free of a history or symptoms of cardiovascular disease, diabetes, or hypertension were recruited via local advertisement.
CMR acquisitionCMR scans were performed on a 1.5T scanner (Magnetom
Aera; Siemens Medical Solutions, Erlangen, Germany) using a 60-channel cardiac phased array receiver coil. The imaging pro-tocol included standard steady state free precession cines and mid-ventricular short axis native MOLLI T1 mapping as part
of MyoMaps available on the scanner [21]. The sampling pro-tocol involved 11 heart beats in total, with the acquisition of 5 images after the first inversion pulse, followed by a recovery phase of 3 heart beats and acquisition of the final 3 images after the second inversion pulse. This sampling protocol is referred to as the 5(3)3 sampling protocol throughout the manuscript. The acquisition parameters were as follows: pixel bandwidth= 1085 Hz/pixel; flip angle=35°; matrix=256×144; slice thick-ness=8 mm, echo time=1.1 ms; repetition time=280 ms; typical field of view=360 mm; voxel size=1.5×1.5×8 mm; field of view phase=85%; acceleration factor for parallel imaging=2; acquisi-tion time=11 heartbeats. Non-rigid motion correction was per-formed to align the set of images acquired at different inversion times and a non-linear least-square curve fitting was used to generate a pixel-wise colored T1 map in-line by the scanner. All CMR scans were screened for any structural abnormalities by Level 3 CMR cardiologists and radiologists.
Imaging analysisAll CMR scans were analyzed using specialist software (Cir-
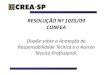
cle Cardiovascular Imaging, Version 5.3.4, Calgary, Canada). Cine images were analyzed based on the current recommenda-tions [2]. A region of interest (ROI) was manually drawn in the inferior septum (≈0.5 cm2) and the left ventricular blood pool (≈1.5 cm2) of the mid-ventricular short axis native MOLLI T1 map. The width of the ROI line in the inferior septum was 3 pixels and care was taken to avoid the inferior right ventricular insertion points and the blood pool by allowing for the myocar-dium to be visible (visually equivalent to at least more than an ROI line width–3 pixels) between the blood pool and ROI. For the blood pool ROI, care was taken to avoid the papillary mus-cles. Fig. 1 illustrates 2 mid ventricular short axis T1 maps from a male and a female volunteer with ROIs drawn on the inferior septum and blood.
Fig. 1. Example of the manual region of interest delineation in the inferior septum and the blood pool with representative values of two mid-ventricular MOLLI T1 maps from a male and a female volun-teer. MOLLI: modified Look-Locker inversion recovery.
Male volunteerMyocardial T1 1004 msBlood T1 1592 ms
Female volunteerMyocardial T1 1020 msBlood T1 1712 ms
MOLLI T1 maps 2000
0 ms

112 CVIA 2017;1(2):110-115
Gender Difference in Native T1 in ChineseCVIA20 T1 maps were randomly chosen for inter-observer and
intra-observer variability of T1 measurements.
Statistical analysesStatistical analyses were performed using SPSS (Ver 22, IBM
Co., IL, USA). Normality was assessed using the Shapiro-Wilk Test. Continuous data was expressed as mean±standard devia-tion (SD) or median (interquartile range), and categorical data was reported as frequencies and percentages. Groups were compared using the paired Student t-test, Wilcoxon signed rank test and unpaired Student t-test or Mann Whitney U test where appropriate. Correlation was assessed using either Pear-son’s correlation coefficient for normally distributed data or Spearman’s rho for non-normally distributed data. Interob-server and intraobserver variability was assessed using the in-traclass correlation coefficient (ICC). Factors significant on uni-variate linear regression analysis were included in a multivariate linear regression analysis. All statistical tests were two-tailed, and p<0.05 was considered statistically significant.
RESULTS
101 healthy Chinese volunteers completed the study proto-
col and were included in the analysis. The mean age was 46±13 (range 21 to 68) years and 51 of the 101 patients (51%) were males. Only 4 volunteers (4%) were smokers. Further details on the clinical and CMR characteristics are presented in Table 1.
Interobserver and intraobserver variabilityThere was excellent interobserver and intraobserver agree-
ment for myocardial T1 (ICC 0.940, 95% CI 0.850–0.976 and ICC 0.978, 95% CI 0.944–0.991, respectively) and blood T1 mea-surements (ICC 0.997, 95% CI 0.0.980–0.999 and ICC 0.997, 95% CI 0.992–0.999, respectively) using manual ROI delineation.
Myocardial and blood T1 of the cohortThe mean myocardial T1 and blood T1 of the whole cohort
were 1013±27 ms and 1618±70 ms, respectively. Females had significantly higher myocardial T1 and blood T1 values than males (1025±26 ms vs. 1001±23 ms, p<0.001; and 1659±60 ms vs. 1577±54 ms, p<0.001, respectively).
Impact of age, heart rate, gender, and blood T1 on myocardial T1
There was no correlation between myocardial T1 and age for both genders as shown in Fig. 2A. There was no difference in heart rate between the genders (female: 62±9 bpm, range 45–90 bpm; male: 62±11 bpm, range 45–90 bpm, p=0.84). How-ever, blood T1 and heart rate were significantly correlated with myocardial T1 in females (blood T1 versus myocardial T1 R2 0.11, p=0.02, heart rate versus myocardial T1 R2 0.12, p=0.016), but not in males as shown in Fig. 2B and C.
Myocardial T1 adjusted for heart rate and blood T1 in females
In females, factors significantly associated with myocardial T1 on univariate linear regression analysis (heart rate and blood T1) were included in a multivariate linear regression analysis, and both factors remained significantly associated with myo-cardial T1. Using the slope derived from the multivariate linear regression analysis, myocardial T1 was adjusted for blood T1 and heart rate in females using the equation below adapted from Reiter et al. [26]:
Adjusted myocardial T1=measured myocardial T1+slopebloodT1 (mean blood T1–measured blood T1)+slopeheart rate (mean heart rate–actual heart rate)
Where slopeblood T1=0.18; slopeheart rate=0.79; mean heart rate=62 beats per minute; mean blood T1=1659 ms.
The mean adjusted myocardial T1 in females was 1025±23 ms and was similar to the non-adjusted myocardial T1 (1025± 26 ms, p=0.95). The gender difference was still present (adjusted
Table 1. Clinical and CMR characteristics of the Chinese partici-pants
Males (n=51) Females (n=50) pClinical
Age (years) 48±14 44±13 0.14Systolic BP (mm Hg) 131±16 121±16 0.003Diastolic BP (mm Hg) 79±9 73±11 0.002Heart rate (bpm) 62±11 62±9 0.84Height (cm) 171±6 159±7 <0.001Weight (kg) 69±12 57±10 <0.001BMI (kg m-2) 24±4 22±4 0.09BSA (m2) 1.81±0.18 1.59±0.15 <0.001
CMRLVEDV (mL) 139±21 110±19 <0.001LVEDVi (mL m-2) 77±9 69±9 <0.001LVESV (mL) 54±13 41±11 <0.001LVESVi (mL m-2) 30±6 26±6 <0.001LVMass (g) 95±18 70±16 <0.001LVMassi (g m-2) 52±8 44±7 <0.001LVEF (%) 61±6 63±6 0.06Blood T1 (ms) 1577±54 1659±60 <0.001Myocardial T1 (ms) 1001±23 1025±26 <0.001
BP: blood pressure, bpm: beats per minute, CMR: cardiovascular mag-netic resonance, LVEDV: left ventricular end diastolic volume, LVED-Vi: indexed left ventricular end diastolic volume, LVESV: left ventricu-lar end systolic volume, LVESVi: indexed left ventricular end systolic volume, LVMass: left ventricular mass, LVMassi: indexed left ventric-ular mass, LVEF: left ventricular ejection fraction

www.e-cvia.org 113
Heerajnarain Bulluck, et al CVIA
myocardial T1 in females: 1025±23 ms, myocardial T1 males: 1001±23 ms, p<0.001). However, there was a 12% (3 ms) reduc-tion in the SD for myocardial T1 in the female cohort.
DISCUSSION
The main findings of our study are; firstly, there was no change in myocardial T1 with age in this Chinese cohort up to 68 years of age. Secondly, myocardial T1 was influenced by heart rate and blood T1 in females but not in males. Furthermore, despite adjusting myocardial T1 for these 2 parameters, the gender difference persisted. Lastly, adjusting myocardial T1 for heart rate and blood T1 in females reduced the variability in this cohort by 12%.
Whether fibrosis increases with age remains a topic of de-bate. Sado et al. [32] previously showed in a cohort of 81 healthy volunteers that extracellular volume fraction (ECV) derived from native and post-contrast T1 did not change with age. How-ever, they used the previous laborious technique for T1 mea-surement rather than the latest generation T1 mapping tech-niques. Most recently, Rosmini et al. [25], in a conference abstract involving 94 healthy volunteers and using the latest MOLLI T1 and ECV mapping technique, showed that T1 values fell with age, but there was no correlation between age and ECV. In a larger healthy volunteer cohort of 342 participants using the shortened MOLLI (ShMOLLI) T1 mapping technique, Piech-nik et al. [22] also showed a reduction in T1 with age, but in fe-males only. Rauhalammi et al. [23] recently showed that myo-cardial T1 by the MOLLI T1 mapping 3(3)3(3)5 sampling protocol was negatively correlated with age in females, but not in males in 84 participants. The impact of age on myocardial T1 has also been investigated in non-healthy volunteer cohorts. Ugander et al. [29] reported an increase in ECV with age in 60 patients with cardiovascular disease, but no scars. In the MESA cohort involving 1231 participants aged 54 to 93 years and
with cardiovascular risk factors (the largest cohort of T1 map-ping reported so far), Liu et al. [24] also showed an increase in T1 and ECV with age (more pronounced in males than females). However, in a sub-group of patients with reduced exposure to cardiovascular risk factors (n=235), there was no correlation be-tween age and ECV. We also found no correlation between age and myocardial T1 in healthy hearts, but the maximum age of our cohort was 68 years.
The gender difference in myocardial T1 and ECV has been reported by several groups [22-26] and of note, all these stud-ies were performed on Siemens scanners. In a multi-centre study using MOLLI T1 mapping on Philips scanners by Dabir et al. [28], no gender difference in myocardial T1 was observed. How-ever, their study included a mixture of healthy individuals (n= 102) and low-risk patients (n=113) and used the 3(3)3(3)5 MOL-LI sampling protocol. We used the optimized 5(3)3 MOLLI sampling protocol which has been shown to have improved ac-curacy compared to the 3(3)3(3)5 MOLLI sampling protocol [27]. It is already recognized that differences in androgen levels between genders influence the cardiac geometry and lead to higher indexed LV mass in males compared to females [33]. Thinner hearts in females may predispose them to partial vol-ume effects. Furthermore, females are known to have lower he-matocrit than males and hematocrit itself has been shown to have an inverse correlation with blood T1 [34,35]. This would contribute to higher T1 and T2 values (already shown by Bön-ner et al. [36]) in the intravascular compartments of females, leading to higher myocardial T1. Although we attempted to adjust myocardial T1 for blood T1 to account for this and our ROI were quite conservative to avoid partial volume effects, the difference between genders was still present. Whether this gender difference in myocardial T1 is due to a true biological difference or is related to the vendor platform and sampling pro-tocol used remains unclear and would require further studies scanning the same participants on scanners from different ven-
Fig. 2. Correlation between myocardial T1 and (A) age; (B) heart rate; (C) blood T1, stratified according to gender. NS: not statistically sig-nificant.
1100
1050
1000
95020 30 40 50 60 70
MaleFemale
Age (years)
Myo
card
ial T
1 (m
s)
A
1100
1050
1000
95040 50 60 70 80 90
MaleFemale
Heart rate (bpm)M
yoca
rdia
l T1
(ms)
B
1100
1050
1000
9501400 1500 1600 1700 1800
MaleFemale
Blood T1 (ms)
Myo
card
ial T
1 (m
s)
C

114 CVIA 2017;1(2):110-115
Gender Difference in Native T1 in ChineseCVIAdors and using different sampling protocols.
Heart rate is known to affect the MOLLI T1 maps due to loss of spatial resolution at higher heart rates, which then leads to an increase in motion and an increase in partial volume effects [27]. Piechnik et al. [22] previously reported an increase of 6 ms in ShMOLLI T1 values for every 10 bpm increase in heart rate. In our study, despite no significant difference in heart rate between genders, heart rate was positively associated with myocardial T1 in females, but not in males. This is likely due to females hav-ing thinner myocardium and therefore may be more prone to in-plane partial volume effects [22]. In a study of 40 healthy vol-unteers [27], myocardial T1 adjusted for blood T1 eliminated the gender difference. That study had a smaller number of par-ticipants compared to our study and furthermore, the MOLLI sampling protocol was 5(4)2 and different from the commonly used sampling protocols. In our study of 101 healthy volunteers, the gender difference was still present after adjusting for blood T1 and heart rate using the 5(3)3 MOLLI sampling protocol. However, the variability in myocardial T1 in females reduced by 12% and may likely represent a reduction in partial volume effects.
Liu et al. [24] explored the impact of ethnicity and found no difference in myocardial T1 values among Caucasian, African, Chinese, and Hispanic groups. The T1 values obtained in our cohort of healthy Chinese Singaporeans were similar to the val-ues reported in a UK cohort [25] using a similar sampling pro-tocol on a Siemens platform at 1.5T (our cohort myocardial T1: males 1001±23 ms and females: 1025±26 ms; UK cohort: males 1008±33 ms and females 1043±37 ms).
The implications of this study are firstly, in centers using MOLLI T1 mapping on a Siemens platform at 1.5T with the 5(3)3 sampling protocol, T1 reference values should be derived for each gender separately. Secondly, myocardial T1 values in females should be adjusted to blood T1 and heart rate, which would reduce variability. The impact of gender, blood T1, and heart rate on myocardial T1 may not be significant in patholo-gies with big changes in T1 values, e.g., myocarditis [37], acute myocardial infarction [11], and amyloidosis [7]. However, in pathologies where myocardial T1 changes are subtler, e.g., hy-pertensive heart disease [17], diabetic cardiomyopathy [18], and aortic stenosis [19], the impact of gender, blood T1, and heart rate may be more significant and must be taken into account.
LimitationsWe only recruited Chinese participants in this study, as they
are the predominant ethnicity in Singapore. We did not admin-ister contrast to rule out late gadolinium enhancement, but a normal scan was confirmed based on normal wall thickness and normal wall motion in a healthy volunteer cohort free of risk factors. For the same reason, ECV data was not available
in this cohort. Hemoglobin and hematocrit results were not col-lected and therefore we could not adjust for these factors. Manu-al ROIs were drawn in the septum for representative T1 values rather than calculating mean segmental T1 values. This was to provide reference values using a method that can be easily performed in a clinical setting. We only used one vendor and one T1 mapping sequence at 1.5T. The variability in myocar-dial T1 may be multi-factorial due to a combination of biologi-cal, physiological, and technical factors, and warrants further investigation.
ConclusionThere was no correlation between age and myocardial T1 by
MOLLI using the 5(3)3 sampling protocol up to an age of 68 years. In females, myocardial T1 was significantly associated with heart rate and blood T1. Adjusting myocardial T1 for heart rate and blood T1 did not eliminate the gender difference, but reduced the variability of myocardial T1 in females. Therefore, centers using MOLLI T1 mapping should provide gender-spe-cific reference values for myocardial T1. Furthermore, heart rate and blood T1 should be taken into account in female par-ticipants, as this may be important when investigating small changes in native T1 in pathologies such as hypertensive heart disease, aortic stenosis, and diabetic cardiomyopathy, in order to detect diffuse interstitial fibrosis more reliably.
Conflicts of InterestThe authors declare that they have no conflict of interest.
AcknowledgmentsThis work was supported by a NMRC RIE2016 Centre Grant and the Brit-
ish Heart Foundation (FS/10/039/28270), and the National Institute for Health Research University College London Hospitals Biomedical Research Centre. We express our gratitude to the staff at the cardiac MRI department on the National Heart Centre, Singapore especially Bao Ru Leong, Elizabeth Pee Chong Goh, Yiying Han and all the healthy volunteer participants.
REFERENCES
1. Kramer CM, Barkhausen J, Flamm SD, Kim RJ, Nagel E; Society for Car-diovascular Magnetic Resonance Board of Trustees Task Force on Stan-dardized Protocols. Standardized cardiovascular magnetic resonance imaging (CMR) protocols, society for cardiovascular magnetic resonance: board of trustees task force on standardized protocols. J Cardiovasc Magn Reson 2008;10:35.
2. Schulz-Menger J, Bluemke DA, Bremerich J, Flamm SD, Fogel MA, Friedrich MG, et al. Standardized image interpretation and post process-ing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) board of trustees task force on standardized post processing. J Cardiovasc Magn Reson 2013;15:35.
3. Bulluck H, Maestrini V, Rosmini S, Abdel-Gadir A, Treibel TA, Castel-letti S, et al. Myocardial T1 mapping. Circ J 2015;79:487-494.
4. Puntmann VO, Voigt T, Chen Z, Mayr M, Karim R, Rhode K, et al. Na-tive T1 mapping in differentiation of normal myocardium from diffuse disease in hypertrophic and dilated cardiomyopathy. JACC Cardiovasc Imaging 2013;6:475-484.
5. White SK, Sado DM, Fontana M, Banypersad SM, Maestrini V, Flett AS,

www.e-cvia.org 115
Heerajnarain Bulluck, et al CVIAet al. T1 mapping for myocardial extracellular volume measurement by CMR: bolus only versus primed infusion technique. JACC Cardiovasc Imaging 2013;6:955-962.
6. Bulluck H, Rosmini S, Abdel-Gadir A, White SK, Bhuva AN, Treibel TA, et al. Automated extracellular volume fraction mapping provides insights into the pathophysiology of left ventricular remodeling post-reperfused ST-elevation myocardial infarction. J Am Heart Assoc 2016;5:e003555.
7. Fontana M, Banypersad SM, Treibel TA, Maestrini V, Sado DM, White SK, et al. Native T1 mapping in transthyretin amyloidosis. JACC Cardio-vasc Imaging 2014;7:157-165.
8. Banypersad SM, Sado DM, Flett AS, Gibbs SD, Pinney JH, Maestrini V, et al. Quantification of myocardial extracellular volume fraction in sys-temic AL amyloidosis: an equilibrium contrast cardiovascular magnetic resonance study. Circ Cardiovasc Imaging 2013;6:34-39.
9. Banypersad SM, Fontana M, Maestrini V, Sado DM, Captur G, Petrie A, et al. T1 mapping and survival in systemic light-chain amyloidosis. Eur Heart J 2015;36:244-251.
10. Ferreira VM, Piechnik SK, Dall’Armellina E, Karamitsos TD, Francis JM, Ntusi N, et al. T(1) mapping for the diagnosis of acute myocarditis using CMR: comparison to T2-weighted and late gadolinium enhanced imag-ing. JACC Cardiovasc Imaging 2013;6:1048-1058.
11. Bulluck H, White SK, Rosmini S, Bhuva A, Treibel TA, Fontana M, et al. T1 mapping and T2 mapping at 3T for quantifying the area-at-risk in re-perfused STEMI patients. J Cardiovasc Magn Reson 2015;17:73.
12. Bulluck H, Rosmini S, Abdel-Gadir A, White SK, Bhuva AN, Treibel TA, et al. Residual myocardial iron following intramyocardial hemorrhage during the convalescent phase of reperfused ST-segment-elevation myo-cardial infarction and adverse left ventricular remodeling. Circ Cardio-vasc Imaging 2016;9:e004940.
13. Sado DM, White SK, Piechnik SK, Banypersad SM, Treibel T, Captur G, et al. Identification and assessment of Anderson-Fabry disease by cardio-vascular magnetic resonance noncontrast myocardial T1 mapping. Circ Cardiovasc Imaging 2013;6:392-398.
14. Pica S, Sado DM, Maestrini V, Fontana M, White SK, Treibel T, et al. Re-producibility of native myocardial T1 mapping in the assessment of Fabry disease and its role in early detection of cardiac involvement by cardio-vascular magnetic resonance. J Cardiovasc Magn Reson 2014;16:99.
15. Sado DM, Maestrini V, Piechnik SK, Banypersad SM, White SK, Flett AS, et al. Noncontrast myocardial T1 mapping using cardiovascular magnetic resonance for iron overload. J Magn Reson Imaging 2015;41:1505-1511.
16. Taylor AJ, Salerno M, Dharmakumar R, Jerosch-Herold M. T1 mapping: basic techniques and clinical applications. JACC Cardiovasc Imaging 2016; 9:67-81.
17. Treibel TA, Zemrak F, Sado DM, Banypersad SM, White SK, Maestrini V, et al. Extracellular volume quantification in isolated hypertension - changes at the detectable limits? J Cardiovasc Magn Reson 2015;17:74.
18. Wong TC, Piehler K, Meier CG, Testa SM, Klock AM, Aneizi AA, et al. Association between extracellular matrix expansion quantified by car-diovascular magnetic resonance and short-term mortality. Circulation 2012;126:1206-1216.
19. Bull S, White SK, Piechnik SK, Flett AS, Ferreira VM, Loudon M, et al. Human non-contrast T1 values and correlation with histology in diffuse fibrosis. Heart 2013;99:932-937.
20. Look D, Locker DR. Time saving in measurement of NMR and EPR re-laxation times. Rev Sci Instrum 1970;41:250-251.
21. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med 2004;52:141-
146.22. Piechnik SK, Ferreira VM, Lewandowski AJ, Ntusi NA, Banerjee R, Hol-
loway C, et al. Normal variation of magnetic resonance T1 relaxation times in the human population at 1.5 T using ShMOLLI. J Cardiovasc Magn Re-son 2013;15:13.
23. Rauhalammi SM, Mangion K, Barrientos PH, Carrick DJ, Clerfond G, McClure J, et al. Native myocardial longitudinal (T1) relaxation time: Re-gional, age, and sex associations in the healthy adult heart. J Magn Reson Imaging 2016;44:541-548.
24. Liu CY, Liu YC, Wu C, Armstrong A, Volpe GJ, van der Geest RJ, et al. Evaluation of age-related interstitial myocardial fibrosis with cardiac magnetic resonance contrast-enhanced T1 mapping: MESA (Multi-Eth-nic Study of Atherosclerosis). J Am Coll Cardiol 2013;62:1280-1287.
25. Rosmini S, Bulluck H, Treibel TA, Abdel-Gadir A, Bhuva AN, Culotta V, et al. Native myocardial T1 and ECV with age and gender developing normal reference ranges - a 94 healthy volunteer study. J Cardiovasc Magn Reson 2016;18(Suppl 1):O42.
26. Reiter U, Reiter G, Dorr K, Greiser A, Maderthaner R, Fuchsjäger M. Normal diastolic and systolic myocardial T1 values at 1.5-T MR imaging: correlations and blood normalization. Radiology 2014;271:365-372.
27. Kellman P, Hansen MS. T1-mapping in the heart: accuracy and preci-sion. J Cardiovasc Magn Reson 2014;16:2.
28. Dabir D, Child N, Kalra A, Rogers T, Gebker R, Jabbour A, et al. Refer-ence values for healthy human myocardium using a T1 mapping method-ology: results from the International T1 Multicenter cardiovascular mag-netic resonance study. J Cardiovasc Magn Reson 2014;16:69.
29. Ugander M, Oki AJ, Hsu LY, Kellman P, Greiser A, Aletras AH, et al. Ex-tracellular volume imaging by magnetic resonance imaging provides in-sights into overt and sub-clinical myocardial pathology. Eur Heart J 2012; 33:1268-1278.
30. Wansapura J, Gottliebson W, Crotty E, Fleck R. Cyclic variation of T1 in the myocardium at 3 T. Magn Reson Imaging 2006;24:889-893.
31. Moon JC, Messroghli DR, Kellman P, Piechnik SK, Robson MD, Ugan-der M, et al. Myocardial T1 mapping and extracellular volume quantifi-cation: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J Cardiovasc Magn Reson 2013;15:92.
32. Sado DM, Flett AS, Banypersad SM, White SK, Maestrini V, Quarta G, et al. Cardiovascular magnetic resonance measurement of myocardial ex-tracellular volume in health and disease. Heart 2012;98:1436-1441.
33. Hassan AF, Kamal MM. Effect of exercise training and anabolic andro-genic steroids on hemodynamics, glycogen content, angiogenesis and apoptosis of cardiac muscle in adult male rats. Int J Health Sci (Qassim) 2013;7:47-60.
34. Treibel TA, Fontana M, Maestrini V, Castelletti S, Rosmini S, Simpson J, et al. Automatic measurement of the myocardial interstitium: synthetic extracellular volume quantification without hematocrit sampling. JACC Cardiovasc Imaging 2016;9:54-63.
35. Rosmini S, Bulluck H, Treibel TA, Bhuva AN, Abdel-Gadir A, Culotta V, et al. Hematocrit, iron and HDL-cholesterol explain 90% of variation in native blood T1. J Cardiovasc Magn Reson 2016;18(Suppl 1):O86.
36. Bönner F, Janzarik N, Jacoby C, Spieker M, Schnackenburg B, Range F, et al. Myocardial T2 mapping reveals age- and sex-related differences in volunteers. J Cardiovasc Magn Reson 2015;17:9.
37. Ferreira VM, Piechnik SK, Dall’Armellina E, Karamitsos TD, Francis JM, Ntusi N, et al. Native T1-mapping detects the location, extent and pat-terns of acute myocarditis without the need for gadolinium contrast agents. J Cardiovasc Magn Reson 2014;16:36.