Embed Size (px)
Citation preview
EGFR pharmDxTM Interpretation Manual
P A T H O L O G Y
For In Vitro Diagnostic Use. FDA-approved as an aid in identifying colorectal cancer patients eligible for treatment with Erbitux® (cetuximab) and VectibixTM (panitumumab).


�EGFR pharmDx™ Interpretation Manual
TAb
lE oF C
on
TEnTs
Introduction 2
EGFR overview 3n EGFR and the HER Family
n EGFR Expression in normal Tissue
The EGFR pharmDx™ Kit 5
Expression Rates and Recommended Data Tracking for EGFR pharmDx™ 6
Technical Tips for optimal EGFR pharmDx™ Performance 7n Tissue Fixation and Variables
n EGFR pharmDxTM Protocol Recommendations
n EGFR pharmDxTM Training Checklist
Quality Control 9
EGFR pharmDx™ Evaluation and Reporting 10n slide Evaluation
n steps to EGFR pharmDxTM Evaluation
Image Guide for Interpretation 12n EGFR pharmDxTM Interpretation Guidelines
staining Patterns 13n Heterogeneous staining
n Homogeneous staining
n EGFR staining of normal and benign Tissues
Factors to Consider in Evaluating EGFR pharmDx™ stains 16n non-specific background
n Possible Causes of non-specific background
Artifacts 17n overdigestion
n Post-Fixation Procedure
n Crush Artifact
n Edge Artifact
n Retraction Artifact
n Thermal Artifact
n non-Evaluable Areas of Tissue
Examples of Cancer stained with EGFR pharmDx™ 19n Colorectal Cancer
EGFR pharmDx™ Immunostaining in a Variety of solid Tumors 23
References 24n Additional EGFR Resources
n Acknowledgements
Table of Contents
Erbitux® is a registered trademark of ImClone Systems, Incorporated. VectibixTM is a registered trademark of Amgen, Incorporated.

� EGFR pharmDx™ Interpretation Manual
InTR
oD
uC
TIo
n
Welcome to the EGFR pharmDx™ Interpretation Manual
This guide for pathologists includes key technical
histological staining and interpretation tips when using
the EGFR pharmDxTM kit. utilization of the suggestions that
follow will ensure that your laboratory achieves the quality
results expected from EGFR pharmDxTM.
The EGFR pharmDxTM Interpretation Manual objectives
are simple:
n Provide an understanding of Epidermal Growth Factor
Receptor biology.
n Give procedure recommendations to ensure the
EGFR pharmDxTM assay is performed consistently
for optimal results.
n Present a standard approach to staining and
interpretation to ensure reproducible results.
n supply pathologists with guidelines for consistent
interpretation of EGFR pharmDx™ to aid in assessing
colorectal cancer patients for Erbitux® or VectibixTM
eligibility.
n To troubleshoot the EGFR pharmDxTM kit if problems
occur.
We hope this EGFR pharmDxTM Interpretation Manual is
useful, and we encourage you to provide feedback on
how we can improve this tool. Contact your local Dako
representative with feedback (see back panel for contact
information).
EGFR pharmDxTM is an FDA-approved assay indicated
as an aid in identifying patients eligible for treatment with
Erbitux® (cetuximab), or VectibixTM (panitumumab) for
EGFR-expressing metastatic colorectal cancer.
Introduction

�EGFR pharmDx™ Interpretation Manual
oVER
VIEWEGFR overview
EGFR and the HER Family
EGFR is a member of the EGF/erbb receptor family of
related growth factor receptors that includes HER2/erbb2
or neu, HER3/erbb3 and HER4/erbb4 (1).
Mouse monoclonal anti-EGFR clone 2-18C9 was selected
for its high specificity for EGFR. The specificity of clone
2-18C9 for EGFR (HER1) and lack of cross-reactivity with
the related HER family receptors were demonstrated by
immunocytochemistry and Western blotting using CHo
cells transiently transfected with vectors expressing
HER2, HER3 and HER4. Further specificity testing by flow
cytometry and Western blotting showed that clone 2-18C9
recognizes both the wild type and the EGFRvIII mutant
form of the receptor. The epitope bound by clone 2-18C9
was found to be a structural epitope in the extracellular
cysteine-rich region of the molecule spanning sub-domain
s2 and proximal to the transmembrane region (3).
Epidermal growth factor receptor (EGFR) is a 170 kDa
transmembrane receptor encoded by the human HER1
gene. The EGFR protein contains an extracellular ligand
binding domain, a transmembrane region and an
intracellular domain with intrinsic protein-tyrosine
kinase activity (see Figure 1). ligand binding of the
EGF receptor activates the EGFR tyrosine kinase
resulting in cell growth and differentiation (1).
EGFR Signaling Networks (2)
Figure 1
Ligand (EGF, TGF-a)
EGFRExtracellular domain
Cell membrane
Intracellular domain
Radiation or selected chemotherapy agents
Cell motility and metastasisCell adhesion, invasiveness
Growth effectsProliferation, differentiation
Angiogenesis effectsBlood vessel recruitment, invasion, metastasisGrowth arrest
or apoptosis
MEK
MAPK
Raf-1RasSOS
Tyrosinekinase
Grb2
Other enzymeor adapter
� EGFR pharmDx™ Interpretation Manual
oVE
RVI
EW
Tissue Type Positive Tissue Element Staining and Staining Pattern
Adrenal Cortical cells (2+): Cytoplasmic
Bone Marrow none
Breast lobular epithelial cells (2+): Membrane and cytoplasmic
Brain (Cerebellum) Molecular layer (1+): Extracellular
Brain/Cerebrum none
Cervix+ basalar squamous epithelial cells (2+): Membrane
Colon** none
Esophagus basalar squamous epithelial cells (2+): Membrane
Heart – none
Kidney Tubules (1+): Cytoplasmic staining (granular)
Liver Hepatocytes (sinusoids) (3+): Membrane bile ducts (3+): Membrane and cytoplasmic
Lung+ Alveolar lining cells/basalar bronchial cells (myoepithelial cells) (2+): Membrane and cytoplasmic
Mesothelial Cells Mesothelial cells (2+): Membrane and cytoplasmic
Ovary none
Pancreas Ducts (2+): Membrane
Parathyroid none
Peripheral Nerve nerve cell processes (1+): Fibrous
Pituitary none
Prostate+ Glandular epithelial cells (2+): Membrane
Salivary Gland Ductal elements (1+): Cytoplasmic
Skeletal Muscle – none
Skin+ basalar squamous cells, adnexal structures (2+): Membrane and cytoplasmic
Small Intestine none
Spleen none
Stomach none
Testis none
Thymus none
Thyroid none
Tonsil basalar squamous epithelium (3+): Membrane and cytoplasmic
Uterus Endometrial gland epithelium (2+): Membrane and cytoplasmic Endometrial stromal cells (2+): Membrane and cytoplasmic Myometrium: none
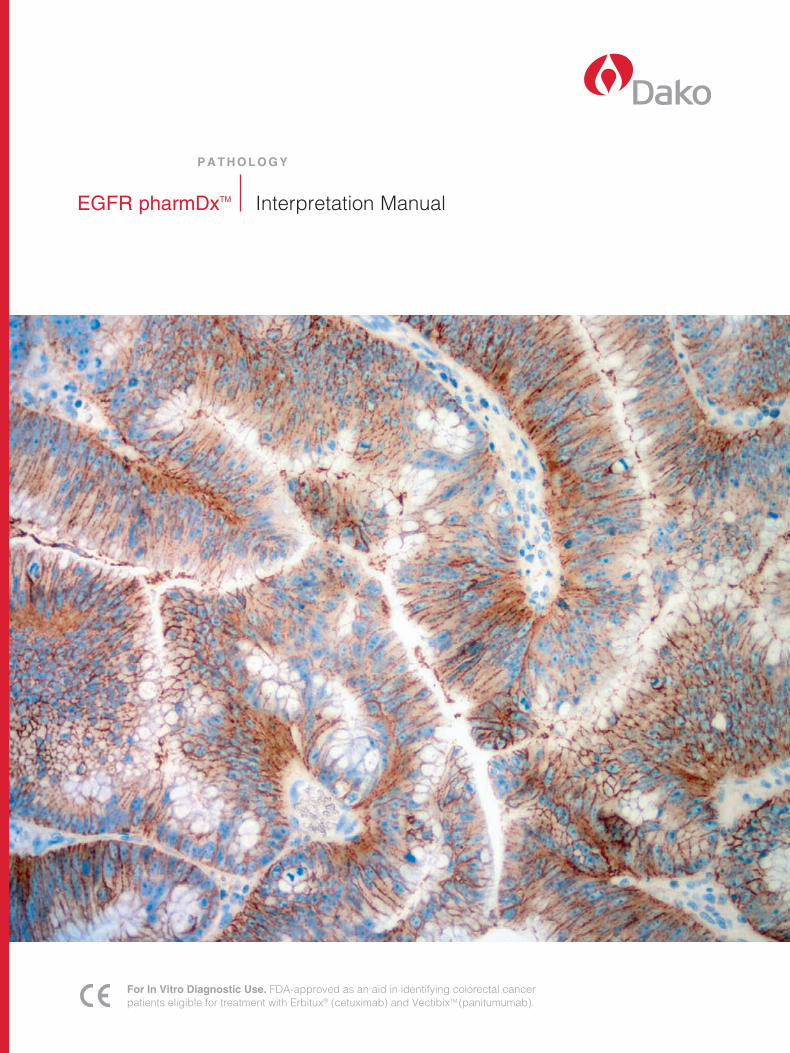
EGFR Expression in Normal Tissue
The EGFR protein is expressed on a variety of normal cells including many epithelial cell types (4-10).
non-epithelial cell types that express EGFR include smooth muscle cells, fibroblasts and perineurium (11).
some examples of normal tissue stained with EGFR pharmDxTM are summarized in the table below. All tissues were
formalin-fixed and paraffin-embedded.
Table �. Evaluation of normal tissue staining by Dako EGFR pharmDxTM*
+ Recommended for positive control tissue (See page 9 for photomicrograph of normal positive tissue staining of cervix) – Recommended for negative control tissue* The majority of tissues tested had positive staining of fibroblasts in stromal tissue (1+, fibrous), as well as perineural fibroblasts
and myoepithelial cells. Endogenous peroxidase-induced staining of granulocytes has been observed occasionally.** Colon tissue may exhibit positive staining of enterocytes, smooth muscle cells, endothelial cells and perineurium.
�EGFR pharmDx™ Interpretation Manual
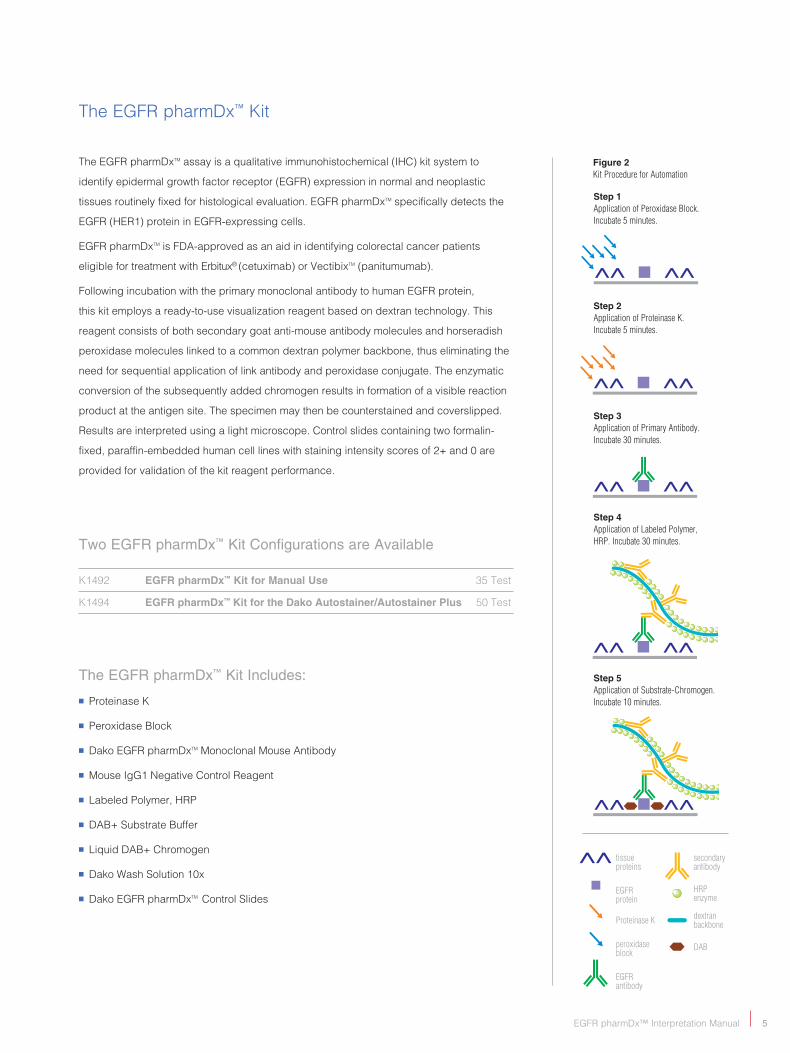
Step 4Application of Labeled Polymer, HRP. Incubate 30 minutes.
Step 5Application of Substrate-Chromogen. Incubate 10 minutes.
Step 1Application of Peroxidase Block. Incubate 5 minutes.
Figure 2Kit Procedure for Automation
Step 2Application of Proteinase K. Incubate 5 minutes.
Step 3Application of Primary Antibody. Incubate 30 minutes.
The EGFR pharmDx™ Kit
The EGFR pharmDxTM assay is a qualitative immunohistochemical (IHC) kit system to
identify epidermal growth factor receptor (EGFR) expression in normal and neoplastic
tissues routinely fixed for histological evaluation. EGFR pharmDxTM specifically detects the
EGFR (HER1) protein in EGFR-expressing cells.
EGFR pharmDxTM is FDA-approved as an aid in identifying colorectal cancer patients
eligible for treatment with Erbitux® (cetuximab) or VectibixTM (panitumumab).
Following incubation with the primary monoclonal antibody to human EGFR protein,
this kit employs a ready-to-use visualization reagent based on dextran technology. This
reagent consists of both secondary goat anti-mouse antibody molecules and horseradish
peroxidase molecules linked to a common dextran polymer backbone, thus eliminating the
need for sequential application of link antibody and peroxidase conjugate. The enzymatic
conversion of the subsequently added chromogen results in formation of a visible reaction
product at the antigen site. The specimen may then be counterstained and coverslipped.
Results are interpreted using a light microscope. Control slides containing two formalin-
fixed, paraffin-embedded human cell lines with staining intensity scores of 2+ and 0 are
provided for validation of the kit reagent performance.
Two EGFR pharmDx™ Kit Configurations are Available K1492 EGFR pharmDx™ Kit for Manual Use 35 Test
K1494 EGFR pharmDx™ Kit for the Dako Autostainer/Autostainer Plus 50 Test
The EGFR pharmDx™ Kit Includes:
n Proteinase K
n Peroxidase block
n Dako EGFR pharmDxTM Monoclonal Mouse Antibody
n Mouse IgG1 negative Control Reagent
n labeled Polymer, HRP
n DAb+ substrate buffer
n liquid DAb+ Chromogen
n Dako Wash solution 10x
n Dako EGFR pharmDxTM Control slides
tissueproteins
EGFRprotein
Proteinase K
peroxidaseblock
EGFRantibody
secondaryantibody
HRP enzyme
dextranbackbone
DAB
� EGFR pharmDx™ Interpretation Manual
THE
EGFR
pha
rmD
x™ K
IT
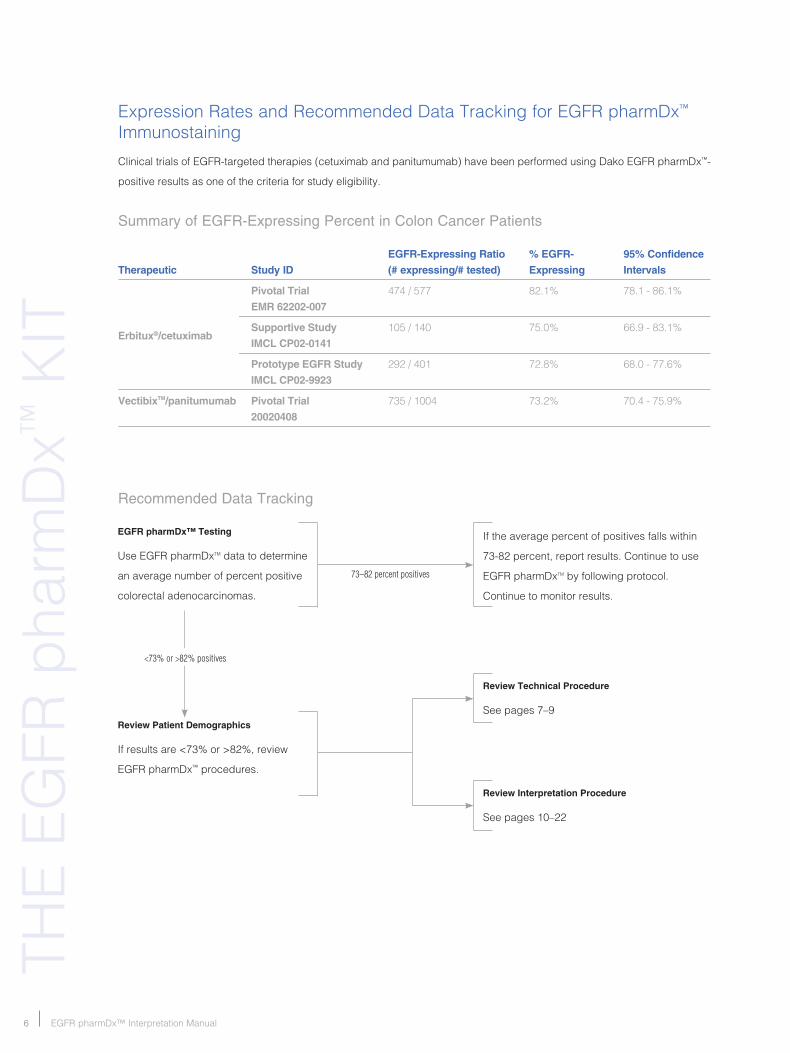
Clinical trials of EGFR-targeted therapies (cetuximab and panitumumab) have been performed using Dako EGFR pharmDx™-
positive results as one of the criteria for study eligibility.
Summary of EGFR-Expressing Percent in Colon Cancer Patients EGFR-Expressing Ratio % EGFR- 95% Confidence
Therapeutic Study ID (# expressing/# tested) Expressing Intervals
Pivotal Trial 474 / 577 82.1% 78.1 - 86.1% EMR 62202-007
Supportive Study 105 / 140 75.0% 66.9 - 83.1% IMCL CP02-0141
Prototype EGFR Study 292 / 401 72.8% 68.0 - 77.6% IMCL CP02-9923
VectibixTM/panitumumab Pivotal Trial 735 / 1004 73.2% 70.4 - 75.9% 20020408
Expression Rates and Recommended Data Tracking for EGFR pharmDx™ Immunostaining
Erbitux®/cetuximab
EGFR pharmDx™ Testing
use EGFR pharmDxTM data to determine
an average number of percent positive
colorectal adenocarcinomas.
If the average percent of positives falls within
73-82 percent, report results. Continue to use
EGFR pharmDxTM by following protocol.
Continue to monitor results.
73–82 percent positives
Review Patient Demographics
If results are <73% or >82%, review
EGFR pharmDx™ procedures.
<73% or >82% positives
Review Technical Procedure
see pages 7–9
Review Interpretation Procedure
see pages 10–22
Recommended Data Tracking
�EGFR pharmDx™ Interpretation Manual
TECH
nIC
Al TIPs
Technical Tips for optimal EGFR pharmDx™ Performance
Tissue Fixation and Variables
Procedural deviations that are related to sample handling
and processing can affect the EGFR pharmDxTM results.
some of the variables that may affect results are as follows:
n non-representative tissue samples
n specimens drying prior to fixation
n Fixation with PreFer fixative (suitable fixatives include 10% (v/v) neutral buffered formalin, 10% (v/v) unbuffered formalin, 25% (v/v) unbuffered formalin, AFA, Pen-Fix, and bouin’s)12
n Age, pH and storage conditions of fixative
n length of fixation
n length of storage of unstained tissue sections
For accurate and consistent results one must adhere to the EGFR pharmDxTM protocol.
High-quality results can be achieved in any laboratory by following these guidelines.
Technical problems may arise in two areas, those involving sample collection and preparation of tissue in the pre-analytical
processing of the specimen and those involving the actual performance of the EGFR pharmDxTM assay itself. Technical
issues relating to the performance of the assay are generally related to procedural deviations from the EGFR pharmDxTM
protocol and can be alleviated.
EGFR pharmDx™ Protocol Recommendations
n If staining must be interrupted, slides may be kept in wash buffer following incubation of the primary antibody for up to one hour at room temperature (20–25 °C).
n specimens preserved in generally used fixatives (10% v/v neutral buffered formalin, 10% v/v unbuffered formalin, 25% v/v unbuffered formalin, AFA, Pen-Fix, and
bouin’s) are suitable for testing with EGFR pharmDxTM. use of EGFR pharmDxTM on PreFer fixed tissues may result in unsatisfactory preservation of morphology.12
n Automated staining: Dako recommends the use of EGFR pharmDxTM on a Dako Autostainer or Autostainer Plus. use of EGFR pharmDxTM on alternative automated platforms has not been validated and may give erroneous results.
n Wash buffer: Dilute the provided wash buffer 1:10 using distilled or deionized water. store unused solution at 2–8 °C no more than seven days. Discard diluted solution if cloudy in appearance. only use wash buffer supplied in the EGFR pharmDxTM kit or TbsT Wash buffer, code s3006.
n storage of Reagents: Reagent and control slides should be stored at 2–8 °C. Do not use the kit after the expiration
date printed on the outside of the kit box.
n False-negative immunostaining can be caused by degradation of the antigen in the tissue over time. specimens should be stained within two months of mounting of tissues on slides when stored at room temperature (20–25 °C).
n Proper Incubations: All incubation times must be performed according to the package insert. stay within the tolerance indicated in the package insert for all incubation times.
n For high-quality results, review the EGFR pharmDxTM Training Checklist (Table 2) prior to beginning your staining run.
� EGFR pharmDx™ Interpretation Manual
TRA
InIn
G C
HEC
KlI
sT
2006
Dak
o P
LE
AS
E P
HO
TO
CO
PY
FO
R Y
OU
R U
SE
Table �. EGFR pharmDx™ Training Checklist
Customer name/Institution _______________________________________________________________________________________
Person Trained/Title _____________________________________________________________________________________________
Manual staining Run
Dako Autostainer software Version _________________________ Dako Autostainer serial number ____________________
Trainer________________________________________________________________ Date ___________________________________
EGFR pharmDxTM is a complete assay system requiring controls to ensure reproducible results.
Yes NoManual or Dako Autostainer Procedure
Control slides and kit stored at 2–8 °C?
Cell line control slides and all reagents warmed to room temperature (20-25 °C) prior to starting assay?
Tissues fixed in validated fixative?
specimens stained within two months of tissue mounting on slides when stored at room temperature?
Clearing solutions changed after 40 slides?
Deparaffinization and rehydration protocol followed?
Wash buffer prepared properly? Prepare sufficient quantity of Wash buffer by diluting Wash buffer 10X, 1:10 in Reagent Quality Water (deionized or distilled water).
Distilled or deionized water (not tap water) used for water washes after last alcohol bath in deparaffinization?
Regressive hematoxylin counterstains are not used?
Manual Procedure
Distilled or deionized water (not tap water) used for water bath after Proteinase K solution step and after substrate-Chromogen solution step?
Diluted Wash buffer used for all wash steps and baths (after Peroxidase-block, Primary Antibody/negative Control Reagent, labeled Polymer HRP)?
buffer bath(s) changed between each step?
Humid chamber used for Primary Antibody/ negative Control Reagent and labeled Polymer incubations?
slides placed in five-minute (±1) buffer baths between Peroxidase block and Proteinase K, negative Control Reagent steps/Primary Antibody, labeled Polymer and DAb+ substrate-Chromogen solution steps?
Proteinase K solution applied for five minutes?
Peroxidase block applied for five minutes and specimen fully covered?
Yes NoPrimary Antibody applied for 30 minutes and specimen fully covered?
labeled Polymer applied for 30 minutes and specimen fully covered?
DAb+ substrate-Chromogen prepared properly?
one drop DAb+ Chromogen to 1 ml DAb+ substrate buffer.
substrate-Chromogen solution applied for 10 minutes and specimen fully covered?
Dako Autostainer Procedure
slides placed in buffer five minutes (±1) before loading onto the Dako Autostainer?
Appropriate protocol template used?
Was the Dako Autostainer programming reviewed for accuracy?
slides rinsed with buffer between steps and double rinsed after the labeled polymer step with an additional five-minute rinse hold?
substrate-Chromogen prepared properly? Add 11 drops of liquid DAb+ Chromogen to one vial of DAb+ substrate buffer and mix.
substrate-Chromogen solution applied for two five-minute applications?
Instrumentation / Equipment
Is regular preventative maintenance performed on the Dako Autostainer?
Do you have all the necessary equipment to perform the EGFR pharmDxTM assay according to protocol?
If not, specify what is missing in comments below.
If you answered “no” to any of the above, you have deviated from protocol and should consult with your local Dako Technical support Representative for assistance.
Additional observations or comments:
________________________________________________________
________________________________________________________
�EGFR pharmDx™ Interpretation Manual
Quality Control
Qu
AlITy C
on
TRo
l
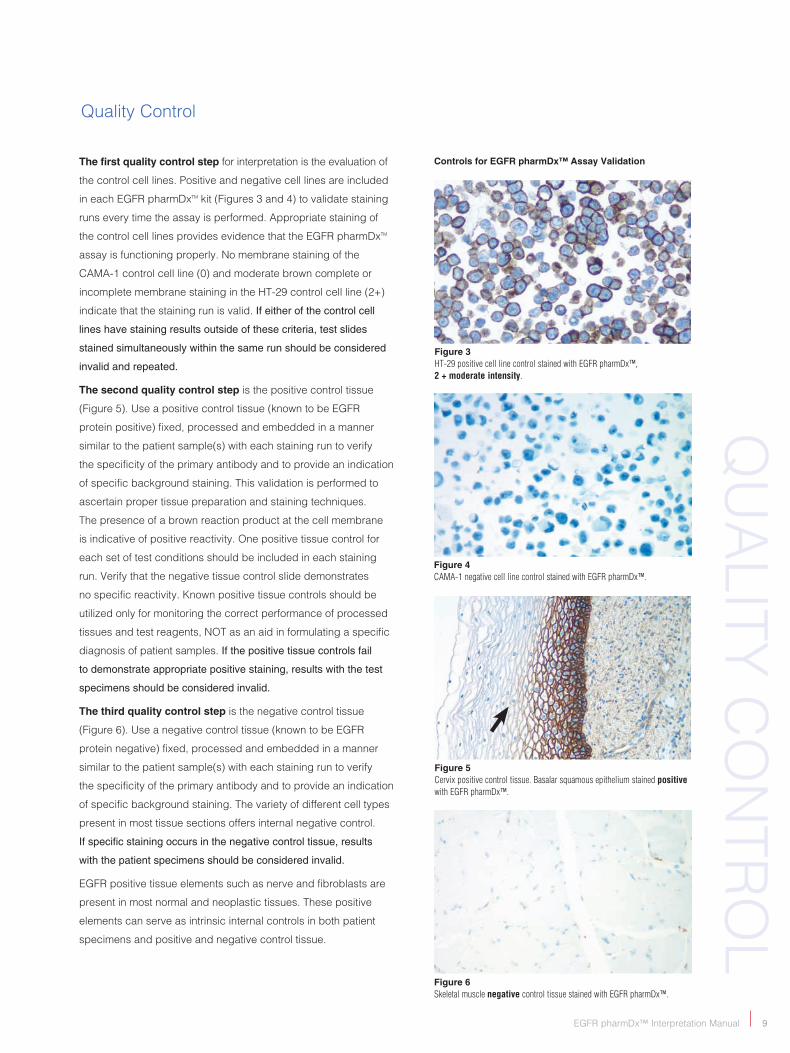
Controls for EGFR pharmDx™ Assay Validation
Figure 3 HT-29 positive cell line control stained with EGFR pharmDx™, 2 + moderate intensity.
Figure 4 CAMA-1 negative cell line control stained with EGFR pharmDx™.
Figure 5 Cervix positive control tissue. Basalar squamous epithelium stained positive with EGFR pharmDx™.
Figure 6 Skeletal muscle negative control tissue stained with EGFR pharmDx™.
The first quality control step for interpretation is the evaluation of
the control cell lines. Positive and negative cell lines are included
in each EGFR pharmDxTM kit (Figures 3 and 4) to validate staining
runs every time the assay is performed. Appropriate staining of
the control cell lines provides evidence that the EGFR pharmDxTM
assay is functioning properly. no membrane staining of the
CAMA-1 control cell line (0) and moderate brown complete or
incomplete membrane staining in the HT-29 control cell line (2+)
indicate that the staining run is valid. If either of the control cell
lines have staining results outside of these criteria, test slides
stained simultaneously within the same run should be considered
invalid and repeated.
The second quality control step is the positive control tissue
(Figure 5). use a positive control tissue (known to be EGFR
protein positive) fixed, processed and embedded in a manner
similar to the patient sample(s) with each staining run to verify
the specificity of the primary antibody and to provide an indication
of specific background staining. This validation is performed to
ascertain proper tissue preparation and staining techniques.
The presence of a brown reaction product at the cell membrane
is indicative of positive reactivity. one positive tissue control for
each set of test conditions should be included in each staining
run. Verify that the negative tissue control slide demonstrates
no specific reactivity. Known positive tissue controls should be
utilized only for monitoring the correct performance of processed
tissues and test reagents, noT as an aid in formulating a specific
diagnosis of patient samples. If the positive tissue controls fail
to demonstrate appropriate positive staining, results with the test
specimens should be considered invalid.
The third quality control step is the negative control tissue
(Figure 6). use a negative control tissue (known to be EGFR
protein negative) fixed, processed and embedded in a manner
similar to the patient sample(s) with each staining run to verify
the specificity of the primary antibody and to provide an indication
of specific background staining. The variety of different cell types
present in most tissue sections offers internal negative control.
If specific staining occurs in the negative control tissue, results
with the patient specimens should be considered invalid.
EGFR positive tissue elements such as nerve and fibroblasts are
present in most normal and neoplastic tissues. These positive
elements can serve as intrinsic internal controls in both patient
specimens and positive and negative control tissue.
�0 EGFR pharmDx™ Interpretation Manual
EVA
luA
TIo
n A
nD
REP
oR
TIn
G
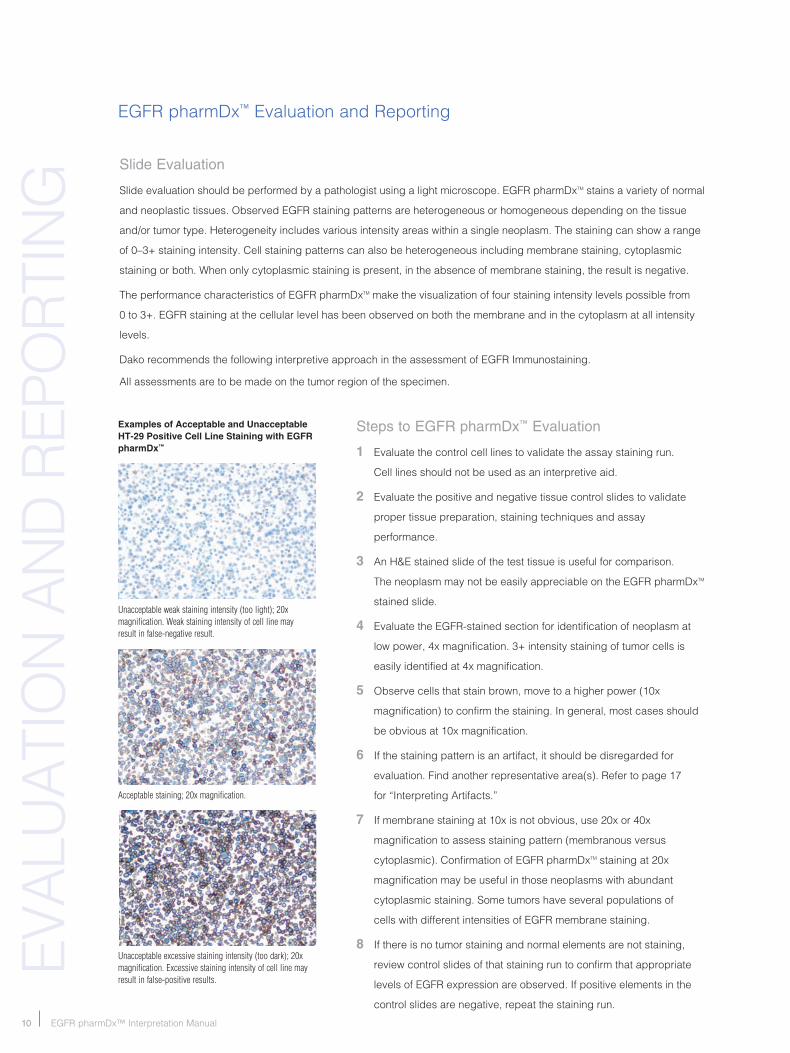
Unacceptable excessive staining intensity (too dark); 20x magnification. Excessive staining intensity of cell line may result in false-positive results.
EGFR pharmDx™ Evaluation and Reporting
Acceptable staining; 20x magnification.
Slide Evaluation
slide evaluation should be performed by a pathologist using a light microscope. EGFR pharmDxTM stains a variety of normal
and neoplastic tissues. observed EGFR staining patterns are heterogeneous or homogeneous depending on the tissue
and/or tumor type. Heterogeneity includes various intensity areas within a single neoplasm. The staining can show a range
of 0–3+ staining intensity. Cell staining patterns can also be heterogeneous including membrane staining, cytoplasmic
staining or both. When only cytoplasmic staining is present, in the absence of membrane staining, the result is negative.
The performance characteristics of EGFR pharmDxTM make the visualization of four staining intensity levels possible from
0 to 3+. EGFR staining at the cellular level has been observed on both the membrane and in the cytoplasm at all intensity
levels.
Dako recommends the following interpretive approach in the assessment of EGFR Immunostaining.
All assessments are to be made on the tumor region of the specimen.
Steps to EGFR pharmDx™ Evaluation
1 Evaluate the control cell lines to validate the assay staining run.
Cell lines should not be used as an interpretive aid.
2 Evaluate the positive and negative tissue control slides to validate
proper tissue preparation, staining techniques and assay
performance.
3 An H&E stained slide of the test tissue is useful for comparison.
The neoplasm may not be easily appreciable on the EGFR pharmDxTM
stained slide.
4 Evaluate the EGFR-stained section for identification of neoplasm at
low power, 4x magnification. 3+ intensity staining of tumor cells is
easily identified at 4x magnification.
5 observe cells that stain brown, move to a higher power (10x
magnification) to confirm the staining. In general, most cases should
be obvious at 10x magnification.
6 If the staining pattern is an artifact, it should be disregarded for
evaluation. Find another representative area(s). Refer to page 17
for “Interpreting Artifacts.”
7 If membrane staining at 10x is not obvious, use 20x or 40x
magnification to assess staining pattern (membranous versus
cytoplasmic). Confirmation of EGFR pharmDxTM staining at 20x
magnification may be useful in those neoplasms with abundant
cytoplasmic staining. some tumors have several populations of
cells with different intensities of EGFR membrane staining.
8 If there is no tumor staining and normal elements are not staining,
review control slides of that staining run to confirm that appropriate
levels of EGFR expression are observed. If positive elements in the
control slides are negative, repeat the staining run.
Examples of Acceptable and Unacceptable HT-29 Positive Cell Line Staining with EGFR pharmDx™
Unacceptable weak staining intensity (too light); 20x magnification. Weak staining intensity of cell line may result in false-negative result.

��EGFR pharmDx™ Interpretation Manual
PA
THo
loG
y R
EP
oR
T FoR
M
Table �. EGFR pharmDx™ Pathology Report Form
Patient name_______________________________________ Collection Date _____________________________________
ordering Physician _________________________________ Received Date _____________________________________
ordering Facility ____________________________________ Report Date ________________________________________
Medical Record # ___________________________________ lab Reference # ____________________________________
speciman ID # _____________________________________ Tumor source ______________________________________
Date of birth _______________________________________ Patient Gender _____________________________________
Description
Patient Result
EGFR protein Positive Negative
EGFR pharmDxTM is indicated as an aid in identifying
colorectal cancer patients eligible for treatment with
Erbitux® (cetuximab) or VectibixTM (panitumumab).
EGFR pharmDx™ staining Results
These definitions of positive and negative results are in accord with published literature12, but may require modification in specific contexts.
Clinical Trials
several clinical trials of EFGR-targeted therapies
(cetuximab and panitumumab) have been performed.
Patients whose tumors had EFGR expression as
demonstrated using the Dako EFGR pharmDxTM assay
were eligible for study enrollment. The response rate
for EGFR-negative patients and patients with EGFR-
positive staining in less than one percent of tumor cells is
unknown as no such patients were present in the clinical
drug trials. Tumors with EGFR-positive staining in ≥1% of
their cells are considered EGFR expressing with regard
to the current EFGR-targeted therapy indications for use.
Deparaffinized tissue and appropriate control tissue
sections are stained using the FDA-approved Dako
EGFR pharmDxTM immunohistochemistry kit.
Tumors should be reported as EGFR positive or EGFR
negative using membrane staining as the evaluable
structure. A tumor cell is EGFR positive if it exhibits
any membrane staining above background, whether
or not it is completely circumferential. A tumor with no
membrane staining above background in any tumor
cell is reported as an EGFR-negative tumor.
2006
Dak
o P
LE
AS
E P
HO
TO
CO
PY
FO
R Y
OU
R U
SE
Report to Treating Physician Definition
EGFR-Negative Tumor Absence of membrane staining above background in all tumor cells.
EGFR-Positive Tumor EGFR-positive staining is defined as any IHC staining of tumor cell membranes above
background level; whether it is complete or incomplete circumferential staining.
Staining Intensity Percent of Tumor Cells Staining
1+, 2+, or 3+ >0%
�� EGFR pharmDx™ Interpretation Manual
InTE
RPR
ETA
TIo
n G
uID
En
EGA
TIVE
REs
ulT
sPo
sITI
VE R
Esu
lTs
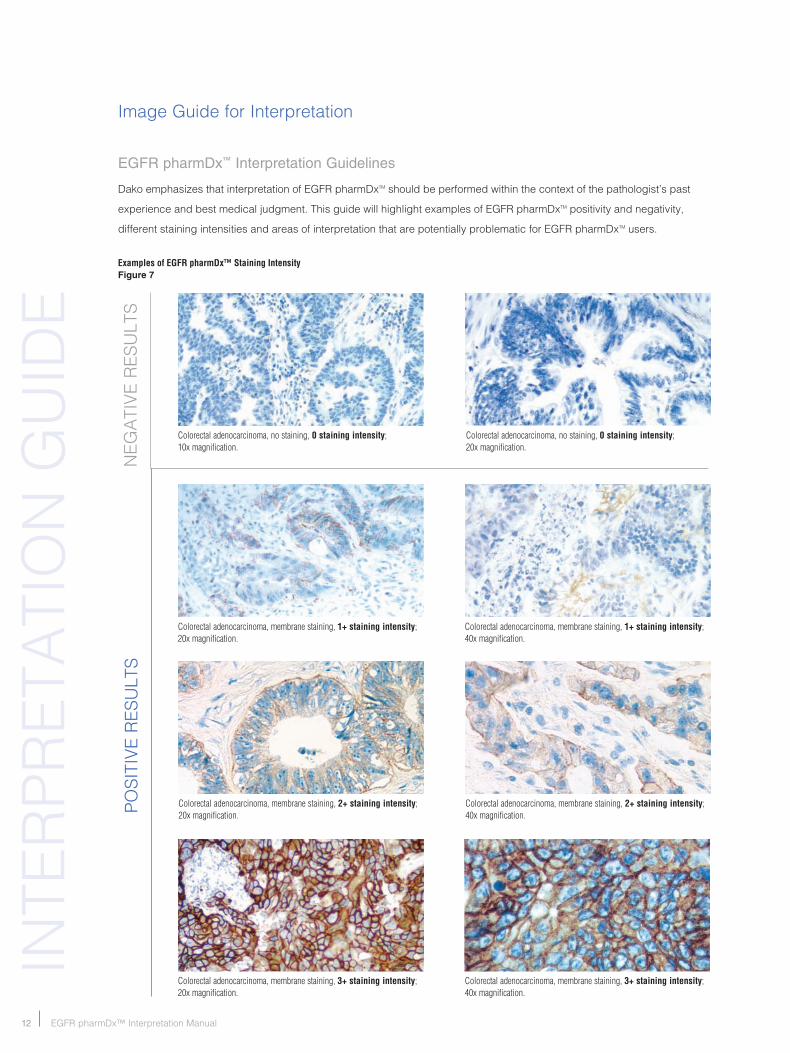
Image Guide for Interpretation
Colorectal adenocarcinoma, no staining, 0 staining intensity; 10x magnification.
Colorectal adenocarcinoma, no staining, 0 staining intensity; 20x magnification.
Colorectal adenocarcinoma, membrane staining, 1+ staining intensity; 20x magnification.
Colorectal adenocarcinoma, membrane staining, 1+ staining intensity; 40x magnification.
Colorectal adenocarcinoma, membrane staining, 2+ staining intensity; 20x magnification.
Colorectal adenocarcinoma, membrane staining, 2+ staining intensity; 40x magnification.
Colorectal adenocarcinoma, membrane staining, 3+ staining intensity; 20x magnification.
Colorectal adenocarcinoma, membrane staining, 3+ staining intensity; 40x magnification.
EGFR pharmDx™ Interpretation Guidelines
Dako emphasizes that interpretation of EGFR pharmDxTM should be performed within the context of the pathologist’s past
experience and best medical judgment. This guide will highlight examples of EGFR pharmDxTM positivity and negativity,
different staining intensities and areas of interpretation that are potentially problematic for EGFR pharmDxTM users.
Examples of EGFR pharmDx™ Staining Intensity Figure 7
��EGFR pharmDx™ Interpretation Manual
sTAIn
InG
PATTER
ns
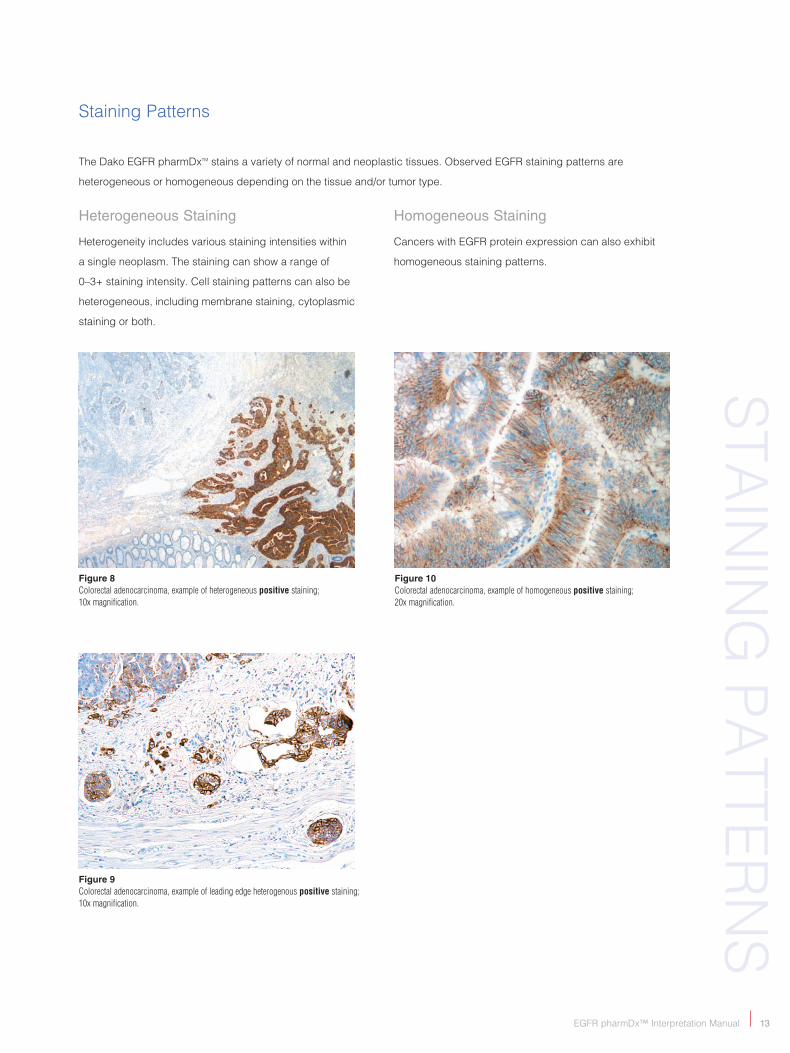
staining Patterns
Figure 8 Colorectal adenocarcinoma, example of heterogeneous positive staining; 10x magnification.
Figure 9Colorectal adenocarcinoma, example of leading edge heterogenous positive staining; 10x magnification.
Figure 10 Colorectal adenocarcinoma, example of homogeneous positive staining; 20x magnification.
The Dako EGFR pharmDxTM stains a variety of normal and neoplastic tissues. observed EGFR staining patterns are
heterogeneous or homogeneous depending on the tissue and/or tumor type.
Heterogeneous Staining
Heterogeneity includes various staining intensities within
a single neoplasm. The staining can show a range of
0–3+ staining intensity. Cell staining patterns can also be
heterogeneous, including membrane staining, cytoplasmic
staining or both.
Homogeneous Staining
Cancers with EGFR protein expression can also exhibit
homogeneous staining patterns.
�� EGFR pharmDx™ Interpretation Manual
EGFR
sTA
InIn
G
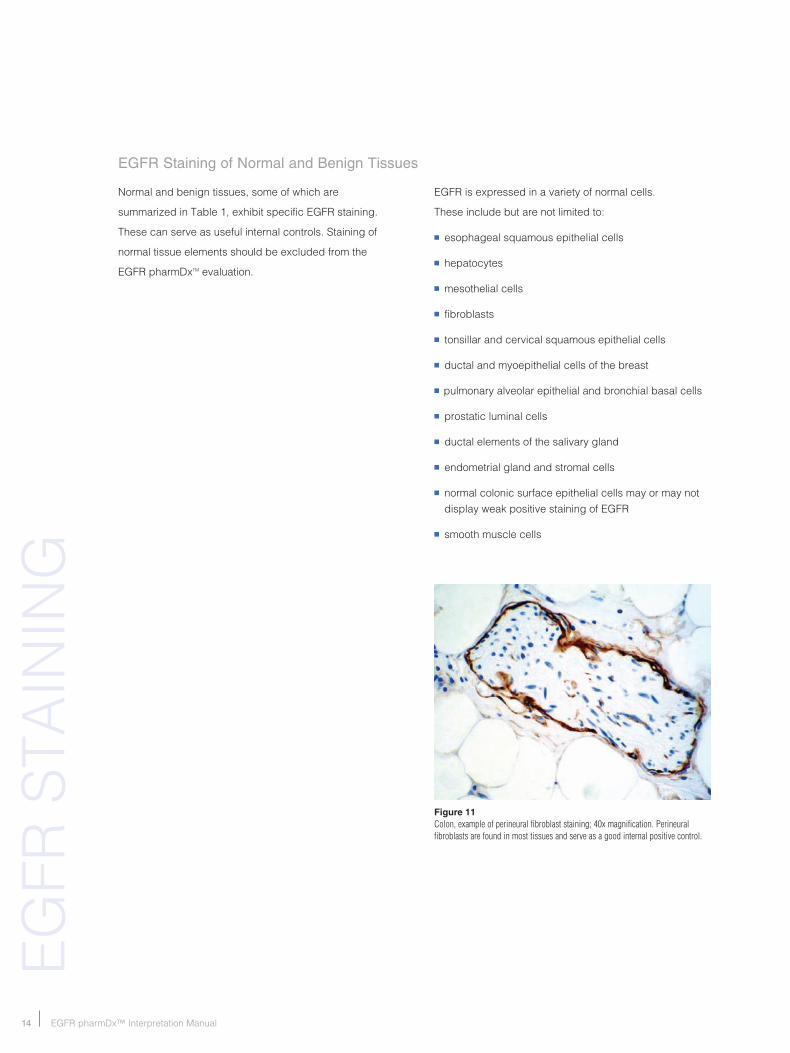
Figure 11 Colon, example of perineural fibroblast staining; 40x magnification. Perineural fibroblasts are found in most tissues and serve as a good internal positive control.
normal and benign tissues, some of which are
summarized in Table 1, exhibit specific EGFR staining.
These can serve as useful internal controls. staining of
normal tissue elements should be excluded from the
EGFR pharmDxTM evaluation.
EGFR Staining of Normal and Benign Tissues
EGFR is expressed in a variety of normal cells.
These include but are not limited to:
n esophageal squamous epithelial cells
n hepatocytes
n mesothelial cells
n fibroblasts
n tonsillar and cervical squamous epithelial cells
n ductal and myoepithelial cells of the breast
n pulmonary alveolar epithelial and bronchial basal cells
n prostatic luminal cells
n ductal elements of the salivary gland
n endometrial gland and stromal cells
n normal colonic surface epithelial cells may or may not display weak positive staining of EGFR
n smooth muscle cells

��EGFR pharmDx™ Interpretation Manual
EGFR
sTAIn
InG
Figure 12 Colorectal adenocarcinoma infiltrating the liver. Example of positively stained normal hepatocytes and negative tumor cells; 10x magnification. The sample is negative.
Figure 15 Needle biopsy from liver exhibiting strong tumor staining; 10x magnification. The sample is positive.
Figure 13 Colorectal adenocarcinoma infiltrating the liver. Example of positively stained normal hepatocytes and negative tumor cells; 20x magnification. The sample is negative.
Needle Biopsy from LiverHepatocyte Staining in the Liver
Figure 14 Colorectal adenocarcinoma infiltrating the liver. Example of positively stained normal hepatocytes and negative tumor cells; 40x magnification. The sample is negative.
�� EGFR pharmDx™ Interpretation Manual
FAC
ToR
s To
Co
nsI
DER
Factors to Consider in Evaluation of EGFR pharmDx™ stains
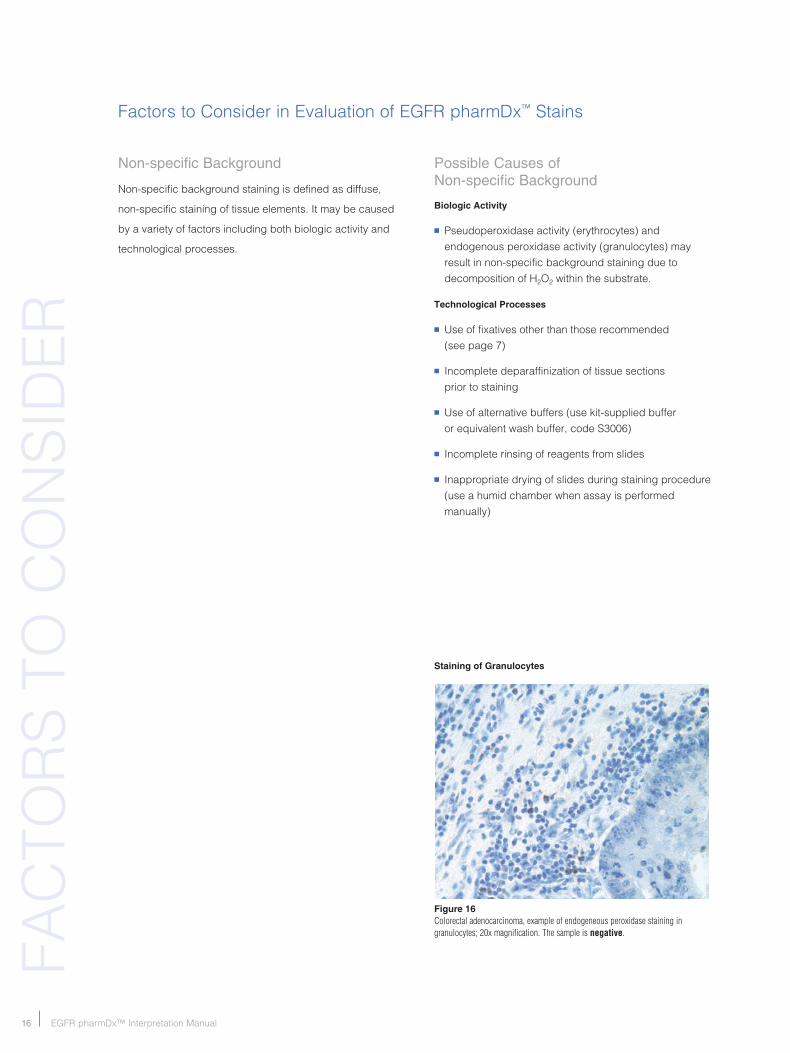
Figure 16 Colorectal adenocarcinoma, example of endogeneous peroxidase staining in granulocytes; 20x magnification. The sample is negative.
Non-specific Background
non-specific background staining is defined as diffuse,
non-specific staining of tissue elements. It may be caused
by a variety of factors including both biologic activity and
technological processes.
Possible Causes of Non-specific Background
Biologic Activity
n Pseudoperoxidase activity (erythrocytes) and endogenous peroxidase activity (granulocytes) may result in non-specific background staining due to decomposition of H2o2 within the substrate.
Technological Processes
n use of fixatives other than those recommended (see page 7)
n Incomplete deparaffinization of tissue sections prior to staining
n use of alternative buffers (use kit-supplied buffer or equivalent wash buffer, code s3006)
n Incomplete rinsing of reagents from slides
n Inappropriate drying of slides during staining procedure (use a humid chamber when assay is performed manually)
Staining of Granulocytes
��EGFR pharmDx™ Interpretation Manual
AR
TIFAC
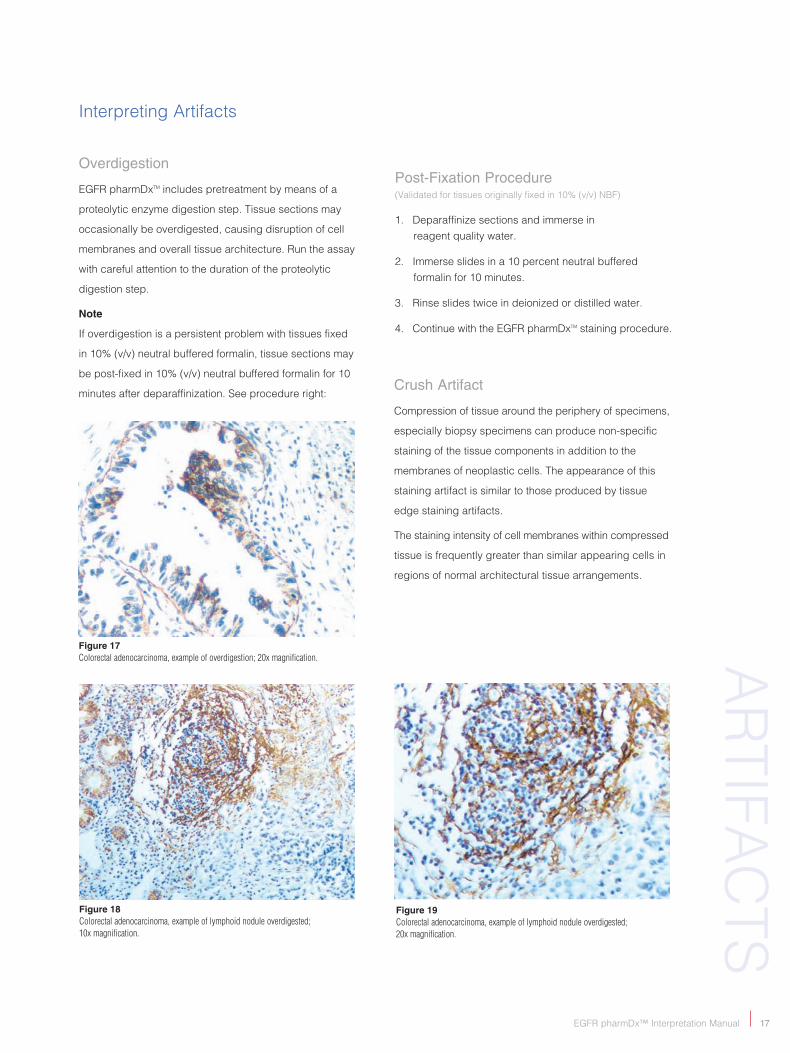
TsFigure 18 Colorectal adenocarcinoma, example of lymphoid nodule overdigested; 10x magnification.
Figure 19 Colorectal adenocarcinoma, example of lymphoid nodule overdigested; 20x magnification.
Figure 17 Colorectal adenocarcinoma, example of overdigestion; 20x magnification.
Interpreting Artifacts
Overdigestion
EGFR pharmDxTM includes pretreatment by means of a
proteolytic enzyme digestion step. Tissue sections may
occasionally be overdigested, causing disruption of cell
membranes and overall tissue architecture. Run the assay
with careful attention to the duration of the proteolytic
digestion step.
Note
If overdigestion is a persistent problem with tissues fixed
in 10% (v/v) neutral buffered formalin, tissue sections may
be post-fixed in 10% (v/v) neutral buffered formalin for 10
minutes after deparaffinization. see procedure right:
Post-Fixation Procedure(Validated for tissues originally fixed in 10% (v/v) nbF)
1. Deparaffinize sections and immerse in reagent quality water.
2. Immerse slides in a 10 percent neutral buffered formalin for 10 minutes.
3. Rinse slides twice in deionized or distilled water.
4. Continue with the EGFR pharmDxTM staining procedure.
Crush Artifact
Compression of tissue around the periphery of specimens,
especially biopsy specimens can produce non-specific
staining of the tissue components in addition to the
membranes of neoplastic cells. The appearance of this
staining artifact is similar to those produced by tissue
edge staining artifacts.
The staining intensity of cell membranes within compressed
tissue is frequently greater than similar appearing cells in
regions of normal architectural tissue arrangements.

�� EGFR pharmDx™ Interpretation Manual
Figure 20 Colorectal adenocarcinoma, example of edge artifact; 10x magnification.
Edge Artifact
Frequently, increased staining is observed around
the periphery of the tissue specimen, known as the
“edge effect.” Edge artifacts are commonly the result
of inappropriate pre-analytic handling of the tissue. The
edge effect represents fixation artifact or tissue drying
prior to fixation. usually the staining artifact is limited to a
thin rim of stained cells with an abrupt termination to the
staining reaction. often the method of surgical extraction
is the cause (see Crushing Artifact section).
Tissue section edge staining artifacts are common if there
are significant tissue section irregularities. Thick tissue
sections may mimic edge artifacts and can be corrected
by recutting the tissue block to produce a uniform, thin,
3-5 µm thick section that is devoid of folds and wrinkles.
When the peripheral positive reaction is only at the edge
of the tissue section, evaluation of EGFR staining should
exclude tumor cells within the region’s edge artifact.
Retraction Artifact
stromal retraction around tumor cell glands can create
clefts where pooled antibody can non-specifically stain.
Thorough washing after the primary antibody incubation
step may prevent this reaction. Retraction space staining
manifests itself as a hemicircumferential reaction around
the periphery of the gland.
Thermal Artifact
Thermal electrocautery may alter nuclei and cell
membranes. Dako recommends that the evaluation
of EGFR pharmDxTM staining be performed on tissue with
no or minimal thermal electrocautery artifacts.
Non-Evaluable Areas of Tissue
Areas of stained slides that should not be evaluated include
dissociated, free-floating groups or aggregates of neoplastic
cells, necrotic cells, and damaged areas of the tissue
section (torn sections, folded or wrinkled areas, etc.).
AR
TIFA
CTs
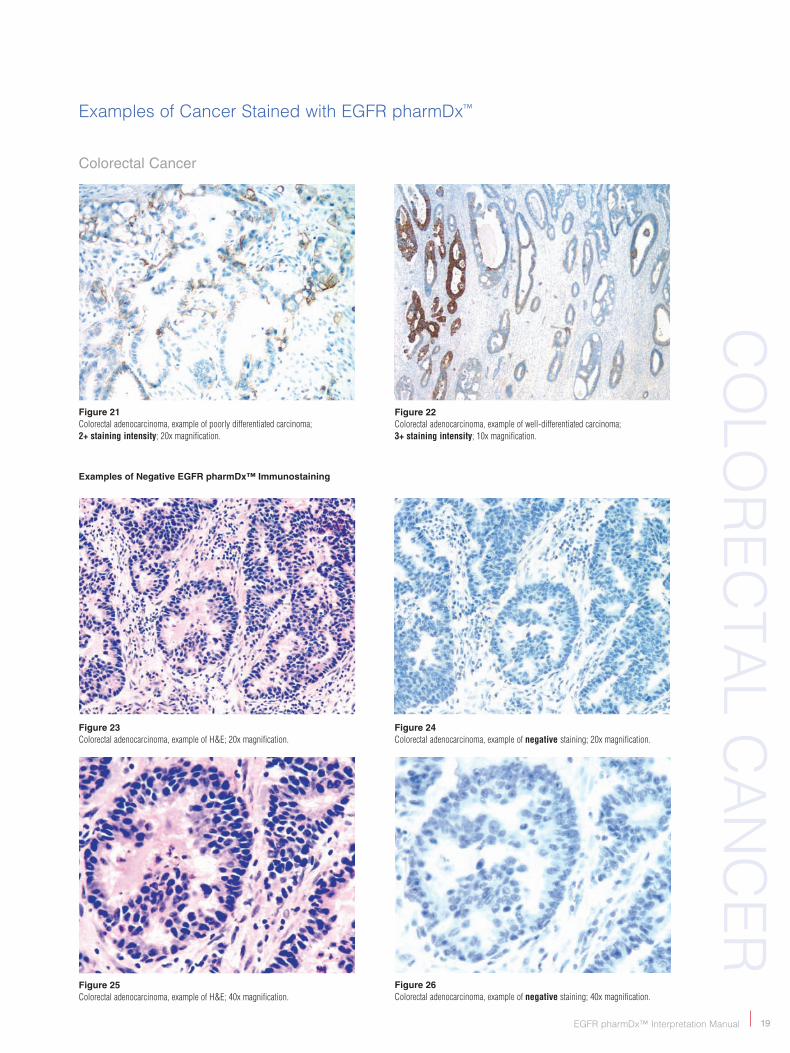
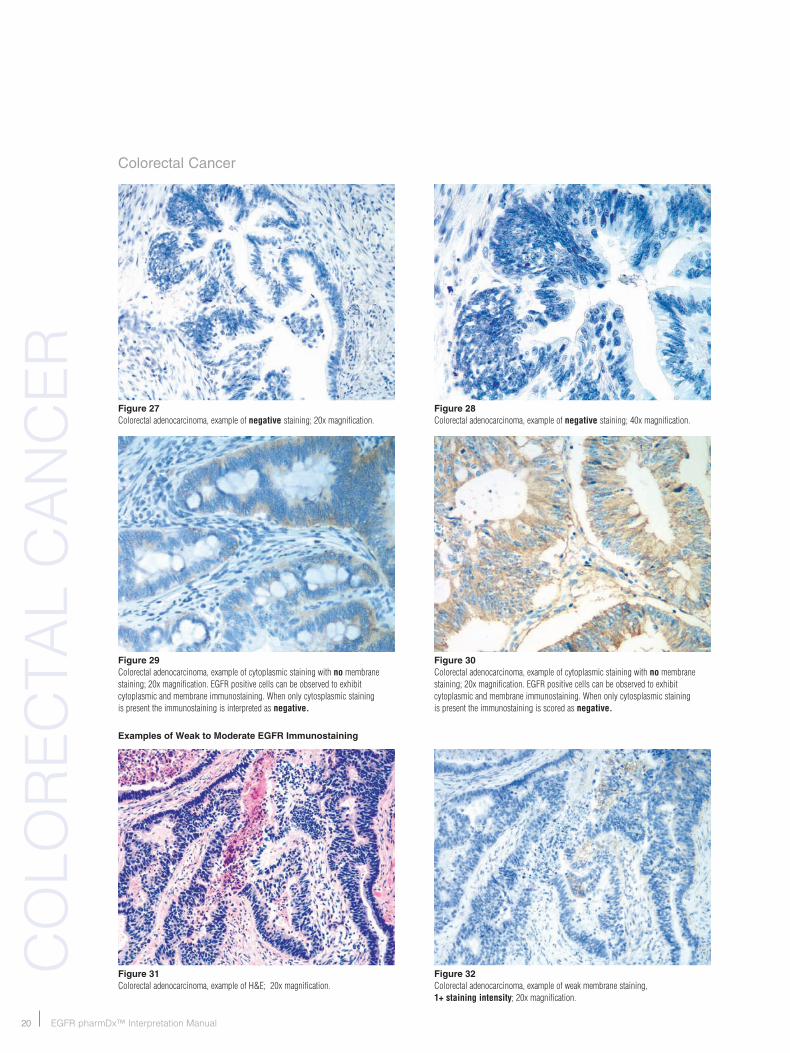
Examples of Cancer stained with EGFR pharmDx™
Colorectal Cancer
Figure 25 Colorectal adenocarcinoma, example of H&E; 40x magnification.
Figure 23 Colorectal adenocarcinoma, example of H&E; 20x magnification.
Figure 24 Colorectal adenocarcinoma, example of negative staining; 20x magnification.
Figure 21 Colorectal adenocarcinoma, example of poorly differentiated carcinoma; 2+ staining intensity; 20x magnification.
Figure 22 Colorectal adenocarcinoma, example of well-differentiated carcinoma; 3+ staining intensity; 10x magnification.
Examples of Negative EGFR pharmDx™ Immunostaining
EGFR pharmDx™ Interpretation Manual ��
Co
loR
ECTA
l CA
nC
ER
Figure 26Colorectal adenocarcinoma, example of negative staining; 40x magnification.
�0 EGFR pharmDx™ Interpretation Manual
Colorectal Cancer
Figure 32 Colorectal adenocarcinoma, example of weak membrane staining, 1+ staining intensity; 20x magnification.
Figure 31 Colorectal adenocarcinoma, example of H&E; 20x magnification.
Figure 29 Colorectal adenocarcinoma, example of cytoplasmic staining with no membrane staining; 20x magnification. EGFR positive cells can be observed to exhibit cytoplasmic and membrane immunostaining. When only cytosplasmic staining is present the immunostaining is interpreted as negative.
Figure 30 Colorectal adenocarcinoma, example of cytoplasmic staining with no membrane staining; 20x magnification. EGFR positive cells can be observed to exhibit cytoplasmic and membrane immunostaining. When only cytosplasmic staining is present the immunostaining is scored as negative.
Examples of Weak to Moderate EGFR Immunostaining
Figure 27 Colorectal adenocarcinoma, example of negative staining; 20x magnification.
Figure 28 Colorectal adenocarcinoma, example of negative staining; 40x magnification.
Co
loR
ECTA
l C
An
CER
��EGFR pharmDx™ Interpretation Manual
Co
loR
ECTA
l CA
nC
ER
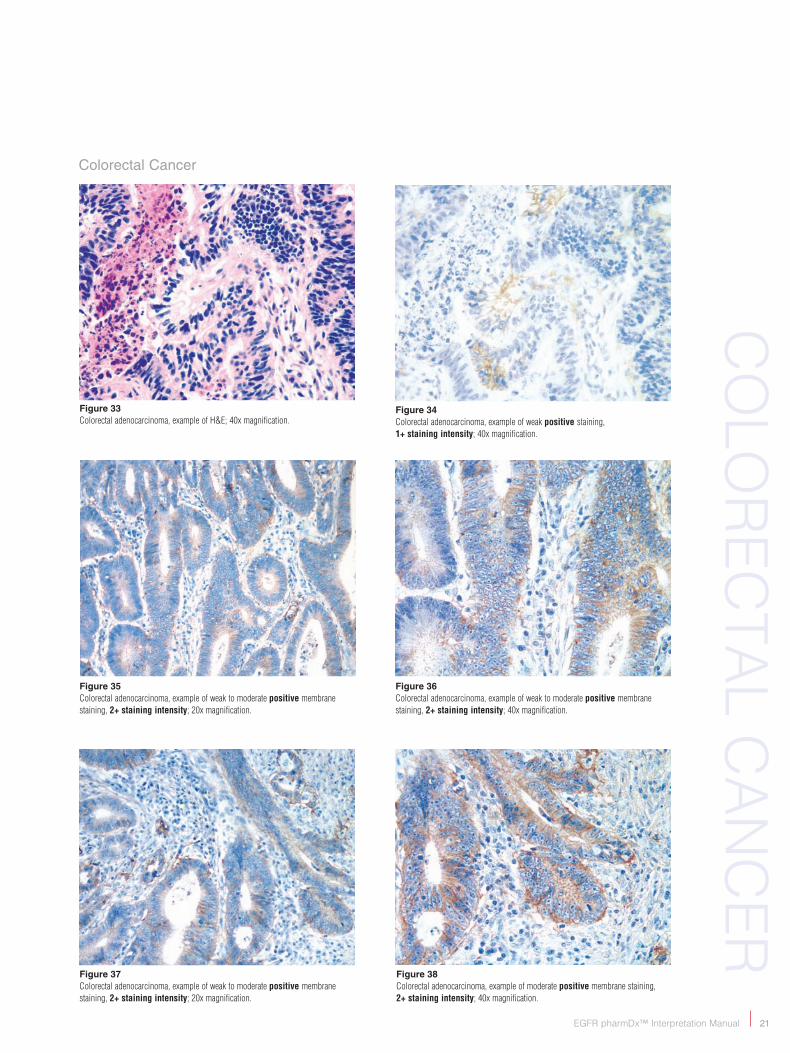
Figure 36 Colorectal adenocarcinoma, example of weak to moderate positive membrane staining, 2+ staining intensity; 40x magnification.
Figure 35 Colorectal adenocarcinoma, example of weak to moderate positive membrane staining, 2+ staining intensity; 20x magnification.
Figure 37 Colorectal adenocarcinoma, example of weak to moderate positive membrane staining, 2+ staining intensity; 20x magnification.
Figure 38 Colorectal adenocarcinoma, example of moderate positive membrane staining, 2+ staining intensity; 40x magnification.
Figure 33 Colorectal adenocarcinoma, example of H&E; 40x magnification.
Figure 34 Colorectal adenocarcinoma, example of weak positive staining, 1+ staining intensity; 40x magnification.
Colorectal Cancer

�� EGFR pharmDx™ Interpretation Manual
Co
loR
ECTA
l C
An
CER
Figure 40 Colorectal adenocarcinoma, example of strong positive membrane staining, 3+ staining intensity; 20x magnification.
Figure 41 Colorectal adenocarcinoma, example of strong positive membrane staining, 3+ staining intensity; 40x magnification.
Figure 44 Colorectal adenocarcinoma, example of strong positive membrane staining, 3+ staining intensity; 40x magnification.
Figure 42 Colorectal adenocarcinoma, example of strong positive membrane staining, 3+ staining intensity; 10x magnification.
Figure 43 Colorectal adenocarcinoma, example of strong positive membrane staining, 3+ staining intensity; 20x magnification.
Colorectal Cancer
Examples of Moderate to Strong EGFR Immunostaining
Figure 39 Colorectal adenocarcinoma, example of strong positive membrane staining, 3+ staining intensity; 10x magnification.
��EGFR pharmDx™ Interpretation Manual
IMM
un
osTA
InIn
G
EGFR pharmDx™ Immunostaining in a Variety of solid Tumors
EGFR is expressed in a number of solid tumors.
The EGFR pharmDxTM assay is a qualitative
immunohistochemical (IHC) kit system useful in
identifying epidermal growth factor receptor expression
in normal and neoplastic tissues routinely fixed for
histological evaluation.
Results from tissue specimens stained using EGFR
pharmDxTM for purposes other than Erbitux® or VectibixTM
assessment have no known clinical utility.

�� EGFR pharmDx™ Interpretation Manual
REF
EREn
CEs
References
1. sliwkowski MX, lofgren JA, lewis GD, et al. nonclinical studies addressing the mechanism of action of Trastuzumab (Herceptin). 1999; seminoncol 26:60-70, (suppl 12).
2. Harari PM, Huang s-M. Modulation of Molecular Targets to Enhance Radiation. 2000; Clin Cancer Res 6:323.
3. Pii K, Andersen FG, Jensen s, spaulding b. Characterization of a new monoclonal antibody, clone 2-18C9, for the measurement of Epidermal Growth Factor Receptor expression in solid tumors. Am Assoc Canc Res 95th annual meeting, orlando, Fl Mar 27–31 2004; Abst #5029.
4. Coussens l, yang-Feng Tl, liao y-C, Chen E, Gray A, McGrath, J seeburg PH, libermann TA, schlessinger J, Francke u, levinson A, ullrich A. Tyrosine kinase receptor with extensive homology to EGF receptor shares chromosomal location with neu oncogene. science 1985; 230: 1132.
5. yamamoto T, Ikawa s, Akiyama T, semba K, nomura n, Miyajima n, saito T, Toyoshima K. similarity of protein encoded by the human c-erb-b-2 gene to epidermal growth factor receptor. nature 1986; 319:230.
6. schechter Al, Hung M-C, Vaidyanathan l, Weinberg RA, yang-Feng Tl, Francke u, ullrich A, Coussens l, The neu gene: An erbb-homologous gene distinct from and unlinked to the gene encoding the EGF receptor. science 1985; 229:976.
7. Gusterson b, Cowley G, smith JA, ozanne b. Cellular localisation of human epidermal growth factor receptor. Cell biol Intl Rpts 1984; 8(8):649.
8. Gullick WJ. Prevalence of aberrant expression of the epidermal growth factor receptor in human cancers. br Eed bull 1991; 47(1):87.
9. sainsbury JRC, Farndon JR, sherbet GV, Harris Al. Epidermal-growth-factor receptors and oestrogen receptors in human breast cancer. lancet 1985; 1(8425):364.
10. ozanne b, Richards Cs, Hendler F, burns D, Gusterson b. over-expression of the EGF receptor is a hallmark of squamous cell carcinomas. J Pathol 1986; 149:9.
11. Werner MH, nanney lb, stoscheck CM, King lE. localization of immunoreactive epidermal growth factor receptors in human nervous system. J Histochem Cytochem 1988; 36:81.
12. Atkins D, Reiffen KA, Tegtmeier Cl, Winther H, bonato Ms and störkel s. Immunohistochemical detection of EGFR in paraffin-embedded tumor tissues: Variation in staining intensity due to choice of fixative and storage time of tissue sections. J Histochem Cytochem 2004; 52:893.
Additional EGFR Resources
n Hong WK, ullrich A. The role of EGFR in solid tumors and implications for therapy. onColoGy bIoTHERAPEuTICs, Volume 1, number 1, 2000.
n Cunningham D, Humblet y, siena s, Khayat D, bleiberg H, santoro A, bets D, Mueser M, Harstick A, Van Custem E. Cetuximab (Erbitux®) in combination with irinotecan or as single agent in patients with EGFR-expressing, irinotecan-refractory metastatic colorectal cancer (study EMR 62202-007 ‘bonD’). AsCo Abstract no. 1012, 2003.
n Mendelsohn J. Epidermal Growth Factor Receptor Inhibition by a Monoclonal Antibody as Anticancer Therapy. Clinical Cancer Research 1997; Vol. 3; 2703-2707.
n ogiso H, Ishitani R, nureki o, Fukai s, yamanaka M, Kim JH, saito K, sakamoto A, Inoue M, shirouzu M, yokoyama s. Crystal structure of the Complex of Human Epidermal Growth Factor and Receptor Extracellular Domains. Cell 2002; Vol. 110; 775-787.
n Erbitux® (cetuximab) Package Insert
n VectibixTM (panitumumab) Package Insert
n EGFR pharmDx™ Package Insert
n spaulding DC, spaulding bo. Epidermal Growth Factor Receptor Expression and Measurement in solid Tumors. seminars in oncology 2002; Vol 29, number 5, suppl 14 (october); 45-54.
n nahta R, Hortobagyi Gn, Esteva FJ. Growth Factor Receptors in breast Cancer: Potential for Therapeutic Intervention. The oncologist 2003; 8:5-17.
n nicholson RI, Gee JMW, Harper ME. EGFR and cancer prognosis. European Journal of Cancer 2001; 37: s9-s15.
n Ciardiello F, Tortora G. Epidermal growth factor receptor (EGFR) as a target in cancer therapy: understanding the role of receptor expression and other molecular determinants that could influence the response to anti-EGFR drugs. European Journal of Cancer 2003; 39: 1348-1354.
n Artegea Cl, baselga J. Clinical Trial Design and End Points for Epidermal Growth Factor Receptor-targeted Therapies: Implications for Drug Development and Practice. Clinical Cancer Research 2003; Vol 9, 1579-1589.
n Goldstein ns, Armin M. Epidermal Growth Factor Receptor Immunohistochemical Reactivity in Patients with American Joint Committee on Cancer stage IV Colon Adenocarcinoma. CAnCER 2001; Volume 92, number 5; 1331-1346.
Acknowledgements
Dr. neal Goldstein, Dr. James Thompson, Dr. Kenneth bloom, Prof. stephan störkel and betsy spaulding contributed by offering their expertise and many images that can be seen throughout this manual.


Corporate HeadquartersDenmarkTel +45 44 85 95 00
Australia+61 2 9316 4633
Austria+43 1 408 4334 50
Belgium+32 016 38 72 20
Canada+1 905 858 8510
Czech Republic+420 541 42 37 10
Denmark+45 44 85 97 56
France+33 1 30 50 00 50
Germany+49 40 69 69 470
Ireland+353 91 768150
Italy+39 02 58 078 1
Japan+81 75 211 3655
The Netherlands+31 20 42 11 100
Norway+47 23 14 05 40
Poland+48 58-661 1879
Spain+34 93 499 05 06
Sweden+46 08 556 20 600
Switzerland+41 41 760 11 66
United Kingdom+44 (0)1 353 66 99 11
United States of America +1 805 566 6655www.dako.com
Distributors in more than 50 countries 0�
0��
0�O
CT
0�



![New Trends In Internal Medicine2009hocc.medicine.psu.ac.th/files/acadamic/New_Trends... · cytopenia EGF-R profile EGFR FISH EGFR FISH docetaxel gefitinib ñu EGFR FISH Lf-]utnn EGF-R](https://img.pdfslide.net/doc/110x75/60098f15be7b15544f1b652e/new-trends-in-internal-cytopenia-egf-r-profile-egfr-fish-egfr-fish-docetaxel-gefitinib.jpg)