Embed Size (px)
Citation preview

515
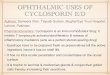
Fig I-Ambulatory ECG tracings (modified lead V5).
Before weight reduction; heart rate 61/min, QTc 0-52, PR 0-13 s.After weight reduction of 7 kg; heart rate 73/min, QTc 0- 35, PR 0- 12 s.
Fig 2-Ambulatory ECG tracings (modified lead V5).
Before weight reduction; atrial fibrillation with ST-T depression.After weight reduction of 5 kg; atrial fibrillation returned to sinus rhythm
and ST-T depression settled to isopotential line.
by 10% for more than 1 min. ECG monitoring with a Holterrecorder (’Accutape 24’; Hittman Medcraft, Skippack,Pennsylvania) showed the mean heart rate throughout the night tobe 62 beats/min. The OT was prolonged in two patients. Fourpatients developed unifocal atrial and ventricular premature beats,one had multifocal ventricular premature beats, and one had ST-Tsegment depression with atrial fibrillation. Polygraphic recordingrevealed the average number of apnoeic episodes to be 314. Thepatients were then put on a reducing diet for 2-8 weeks, initially600 kcal, and then 300 kcal, with a weight reduction of 4-11 kg. Themean basal Sa02 improved (see table) and hypoxic dips werereduced significantly. The mean heart rate also improved to
77 - 6± 15’ 1 beats/min, the OTc decreased (in one subject from 0 - 52to 0 - 38; fig 1). Ventricular and atrial premature beats were reducedin patients 1, 2, and 4, and in patient 4 the ST-T depression settledto the isopotential line with sinus rhythm after 7 kg weight loss (fig2). Apnoeic episodes during REM (rapid eye movement) sleep wereless frequent after weight loss (table).The improvements in these obese patients with sleep apnoea
syndrome thus include better oxygen saturation, less apnoea, lesshypersomnia, and ECG changes. Guilleminault et al suggest thattracheostomy is the treatment of choice. We do not agree. In veryobese patients with sleep apnoea syndrome weight reduction is thetreatment of choice, although reports are not always encouraging.4 4Our patients with sleep apnoea syndrome responded to weightreduction and clinical improvement was similar to that achieved bytracheostomy.4 Tracheostomy may be complicated by bleeding,subcutaneous emphysema, recurrent purulent bronchitis, andpsychological difFiculties.l4 If the problem is explained and thepatient is reassured, weight reduction may be successful in treatingthis difficult condition.
Department of Medicine,University Hospital of Wales,Cardiff CF4 4XW
V. G. TIRLAPURM. A. MIR
HUMAN LYMPHOCYTES TRANSFORMED WITHEPSTEIN-BARR VIRUS PRODUCE ANTIBODIES
AGAINST THE SPOROZOITE STAGE OFPLASMODIUM FALCIPARUM
SiR,-In 1983, to produce human monoclonal antibodies againstasexual erythrocytic stages of Plasmodium falciparum, we
transformed lymphocytes from African patients with Epstein-Barrvirus (EBV). Peripheral blood lymphocytes, obtained after ’Ficoll-Hypaque’ centrifugation, were suspended in tissue culture mediumfrom the EBV-producing marmoset cell line B95-8. After 1 h at
37°C, the lymphocytes were resuspended at 106 cells/ml in RPMI1640 medium containing 20% v/v fetal calf serum with penicillin100 IU/ml, streptomycin 100 mg/ml, and glutamine 2 mmol/1. Theywere incubated, in 25 ml Falcon flasks at 37°C, in a humidifiedatmosphere with air+5% CO2 and fed weekly. After 3, 4, and 6weeks of cell proliferation the culture supernatants were tested for Pfalciparum antibodies by indirect immunofluorescence (IFL).
Antibody production has since been improved by the addition of0-2 2 g/ml of cyclosporin to the culture medium. After labelling ofsynchronised parasites with 35S-methionine, electrophoresis onSDS-polyacrylamide gels, and autoradiography (techniquesdescribed in detail elsewhere2) these antibodies permitted theidentification of some defined Pfalciparum antigens (unpublished).We now wish to report on the possibility of obtaining
antisporozoite antibodies of Pfalciparum by the same technique ofEBV transformation. Sporozoites were isolated from the salivaryglands of infected mosquitoes (A stephensi) fed on the blood ofpatients which contained gametocytes. The reaction included theuse of sporozoites fixed by treatment with 1% glutaraldehyde and ofanti-human gammaglobulin conjugate (Institut Pasteur). To date,only the lymphocytes of patients from Guinean Africa (Congo,Gabon, Benin) have proved to be producers of antisporozoiteantibodies. This region is characterised by high rainfall (> 1250 mm
per annum) and the virtually uninterrupted high transmission ofmalaria (80-400 potentially infecting mosquito bites per adult perannum 3).The antibodies seem to be directed against the membrane of the
parasite. Cell cloning is in progress with a view to obtaining stablelines secreting monoclonal antibodies, which could allowidentification of antigens of sporozoite stage of Pfalciparum.Central Parasitologyand Tropical Medicine Laboratory,
Hôpital de la Pitié-Salpétrière,75013 Paris, France
L. MONJOURC. ALFREDI. PLOTON
Tumour Epidemiologyand Immunovirology Laboratory,
Alexis Carrel Medical Faculty, Lyon C. DESGRANGES
ORSTOM,Bobo-Dioulasso, Upper Volta P. CARNEVALE
Central Parasitologyand Tropical Medicine Laboratory,
Hôpital de la Pitié-Salpétrière, Paris
D. MAZIERO. BRANDICOURT.M. GENTILINI
CYCLOSPORIN IN INFILTRATIVE EYE DISEASE
SIR,-Weetman et al4 have reported benefit from cyclosporin ininfiltrative eye disease in two patients with Graves’
ophthalmopathy. These encouraging results prompted us to trycyclosporin in three patients with long-standing Graves’ eyedisease grade IV-V, in whom corticosteroid therapy and, in twocases, retro-orbital irradiation had been unsuccessful.
Computerised tomography (CT), nuclear magnetic resonance
(NMR), and ultrasound studies of the eye muscles revealed
thickening of more than one orbital muscle (greatest thickness inCT and NMR being 10,9, and 9 mm in the three cases). During thestudy the patients were euthyroid (as measured by T3, T4, free T3,rT3 and TRH test). Cellular immunity was studied in two patientsand revealed a polyclonal B-cell activation with an excess of terminalB cells (15-20%) and an OKT 4/OKT 8 ratios of 1 - 38 and 1 - 6.Cyclosporin therapy was started at 5mg/kg in two doses, and drug
levels, measured radioimmunologically, lay in the .range foundeffective in kidney and liver transplantation (400-1000 ng/ml).5 Noside-effects of treatment, in respect of liver or kidney function, wereobserved.
1. Monjour L, Desgranges C, Alfred C, Ploton I, Karabinis A. Production of humanmonoclonal antibodies against asexual erythrocytic stages of Plasmodum falciparum.Lancet 1983; i: 1337-38.
2. Dubois Ph, DedetJP, Fandeur T, et al. Protective immunisation of the squirrel monkeyagainst asexual blood stages of Plasmodium falciparum using parasite proteinfraction. Proc Natl Acad Sci USA (in press).
3. Richard A. Aspects épidémiologiques et cliniques du paludisme dans les villages de laforêt du Mayombe (Congo). MD thesis, Paris, 1984.
4. Weetman AP, McGregor AM, Ludgate M, et al. Cyclosporin improves Graves’ophthalmopathy. Lancet 1983; ii: 486-89.
5. Wonigeit K, et al. Special aspects of immunosupression with cyclosporine in LiverTransplantation. Transplantation Proc 1983; 15: 2586-91.

516
After 8 weeks of therapy the immunological status was almostnormal in all three patients. Terminal B-cells returned to normalpercentages (1%, 2%) and OKT 4/OKT 8 ratios rose to 2-38 and2 60, respectively. This suggests that cyclosporin, at least for thedisturbed immunoregulation of infiltrative eye disease, is effective.However, clinically there was no improvement: no patient reportedany change in eye symptoms nor did CT, NMR, or ultrasoundappearances change.Thus in three patients with infiltrative eye disease who had had
eye symptoms for more than a year cyclosporin was not effective.Prospective studies of cyclosporin in rapidly progressive disease,with measurement of drug levels and CT measurement of eyemuscles, may be justified. r, r_ _ _ _ __
Departments of Internal Medicine,Radiology, Nuclear Medicine, and Surgery,
Medizinische Hochschule Hannover,D-3000 Hannover 61, West Germany
G. BRABANTH. PETERH. BECKERR. SCHWARZROCKK. WONIGEITR. D. HESCH
NECROTISING FASCIITIS DUE TO GROUP C AND GHAEMOLYTIC STREPTOCOCCUS AFTER CHIROPODY
SiR,-Two patients recently presented with necrotising fasciitis(gangrene)-one due to a group C and the other to a group G(3-haemolytic streptococcus. Group C and G streptococci have notpreviously been recorded as a cause of this infection.A 75-year-old woman with syringomyelia, but otherwise well and
mobile with the aid of a Zimmer frame, was seen at home by achiropodist who injured the skin when cutting the hail of her greattoe. 2 days after this minor injury, the toe was swollen, and within 3days cellulitis had spread into her calf. Several days later she wasadmitted to hospital with blistering and early necrosis over her calfwhich was thought likely to be due to Streptococcuspyogenes. She wastreated with high doses of penicillin and gentamicin (because of thepossibility of staphylococcal infection), although the first culturesfrom the superficial tissue grew neither aerobic nor anaerobicbacteria. 1 week later there was no further spreading cellulitis butthe necrotic tissue that remained required surgical debridement.The denuded area rapidly granulated and later healed withoutgrafting. Group G haemolytic streptococci were cultured fromnecrotic tissue removed at operation as deep as the fascia, despite thestreptococci being fully sensitive to penicillin.An 82-year-old woman with atherosclerosis was attended by
another chiropodist who also injured the skin near a toenail. Thispatient also had cellulitis, spreading from her toe, up her calf, toabove the knee. Sloughing necrosis developed rapidly at nearly thesame site as in the first case (figure). There was no bacterial growthfrom the surface tissue on admission but group C haemolyticstreptococci were grown from the deeper tissue obtained at
debridement.Necrotising fasciitis due to Strep pyogenes has been recognised
since 1924.1 However, the infection is seen more commonly now inelderly people2,3 and is often not diagnosed in its early stages.Antibiotics prevent spread of the infection but debridement is
eventually required; the streptococci are often grown from thenecrotic tissue because the penicillin does not penetrate. Thetreatment of choice is still removal of all necrotic tissue.4 4
The group G streptococcus from the first patient was T type7/PT5356 whilst the group C streptococcus from the second patientwas T type PT5582. The first patient had a rise in anti-streptolysin0 (ASO) from 140 to 800, and a rise in antibody titre to group C/Ghyaluronidase5 from 10 to 40. There was no rise in titre in the anti-
1. Meleney FL. Hemolytic streptococcus gangrene. Arch Surg 1924; 9: 317-64.2. Reid RI, Briggs RF, Seal DV, Pearson AD. Virulent Streptococcus pyogenes: Outbreak
and spread within a geriatric unit. J Infect 1983; 6: 219-25.3. Aitken DR, Mackett T, Smith LL. The changing pattern of hemolytic streptococcal
gangrene. Arch Surg 1982; 117: 561-67.4. Leppard BJ, Seal DV. The value of bacteriology and serology in the diagnosis of
necrotizing fasciitis. Br J Dermatol 1983; 109: 37-44.5 Hallas G, Widdowson JP. Antibody to hyaluronidases of streptococci of Lancefield
groups C and G. In: Holm SE, Christensen P, eds. Proceedings of the VIIIthinternational symposium on streptococci. Surrey, UK: Reed books, 1981.
DNase B test, which remained at 50, nor in antibodies to group A(Strep pyogenes) hyaluronidase which remained at 32, both being lownormal titres. The second patient had a rise in ASO from 280 to 720,but no rise in antibodies to group C/G hyaluronidase; there was alsono rise in antibody titres to group A DNase and hyaluronidase from50 and 32, respectively. In contrast, patients with necrotisingfasciitis due to Strep pyogenes acquired very high titres of specificanti-DNase B and anti-hyaluronidase;4 the failure to demonstratesuch antibodies in both our patients confirmed that the infectionwas not due. to that organism. However, the group C/G
hyaluronidase antigen is less potent than group A hyaluronidase, sothat a negative result does not exclude infection.Groups C and G haemolytic streptococci are recognised causes of
pharyngitis and cellulitis associated with chronic ulceration but areotherwise regarded to be of low virulence. They have occasionallybeen isolated from patients with septic arthritis, endocarditis,septicaemia, and pneumonia but neither have previously beenrecorded as a cause of necrotising fasciitis. These organismsoccasionally colonise the throat, rectum, and other sites such as toewebs (in up to 3% of the normal population) but are frequentlycommensal in the mouth and bowel of domestic animals. However,neither of our patients had rectal carriage of their strain nor did theykeep pets. Whilst both patients are elderly neither has diabetesmellitus, malignancy, or immunosuppression, which are recognisedconditions predisposing to streptococcal infection.
Case 2: Sloughing necrosis of calf.
Most clinicians dealing with elderly patients with vascular ordiabetic disease recognise chiropody as a potential cause ofinduction of both infection and unnecessary tissue trauma. Most ofthese infections result merely in local digital infection and/ornecrosis but they can, in the long term, be a precipitating factornecessitating either local or major amputation. Presumably, in bothour patients, the streptococci gained entrance to the tissues at thetime of trauma, and we have cultured these organisms from the toewebs of uninfected patients. We recommend that chiropodistsliberally apply an antiseptic to patients’ feet before they treat them.Products suitable for this purpose include chlorhexidine or
povidone iodine, but at least 5 min must be allowed for them to act;often chiropody begins too soon after the application of antiseptic.Washing the patients’ feet the day before with ’Hibiscrub’ (4%chlorhexidine/detergent) would be an added safeguard to preventinfection, particularly since chlorhexidine has a persistentantibacterial effect on the skin for at least 24 h.
We thank Dr G. Colman for T typing the group C and G streptococci, MissG. Hallas for the group C/G hyaluromdase antibody tests at the Central PublicHealth Laboratory, Colindale, and Dr R. Holliman for help in investigation ofthe patients.
Departments of Microbiology,Geriatrics, and Surgery,
Northwick Park Hospital,Harrow, Middx HA1 3UJ
N. GAUNTK. ROGERSD. SEALM. DENHAM
J. LEWIS
6. Editorial. Group G streptococci. Lancet 1984, i: 144.
















![Cyclosporin A-Induced Hyperlipidemia · 2012. 9. 30. · Cyclosporin A-Induced Hyperlipidemia 341 2.4. Plasma lipoprotein (a) Lipoprotein (a) [Lp(a)] is a LDL-like lipoprotein consisting](https://img.pdfslide.net/doc/110x75/60b482bc2d15520abb15cefc/cyclosporin-a-induced-hyperlipidemia-2012-9-30-cyclosporin-a-induced-hyperlipidemia.jpg)










