Embed Size (px)
Citation preview

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 1/12
Advertisement
Leading the way in experimentaland clinical research in hematology Advanced Search
search
D-dimer to guide the duration of anticoagulation in patientswith venous thromboembolism: a management study
Gualtiero Palareti , Benilde Cosmi , Cristina Legnani , Emilia Antonucci , Valeria De Micheli , Angelo Ghirarduzzi , Daniela Poli ,
Sophie Testa , Alberto Tosetto , Vittorio Pengo , and Paolo Prandoni , on behalf of the DULCIS (D-dimer and ULtrasonography in
Combination Italian Study) Investigators
Author Affiliations
Key Points
The duration of anticoagulation after VTE is uncertain; this management study intended to identify patients with low/high
recurrence risk.
Patients with persistently negative D-dimers after stopping standard therapy have a low recurrence risk and can stop
anticoagulation.
Abstract
The optimal duration of anticoagulation in patients with venous thromboembolism (VTE) is uncertain. We investigated whether
persistently negative D-dimers in patients with vein recanalization or stable thrombotic burden can identify subjects at low recurrence
risk. Outpatients with a first VTE (unprovoked or associated with weak risk factors) were eligible after at least 3 months (12 in those with
residual thrombosis) of anticoagulation. They received serial D-dimer measurements using commercial assays with predefined age/sex-
specific cutoffs and were followed for up to 2 years. Of 1010 patients, anticoagulation was stopped in 528 (52.3%) with persistently
negative D-dimer who subsequently experienced 25 recurrences (3.0% pt-y; 95% confidence interval [CI], 2.0-4.4%). Of the remaining 482
patients, 373 resumed anticoagulation and 109 refused it. Recurrent VTE developed in 15 patients (8.8% pt-y; 95% CI, 5.0-14.1) of the
latter group and in 4 of the former (0.7% pt-y; 95% CI, 0.2-1.7; hazard ratio = 2.92; 95% CI, 1.87-9.72; P = .0006). Major bleeding occurred
in 14 patients (2.3% pt-y; 95% CI, 1.3-3.9) who resumed anticoagulation. Serial D-dimer measurement is suitable in clinical practice for the
identification of VTE patients in whom anticoagulation can be safely discontinued. This study was registered at clinicaltrials.gov as
#NCT00954395.
Introduction
Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), tends to recur, especially
when the event is idiopathic or associated with a permanent prothrombotic conditions. The cumulative rate of recurrence 10 years after
withdrawal of anticoagulation was reported to be ∼50% in patients with a first unprovoked VTE and ∼20% after a provoked event.
Anticoagulation for 3 months is recommended in all VTE patients, whereas indefinite anticoagulation is suggested in patients with
idiopathic VTE and without high bleeding risk, because the recurrence rate after stopping anticoagulation is independent of the duration
of initial treatment.
Altered D-dimer levels after anticoagulation is stopped in patients with a first VTE and the persistence of residual vein thrombosis (RVT)
after DVT have been shown to be a risk factor for recurrence.
1 1 1 2 3 4 2
5 6 7 8
1
2
3
4,5
6
7
Home / July 10, 2014; Blood: 124 (2)
Current Issue First Edition Topics Collections All Issues Abstracts
Home About Blood Authors Submit to Blood Subscriptions Classifieds
ASH Home Blood App My Folders Alerts RSS Institution: GEORGE WASHINGTON UNIV MED CTR My Account Sign In
Skip to main content

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 2/12
Table 1
Criteria for exclusion/inclusion in the study
We performed a prospective cohort study in outpatients with a single episode of proximal DVT of the lower limbs and/or PE who had
received a standard course of anticoagulation (>3 months), or at least 12 months in case of RVT. We sought to assess whether a
management procedure involving serial D-dimer testing and RVT assessment can identify a subset of subjects at low risk of recurrence in
whom anticoagulation can be safely discontinued.
Methods
Study patients
This was a multicenter, prospective cohort study involving patients of both sexes aged ≥18 years who had experienced a first
symptomatic VTE episode, including proximal DVT of the legs, PE, or both, that was either idiopathic or associated with weak risk factors
(WRFs; Table 1). The index event was objectively confirmed by compression ultrasonography (CUS), ventilation-perfusion lung scan, or
computed tomographic pulmonary angiography (CTPA), as appropriate, and treated according to international guidelines, including
acute and long-term anticoagulant therapy and, in the case of DVT, compression elastic stockings (30-40 mm Hg at the ankle). All
screened patients were examined to assess for the presence of criteria for exclusion, for short or extended anticoagulation, and finally
for inclusion in the study (see detailed criteria in Table 1). Patients were eligible if they had completed at least 3 months of therapy with a
vitamin K antagonist (VKA, either warfarin [Coumadin, Bristol-Myers Squibb] or acenocoumarol [Sintrom, Novartis Pharma]), with a target
INR of 2.5 (range, 2.0-3.0).
Inclusion criteria
Age ≥18 y
First episode of proximal VTE of lower limbs and/or PE that was:
idiopathic or associated with one or more of following factors:
minor, arthroscopic, or laparoscopic general surgery
pregnancy or puerperium
contraceptive or replacement hormonal therapy
long trip (>6 h)
minor trauma (not requiring hospitalization, plaster casting, or immobilization)
hospitalization in a medical hospital
reduced mobility (not complete immobilization)
Anticoagulation therapy (VKA, INR 2.0-3.0) for at least 3 mo
Ability to provide informed consent
Prespecified criteria for exclusion
Age <18 y
Duration of anticoagulation <3 mo
Inability or refusal to give consent
Limited life expectation (<1 y)
Increased systolic pulmonary arterial pressure (values ≥35 mm Hg [or ≥40 mm Hg if BMI ≥30 or age ≥75 y] estimated with echocardiography)
Geographical inaccessibility
Venous thrombosis in different sites (upper limbs, splanchnic veins, jugular or cerebral veins)
Pregnancy or puerperium (first 6 weeks after birth) at the time of screening examination
Severe renal (creatinine level >2 mg/dL [177 μmol/L]) or liver failure (eg, acute hepatitis, chronic active hepatitis, or cirrhosis; or an alanine aminotransferase level that was 3 timesthe upper limit of the normal range or higher)
Criteria for short anticoagulation
VTE post major surgery (within 3 mo)
VTE post bed resting (≥4 d)
VTE post major trauma (within 3 mo)
VTE post plasters or immobilization (within 3 mo)
High bleeding risk
Criteria for extended anticoagulation
>1 documented VTE episode (proximal DVT and/or PE)
Active cancer or hematologic disease
Antithrombin deficiency
Antiphospholipid antibody syndrome (Sydney criteria)
PE with shock or life-threatening prolonged hypotension

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 3/12
BMI, body mass index; INR, international normalized ratio; NYHA, New York Heart Association.
Table 2
Age- and sex-specific cutoff levels for the different D-dimer assays adopted in the study
For comparison, the cutoff values recommended by manufacturers for VTE exclusion are also shown.
Table 1
Criteria for exclusion/inclusion in the study
Management procedures
All eligible patients were examined after at least 3 months of anticoagulation to assess their conditions for study enrollment. Before
inclusion, all patients received a bilateral CUS examination of the proximal deep veins (common femoral, superficial femoral, and
popliteal), and those presenting with RVT (>4-mm vein diameter at probe compression in the transverse section ) in at least one of the
aforementioned veins were included in the study only after completing a total of 12 months of VKA therapy.
All included patients underwent a serial D-dimer assessment starting at baseline during anticoagulation (T0). Patients with positive
baseline D-dimer (adopting the criteria indicated next) were instructed to continue anticoagulation, whereas those with negative D-dimer
were recommended to stop VKA and to repeat D-dimer testing after 15 to 18 days (T15), 25 to 35 (T30), 55 to 65 (T60), and 85 to 95
(T90) days from T0. Patients were recommended to resume anticoagulation at the first positive D-dimer result.
D-dimer assays and prespecified cutoff values
D-dimer levels were assessed with the quantitative assay routinely used in each participating center, provided that it was one of the
following: (1) VIDAS D-dimer Exclusion (bioMerieux, Lyon, France), (2) Innovance D-DIMER (Siemens, Deerfield, IL), (3) HemosIL D-dimer
HS (Instrumentation Laboratory, Milan, Italy), (4) HemosIL D-dimer (Instrumentation Laboratory), and (5) STA Liatest D-dimer
(DiagnosticaStago, Asnieres-sur-Seine, France). As discussed elsewhere, age and sex specific cutoff values were calculated for risk of
recurrence and used in the aforementioned tests, instead of those recommended by the manufacturers for VTE exclusion. These specific
cutoff values were determined by using stored frozen plasma aliquots collected from the patients included in the Prolong and Prolong
II studies. These aliquots were centralized in the coordinating center laboratory. Two predefinite criteria were adopted to select cutoff
values for the assays: (1) the percentage of patients with above cutoff D-dimer after one month from anticoagulation was stopped had to
be as close as possible to that obtained in the Prolong study at the same timing (36.7%) and within 95% confidence interval (CI, 32.8-
40.6), and (2) the percentage of VTE recurrence in patients with below cutoff D-dimer had to be as low as possible.
The adopted D-dimer cutoffs (Table 2) differed markedly in relation to age and sex. The adopted cutoffs for young males were similar or
even lower than those recommended for VTE exclusion; they were slightly higher for young females but noticeably higher for males and
females over 70 years.
Table 2
Age- and sex-specific cutoff levels for the different D-dimer assays adopted in the study
Study outcomes and follow-up
Patients were followed for a maximum of 2 years, and were seen at the clinical centers at intervals of 3 to 6 months, or they were
monitored for VKA dosing. Patients were instructed to contact the clinical center immediately in case of symptoms suggestive of VTE or
bleeding.
The main study outcome was the composite of confirmed recurrent VTE and death caused by VTE. In cases of suspected DVT recurrence,
Different indications for anticoagulation
Severe cardiorspiratory insufficiency (NYHA 3 or 4)
8
9
6
10
Commercial D-dimer assay (manufacturer)ng/mL
Males≤70 y
Males>70 y
Females≤70 y
Females>70 y
Cutoff values currently recommended by manufacturers for VTEexclusion
VIDAS D-dimer Exclusion (bio-Merrieux) 490 1050 600 1300 500
Innovance D-DIMER (Siemens) 500 950 550 1150 500
HemosIL D-dimer HS (InstrumentationLaboratory)
170 345 215 430 230
HemosIL D-dimer (InstrumentationLaboratory)
205 300 225 330 230
STA Liatest D-dimer (Diagnostica Stago) 340 700 450 1050 500

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 4/12
CUS results were compared with those of the last available previous examination. Any recurrent DVT was adjudicated if a previously fully
compressible segment (contralateral or ipsilateral) was no longer compressible or if an increase of at least 4 mm in the diameter of the
residual thrombus during compression was detected. In patients with suspected PE, recurrence was diagnosed on the basis of objective
algorithms incorporating clinical probability; ventilation-perfusion lung scanning; or CTPA, CUS, and/or D-dimer testing as
appropriate. Major bleeding events, defined by the International Society of Thrombosis and Haemostasis, were also recorded.
All suspected outcome events and deaths were evaluated by a central adjudication committee whose members were unaware of patient
name, D-dimer testing results at inclusion, management, or enrolling center. All patients gave their written informed consent for
participation. The institutional review boards of all participating centers approved the study, which was conducted in accordance with the
Declaration of Helsinki.
Statistical analysis and sample size
On the basis of a cumulative recurrence rate in patients with provoked VTE of 6.7% after 24 months from VKA suspension, we designed
the study to have an 80% power to detect a recurrence rate below a clinically acceptable incidence of 9% of the composite end point after
24 months. According to Shen, the required sample size in those suspending VKA was 530.
Differences between groups were assessed using the χ test with Yates’ correction for categorical variables and the Mann-Whitney U test
for continuous variables. Kaplan-Meier survival curves were plotted to estimate the cumulative incidence of symptomatic recurrent VTE;
hazard ratios (HR) and their 95% CIs were calculated. The data were analyzed with the use of Prism software (Version 3.0, GraphPad
Software Incorporated, San Diego, CA) and SPSS software (version 11.0 SPSS Inc., IBM, Armonk, NY).
Results
Patients and management
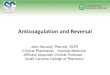
Figure 1 shows the study flow chart. In the 18 participating centers, 2458 patients with a first episode of VTE were screened between July
2008 and December 2011. Of these patients, 1401 (57.0%) were excluded for predefined criteria (442) or for criteria leading to short
(353) or extended anticoagulation (606). A total of 1057 patients (43.0% of the screened population) were eligible. Forty-seven (4.4%)
patients were then excluded from the study because of consent withdrawal (16) or for conditions requiring continued anticoagulation
(27), or they were lost to follow-up after the first D-dimer test (4). The remaining 1010 patients (560 males) followed the management
procedure and were analyzed; the index event was idiopathic in 771 (76.3%) patients and was associated with WRF in the remaining 239
(23.7%).
Figure 1
Flow chart of the DULCIS study. The prespecified criteria for exclusion from the study andfor short or extended anticoagulant treatment are reported in Table 1. #Patients wereexcluded for the following reasons: consent withdrawal (16), presented conditions requiringanticoagulation (27), had only the first D-dimer testing, were then lost to follow up (4).
Table 3 shows the characteristics of the analyzed patients. D-dimer was persistently negative (below cutoff levels) in 528 patients (52.3%;
277 males) who stopped anticoagulation and included 15 patients (as intention-to-treat analysis) with incomplete serial D-dimer testing
and/or a short follow-up. D-dimer was positive (above cutoffs) in 482 (47.7%) patients (significantly older than those with normal D-
dimer) who were advised to resume VKAs at the first positive D-dimer result. However, 109 of these (10.8%, 70 males; 22.6% of all the
8
11,12
13
14
15
2

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 5/12
Table 3
Baseline characteristics of the 1010 study patients
FU, follow-up; IQ, interquartile range; NA, not available.
|
* Fifteen of these patients were included in the analysis (as intention-to-treat), though their serial D-dimer testing was still incomplete (being enrolled late) and/or
had a short follow-up.
subjects with positive D-dimer) refused to do so and continued follow-up, whereas the remaining 373 (36.9%; 213 males), significantly
older than those who refused, resumed anticoagulation therapy. The prevalence of positive D-dimer was significantly higher in patients
with an idiopathic index event (51.1%) than in those with events associated with WRF (36.8%, P < .0001); it was lower (P < .01) in young
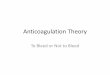
females (38.3%) than in the other subgroups in which the prevalence ranged between 50.4% and 53.7%. As is shown in Figure 2, the
highest rate of positive D-dimer in the whole study population was detected at 15 days (20.8%) after stopping anticoagulation, with an
overall positivity of 48.8% at the end of serial testing (at 90 days). A persistent RVT was detected in 119 patients, of whom 56 had negative
D-dimer (10.6% of the 528 total patients with persistently negative assay), and 63 had positive D-dimer (13.1% of the 482 patients with
positive assay).
Table 3
Baseline characteristics of the 1010 study patients
Characteristic Negative D-dimer(N = 528)
Positive D-dimer(N = 482)
Pvalue
Positive D-dimer withoutanticoagulation (N = 109)
Positive D-dimer withanticoagulation (N = 373)
Pvalue
Male sex, n (%) 277 (52.5) 283 (58.7) .055 70 (64.2) 213 (57.1) .230
Age (y), median (IQ) 63 (45-75) 69 (58-79) <.0001 64 (49-72) 71 (61-80) <.0001
Age >70 y, n (%) 201 (38.1) 223 (46.3) .011 32 (29.3) 191 (51.2) <.0001
Type of VTE, n (%)
Proximal DVT with no PE 285 (54.5) 244 (51.4) .384 53 (49.1) 191 (52.0) .677
DVT plus symptomatic PE 97 (18.5) 113 (23.8) .037 26 (24.1) 87 (23.7) .968
Isolated PE 141 (27.0) (5 NA) 118 (24.8) (7 NA) .379 29 (26.8) (1 NA) 89 (24.3) (6 NA) .689
Type of risk factors, n (%)
Idiopathic 377 (71.4) 394 (81.7) <.0001 83 (76.1) 311 (83.4)
WRFs 151 (28.6) 88 (18.3) <.0001 26 (23.9) 62 (16.6) .115
Minor general, laparoscopic, orarthroscopic surgery
7 2 1 1 .115
Pregnancy or puerperium 3 1 1 0
Hormonal contraceptivereplacement therapy
90 30 11 19
8 2 1 1
Long travel 5 8 3 5
Minor trauma, leg injury, reducedmobility
17 20 8 13
Hospitalization in a medical ward 21 27 1 23
Duration of previousanticoagulation, n (%)
≤6 mo 160 (30.3) 141 (29.3) .784 29 (26.6) 112 (30.0) .574
7-12 mo 297 (56.2) 272 (56.4) 1.000 61 (56.0) 211 (56.6) .999
>12 mo 71 (13.5) 69 (14.3) .786 19 (17.4) 50 (13.4) .375
Total duration of FU for all patients,y
829 772 171 601
FU, y, median (IQ) 1.93 (1.25-2.00) 1.90 (1.29-2.00) .508 1.97 (1.23-2.00) 1.88 (1.29-2.00) .990
Duration of FU, n
2 y 266 239 59 180
1-2 y 169 165 29 136
<1 y 57 49 7 42
Patients censored during FU, n (%) 36 (6.8) 29 (6.0) .697 14 (12.8) 15 (4.0) .002
Lost to FU, n (%) 6 (1.1) 1 (0.2) .179 1 (0.9) 0 .535
Presence of RVT (>4 mm), n (%) 56 (10.6) 63 (13.1) .263 5 (4.6) 58 (15.5) .005
Associated antiplatelet treatment, n(%)
53 (10.0) 42 (8.7) .553 10 (9.2) 32 (8.6) .999
*

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 6/12
Table 4
Clinical events occurred in the investigated patients
SVT, superficial vein thrombosis.
|
* Total follow-up.
|
† No death could be attributed to thrombotic event.
Figure 2
Prevalence of first-time-ever D-dimer result above the predefined cutofflevels in the investigated study population at the serial measurementdays after VKA withdrawal. The percentages are calculated vs the totalnumber of patients included.
Outcomes
Primary outcomes (Table 4) occurred in 25 of 528 patients with negative D-dimer (4.7%; 95% CI, 3.2-6.9; 3.0 per 100 pt-y, 95% CI, 2.0-4.4)
and in 15 of 109 patients who had positive D-dimer results but refused to resume anticoagulation (13.8%; 95% CI, 7.9-21.7; 8.8 per 100
pt-y; 95% CI, 5.0-14.1). The HR of outcome incidence of the latter vs the former was 2.92 (95% CI, 1.87-9.72; P = .0006). The effect of age,
sex, and type of index event on the occurrence of primary outcomes in patients who did not resume anticoagulation is shown in Table 5.
In patients with negative D-dimer, events were significantly more frequent in those aged >70 years than in younger patients (8.9% vs 2.1%;
P = .0008), and in patients with idiopathic than in those with secondary VTE (6.1% vs 1.3%; P = .036), although no differences were present
in relation to age and type of index event in patients with positive D-dimer. No difference was detected between males and females, either
with negative or positive D-dimer. Thirty of 120 women who received hormonal contraception at the moment of the event (included in the
study for this WRF) had positive D-dimer. However, 11 of them refused to resume anticoagulation and there was subsequently one
recurrent event in this subgroup (9.1%; 4.9% per 100 pt-y), whereas only one event occurred in the remaining 90 women who always had
negative D-dimer (1.1%; 0.65 per 100 pt-y). Four events (1 young male and 3 elderly women, all with negative D-dimer at T0) occurred
during the interval before the T15 D-dimer control. In patients with positive D-dimer, there were no differences in age, sex, or type of
index event. Among all patients who did not resume anticoagulation, there was no difference in recurrence in those either with or
without RVT (5.3% vs 6.3%, respectively) or in those who either received aspirin or did not (6.3% vs 6.2%, respectively).
Negative D-dimer, no anticoagulation (n =528; 829 y)
Positive D-dimer, anticoagulation refused (n= 109; 171 y)
Positive D-dimer, anticoagulation resumed (n= 373; 601 y)
Primary outcomes, n, %(95% CI)
25 (4.7%; 3.2-6.9) 15 (13.8%; 7.9-21.7) 4 (1.1%; 0.3-2.7)
Incidence per 100 pt-y, %(95% CI)
3.0% (2.0-4.4) 8.8% (5.0-14.1) 0.7% (0.2-1.7)
Type of event(idiopathic), n
DVT 16 (14) 8 (6) 1
PE 5 (5) 3 (3) 2 (1)
DVT+PE 4 (3) 4 (2) 1
Other outcomes, n
Death 1 0 5
Isolated distal DVT 9 2 0
SVT 19 2 2
Arterial vascular event 3 0 1
Major bleeding, n, % (95%CI)
0 0 14 (3.7%; 2.1-6.2)
Incidence per 100 pt-y, %(95% CI)
2.3% (1.3-3.9)
* * *
§
¶
†
‡

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 7/12
|
‡ 1 major bleeding was fatal.
|
§ P = .0008 patients with negative D-dimer.
|
¶ P < .0009 vs patients with negative D-dimer.
Table 5
Cumulative rates (no. per 100 patient-years) of primary study outcomes in relation to age, sex, and type of index event in patients who did not resume anticoagulation
Table 4
Clinical events occurred in the investigated patients
Table 5
Cumulative rates (no. per 100 patient-years) of primary study outcomes in relation to age, sex, and type of index event in patients who did not resumeanticoagulation
Among the patients with positive D-dimer who did not resume anticoagulation, the rate of recurrence was higher in those whose D-dimer
became positive within one month from VKA withdrawal than in those whose D-dimer became positive later; however, the difference did
not reach statistical difference, probably owing to the low number of cases (13/77 [16.9%] vs 2/32 [6.2%], P = .247; the 2 subjects with
late-positive D-dimer who recurred were both young).
In patients who resumed anticoagulation after a positive D-dimer result, 4 thrombotic events (1.1%; 95% CI, 0.3-2.7; 0.7 per 100 pt-y, 95%
CI, 0.2-1.7) and 14 major hemorrhages (fatal in 1) (3.7%, 95% CI, 2.1-6.2; 2.3 per 100 pt-y, 95% CI, 1.3-3.9) occurred. The rate of bleeding
was higher in elderly (4.7%) than in younger (2.7%) patients, but the difference was not significant (P = .460).
Discussion
Our study shows that a management procedure based on repeated D-dimer testing can be used in patients with a single VTE event that is
either idiopathic or associated with WRFs to identify those with a low risk of recurrence and in whom anticoagulation can be discontinued.
Anticoagulation was withdrawn on the basis of D-dimer tests persistently below age- and gender-specific cutoffs in >50% of patients, in
whom the subsequent annual recurrence rate was 3%. The recurrence rate in the present study was below the rates recommended as
acceptable by the Subcommittee on Control of Anticoagulation of the International Society on Thrombosis and Haemostasis to justify
stopping anticoagulant therapy (5% at 1 year and 15% at 5 years, with an upper boundary limit of 8% at 1 year).
In our study, all the screened patients underwent investigation for the presence of RVT before inclusion, and those with RVT were
included only after completing one year of anticoagulation. RVT has long been considered a predictor of recurrence and a criterion
to guide the duration of anticoagulation. A recent systematic review of available studies found that RVT is associated with a
significant, albeit modest, increase in the risk of recurrent VTE in patients with (unprovoked or provoked) DVT. The authors concluded
that the role of RVT in assessing the risk of recurrent VTE after stopping anticoagulation in patients with unprovoked DVT remains
unclear and warrants further investigations. Although the present study was not designed to give an answer to the issue of whether
detecting RVT may help guide the duration of anticoagulation, we decided to give patients with RVT a period of anticoagulation long
enough (1 year) to achieve a steady-state thrombus condition before starting D-dimer measurements. Of interest, in our cohort patients
who did not resume anticoagulation, we failed to show any appreciable difference in recurrence rates between those with and without
RVT.
Regarding D-dimer measurement, the current study had important differences from the previous and similar Prolong and Prolong II
studies, in which the same assay (qualitative and calibrated for VTE exclusion) was used in all participating centers. In the present
Age Sex Type of index event
≤70 y >70 y Pvalue
Males Females Pvalue
Idiopathic WRF Pvalue
Patients with negative D-dimer, n (%) 327 (61.9) 201 (38.1) 277 (52.2) 251 (47.8) 377 (71.4) 151 (28.6)
Primary outcomes, % (95% CI) 2.1 (0.9-4.4)
8.9 (5.4-13.8)
.0008 4.7 (2.5-7.9)
4.8 (2.5-8.2)
.886 6.1 (3.9-9) 1.3 (0.2-4.7)
.036
Patients with positive D-dimer who did not resumeanticoagulation n (%)
77 (70.6) 32 (29.4) 70 (64.2) 39 (35.8) 83 (76.1) 26 (23.9)
Primary outcomes, % (95% CI) 14.3 (7.4-24.1)
12.5 (3.5-29.0)
.956 10.0 (4.1-19.5)
20.5 (9.3-36.5)
.220 15.7 (8.6-25.3)
7.7 (1.0-25.1)
.483
16
17⇓-19
7,20 21
6,10

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 8/12
study, centers used their routine commercial quantitative assay, but with age- and sex-specific cutoffs. D-dimer levels increase with
age and are higher in women. Compared with the cutoff levels recommended by manufacturers for VTE exclusion, those set for
this study were much higher in elderly patients, but were similar or even lower in younger patients, especially in men. As a result, more
elderly patients discontinued anticoagulation, whereas the opposite was true for younger patients, especially males. This effect, together
with the higher thrombosis risk associated with age, may account for the higher recurrence rate in elderly than in younger patients. Lower
cutoff levels might have further lowered the recurrence rate in elderly patients; however, this would have been offset in part by an
increase in the proportion of those to be anticoagulated indefinitely, with the associated bleeding risk. Although the cutoff levels adopted
in the present study for young subjects proved to be very effective, we believe that a refinement in the cutoff levels for elderly patients is
advisable to optimize the relationship between an acceptable rate of recurrence and the proportion of anticoagulated patients. We
currently cannot indicate specific cutoff values, different from those used in the study, to be recommended for managing this patient
population, and we propose this issue as an important target for future clinical studies.
In the Prolong study, D-dimer was tested only once at one month after VKA interruption, whereas in the Prolong II study, patients whose
D-dimer levels became abnormal beyond one month after VKA withdrawal had a higher risk of recurrence. As is shown in Figure 2, the
highest rate of positive D-dimer tests was detected after 15 days (20.8%), with 13.1% positive results at 30 days after VKA withdrawal and
another 10% positive results afterward. Among the patients who refused to resume anticoagulation, the recurrence rate in those whose D-
dimer became positive after one month (2 cases, both young patients) was lower but not statistically different than in those with earlier
positive results. Although we may suggest omitting the D-dimer measurement during anticoagulation (T0) in clinical practice (4 very early
recurrences could not be avoided after a negative D-dimer at T0), we believe that the present results confirm the validity of extending D-
dimer assessment beyond one month to increase the protection from recurrence, especially in young patients.
The risk of recurrent VTE has consistently been found to be higher in men than in women. In our study, the difference in the
recurrence rate between men and women disappeared when the comparison was made separately among patients with or without
positive D-dimer (Table 5). This suggests that D-dimer is an important marker of recurrent thromboembolism and has the potential to
compensate for the difference in the gender-related recurrence risk once a proper adjustment of cutoff levels is performed.
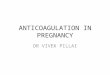
Patients were invited to prolong or resume anticoagulation as soon as the D-dimer test result was positive. However, approximately one-
fifth of patients refused to resume VKA, and their recurrence rate was about threefold higher than in patients with persistently negative D-
dimer (Figure 3). Patients with positive D-dimer who refused to resume anticoagulation were significantly younger than those who agreed
to resume anticoagulation, thus showing that young patients with a first VTE are more reluctant to accept an indefinite anticoagulation;
no other significant differences could be detected between these 2 groups (Table 3). These results provide further compelling evidence
that D-dimer testing can be used to distinguish patients with a high recurrence risk.
Figure 3
Kaplan-Meier cumulative event rates for the primary efficacy outcome inpatients with persistently negative D-dimer results in whomanticoagulation was definitively stopped (dotted line) and in those withpositive D-dimer results who refused to resume anticoagulation(continuous line).
The risk of recurrence is higher after idiopathic events ; however, it is not negligible when the events are associated with WRFs. In fact,
Iorio et al showed a recurrence rate of 4.2% patient-years in subjects whose index event was secondary to nonsurgical risk factors. The
proportion of patients with VTE events associated with WRFs is generally relevant (one-fourth of all included patients in our study) and it
is important to give them justified clinical advice. This is why our study included patients with either idiopathic events or events associated
with WRFs, because we intended to propose and analyze the efficacy and safety of a practical model to manage the duration of
anticoagulation in patients after a first VTE event. Our study showed that the majority of the patients with an index event associated with
a WRF (64.4%) had negative D-dimer and stopped anticoagulation. As expected, among the patients with positive D-dimer who did not
resume anticoagulation, the rate of recurrence was almost twice as high in patients with an idiopathic event as in those with WRFs;
however, among the latter patients, the rate of recurrence was higher in those with positive than in those with negative D-dimer (Table 5;
22⇓-24 25
6
10
26⇓⇓⇓-30
1,2
14

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 9/12
the difference did not reach statistical significance, probably for the limited number of patients). Furthermore, among young women who
had a VTE during hormonal contraception, a population usually considered at low risk, one case of recurrence occurred among the 11 of
those with positive D-dimer who did not resume anticoagulation, and only one recurrence occurred among the 90 of them with negative
D-dimer (9.1% vs 1.1%). These results, while confirming the higher risk of recurrence when the index VTE event is idiopathic, also indicate
that D-dimer can be useful to evaluate the risk of recurrence in individual patients with nonidiopathic VTE.
Among the 373 patients who resumed anticoagulation, 4 experienced VTE events (1.1%) (mainly in association with temporary
interruption of anticoagulation), and 14 (3.7%) had major bleeding events (1 fatal) during follow-up. Thus, the cumulative rate of harmful
events associated with anticoagulation in these subjects was not different from that observed in patients with negative D-dimer who
discontinued anticoagulation. This further supports the benefit of identifying patients at lower risk of recurrence in whom
anticoagulation can be discontinued.
The most innovative aspects of the management procedure adopted in this study also have potential limitations. First, serial D-dimer
testing may be inconvenient for both patients and physicians; to simplify this approach, we suggest the omission of testing during
anticoagulation (T0), but we still advise to repeat D-dimer measurement beyond one month after anticoagulation is stopped. Second,
some patients, especially younger ones, can disagree with prolonging or resuming anticoagulation based only on a single blood test
result. Third, the age and sex-specific D-dimer cutoff levels adopted in this study for patients aged >70 years were substantially high
(twice as high as the upper normal limit indicated for diagnostic purposes). This may generate some confusion in professionals used to
the cutoffs established for VTE exclusion and may raise perplexity in labeling as negative such high results. Finally, repeating the D-dimer
assay in the first 3 months after anticoagulation is stopped, using cutoff values different than those for VTE exclusion, may generate
confusion in professionals, especially in the case of VTE recurrence suspicion during this period.
In conclusion, our study showed that, based on persistently normal D-dimer tests, anticoagulation could be stopped in >50% of patients
included after a single idiopathic VTE or associated with WRFs; the recurrence rate during follow-up was as low as 3.0 per 100 pt-y (95%
CI, 2.0-4.4), which is below the rates recommended as acceptable to justify anticoagulation discontinuation.
Authorship
Contribution: All authors contributed to the design of the study; B.C., V.D.M., A.G., D.P., S.T., and A.T. contributed to data collection; B.C.,
E.A., and C.L. contributed to data analysis; all authors contributed to the interpretation of the data collected; and G.P. wrote the first draft
of the manuscript, and all the authors contributed to its final changes.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
A full list of study investigators can be found in the Appendix.
Correspondence: Gualtiero Palareti, Department of Angiology & Blood Coagulation, University Hospital Policlinico S. Orsola-Malpighi, Via
Albertoni 15, 40138 Bologna, Italy; e-mail: [email protected].
Acknowledgments
The Italian Federation of Anticoagulation Clinics (FCSA) supported this study by inviting the affiliated centers to take part in the study and
by organizing and supporting the meetings necessary to start and finalize the study. The Department of Angiology and Blood
Coagulation of University Hospital of Bologna supported the collection and analysis of the data
Appendix
The following were members of the DULCIS study group (the numbers of patients who participated in the study appear in parentheses):
Gualtiero Palareti, Benilde Cosmi, Cristina Legnani, Divisione di Angiologia e Malattie della Coagulazione, Azienda Ospedaliero–
Universitaria di Bologna, Policlinico S. Orsola–Malpighi, Bologna, Coordinator Center (270); Nicoletta Erba, Valeria De Micheli, U.O.
Patologia Clinica, Azienda Ospedaliera provincia di Lecco (139); Angelo Ghirarduzzi, Maria Rosaria Veropalumbo, Ugolotti Maria Chiara,
Angiologia, ASMN-IRCCS–Reggio Emilia, Reggio Emilia (126); Daniela Poli, Domenico Prisco, Emilia Antonucci, Malattie Aterotrombotiche,
AOU–Careggi, Firenze (114); Sophie Testa, Oriana Paoletti, Centro Emostasi e Trombosi, AO Istituti Ospitalieri, Cremona (87); Alberto
Tosetto, Divisione Ematologia, Ospedale S. Bortolo ULSS 6–Vicenza (54); Anna Falanga, Teresa Lerede SIMT Centro Emostasi e Trombosi
Ospedali Riuniti di Bergamo (48); Steidl Luigi, Marco Donadini, Elena Rancan, Medicina Interna 1°–Ambulatorio Emostasi e Trombosi,
Ospedale Di Circolo-Università dell'Insubria, Varese (42); Roberto Quintavalla, Piera Maria Ferrini, Medicina Interna a d indirizzo
Angiologico e Coagulativo, Ospedale Maggiore Azienda Ospedaliero–Universitaria di Parma (36); Rita C. Santoro, Centro Emofilia
Emostasi e Trombosi, Az. Osp. “Pugliese-Ciaccio”, Catanzaro (34); Francesco Orlandini, Raffaella Benedetti, Medicina Interna, Osp. Civile
S.Andrea–ASL 5 presidio Levante Ligure, La Spezia (32); Marco Cattaneo, Federico Lussana, Elena Bertinato, Medicina III, A.O. San Paolo–
16

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 10/12
Università di Milano, Milano (28); Roberto Cappelli, Medicina Interna 2, Azienda Ospedaliero–Universitaria Senese, Siena (21); Attilia Maria
Pizzini, Medicina 1° Centro Emostasi e Trombosi, Ospedale Santa Maria Nuova, Reggio Emilia (20); Lucia Angeloni, Geriatria, Ospedale
Maggiore Bologna (10); Armando D’Angelo, Luciano Crippa, Ambulatorio Emostasi e Trombosi, Ospedale S. Raffaele, Milano (10); Roberta
Bortolotti, Medicina, Ospedale di San Giovanni Persiceto, Bologna (8); Maria Rita Vandelli, Med. Cardiovascolare–Mod. Organizzativo
Angiologia, Centro Trombosi, Nuovo Ospedale Civile S. Agostino Estense, Baggiovara Modena (4). Executive Committee: Gualtiero Palareti
(Bologna), Vittorio Pengo (Padova), Paolo Prandoni (Padova); Steering Committee: Walter Ageno (Varese), Angelo Ghirarduzzi (Reggio
Emilia), Domenico Prisco (Firenze), Sophie Testa (Cremona), Alberto Tosetto (Vicenza), Armando Tripodi (Milano); Adjudication
Committee: Davide Imberti (Piacenza), Marco Moia (Milano), Raffaele Pesavento (Padova); External Safety Committee: Nicola Magrini
(Bologna), Francesco Marongiu (Cagliari), Pietro Zonzin (Rovigo); Scientific Secretariat: Benilde Cosmi (Bologna); referent for laboratory
issues: Cristina Legnani (Bologna); data manager (collection and processing): Noemi Piaggesi (Bologna); data analysis: Benilde Cosmi
(Bologna), Daniela Poli (Firenze), Mauro Silingardi (Reggio Emilia).
Footnotes
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this
article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Submitted January 6, 2014.
Accepted May 7, 2014.
© 2014 by The American Society of Hematology
References
1. Christiansen SC, Cannegieter SC, Koster T, Vandenbroucke JP, Rosendaal FR. Thrombophilia, clinical factors, and recurrent venous thrombotic events.
JAMA 2005;293(19):2352-2361.
2. Prandoni P, Noventa F, Ghirarduzzi A, et al. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute
proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica 2007;92(2):199-205.
3. Kearon C, Akl EA, Comerota AJ, et al. Chest . Vol. 141.(2 Suppl) 2012. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention
of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines.; p. e419S-e494S.
4. Agnelli G, Prandoni P, Santamaria MG, et al; Warfarin Optimal Duration Italian Trial Investigators. Three months versus one year of oral anticoagulant
therapy for idiopathic deep venous thrombosis. N Engl J Med 2001;345(3):165-169.
5. Boutitie F, Pinede L, Schulman S, et al. Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism
on risk of recurrence after stopping treatment: analysis of individual participants’ data from seven trials. BMJ 2011;342:d3036.
6. Palareti G, Cosmi B, Legnani C, et al; PROLONG Investigators. D-dimer testing to determine the duration of anticoagulation therapy. N Engl J Med
2006;355(17):1780-1789.
7. Prandoni P, Prins MH, Lensing AW, et al; AESOPUS Investigators. Residual thrombosis on ultrasonography to guide the duration of anticoagulation in
patients with deep venous thrombosis: a randomized trial. Ann Intern Med 2009;150(9):577-585.
8. Prandoni P, Cogo A, Bernardi E, et al. A simple ultrasound approach for detection of recurrent proximal-vein thrombosis. Circulation 1993;88(4 Pt
1):1730-1735.
9. Legnani C, Cini M, Cosmi B, et al. Age and gender specific cut-off values to improve the performance of D-dimer assays to predict the risk of venous
thromboembolism recurrence. Intern Emerg Med 2013;8(3):229-236.
10. Cosmi B, Legnani C, Tosetto A, et al; PROLONG Investigators (on behalf of Italian Federation of Anticoagulation Clinics). Usefulness of repeated D-
dimer testing after stopping anticoagulation for a first episode of unprovoked venous thromboembolism: the PROLONG II prospective study. Blood
2010;115(3):481-488.
11. Fedullo PF, Tapson VF. Clinical practice. The evaluation of suspected pulmonary embolism. N Engl J Med 2003;349(13):1247-1256.
12. Kearon C. Diagnosis of pulmonary embolism. CMAJ 2003;168(2):183-194.
13. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on
Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 11/12
Thromb Haemost 2005;3(4):692-694.
14. Iorio A, Kearon C, Filippucci E, et al. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk
factor: a systematic review. Arch Intern Med 2010;170(19):1710-1716.
15. Shen LZ. Sample size determination for controlling the upper confidence limit of incidence rate of a binomial endpoint. J Biopharm Stat
1998;8(3):489-496.
16. Kearon C, Iorio A, Palareti G; Subcommittee on Control of Anticoagulation of the SSC of the ISTH. Risk of recurrent venous thromboembolism after
stopping treatment in cohort studies: recommendation for acceptable rates and standardized reporting. J Thromb Haemost 2010;8(10):2313-2315.
17. Prandoni P, Lensing AWA, Prins MH, et al. Residual venous thrombosis as a predictive factor of recurrent venous thromboembolism. Ann Intern Med
2002;137(12):955-960.
18. Piovella F, Crippa L, Barone M, et al. Normalization rates of compression ultrasonography in patients with a first episode of deep vein thrombosis of
the lower limbs: association with recurrence and new thrombosis. Haematologica 2002;87(5):515-522.
19. Young L, Ockelford P, Milne D, Rolfe-Vyson V, Mckelvie S, Harper P. Post-treatment residual thrombus increases the risk of recurrent deep vein
thrombosis and mortality. J Thromb Haemost 2006;4(9):1919-1924.
20. Siragusa S, Malato A, Saccullo G, et al. Residual vein thrombosis for assessing duration of anticoagulation after unprovoked deep vein thrombosis of
the lower limbs: the extended DACUS study. Am J Hematol 2011;86(11):914-917.
21. Carrier M, Rodger MA, Wells PS, Righini M, LE Gal G. Residual vein obstruction to predict the risk of recurrent venous thromboembolism in patients
with deep vein thrombosis: a systematic review and meta-analysis. J Thromb Haemost 2011;9(6):1119-1125.
22. Hager K, Platt D. Fibrin degeneration product concentrations (D-dimers) in the course of ageing. Gerontology 1995;41(3):159-165.
23. Pieper CF, Rao KMK, Currie MS, Harris TB, Cohen HJ. Age, functional status, and racial differences in plasma D-dimer levels in community-dwelling
elderly persons. J Gerontol A Biol Sci Med Sci 2000;55(11):M649-M657.
24. Harper PL, Theakston E, Ahmed J, Ockelford P. D-dimer concentration increases with age reducing the clinical value of the D-dimer assay in the
elderly. Intern Med J 2007;37(9):607-613.
25. Rudnicka AR, Rumley A, Lowe GDO, Strachan DP. Diurnal, seasonal, and blood-processing patterns in levels of circulating fibrinogen, fibrin D-dimer,
C-reactive protein, tissue plasminogen activator, and von Willebrand factor in a 45-year-old population. Circulation 2007;115(8):996-1003.
26. Kyrle PA, Minar E, Bialonczyk C, Hirschl M, Weltermann A, Eichinger S. The risk of recurrent venous thromboembolism in men and women. N Engl J
Med 2004;350(25):2558-2563.
27. Baglin T, Luddington R, Brown K, Baglin C. High risk of recurrent venous thromboembolism in men. J Thromb Haemost 2004;2(12):2152-2155.
28. McRae S, Tran H, Schulman S, Ginsberg J, Kearon C. Effect of patient’s sex on risk of recurrent venous thromboembolism: a meta-analysis. Lancet
2006;368(9533):371-378.
29. Rodger MA, Kahn SR, Wells PS, et al. Identifying unprovoked thromboembolism patients at low risk for recurrence who can discontinue anticoagulant
therapy. CMAJ 2008;179(5):417-426.
30. Eichinger S, Heinze G, Jandeck LM, Kyrle PA. Risk assessment of recurrence in patients with unprovoked deep vein thrombosis or pulmonary
embolism: the Vienna prediction model. Circulation 2010;121(14):1630-1636.
Advertisement
Leading the way in experimental andclinical research in hematology
American Society of Hematology2021 L Street NW, Suite 900, Washington, DC 20036Phone 202-776-0544 | Fax 202-776-0545
Current Issue Subscriptions Submit to Blood Information for:

7/18/2014 Blood Journal | D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
http://www.bloodjournal.org.proxygw.wrlc.org/content/124/2/196.full.print? 12/12
First Edition
Topics
Collections
All Issues
Abstracts
About Blood
Newsroom
Public Access
Permissions
Order Reprints
Alerts
RSS
Blood App
Contact Us
Feedback
Authors
Subscribers
Institutions/Librarians
Advertisers
ASH Home Research Education Advocacy Meetings ASH Store
Copyright © 2014 by American Society of Hematology