Embed Size (px)
Citation preview
Dallas, TX • November 2–4, 2012
GRANUOCYTE TRANSFUSIONS
Dallas, TX • November 2–4, 2012
THERESA SULLIVAN, RN,CNSMID-LEVEL PROVIDER
DEPARTMENT OF LEUKEMIA
MD ANDERSON CANCER CENTER
HOUSTON,TEXAS
Dallas, TX • November 2–4, 2012
OBJECTIVES
• At the end of this session the participant will be able to:
1. List the criteria required for granulocyte transfusion.
2. Discuss the granulocyte collection process.
Dallas, TX • November 2–4, 2012
History of GranulocyteTransfusions
• 1959-1961 Collecting, processing and transfusing of platelets cut death rates from hemorrhage in children with acute leukemia.
• 1960-1962 Focus now to infection – Granulocytes (WBC’s) collected from CML patients are transfused to pediatric leukemia patients.
Dallas, TX • November 2–4, 2012
History of GranulocyteTransfusions
• 1962- July 1965 Collaborative effort with George Judson of IBM, Robert Eisel and Dr. Freireich to develop a blood cell separator.
• July 1965 Clinical tests start on developed separator. Dr. Freireich moves to MDACC.
Dallas, TX • November 2–4, 2012
History of GranulocyteTransfusions
• 1966 New and improved NCI-IBM blood cell separator offered for field trial, MDACC gets 1of 3.
• 1974 Use of HES and steroids bring granulocyte collection process to forefront again.

Dallas, TX • November 2–4, 2012
Dallas, TX • November 2–4, 2012
History of Granulocyte Transfusions
• 1995 Advent and use of G-CSF enabled higher yield of granulocytes (WBC’s) to be collected.
• 2011 Approximately 950 granulocyte transfusions collected at MDACC.
• 2012 MDACC plans comparative study of prophylaxis vs. therapeutic use of granulocyte transfusions.
Dallas, TX • November 2–4, 2012
Indications for Granulocyte Transfusions
• Life threatening bacterial infection in a setting of prolonged neutropenia. (ANC<5)
• Life threatening fungal infection in a setting of prolonged neutropenia.
• Deteriorating condition with known infection and “correct” antibiotics.
• Improvement in infection for BMT option.
Dallas, TX • November 2–4, 2012
Neutropenia
• Risk Category ANC• 0 - none within normal limits • 1 - mild > 1500 - < 2000/mm3• 2 - moderate > 1000 - < 1500/mm3• 3 - severe > 500 - < 1000/mm3• 4 - life threatening < 500/mm3
NCI- CTC 3.0

Dallas, TX • November 2–4, 2012
Neutropenia
• Direct relationship to the degree of neutropenia and risk of infection.
• Direct relationship to the duration of neutropenia and risk of infection.

Dallas, TX • November 2–4, 2012
Process of Granulocyte Collection
• Identify possible donors
• Family members/ friends preferable
• Screening process for donors
• Standard blood banking screening
• Obtain and inject G- CSF
• 600 mcg by 8pm evening prior
• Decadron 8 mg orally
• Minimum side effects to donor

Dallas, TX • November 2–4, 2012
Process of Granulocyte Collection
• Granulocytes (WBC’s) donated- 8am
• 1 1/2 body volume processed
• 2 1/2 - 3 hour duration
• 2 arm procedure
• Males can donate 5x every other day
• Females can donate 4x every other day

Dallas, TX • November 2–4, 2012
Dallas, TX • November 2–4, 2012
Dallas, TX • November 2–4, 2012
Process of Granulocyte Collection
• Granulocytes ready for infusion by early afternoon
• All granulocytes irradiated
• Half life of granulocytes is six hours
• Transfuse within 2 hours of collection
• No good way to store granulocytes
Dallas, TX • November 2–4, 2012
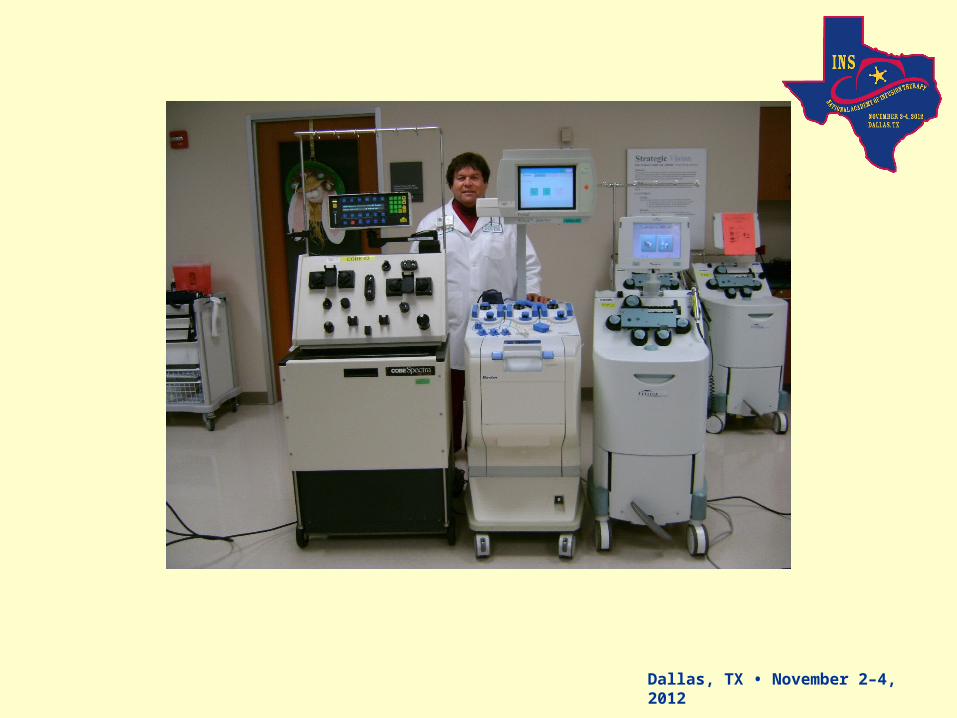
Process of Granulocyte Collection
• Use of COBE/Spectra continuous flow blood cell separator.
• Aim of Yield
• minimum 4 x 10(10) cells
• average 8 x 10(10) cells
• No need for ABO compatibility
• most RBC’s are taken out
• No need to be CMV negative

Dallas, TX • November 2–4, 2012
Dallas, TX • November 2–4, 2012
Dallas, TX • November 2–4, 2012
Granulocyte Infusions
• Transfuse over 1-2 hours
• Premedicate: 650 mg acetaminophen po 25 mg diphenhydramine IV
50-100 mg hydrocortisone IV
Meperidine for rigors prn
• Give 2 hours apart from Amphotericin B preparations
• Monitor patient for possible reactions
Dallas, TX • November 2–4, 2012
Dallas, TX • November 2–4, 2012
Possible Reactions/ Nursing Interventions
• Fever, chills r/o granulocyte reaction• Intervention: Hold transfusion Repeat premedications
Give meperidine If better can restart after 30
minutes.
Dallas, TX • November 2–4, 2012
Possible Reactions/ Nursing Interventions
• Dyspnea r/o fluid overload vs. WBC migration range from overload/pulmonary
edema/ARDS• Intervention: Furosemide IV, breathing treatment Slow infusion rate Possible intubation
Dallas, TX • November 2–4, 2012
Possible Reactions/Nursing
Interventions• Pain at infection site
i.e. chest pain, lesions
• Intervention:
analgesics
Dallas, TX • November 2–4, 2012
Evaluating Response
• Disappearance of fever
• Clearance of positive cultures
• Improvement in physical findings
• Improvement in imaging (CT, CXR)
• Improvement in performance status
Dallas, TX • November 2–4, 2012
Case Study
• 10/12/10 26 yr old married female with relapsed ALL s/p allogeneic transplant. Admit for fever and increasing counts. Start Methotrexate and Peg L- asparaginase.
• 10/16/10 c/o facial pain with sinus pressure. CT c/w acute sinusitis. Seen by ENT, frozen section—fungal hyphae.
• 10/20/10 Ambisone, caspofungin started then posaconazole
• 10/22/10 Granulocytes started. Debridement #1.

Dallas, TX • November 2–4, 2012
Case Study
• 10/31/10 Debridement # 2, biopsy still positive.
• 11/15/10 Debridement # 3, no evidence of fungus per ENT
• 11/21/10 SCT evaluation, two goals met: Decrease blast < 10% and control of fungal infection
Dallas, TX • November 2–4, 2012
Case Study
• Received total of 35 WBC transfusions over eight week period.
• Tolerated well
• Able to do some transfusions outpatient
• 12/10/10 Begin cord transplant regimen
• 12/19/10 Date of infusion of stem cells

Dallas, TX • November 2–4, 2012
Future
• Comparative study to determine if standard of care prophylactic antibiotics plus prophylactic white blood cell transfusions decrease the rate of infection compared to prophylactic antibiotics alone
Dallas, TX • November 2–4, 2012
THANK YOU!

Dallas, TX • November 2–4, 2012
QUESTIONS ?