Embed Size (px)
Citation preview

Damage pathways in prolonged deformationwith respect to pressure ulcers
Literature report of PhD thesis
K.K. CeelenSeptember 2004
BMTE04.49
Promotor: prof. F.P.T. Baaijens
Coach: dr. ir. C.W.J. Oomens
Eindhoven University of TechnologyDepartment of Biomedical EngineeringSection Materials TechnologyDivision Biomechanics and Tissue Engineering

Contents
Abbreviations 5
1 Introduction 8
2 Metabolism 9
2.1 Glucose metabolism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.1.1 Glycolysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.1.2 Anaerobic glycolysis . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.1.3 Tricarboxylic acid cycle . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2 Fatty acid metabolism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.3 Protein metabolism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.4 ATP generation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
2.4.1 Electron transport chain and oxidative phosphorylation . . . . . . 13
2.4.2 ATP synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
2.5 Coupling between metabolism and subcellular structural organization . . 14
3 Homeostasis 16
3.1 Redox state . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3.1.1 Reactive oxygen species . . . . . . . . . . . . . . . . . . . . . . . . 16
3.1.2 Reactive nitrogen species . . . . . . . . . . . . . . . . . . . . . . . 17
3.2 Ion homeostasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3.2.1 Volume regulation . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
2

Contents
4 Ischemia/reperfusion 20
4.1 Ischemia and damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4.1.1 Pressure and perfusion . . . . . . . . . . . . . . . . . . . . . . . . . 21
4.1.2 Damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
4.2 Ischemia/reperfusion and damage . . . . . . . . . . . . . . . . . . . . . . . 24
4.2.1 Reperfusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
4.2.2 Damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
5 Impaired lymph drainage 27
5.1 Pressure and lymph drainage . . . . . . . . . . . . . . . . . . . . . . . . . 27
5.2 Lymph drainage and pressure ulcers . . . . . . . . . . . . . . . . . . . . . 28
6 Cellular deformation 29
6.1 Cell membranes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
6.2 Skeletal muscle cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
6.3 Skeletal muscle tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
7 Cell death 34
7.1 Apoptosis and necrosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
7.1.1 Apoptosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
7.1.2 Necrosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
7.2 Hypoxia and cell death . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
7.3 Ions and cell death . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
7.4 Reactive oxygen species and cell death . . . . . . . . . . . . . . . . . . . . 43
7.5 Reactive nitrogen species and cell death . . . . . . . . . . . . . . . . . . . 43
8 Existing theoretical models 46
8.1 Energy metabolism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
8.2 Disturbed ion homeostasis . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
8.3 Perfusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
8.4 Lymph flow . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
8.5 Deformation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
3

Contents
9 Discussion 51
9.1 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
9.2 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
9.3 Future plans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Bibliography 54
A Muscle structure 70
B Signalling molecules in apoptosis 72
4

Abbreviations
[..]e extracellular concentration[..]i intracellular concentrationADP adenosine diphosphateAMP adenosine monophosphateANT adenine nucleotide translocase / ATP-ADP translocaseAP-1 transcription factor activator protein-1APAF-1 apoptosis protease activating factor-1ATP adenosine triphosphateBax/Bak/Bad pro-apoptotic Bcl-2 family proteinsBcl-2 founding member of Bcl-2 family, critical regulators of apoptosisBcl-XL anti-apoptotic Bcl-2 family proteinBid pro-apoptotic Bcl-2 family memberCAD caspase-activated DNAsecGMP cyclic guanosine monophosphateCK creatine kinaseCP creatine phosphatecPLA2 cytosolic phospholipase A2dATP deoxy-adenosine triphophateDISC death-inducing signalling complexe.r. endoplasmic reticulumecm extracellular matrixECP energy charge potentialEndoG endonuclease GERK extracellular signal-regulated kinaseETC electron transport chainF6P fructose-6-phosphateFAD flavoproteinFADD Fas-associated death domain proteinFADH2 reduced flavoproteinFas (CD95) death receptorFasL ligand for death receptor FasFBP fructose-1,6-biphosphate
5

Abbreviations
FE finite elementFGF fibroblast growth factorG3P glyceraldehyde-3-phosphateG6P glucose-6-phosphateGPx glutathione peroxidaseGSH glutathioneGSSG glutathione disulfideH2O2 hydrogen peroxideHNO2 nitrous acidIκB inhibitor of NF-κBIAP inhibitor of apoptosis proteinJNK (SAPK) c-Jun N-terminal protein kinases (stress-activated protein kinase)Km Michaelis-Menten constantLDH lactate dehydrogenaseMAP2K/MAPKK/MEK/MKK mitogen activator protein kinase kinaseMAP3K/MAPKKK/MEKK mitogen activator protein kinase kinase kinaseMAPK mitogen activator protein kinaseNAD+ nicotinamide coenzymeNADH+H+ reduced nicotinamide coenzymeNADP+ nicotinamide adenine dinucleotide phosphateNADPH++H+ reduced nicotinamide adenine dinucleotide phosphateNF-κB nuclear factor κBNO· nitric oxideNO2 nitrogen dioxideNO−
2 nitrite ionNO−
3 nitrate ionNOS nitric oxide synthaseO2·− superoxide·OH hydroxyl radicalomi/HtrA2 high-temperature requirement serine protease A2ONOO− peroxynitritePi inorganic phosphatep38 major component of the stress-induced apoptotic pathwayPARP poly(ADP-ribose)polymerasePEP phosphoenolpyruvatePFK phospofructokinasePI3K phosphoinositide-3 kinasePTP permeability transition poreRNS reactive nitrogen speciesROS reactive oxygen speciess.r. sarcoplasmic reticulum (muscle endoplasmic reticulum)Smac/Diablo second mitochondrial activator of caspases / direct IAP-binding protein
with low pISOD superoxide dismutase
6

Abbreviations
tBid truncated Bid, active form of BidTCA tricarboxylic acid / Krebs / citric acid cycleTE tissue engineeredTNFα tumor necrosis factor αTNFR tumor necrosis factor receptorTRADD TNFR-1 associated death domain proteinTRAIL tumor necrosis factor-α-related apoptosis-inducing ligandUQ coenzyme QUQH2 reduced coenzyme QVDAC voltage-dependent anion channelVEGF vascular endothelial growth factorXD xanthine dehydrogenaseXO xanthine oxidase
7

Chapter 1
Introduction
Despite guidelines for prevention and treatment, pressure ulcers are still a problem inhealth care. Especially bedridden en wheelchair bound people are at risk for developingthese painful ulcers, which are difficult to treat.Pressure ulcers are defined as localized areas of degenerated tissue caused by prolongedmechanical loading. The damage may extend from the skin to underlying tissues suchas subcutaneous fat and skeletal muscle, but they can also start in skeletal muscle andthen progress towards the skin. There is evidence that muscle tissue is more sensitiveto sustained mechanical loading than skin tissue.43,139,160 The prevalence of these ulcersinvolving skeletal muscle tissue (type IV) is lower than that of the more superficial typeI to III ulcers17,75, with the highest occurrence of the deep wounds in nursing homes andinstitutions for physically handicapped people.7,17 But the ones starting deep are verydangerous because they are not visible from the outside until they have reached the skin,and form a large and serious wound.
Ischemia and reperfusion, impaired lymph drainage and cell compression have all beenput forward as aetiological pathways, but many questions remain unanswered. Is there1 pathway more important than the other ones, and if so, which one is that and why?Do the different pathways reinforce each other, or do they simply add? What is themechanism that produces damage as a direct result of cellular deformation? What is theearliest sign of damage eventually leading to a pressure ulcer?
The subject of this literature study is the mechanisms probably involved in the de-velopment of damage in skeletal muscle as a result of the application of an external load.Therefore, first an overview of metabolism and homeostasis is given to provide some back-ground for studying the damage and death pathways initiated by ischemia/reperfusion,impaired lymph drainage and cellular deformation.The goal is to do a proposal for a theoretical model aimed at elucidating part of thecomplicated processes initiating pressure ulcer formation in muscle, in combination withexperimental models used in our research group. A better understanding of this aetiol-ogy should lead to identification of useful parameters to assess patient susceptibility topressure ulcers.
8

Chapter 2
Metabolism
Since the hypothesized aetiological pathways for pressure ulcers affect the energy pro-duction, a summary of metabolism is provided here.Metabolizing substrates to eventually yield ATP provides a cell the energy to fuel itsessential processes. The preferred substrates for skeletal muscle cells in rest are fattyacids, glucose or ketone bodies. The muscle cells possess an energy reservoir of glycogen,and as a final resort, muscle proteins can be degraded to amino acids and metabolized togenerate ATP.56 For the regulation of these metabolic processes, intracellular structureand localization of the processes are very important.
2.1 Glucose metabolism
2.1.1 Glycolysis
Upon entering the cell, glucose is phosphorylated to glucose-6-phosphate (G6P) by hex-okinase, using 1 ATP per molecule of glucose (figure 2.1), and requiring Mg2+. Thispriming step takes place in the cytosol and ensures that glucose does not leave the cellsince the cell membrane is virtually impermeable for G6P. Another advantage is thatthe intracellular glucose concentration is kept low, favoring diffusion of glucose into thecell.56 The activity of hexokinase is inhibited by high levels of its product G6P.56
Stored glycogen can be mobilized to generate energy by cleaving off glucose units. Theseglucose units are actually glucose-1-phosphate, which is converted to G6P to proceedinto glycolysis.56
After isomerization of G6P to fructose-6-phosphate (F6P), phoshofructokinase (PFK)uses another molecule of ATP to produce fructose-1,6-biphosphate (FBP)(figure 2.1).This step commits the cell to metabolizing glucose rather than using it for anabolic pur-poses, and it is the most important regulatory site in glycolysis.56
Among the regulators of PFK are ATP, AMP and citrate. High levels of ATP lowerthe affinity of the enzyme for F6P, and slow down its activity. Because ATP levelsnormally do not vary much, additional regulation is accomplished by AMP. When theATP availability in a cell falls, adenylate kinase can provide some ATP by catalyzingthe conversion of 2 ADP into AMP and ATP. The kinetics of this reaction cause large
9

Metabolism Glucose metabolism
relative variations in AMP concentration, making PFK activity dependent on cellularenergy status.56 Citrate is an intermediate of the tricarboxylic acid (TCA) cycle, andits involvement in PFK regulation inhibits high rates of glycolysis when the TCA cycleis already saturated.56
In the next step, the 6-carbon FBP is split into 2 3-carbon glyceraldehyde-3-phosphate(G3P) molecules. Here, the second phase of glycolysis starts, which yields 4 moleculesof ATP and 2 NADH + 2 H+ per molecule of glucose metabolized.56
The last step results in the formation of pyruvate from phosphoenolpyruvate (PEP),catalyzed by pyruvate kinase. This is the third and final regulatory site in glycolysis,and requires Mg2+ as well as K+. Pyruvate kinase is activated by AMP and FBP, andinhibited by ATP, acetyl-CoA, and the amino acid alanine (figure 2.1).56
The fate of the products of glycolysis depends on the availability of oxygen. Under aer-obic conditions, pyruvate is further metabolized in the tricarboxylic acid (TCA) cycle,and NADH+H+ are reoxidized in the electron transport chain (section 2.4.1). Anaerobicconditions however, force a cell to convert pyruvate to lactic acid to recycle NADH+H+.56
2.1.2 Anaerobic glycolysis
When the available oxygen is not sufficient to reoxidize all the NADH and FADH2 pro-duced when pyruvate enters the TCA cycle, the excess pyruvate is reduced to lactateby lactate dehydrogenase (LDH), thereby reconstituting NAD+ from NADH+H+ (figure2.1). In this way, no additional ATP is generated, making the total net ATP productiononly 2 moles per mole of glucose consumed.56 Besides this much lower efficiency in ATPgeneration, the lactate that is produced lowers the pH.
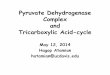
2.1.3 Tricarboxylic acid cycle
When there is enough oxygen in the cell, pyruvate is transported from the cytosol tothe mitochondria, where all subsequent metabolic steps take place. It is then convertedto acetyl-coenzyme A (acetyl-CoA), and oxidized to CO2 in the TCA cycle (also calledcitric acid or Krebs cycle)(figure 2.1).The formation of acetyl-CoA from pyruvate again uses NAD+ and forms NADH+H+,and the first CO2 molecule is produced. This reaction is mediated by pyruvate dehydro-genase which is carefully regulated because once pyruvate is converted to acetyl-CoA, itcannot be used anymore to resynthesize glucose, but instead is committed to the TCAcycle or to fatty acid synthesis. The energy status of the cell exerts control over theactivity of pyruvate dehydrogenase (figure 2.1).Acetyl-CoA then enters the cycle, and citrate synthase immediately catalyzes its com-bination with oxaloacetate to form citrate. Regulation of this enzyme occurs throughinhibition by NADH and succinyl-CoA, one of the intermediates of the cycle.Via isocitrate, α-ketoglutarate is formed, catalyzed by isocitrate dehydrogenase, whichprovides the first connection between the TCA cycle and the electron transport chainvia its production of NADH+H+. Because isocitrate dehydrogenase activity commitscitrate to the catabolic TCA cycle instead of being converted to acetyl-CoA an used inanabolic reactions in the cytosol, it is highly regulated. NADH and ATP are inhibitors,whereas NAD+ and ADP are activators.56
10

Metabolism Glucose metabolism
Figure 2.1: Glycolysis and the TCA cycle. (filled arrows mean stimulation; thick perpendicularbars mean inhibition; enzymes are written in italic)
11

Metabolism Fatty acid metabolism
The next step again produces NADH+H+, and is regulated by AMP, NADH, and itsproduct succinyl-CoA (figure 2.1). Then, the action of succinyl-CoA synthase producessuccinate and GTP, which can then transfer its energy to ADP to directly produce 1molecule of ATP.Oxidation of succinate to fumarate is carried out by succinate dehydrogenase, which isactually complex II of the electron transport chain (section 2.4.1). This reaction doesnot yield enough energy to reduce NAD+, but it can reduce FAD.Two last steps complete the cycle by regenerating oxaloacetate, meanwhile producingstill more NADH+H+.56
2.2 Fatty acid metabolism
Fatty acids are stored as triacylglycerol, mainly in specialized adipose cells, but thereis also a small amount stored in muscle cells. Triacylglycerol is hydrolyzed to release 3fatty acids, which are then metabolized in the β-oxidation pathway to yield acetyl-CoA,FADH2 and NADH+H+.β-oxidation begins with the addition of coenzyme A to the fatty acid. Hereby, ATP isdegraded to AMP and 2 Pi. This reaction takes place at the outer mitochondrial mem-brane, or at the surface of the endoplasmic reticulum for long-chain fatty acids, whileit occurs inside the mitochondria for short- and medium-length fatty acids. The fattyacyl-CoA derivatives are then carried across the mitochondrial membranes, because allthe other enzymes of the β-oxidation reside in the mitochondrial matrix. Short- andmedium-chain fatty acids in contrast, are transported into the matrix before they reactwith coenzyme A.Then, a cycle of 4 steps is repeated until the entire fatty acid is split into 2-carbonunits of acetyl-CoA, which can enter the TCA-cycle (figure 2.1). In each cycle of theβ-oxidation, 1 molecule of FADH2 is formed, and 1 NADH+H+, both of which can bereoxidized in the electron transport chain yielding 4 molecules of ATP per β-oxidationcycle. Each rotation of the TCA cycle with subsequent electron transport chain addsanother 10 molecules of ATP.56
An alternative route of energy production from fatty acids is via the generation of ketonebodies from acetyl-CoA, which occurs primarily in the liver. These ketone bodies areeasily transportable through the blood, to deliver them to energy-requiring cells, whichconvert them to acetyl-CoA again.56
2.3 Protein metabolism
Breakdown of proteins into amino acids provides another source of substrates for theTCA cycle, but it is unusual under normal circumstances. When amino acids are usedas an energy source, for example in starvation, they first have to be deaminated, releasingammonia. Liver cells remove this ammonia from the blood and convert it to urea, whichis excreted by the kidneys.69 The amino acids can then be converted to pyruvate or oneof the intermediates of the TCA cycle, and subsequently enter the TCA cycle, or beconverted to lactate.56,69
12

Metabolism ATP generation
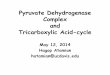
Figure 2.2: Electron transport and oxidative phosphorylation in the inner mitochondrial mem-brane: Complexes I and II transfer electrons via complex III to complex IV, which reduces oxygen.The action of complexes I, III and IV produces a proton gradient across the inner mitochondrialmembrane, driving the actual ATP formation.56
2.4 ATP generation
ATP is the energy currency in cells. Only a small amount of ATP is stored in the cell,but this is supplemented with a little creatine phosphate (CP). Creatine kinase (CK)catalyzes the conversion of CP to creatine, thereby phosphorylating ADP to ATP. Theearlier mentioned adenylate kinase is another enzyme involved in ATP/ADP homeostasis(figure 2.1).56,104 Both enzymes also catalyze the reverse reactions.But ATP is generated mainly as a result of oxidative phosphorylation in the mitochon-dria, and a little is directly produced during glycolysis and the tricarboxylic acid cycle.
2.4.1 Electron transport chain and oxidative phosphorylation
During the oxidation of metabolites, nicotinamide coenzymes (NAD+) and flavopro-teins (FAD) are reduced to NADH+H+ and FADH2 respectively.56 Reoxidation of thesemolecules in mitochondria shuttles the stored energy into ATP.For this purpose, an electron transport chain (ETC) consisting of 4 distinct protein com-plexes exists in the inner membrane of mitochondria. The first two complexes transferelectrons and protons from NADH+H+ and FADH2 to reduce coenzyme Q (UQ) toUQH2. Complex III reduces cytochrome c with the electrons from UQH2, while its pro-tons are transported to the intermembrane space. Additional protons are transportedfrom the mitochondrial matrix to the intermembrane space through the actions of com-plexes I, III and IV (figure 2.2). Complex IV, which is called cytochrome c oxidase,catalyzes the reduction of O2, which is the final acceptor of the electrons. Together withprotons from the mitochondrial matrix, it is converted to water.Regulation of oxidative phosphorylation occurs through ATP-demand, the supply of
13

Metabolism Coupling between metabolism and subcellular structural organization
NADH+H+, FADH2 and oxygen, and diffusion restrictions and the CK system (section2.5).98
2.4.2 ATP synthesis
The proton gradient across the inner mitochondrial membrane created with the ETCdrives the actual ATP synthesis. This is carried out by ATP synthase (also called F1F0-ATPase), located in the inner mitochondrial membrane. This enzyme dissipates theproton gradient by moving 4 protons to the mitochondrial matrix while forming 1 ATPfrom ADP and Pi. Given that every 2 electrons that pass from NADH+H+ to O2 transferapproximately 10 protons across the inner mitochondrial membrane, 5 molecules of ATPare formed for every molecule of oxygen consumed, or 2.5 for every pair of NADH+H+.However, in the case of FADH2 electrons, this is only 1.5 per NADH+H+, because theelectrons and protons from FADH2 are removed by complex II, which does not contributeto the proton gradient (figure 2.2).ATP is then exchanged with ADP by ATP-ADP translocase (also called adenine nu-cleotide translocase (ANT)), delivering ATP to the cytosol and transporting ADP to themitochondria to be converted to ATP again.
2.5 Coupling between metabolism and subcellular struc-tural organization
More and more evidence is accumulating that compartmentation, channelling of sub-strates between two consecutive enzymes, close proximity of two consecutive enzymes orof enzyme and the site of substrate formation, are important for metabolic rates.49,77,172
This means that substrate and enzyme localizations in the highly structured, dynamiccell organization with organelles, pumps, motors and channels, are essential in under-standing and predicting a cell’s energy status.Indications for the necessary existence of structural regulation are constrained movementof macromolecules by cellular structures, and of small molecules by binding or collisionswith solid cell structures, or by cytoplasmic viscosity.77
An important advantage of the structurally ordered metabolism is that it can explainthe large variations in metabolic rates with minimal changes in substrate concentrations(homeostasis). Higher metabolic rates would simply occur through higher intracellularconvection rates.76
The CK shuttle system is an example of a way in which the cell handles diffusion dif-ficulties. It helps overcome the ADP diffusion restrictions of the outer mitochondrialmembrane.98,172 CK in the intermitochondrial space catalyzes the transfer of the high-energy phosphate from ATP to creatine, creating CP, ADP and H+.94,96,161 CP is ableto cross the outer mitochondrial membrane, and in the cytosol or at the myofibrils, cy-tosolic or myofibrillar CK catalyzes the reverse reaction to create ATP at the sites whereit is needed.
14

Metabolism Coupling between metabolism and subcellular structural organization
Andrienko et al.6 found evidence of the existence of intracellular energetic units, func-tional complexes of mitochondria, sarcoplasmic reticulum and myofibrils in cardiac my-ocytes. Mitochondrial structure and oxygen consumption were affected by Ca2+-inducedcontraction.Glycolytic enzymes are also confined to a specific site in the cell. With the exception ofhexokinase, which can reversibly bind to mitochondria3, glycolytic enzymes are predom-inantly localized at the myofibrillar I-band (appendix A).46,147 Kraft et al.96 found thatmuscle type CK was co-localized to the I-band with the glycolytic enzyme PFK at rela-tively acidic pH (pH 6.5). This coupling between glycolysis and CK could be functionalin converting the glycolytically produced ATP into CP, maintaining low ATP levels andthereby preventing PFK inhibition by ATP.Other cellular adaptations to facilitate intracellular energetic communication may in-clude cytoplasmic streaming, movement of mitochondria in response to energy demand,and flux transfer chains in which incoming ligands at one end of a rapid-equilibratingenzyme chain, increase their own concentration at the other end.49
15

Chapter 3
Homeostasis
Controlling the intra- and extracellular space is essential for a tissue to stay healthy.This means that, among others, the pH has to be kept constant, the redox state of thecell has to be regulated and ion homeostasis has to be maintained. To accomplish this,membrane integrity and energy production are essential. Membranes serve to separatethe intra- and extracellular compartments as well as intracellular organelles from thecytosol.There are a lot of ways in which the delicate tissue homeostasis can be disturbed, leadingto cellular damage and eventually cell death. To understand these damage-producingmechanisms probably involved in pressure ulcer development, a few homeostatic pro-cesses will be discussed here.
3.1 Redox state
Cells continuously produce free radicals, such as nitric oxide, and reactive oxygen species(ROS) as part of metabolic processes.41,182 These reactive nitrogen and reactive oxygenspecies have numerous interactions. An elaborate antioxidant system neutralizes thesemolecules to maintain a homeostatic redox state in the cell. Oxidative stress results froman imbalance between ROS and antioxidants.
3.1.1 Reactive oxygen species
The ROS that are generated in cells include free radicals such as superoxide (O2·−) andhydroxyl radicals (·OH), as well as nonradical reactive species like hydrogen peroxide(H2O2).The most important source of these molecules is the electron transport chain in themitochondria, which uses up to 5% of the oxygen consumed to generate ROS.41,59,182
Complex I and UQ can accept either one or two electrons, and in the first case, theybecome free radicals capable of reducing O2 to superoxide.Another source of superoxide, which becomes more relevant in ischemia, is xanthine ox-idase (XO). The enzyme xanthine dehydrogenase (XD) can be converted to XO, which
16

Homeostasis Redox state
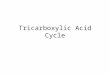
Figure 3.1: Glutathione defense against ROS: Oxidation of GSH reduces H2O2 to water. GSHcan be reconstituted from GSSG by the action of glutathione reductase while using NADPH.182
can transport electrons to O2.59,123
Most of the superoxide ends up as hydrogen peroxide, either by spontaneous or by en-zymatic dismutation. Superoxide dismutase (SOD) catalyzes the dismutation in thefollowing reaction:83
2 O2·− + 2 H+ → O2 + H2O2
H2O2 can react according to the Fenton reaction or the Haber-Weiss reaction to form·OH:41,59,83
Fenton reaction: Fe2+ + H2O2 → Fe3+ + ·OH + −OHHaber-Weiss reaction: O2·− + H2O2 → O2 + ·OH + −OHCellular defense against ROS consists of antioxidants and enzymes. Hydrogen peroxidemay be converted to water and oxygen by catalase:59
2 H2O2 → 2 H2O + O2
But one of the most important cellular defenses against ROS is glutathione (GSH). This isan antioxidant that is oxidized to glutathione disulfide (GSSG), catalyzed by glutathioneperoxidase (GPx). Simultaneously, hydrogen peroxide is reduced to water (figure 3.1).182
Glutathione reductase then converts GSSG back to GSH, thereby using NADPH+H+,which can be reconstituted from NADP+ via the pentose phosphate pathway.56,59,123,182
Apart from the detoxification of hydrogen peroxide, GSH is also involved in the protec-tion against membrane lipid peroxidation: GSH regenerates ascorbate from its oxidizedform, which in turn can regenerate α-tocopherol from its radical form at the lipid-waterinterface. α-Tocopherol is the major lipid-soluble antioxidant, providing protection tomembrane poly-unsaturated fatty acids vulnerable for lipid peroxidation by free radicals,which can severely interfere with membrane function.123
3.1.2 Reactive nitrogen species
Nitric oxide (NO·) is a free radical that is involved in many physiological processes inskeletal muscles, including vascular control, metabolism, and contractile functions. Itis a small, reactive, freely diffusing gas molecule.59,154 Its synthesis requires molecularoxygen:l-arginine + O2 + NADPH → citrulline + NO·This reaction is catalyzed by nitric oxide synthase (NOS), which exists in a few isoforms,
17

Homeostasis Ion homeostasis
including a mitochondrial103 and an inducible one that is expressed in the cytosol inresponse to cytokines. NOS is regulated by calmodulin, which is dependent on Ca2+.154
NO· may subsequently react with O2 to produce the more reactive radical nitrogendioxide:59
2 NO· + O2 → 2 NO·2
But most of the time, it is scavenged by oxyhemoglobin or oxymyoglobin to producemethemoglobin or metmyoglobin and nitrate (NO−
3 )26,52,59,154, or it is oxidized to thenitrite ion (NO−
2 ):59
4 NO· + O2 + 2 H2O → 4 NO−2
Vitamin E (γ-tocopherol) is the main membrane antioxidant against NO·.41Other reactive nitrogen species (RNS) are generated when nitric oxide reacts with ROS:59
peroxynitrite formation: NO· + O2·− → ONOO−
nitrous acid formation: NO· + ·OH → HNO2
At the level of the NO· synthesis, there is also an interaction with ROS. When theavailability of l-arginine is limited or the active site of NOS is inhibited, NOS can generatesuperoxide instead of NO·.154
3.2 Ion homeostasis
The cell membrane functions as a selective barrier for ions and other molecules. This ex-plains the differences in ion concentrations between intracellular and extracellular milieu(table 3.1), crucial to normal cell functioning. The ion gradients across the cell mem-brane also lead to a polarization of the membrane, with a negative potential of -60mVin the cell.15
Table 3.1: Ion concentrations15,69,196
ion extracellular fluid intracellular fluidNa+ (mM) 142-145 10-15K+ (mM) 4-4.5 120-150Ca2+ (mM) 1.2-2.4 <10−4
H+ (mM) 4·10−5 (pH 7.4) 6·10−5-1·10−4 (pH 7.0-7.2)Cl− (mM) 100-120 4-20
Note that concentrations may vary somewhat in different cell types15,196
Passive and active transport, either through the lipid bilayer constituting the cell mem-brane, or through proteins in this bilayer, serve to maintain the ion gradients. Passivetransport either occurs through simple diffusion through the cell membrane, or throughfacilitated diffusion through protein pores, gated channels or carriers spanning the mem-brane. Active transport can be both primary, using ATP, or secondary, using the move-ment of one solute down its gradient to fuel the transport of another solute against itsgradient.15
The Na+/K+ pump in the cell membrane is one of the most important ion pumps. Itexchanges 2 extracellular K+ ions for 3 intracellular Na+ ions to keep [Na+]i low and[K+]e high. At the same time, the 2:3 ratio makes this pump electrogenic, contributingto the negative potential inside the cell. Creating a steep K+ gradient favors a K+ ef-flux, and since this efflux is unmatched by an anion efflux, this is the main cause of thenegative potential.
18

Homeostasis Ion homeostasis
This negative potential repels Cl−, resulting in a [Cl−]i that is 10 times lower than [Cl−]e,at least in skeletal muscle cells since they have no active uptake of Cl−.15
The steep Na+ gradient is used as a driving force for a lot of exchangers. Na+/Ca2+
exchangers, together with Ca2+ pumps in the cell and e.r. membrane keep [Ca2+]i 4 or-ders of magnitude lower than [Ca2+]e. The Na+/H+ exchanger and Na+-driven HCO−
3
transporters maintain the pH and [HCO−3 ]i at their steady state values.
Calcium homeostasis is extremely important in muscle cells because it is associatedwith excitation-contraction coupling. Stimulation initiates a large Ca2+-flux from thesarcoplasmic reticulum to the cytoplasm, where it binds to troponin C to release inhibi-tion of actin-myosin interaction. At the end of stimulation, calcium is rapidly pumpedback into the sarcoplasmic reticulum, leaving the cytosol almost completely devoid ofcalcium (Toth et al.177 report 100nM as a frequently used value for intracellular Ca2+
in resting skeletal muscle). Thus, the sarcoplasmic reticulum stores a lot of calcium, andthe calcium concentration in muscle cytosol reaches a peak value far above the valuementioned in table 3.1, although most of it will be bound.
3.2.1 Volume regulation
Transport of water across the cell membrane is a passive process, which responds todifferences in osmolality between both sides of the membrane, an osmotic pressure differ-ence. The Na+/K+ pump is extremely important in keeping normal cell volume, becauseit extrudes 3 Na+ in exchange for 2 K+ to counteract their passive fluxes, and to com-pensate for the intracellular presence of non-permeable solutes.15,134 Consequently, thereis no osmotic pressure difference across the membrane, and no net water movement.15
Cells respond to changes in volume by activating channels or transporters to transfersolutes across the membrane, in particular K+ and Cl−. Water will follow through os-mosis, bringing cell volume back to normal.15
The lymphatic system is also important in maintaining osmotic and hydrostatic pressuresin a tissue, and thereby regulates tissue volume. It does this by providing a transportsystem for fluid and proteins that cannot be reabsorbed into blood capillaries.175 Inthe lymphatic capillaries between the cells, which consist of no more than one layer ofendothelial cells, lymph is formed.The high permeability of the lymph vessels implies that lymph has nearly the samecomposition and concentration as interstitial fluid, and that uptake of macromoleculesinto the lymph vessels is probably limited by movement through the extracellular matrix(ecm).175
Lymph flow is driven by intermittent external compression (from muscle contraction,arterial pulsations, or respiration), as well as by intrinsic pumping of the larger vessels.These vessels have valves, and their walls contain smooth muscle cells. A segment be-tween two valves automatically contracts when it is stretched with fluid, draining a tissueof excess fluid, and preventing hydrostatic pressure build-up.69,175
19

Chapter 4
Ischemia/reperfusion
Vascular supply to a muscle consists of external feed arteries, of which the arteriolarnetwork branches that enters the muscle. After several orders of branching, the terminalarterioles are the last branches to contain smooth muscle cells, and thus control bloodflow. Each terminal arteriole supplies a group of 15 to 20 capillaries that run parallel tothe muscle fibers for 1mm or less, to end in a collecting venule. Each group is called amicrovascular unit (figure 4.1).
Figure 4.1: Skeletal muscle circulation: The feed arteries (not shown) branch into the primaryarterioles, from which eventually the terminal arterioles branch off, that each supply one mi-crovascular unit, consisting of 15-20 capillaries that directly overly the individual muscle fibers.Blood in these capillaries collects into the collecting venules.15
20

Ischemia/reperfusion Ischemia and damage
4.1 Ischemia and damage
Ischemia has often been thought to be one of the major factors in pressure ulcer de-velopment.31,66,100,156,158,164,177 Tissue compression would cause diminished blood flowthrough the tissue, compromising nutrient and oxygen supply as well as waste productremoval.
4.1.1 Pressure and perfusion
Blood flow is proportional to the pressure gradient over the blood vessel divided by theresistance to flow. In capillary beds, this resistance to flow is mainly determined by theupstream resistance. Both myogenic regulation and chemical factors serve to maintainappropriate tissue perfusion under changing conditions. Myogenic regulation refers tothe intrinsic property of smooth muscle cells in vessel walls to contract when they arestretched, resulting in vasoconstriction. Interstitial pH and concentrations of oxygen, lac-tate, ATP and ADP for example, are chemical factors that locally affect smooth musclecell contraction to increase blood flow when metabolism is increased.15
Externally applied loads may interfere with the normal capillary perfusion, either throughsome degree of capillary collapse, or through a decrease in the driving pressure gradientor an increase in vascular resistance. The first mechanism simply states that after acertain rise in intramuscular pressure, the transmural pressure that normally keeps thecapillary open, becomes smaller and the capillary lumen diminishes or closes.186 Thelatter phenomenon can be explained by the vascular waterfall theory.
This theory describes the interaction between the intramuscular pressure and bloodflow. It states that when intramuscular pressure is above outflow pressure, the pressuregradient between inflow and intramuscular pressure is the driving force for perfusioninstead of the difference between inflow and outflow pressure.47,155,170
Evidence for this theory came among others from Reneman et al.155 and Shrier et al.170.They placed a muscle in an airtight box and increased the pressure inside the box. Thisresulted in an increase in intramuscular pressure approximately equal to the applied boxpressure. As a result, transmural pressure decreases and venules are the first to be com-pressed due to their high compliance. Venular pressure increases to levels comparableto the intramuscular pressure, as long as this is higher than venular pressure.128,155 Inthis range, blood flow was independent of venous outflow pressure, and decreased pro-portional to the box pressure.71,128,170,186 Since arterial pressure remains constant, thedriving force for the flow is the arterial pressure minus box (intramuscular) pressurerather than arterial pressure minus outflow venous pressure.Both Shrier et al.170 and Mellander et al.128 found that resistance between arterial inflowand venules was only slightly increased, and could have only a minor contribution to theobserved flow impairment. The pressure downstream of the increased venular pressuretends to decrease as a result of the diminished flow. Thus, the intravascular pressurefalls from approximately intramuscular pressure to systemic venous pressure, which iscalled the vascular waterfall.
The above mentioned studies were all performed to gain more insight into the compart-
21

Ischemia/reperfusion Ischemia and damage
ment syndrome, and assumed a homogeneous elevation of the intramuscular pressure.The question remains whether the vascular waterfall theory is also necessary to explainperfusion patterns in situations of locally elevated pressures, such as is the case in pres-sure ulcer development.Vankan et al.183 developed a biphasic porous media model with a hierarchical bloodflow from arteries, via arterioles, capillaries and venules to veins, and elastic blood vesselwalls to relate the local blood volume to the transmural pressure. Results from thismodel were consistent with experimental findings by Shrier et al.170, and thus predictedthe existence of a vascular waterfall in the venous compartment, without assuming itbeforehand.Van Donkelaar et al.47 used this finite element (FE) model to simulate blood perfusion ina contracting muscle, in which intramuscular pressure was heterogeneously distributed.They demonstrated that local spatial interactions between intramuscular and venouspressures determine perfusion, in full agreement with the vascular waterfall theory. Butthe finding that venous pressure may increase independent of the intramuscular pressure,but instead due to impeded venous drainage downstream (figure 4.2), is in contrast withthis theory. The location of the supplying arteries and draining veins appeared to beimportant.
Figure 4.2: Venous pressure, intramuscular pressure, and capillary flow in contracting skeletalmuscle: In the upper panels, there is one supplying artery and one draining vein at the left endof the muscle. In the lower panels, there is an additional pair of large vessels at the right end.47
4.1.2 Damage
Since skeletal muscle cells are known to survive maximally 4 hours of ischemia12, cellularinjury is likely to follow a prolonged period of ischemia. The extent of the damage isdirectly related to the severity and duration of the ischemia.Obviously, ischemia and the concomitant hypoxia seriously interfere with metabolismbecause of a lack of oxygen and nutrient supply. A cell has to rely on its endogenousenergy stores, being ATP, CP, glycogen, triacylglycerol, and proteins. If there is stillsome oxygen supply, oxidative phosphorylation can take place at a reduced rate. Atsome point however, the NAD+/NADH ratio will be too low to sustain adequate TCAcycling, and the cell has to rely solely on anaerobic glycolysis (section 2.1.2). Due to theconsequent lactate and H+ accumulation, aggravated if venous and lymphatic drainageare also affected, intracellular pH decreases, and added to the low NAD+/NADH ratio,this slows down glycolysis. Lactate formation however, helps increase the NAD+/NADHratio, thereby providing the cell the opportunity to still generate energy.
22

Ischemia/reperfusion Ischemia and damage
Knight et al.91 applied a load to the sacrum of human volunteers and simultaneouslyrecorded local transcutaneous tensions of oxygen and carbon dioxide, and analyzed col-lected sweat for lactate and urea. They found that a 60% reduction in transcutaneouspO2 coincided with a threshold for CO2, urea and lactate accumulation. Accumulationsof CO2 are the result of impaired waste removal and increased anaerobic glycolysis re-spectively, two different aspects of tissue ischemia. Therefore, Knight et al.91 suggestedthat a 60% reduction in pO2 could be a critical level for the development of tissue damage.
Lindsay et al.111 assessed the concentrations of various metabolites after 4 and 5 hoursof ischemia. In both cases, CP was almost entirely depleted but it was rapidly restoredduring reperfusion, reaching its initial levels after 30 to 45 minutes following 5 hoursof ischemia, and already after 5 minutes of reperfusion following 4 hours of ischemia,followed by an overshoot.The energy charge potential (ECP), considered to be a good measure of a cell’s energystatus, and equal to ATP+1/2ADP
ATP+ADP+AMP , was reduced to less than 90% of its pre-ischemicvalue, but almost completely restored within 5 minutes of reperfusion after 4 hours ofischemia. But 5 hours of ischemia led to a more serious reduction in ECP of almost 25%,which had not fully recovered after 45 minutes of reperfusion. Reduced ATP levels werethe most important contributors to these ECP reductions, and they did not recover in45 minutes of reperfusion.Hayes et al.73 found a reduction to less than 85% of pre-ischemic values after 4 hoursof ischemia, and a recovery to nearly 95% after 30 minutes of reperfusion, comparableto the results of Lindsay et al.111 A significant relation between the extent of energydepletion and the amount of necrosis was found by Hayes et al.73, which is supported bythe findings of Lindsay et al.111
A consequence of the decreased ATP production is diminished activity of membraneion pumps, disturbing ion homeostasis (section 7.2), impaired synthesis of chemical com-pounds in the cell, and interference with mechanical work.69 But hypoxia also leads todamage through interference with other processes in the cell than energy metabolism.The small amount of oxygen that is present can be converted to reactive oxygen speciesthrough the action of the electron transport chain30 or XO105, of which the harmful ef-fects are described in section 7.4. Hypoxia can also induce NOS, generating reactivenitrogen species103 (section 7.5).
Damage to skeletal muscle due to ischemia can be reduced by ischemic precondition-ing.9,187,188 A brief period of ischemia (up to 45 minutes), followed by reperfusion of upto 60 minutes provides protection against the injury induced by a subsequent longer pe-riod of ischemia, called early or classic preconditioning. Late or delayed preconditioningis a term used for the protective effect seen when the reperfusion period is lengthened to24 hours or more.9,51,187,188
Badhwar et al.9 preconditioned rat skeletal muscle with 5 cycles of 10 minutes of is-chemia separated by 10 minutes of reperfusion. They found slightly less injury in thepreconditioned muscle than in the non-preconditioned muscle following 2 hours of is-chemia and 90 minutes of reperfusion, but this difference was not visible immediatelyafter the 2 hours of ischemia. Inhibition of the inducible form of NOS during precondi-tioning abolished the protection against tissue injury afforded by preconditioning, but itdid not abolish the increase in the amount of perfused capillaries seen during reperfusion
23

Ischemia/reperfusion Ischemia/reperfusion and damage
in the preconditioned muscle.Late preconditioning is most probably mediated by induction of the synthesis of cer-tain proteins, among which antioxidant enzymes.51 Wang et al.188 demonstrated thatadenosine, a dilator of small arteries and arterioles, and nitric oxide administration bothmimicked the effect of late ischemic preconditioning, and that the effect of nitric oxidewas dependent on adenosine.
4.2 Ischemia/reperfusion and damage
Besides ischemia induced by an external load, removal of this load to restore perfusion tothe ischemic tissue, can also constitute a problem. It can exacerbate the damage insteadof relieving the tissue of its shortages and removing excess waste.
4.2.1 Reperfusion
A lowered transmural pressure in the arterioles, the oxygen lack in the cells, vasodila-tory agents released from the anoxic cells, or a combination of these may all lead tovasodilatation after ischemia, resulting in reactive hyperaemia, an increased blood flowresponse immediately after an ischemic period.130
But after an extended period of ischemia, intravascular hemoconcentration and throm-bosis, swelling of capillary endothelial cells (as a result of deficient cell energy reserve),leukocyte plugging of capillaries, increased extravascular tissue pressure caused by inter-stitial oedema formation or cellular oedema, and irreversible contraction of the smoothmuscle cells in the feeding arterioles due to a rise in intracellular Ca2+, can alternativelylead to the ’no-reflow’ phenomenon.2,129,130
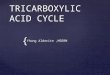
Blaisdell12 mentions that this does not occur until after 6 hours or more of completeischemia. Indeed, Homer-Vanniasinkam et al.80 found a small transient increase in per-fusion after 6 hours of ischemia, rising to approximately 30% of the pre-ischemic valueafter 2 hours of reperfusion, but declining again to almost zero after 4 hours of reperfu-sion. Bonheur et al.14 also found a decline in perfusion after an initial incline, but theperfusion peak was earlier and higher. After 6 hours of ischemia, perfusion recovered toapproximately 50% of the pre-ischemic perfusion after 1 minute of reperfusion. There-after, it gradually decreased to roughly 20% after 4 hours (figure 4.3).An ischemic period of only 3 hours gave the same trend in reperfusion, but with totalrecovery to pre-ischemic perfusion after 1 minute, and a 50% reduction after 4 hours.Only 1 hour of ischemia did not lead to significant differences in perfusion compared tocontrol values (figure 4.3).
4.2.2 Damage
If perfusion restoration is successful, it can be even more harmful than ischemia itself.Breakdown products from dying cells (such as Pi, lactate, myoglobin, nucleotides, K+,proteolytic enzymes, nucleotides and purine bases G and A) are triggers for an inflam-matory response. The inflammatory cells are required to clean up the damaged tissue,
24

Ischemia/reperfusion Ischemia/reperfusion and damage
Figure 4.3: Relationship between duration of limb ischemia and reperfusion: Perfusion in micesubjected to 1 hour of ischemia followed by reperfusion returned to basal levels during reperfusion(1/4 I/R). In contrast, mice exposed to 3 (3/4 I/R) or 6 (6/4 I/R) hours of ischemia decreasedtheir flow during reperfusion significantly when compared to sham mice (*P<0.05). There is alsoa significant difference between reperfusion in mice exposed to 6 hours of ischemia compared tomice exposed to only 3 h of ischemia (+P<0.05).14
but they can also have adverse effects.12 They release additional inflammatory medi-ators, proteolytic enzymes that destruct the endothelial’s barrier function, and oxygenfree radicals.2,12
Destruction of the endothelial’s barrier function implies among others an increased vascu-lar permeability to plasma proteins99,115,167, with ensuing progressive interstitial oedemaupon reperfusion.12,14,80,102,138 Kurose et al.99 already found an increase in protein leak-age from post-capillary venules after only 20 minutes of ischemia. Nanobashvili et al.138
observed mild interstitial oedema after 1 hour of ischemia followed by 2 hours of reper-fusion, and severe oedema when the ischemic period was extended to 2.5 hours.Abnormal levels of oxygen free radicals are abundantly studied and very importantmolecular mediators of ischemia/reperfusion injury because they inflict a lot of da-mage.9,81,111,164,173 They are not only generated by the invading inflammatory cells,but also by the previously ischemic muscle cells. Excess catabolic activity during is-chemia leads to accumulation of precursors of ATP, which are eventually degraded tohypoxanthine or xanthine. Accumulation of intracellular Ca2+ leads to the conversion ofXD into XO123,130, which stimulates the reaction of (hypo-)xanthine with oxygen uponreperfusion, producing superoxide2,123,130 with all kinds of deleterious consequences (sec-tion 7.4).Depletion of glutathione during ischemia also contributes to the oxidative stress duringreperfusion because of a reduction in protection.123 The inflammatory response is aggra-vated through the attraction of leukocytes as a result of the oxidative stress.2
25

Ischemia/reperfusion Ischemia/reperfusion and damage
There have been a lot of studies regarding the amount of damage after different durationsof ischemia and reperfusion. Most of them used rats, and a tourniquet or microvascularclips to induce ischemia in one leg of the animals. Damage assessment ranged from mi-croscopy to different biochemical markers for necrosis, or functional properties.Some of the researchers assessed injury immediately after the release of ischemia, andfound damaged cells.4,9, 19 Most of them saw this damage increase during a few hoursof reperfusion9,19, but Akahane et al.4 did not reassess damage until after 3 days ofreperfusion, and found that damage due to 3 hours of ischemia was reversed then. How-ever, 6 hours of ischemia resulted in too much damage to reverse, even with 7 days ofreperfusion. Cowled et al.39 also saw a decrease in damage due to 4 hours of ischemiaafter 72 hours of reperfusion compared to 24 hours, and the same goes for Paek et al.141
who observed a decrease from 3 to 24 days.Others did not see any muscle damage after ischemia alone, but only after some reper-fusion.80,81,138 There are also a lot of studies in which they only assessed damage duringreperfusion, so from these studies no conclusions can be drawn about whether or notreperfusion is necessary to initiate damage.14,39,67,73,100,102,111,141,144,164
Although most studies focused on necrosis, some specifically looked for apoptosis anddid not find it. Cowled et al.39 and Knight et al.90 did not see any apoptotic muscle cellsafter 2 and 4 hours of ischemia respectively and 2 to 72 hours of reperfusion. On theother hand, Hatoko et al.72 did find apoptosis in skeletal muscle cells after both 3 and 6hours of ischemia followed by reperfusion, and so did Santore et al.162 in lung epithelialcells after 48 hours of anoxia, and Webster et al.190 and de Moissac et al.133 in cardiacmyocytes.
26

Chapter 5
Impaired lymph drainage
5.1 Pressure and lymph drainage
The task of the lymphatic system is to keep osmotic pressure in the interstitium constant,and to prevent the hydrostatic pressure from rising to unacceptable levels. Therefore,high interstitial pressures lead to increased lymph drainage, until it reaches a certainmaximum rate.69,122,152 Then, lymphatic drainage remains constant despite a furtherrise in hydrostatic pressure, but too high pressures lead to impaired drainage.122 Milleret al.131 found that lymph clearance in the skin increased until the externally appliedpressure exceeded 60-70 mmHg (8-9.3 kPa). Then, clearance rapidly fell to zero.Anchoring filaments are responsible for the high sensitivity of the lymphatic capillary lu-men to interstitial stresses, because they tether lymphatic endothelial cells to the ecm.175
When interstitial fluid accumulates, the permeability of the lymphatic capillaries becomeslarger as a result of tension on the anchoring filaments (figure 5.1).69,149,175 Fluid subse-quently enters the lymphatic capillaries and increases the intravascular pressure, whichthen causes closure of the overlapping endothelial cells to prevent backward flow into theecm.69 Thus, lymphatic capillaries do not collapse under increased tissue pressure175, atleast not when this pressure is the result of an increased amount of fluid.
Figure 5.1: Cross-section of lymphatic capillaries: Tension on the anchoring filaments leads toopenings between the overlapping endothelial cells, to enable fluid to enter the lymphatic capil-lary.175
But increasing tissue pressure may also compress the larger lymphatics, thereby imped-ing lymph flow and opposing the increased lymph entry.69,149 Another possibility is thatthe anchoring filaments or the lymphatic capillaries become damaged, also leading to
27

Impaired lymph drainage Lymph drainage and pressure ulcers
inhibition of lymph flow.149
The consequence of reduced lymphatic clearance is accumulation of metabolic wasteproducts, proteins and enzymes.149 The accompanying disturbed osmotic balance leadsto extracellular oedema, which lengthens the diffusion distance from capillaries to cells.
5.2 Lymph drainage and pressure ulcers
Oedema is included in the description of the first stage of pressure ulcers, involvingonly superficial skin layers.1 Diegelmann44 found less evidence of matrix dissociationand edema in the deeper regions of biopsies of chronic pressure ulcer wounds (stage IIIor IV) than in the upper areas.44 But Nanobashvili et al.138, Bonheur et al.14, Homer-Vanniasinkam et al.80 and Labbe et al.102 did find oedema in muscle tissue after extendedperiods of ischemia/reperfusion.Swartz et al.176 made mice tails oedematous (50-100% increase in tail diameter) by lig-ation of the lymphatics at the tail base. They found that increased hydrostatic pressuredue to oedema caused a decrease in lymphatic drainage.However, it can be argued that skeletal muscle oedema has another cause than impededlymphatic drainage since the permeability of blood capillaries in skeletal muscles is verylow compared to that in most other tissues, so there is not much fluid filtration andlymphatic drainage is relatively unimportant.69 The endomysium of muscles does noteven have real lymphatic channels, but just prelymphatics, which are minute interstitialchannels.69
Still, already in 1981, Reddy et al.150 suggested that the slow viscous flow of inter-stitial fluid might play a significant role in tissue breakdown in pressure ulcers, becausethey found a similarity between pressure-duration relationship in the experimental pro-duction of pressure ulcers, and the inverse relationship between pressure intensity andload duration required to squeeze a certain part of the interstitial fluid out of a pressur-ized volume into a non-pressurized surrounding volume150.Reddy et al.151 also found that only part of an externally applied pressure was trans-mitted to the interstitial fluid, and hypothesized that the rest was supported by theextracellular collagen network. Increased collagen catabolism as observed in spinal cordinjured patients34 would result in increased loading of interstitial fluid and the blood andlymph capillaries, possibly explaining the increased susceptibility to pressure ulcers fromspinal cord injured patients.149
Apart from the effect of external pressure on the lymphatics, immobility, one of the riskfactors for pressure ulcer development, might contribute to lymph stasis since musclecontraction is one of the driving forces for lymph propulsion (section 3.2.1). Further-more, ischemia could affect the smooth muscle cells in the lymphatics, impairing theircontraction, which also leads to a stagnation of lymph flow.
28

Chapter 6
Cellular deformation
This chapter concerns direct harmful effects of compression of the skeletal muscle cells.Sustained deformation of cells may cause local membrane stresses, volume changes, andmodifications in cytoskeletal organization, which may damage the cell.18,36
6.1 Cell membranes
Friedrich et al.54 and Kato et al.87 studied the influence of high hydrostatic pressureson plasma membranes. Friedrich et al.54 assessed membrane ion conductances of mouseskeletal muscle after high-pressure treatment, and Kato et al.87 specifically looked atthe Na+/K+ ATPase activity in pig kidney membranes. They both applied hydrostaticpressures in the range of MPa’s, which is much higher than the pressures usually foundin pressure ulcer research.18,110,140 Therefore, the results from Kato et al.87 do not pro-vide definite proof that the Na+/K+ pump is unimpaired when intramuscular pressuresare increased to kPa’s, but it is rather likely. Friedrich et al.’s54 results do not evenshow changes at pressures as high as 10 MPa, indicating that the increased hydrostaticpressure occurring in skeletal muscles at the onset of pressure ulcers will probably notcause any disturbance of ion conductance across the cell membrane.It has also been reported that the membrane lipid bilayer is almost volumetrically incom-pressible, and will not change its density under hydrostatic pressures up to 10 MPa.70
The area of the bilayer is at least 10-fold more compressible, and thus when the areachanges, this will always be accompanied by a proportional change in membrane thick-ness to maintain a constant volume. But expansion of the area by more than 2-4% willalready lead to membrane rupture, since additional space between the polar head groupsof the lipids allows more water between the hydrophobic lipid tails, destabilizing thebilayer.70
Deformation of cell membranes could well be more harmful than pure hydrostatic pres-sures. Vlahakis et al.185 already found wounded alveolar epithelial cells, i.e. plasmamembrane breaks, at a dynamic membrane strain amplitude of only 9%. They alsofound evidence for protection through a mechanism called deformation-induced lipidtrafficking, meaning lipid transport to and insertion into the plasma membrane. Bothincreased and decreased cytoskeletal stiffness impaired this mechanism, and hence in-
29

Cellular deformation Skeletal muscle cells
creased the probability of membrane breaks.
But membrane disruptions are very common in skeletal myocytes, and are normallyrapidly resealed by Ca2+-dependent fusion of intracellular vesicles with the cell mem-brane.5,127,185 In dystrophic myotubes, lack of dystrophin which connects ecm andcytoskeleton, leads to more frequent cell membrane disruptions during contractions.5
Resealing leads to the incorporation of vesicles with Ca2+ leak channels. The highsubsarcolemmal Ca2+ concentration activates calpains, which hydrolyze the Ca2+ leakchannels. This seems to be necessary for their long-lasting activity, and leads to moreand more Ca2+ influx.5
Constantin et al.38 found no global cellular Ca2+ overload after inhibition of actin fila-ment assembly, suggesting that these cytoskeletal filaments, which connect the contractileproteins to the ecm via dystrophin among others, are not important for Ca2+ homeosta-sis. But their results do not rule out local, restricted Ca2+ accumulations at particularsubcellular sites such as the subsarcolemmal area for example.38
Because Ca2+ is involved in the regulation of a wide variety of processes in the cell,including harmful ones, [Ca2+]i elevation due to membrane ruptures could contributeto damage. Prolonged mechanical deformation might increase membrane rupture fre-quency, initiating the above mentioned Ca2+ leakage into the cell.
Gonzalez-Serratos et al.60 investigated the healing of mechanical injuries in isolatedfrog skeletal muscles. Membrane rupture was produced by applying negative pressureto it through a glass micropipette. They found that when the bathing solution was sup-plemented with phosphatidylcholine, the most abundant membrane phospholipid, largerinjuries could be healed. Removing Ca2+ from the bathing solution prevented this heal-ing, possibly because it is necessary for adhesion and fusion of phospholipid vesicles.Healing did not occur with too low concentrations of phosphatidylcholine, or too largeinjuries.Another interesting finding was that the sarcolemma of unloaded skeletal muscles seemedto be more susceptible to mechanical load-induced wounding than the sarcolemma ofnormal muscle.33 Healthy men were subjected to 14 days of bed rest, and half of themexercised their legs every other day. The non-exercising group showed reduced levels ofmuscle type CK after 14 days compared to pre-bed rest levels, indicating that the con-stitutive membrane wounding had decreased. This decreased wounding can also explainthe decreased levels of fibroblast growth factor (FGF), for which mechanical membranedamage had previously been shown to be an efficient release mechanism. This in turnmay explain the atrophy found in these muscles, and not in the muscles of the exercisingmen, whose serum FGF levels were higher than before the bed rest period.In this exercising group, there was also an increase in CK compared to pre-bed rest levels,and this was even much larger than that of ambulatory men doing the same exercises,leading to the conclusion that bed rest increases the susceptibility to membrane injury.
6.2 Skeletal muscle cells
Bouten et al.18 compressed C2C12 mouse skeletal myoblasts and myotubes seeded inagarose, and determined deformations of single cells. The ratio of the diameters of the
30

Cellular deformation Skeletal muscle cells
cell parallel and perpendicular to the compression axis (deformation index) decreasedsignificantly as strain increased to 20% and 40%. Also, membrane buckling, which couldbe precursory to membrane rupture, was observed at strains of 30-40% for myoblasts,and at strains of only 20% for spherical myotubes. Since oxygen and nutrient supplieswere equal in strained and unstrained constructs, the fall in viability over time at 20%strain, supports the hypothesized role for cellular deformation in the initiation of da-mage.It would be interesting to know if there is a relationship between the amount of de-formation and the extent of damage. However, Bouten et al.18 only assessed damageduring 20% strain, and despite a significant difference between myoblast and myotubedeformation indices and membrane buckling at this strain level, there was no differencein damage evolution between these 2 subpopulations.Wang et al.189 performed compression experiments on similar constructs, but they triedto increase the number of myotubes. Applying a gross compression of 10% did not leadto significantly elevated numbers of damaged/dead cells, except after 4 and 12 hours.But 20% straining did induce a significant difference between strained and unstrainedconstructs, which increased over time. After 12 hours of straining, a maximum percent-age of damage/dead cells was reached of approximately 75%.Myotubes seemed to be specifically sensitive to compression, since the viability of spher-ical myotubes was only slightly above 10%, and that of elongated myotubes was zerowithin 1 hour of compression.Direct application of these results to the in vivo situation is difficult, since the amount ofmyotubes was small, while cells in real skeletal muscle tissue are all elongated, and theyhad no cross-striations18. Furthermore, extracellular matrix, which probably influencesthe cytoskeletal integrity, was absent from the cultures.18
Breuls et al.21 compressed tissue-engineered skeletal muscle constructs with more elon-gated myotubes, which were embedded in a collagen/matrigel mixture. They found that30% and 50% straining led to a decreasing viability with time, with steepness and onsetof the decline dependent on the level of straining (figure 6.1).
Figure 6.1: Percentage dead cells as a function of time: The extent of the damage is dependenton time and the level of compression.20
31

Cellular deformation Skeletal muscle cells
The absence of a damage gradient from the center of the indentor to the periphery, theabsence of increased damage in constructs with the indentor just resting on them withoutfurther compression, and the fact that propidium iodide could still diffuse to damagedcells beneath the indentor, made them suggest that prolonged cell deformation provokedthe damage, and not nutrient shortage.
Peeters et al.142 compressed single C2C12 mouse skeletal myoblast cells with a micro-indenter, and visualized the cells with a confocal laser scanning microscope. The surfacearea of the cells increased significantly to a maximum of around 150% of its initial valueat 45% compression, while the volume of the cell remained fairly constant. The im-ages show that the cells predominantly deform perpendicular to their long axis (figure6.2(a)), which coincides with the direction of the actin filaments (figure 6.2(b)). Theseactin stress fibers form connections between focal adhesion points and the cell interior,and provide a large part of the resistance against deformation.143,163
(a) (b)
Figure 6.2: (a) Confocal microscopy images of a cell for different indentations. It can be seen thatthe cell diameter increases more perpendicular to its long axis (I2) than along this axis (I1).142
(b) Actin fibers in C2C12 mouse skeletal muscle cells.142
The lower right image in figure 6.2(a) shows a disrupted cell membrane at a compressionlevel of more than 50%. Therefore, Peeters et al.142 omitted compression levels of morethan 50% from their analyses, though this deformation level will be particularly impor-tant in a deformation damage analysis. It is also interesting to note that the volumetended to increase at this level of compression, although the change was not yet signifi-cant.With regard to pressure ulcers, the timescale at which Peeters et al.142 worked is far toosmall, being only a few minutes. Repeating the experiments on a timescale of hours islikely to change the outcome, since the cells have time to reestablish a steady state.
32

Cellular deformation Skeletal muscle tissue
6.3 Skeletal muscle tissue
Bosboom et al.16 compared MRI-assessed muscle damage in a rat subjected to pressureapplication with maximum shear strain distributions predicted with FE simulations.Possibly due to modelling uncertainties, the locations of muscle damage and highestshear strains did not really show much overlap.At this university, compression experiments are conducted on rat hindlimb muscles inwhich damage evolution is monitored with MRI. Preliminary results from comparison ofdamage locations with sites of high maximal shear strains in a dedicated FE model ofthe rat hindlimb, show a promising correlation.40
33

Chapter 7
Cell death
Having discussed the damage-initiating processes that are probably involved in the evo-lution of pressure ulcers, this chapter deals with the ensuing pathway to cell death.
7.1 Apoptosis and necrosis
Cell death can occur either in a slow, organized way, which is called programmed celldeath or apoptosis, or in a rapid, uncontrolled way, termed necrosis. The term secondarynecrosis is sometimes also used to describe the final stage of apoptosis.Recently however, evidence emerged that apoptosis and necrosis have some overlap195,and that necrosis may also be a programmed form of cell death occurring in pathologicalas well as in physiological conditions.8,113,148
Apoptosis and necrosis can occur at the same time in one tissue, having similar signalsand initial mechanisms.107,148 The intensity of the insult and the intracellular amountof ATP may be critical in selecting the cell death pathway.68,107,196 Several studies haveeven reported simultaneously occurring apoptotic and necrotic characteristics in one cell,termed hybrid cell death.148,195
7.1.1 Apoptosis
Apoptosis can occur in single cells surrounded by healthy neighbors. Characteristicsof apoptotic cells are cell shrinkage, DNA condensation and fragmentation, and main-tenance of organelle integrity.8 The cell membrane remains largely intact, but phos-phatidylserine is translocated to the outer leaflet to make apoptotic cells recognizableby macrophages. Finally, cell membrane blebbing occurs, an active process thoughtto be driven by contractile forces generated by the actin-myosin filaments37, and thecell fragments into smaller parts, termed apoptotic bodies, which are phagocytozed bymacrophages.37,63,88 How much apoptosis contributes to pressure ulcer formation re-mains a question, since apoptotic cells are normally orderly removed.However, this neat way of cell death requires energy. Therefore, apoptosis cannot occurwhen cells are deprived of both oxygen and glucose.25,88,107 But Leist et al.107 found
34

Cell death Apoptosis and necrosis
that supply of only glucose, allowing anaerobic glycolytic ATP generation, was alreadysufficient to execute apoptosis.After an insult that does not deplete the cell’s energy, apoptosis is activated either extrin-sically or intrinsically. In the first case, an external signal induces receptor aggregation inthe cell membrane, forming a death-inducing signalling complex (DISC).11 The intrinsicpathway is activated by an apoptotic stimulus inside the cell.11
Intrinsic pathwayIn the intrinsic, or mitochondrial pathway (figure 7.1), Ca2+, NO·, reactive oxygen species(ROS), fatty acids, or caspase activation can trigger the release of harmful molecules fromthe mitochondria into the cytosol.8,25,88,106 This is mediated by pro-apoptotic Bcl-2 fam-ily proteins, e.g. Bax or Bak, and can be inhibited by anti-apoptotic Bcl-2 proteins.25,153
Figure 7.1: The extrinsic, intrinsic, and endoplasmic reticulum stress pathways for apoptosis:In the extrinsic pathway, coupling of FasL or TNFα to their respective receptors Fas or TNFRrecruits adaptor proteins FADD or TRADD, leading to activation of caspase-8. This caspase inturn activates either caspase-3 or Bid. Activated Bid (tBid) triggers the release of several noxioussubstances from the mitochondria, mediated by Bax. A disturbed environment is the stimulus forthe intrinsic apoptotic pathway, also leading to a loss of mitochondrial membrane integrity. Inthe cytosol, cytochrome c, APAF-1, procaspase-9 and dATP form the apoptosome, which alsoleads to activation of procaspase-3 or -7.11 Disturbed functioning of the e.r. leads to activation ofcaspase-12 with the help of Bax/Bak. The activated caspase-12 in turn stimulates the conversionof procaspase-9 to caspase-9.136 (filled arrows mean stimulation; thick perpendicular bars meaninhibition; large red oval in the middle represents mitochondria; bottom left green oval representsnuclei; bottom right orange shape represents sarcoplasmic reticulum; curved blue line on the rightrepresents the sarcolemma)
35

Cell death Apoptosis and necrosis
The loss of mitochondrial membrane integrity implicates the opening of the permeabilitytransition pore (PTP)11,48,153, consisting of the voltage dependent anion channel (VDAC)in the outer mitochondrial membrane, ANT in the inner membrane, and cyclophilin Din the mitochondrial matrix. Together, these molecules form a non-specific ion channel,permitting the passage of molecules up to 1500 Da.153,168
Fontaine et al.53 found that PTP opening was directly dependent on the electron fluxthrough complex I of the respiratory chain, and the transmembrane proton gradient inskeletal muscle mitochondria. The oxidation-reduction state of NAD+ did not affect thethe PTP opening, nor did the generation of H2O2.
PTP opening causes the release of cytochrome c25,45,53,88,153,168, procaspase-9153 andapoptosis protease activating factor-1 (APAF-1)11. Together with dATP, these moleculesform an apoptosome.11,45,153 This complex activates effector caspase-7136,198, or caspase-3, responsible for DNA fragmentation41,45,133, protein degradation106, and cell membranetransformation to facilitate recognition by macrophages88 (figure 7.1). It also inhibitsPARP, which is stimulated by DNA damage to repair it, but concomitantly depletesATP (appendix B).145
Smac/Diablo (second mitochondrial activator of caspases / direct IAP-binding proteinwith low pI)45,153,168, apoptosis inducing factor (AIF)45,53,153,168, and Omi/HtrA2153,168
are also released from the mitochondrial intermembrane space, all of which promoteapoptosis (appendix B).Another result of PTP opening is an influx of protons into the mitochondria, causing adisturbance of oxidative phosphorylation resulting in ATP depletion.53,153,168 This im-plies that PTP opening is not restricted to the apoptotic cell death pathway, because ifthe ATP level falls below a critical value, necrotic cell death ensues.153
The influx of protons also leads to mitochondrial swelling and disruption of the outermitochondrial membrane, allowing further leakage of molecules from the intermembranespace. Some of the signalling molecules playing a role in the apoptosis pathway, arebriefly discussed in appendix B.
Extrinsic pathwayIn the extrinsic pathway, a death ligand (e.g. FasL or TNFα) binds to its receptor(Fas (CD95) or TNFR) on the cell membrane and subsequently promotes the assemblyand activation of the death-inducing signalling complex (DISC) (figure 7.1).10,25,88,153
This occurs with the help of adaptor proteins (FADD or TRADD), which are also in-volved in the subsequent activation of caspase-8.25 Caspase-8 in turn causes cleavageof pro-apoptotic Bid resulting in the active tBid, or it can directly activate caspase-310,25,106,124,153.tBid can activate Bax and Bak106,168, which insert into the mitochondrial outer mem-brane.198 In the presence of these pro-apoptotic Bcl-2 family members, tBid inducesPTP-opening, permitting cross-talk between the intrinsic and extrinsic pathway.106,168
Endoplasmic reticulum stress pathwayCa2+ depletion from the endoplasmic reticulum (e.r., also called sarcoplasmic reticulum(s.r.) in skeletal muscle cells) is one of the stimuli that can disturb e.r. function, andlead to e.r. stress.198 The result is activation of Bax or Bak on the e.r. and subsequentactivation of caspase-12 and further e.r. Ca2+ depletion.136,137 Caspase-12 in turn, canactivate caspase-9 (figure 7.1).136
36

Cell death Hypoxia and cell death
Morishima et al.136 found that the mitochondrial transmembrane potential did notchange during this e.r. stress pathway of apoptosis, and no cytochrome c was releasedinto the cytoplasm, indicating that mitochondrial damage was absent.
It should be noted that some of the above mentioned processes may be specific to certaincell types, and contradictory experimental findings exist.24,25,132 For example, Burgesset al.27 found no APAF-1 in human skeletal muscle cytosols. As a result, no functionalapoptosome could be formed to activate pro-caspases-3 and -9, which they did find inthe cytosols. On the other hand, Dirks et al.45 did find APAF-1 in rat skeletal musclecells.A complicating factor in skeletal muscle cells is that they are multi-nucleated, and thatit is possible that only one or a few of a fiber’s nuclei are apoptotic.180 De Torres et al.180
also found that the cytoplasm was only degenerating in the vicinity of such apoptoticnuclei, while it was completely healthy in the rest of the cell. The relation between thenumber of apoptotic nuclei and the integrity and function of the complete cell is notknown.165
7.1.2 Necrosis
Necrosis can occur in response to the same stimuli as apoptosis, but it will occur whenthe stimuli are stronger and the cell is not in control anymore.148 It was shown forexample that Fas receptors were involved not only in caspase-dependent apoptosis butalso in caspase-independent necrosis (figure 7.2).148 Bcl-2, Bcl-XL (appendix B) andcaspases also modulate apoptosis as well as necrosis, although the exact mechanism isstill unclear.148,169 Mitochondria, being the major ATP sources in the cell, generatorsof ROS, and release sites of several apoptogenic/necrogenic factors, may also promotenecrosis or apoptosis, depending on the interplay between all these factors.148
A rapid depletion of ATP forces the cell into necrosis since apoptosis is an energy-consuming process. As a result of the lack of ATP, ionic gradients across the cell mem-brane will be lost because active pumping is no longer possible. Cytoplasmic swelling anddisruption of the plasma membrane occur, and organelles are destructed. Intracellularcontents are released and an inflammatory reaction ensues. This is a fast type of celldeath and usually affects multiple cells.8,190
Necrosis is further characterized by pyknotic nuclei (condensed nuclear contents), andrandom DNA degradation in contrast to the oligonucleosome fragments from apoptoticcells that form a ladder pattern on agarose gels.68,148 Another discriminating event be-tween apoptosis and necrosis is loss of integrity of the cell membrane, which does notoccur early in apoptosis to a large extent, while it does in necrosis. Caspase-dependentcleavage and subsequent inactivation of cytosolic Ca2+-dependent phospholipase A2(cPLA2) might be responsible for this difference.148
7.2 Hypoxia and cell death
IonsHypoxia disturbs cell homeostasis and hence may lead to cell damage or death (figure
37

Cell death Hypoxia and cell death
Figure 7.2: Hypothetical sequence of events leading to necrosis: Cytokines binding to death recep-tors, ischemia, oxidative stress and extensive DNA damage can all activate stress kinases, settinginto motion a cascade of harmful events that ultimately lead to cell membrane permeabilization.148
7.3). ATP shortage resulting from a decreased rate of oxidative phosphorylation is oneof the consequences of hypoxia that may initiate this damage. The compensatory in-crease in glycolytic metabolism decreases the pH, which can also trigger cell death.190
The increased concentration of H+ in the cell prompts Na+/H+ exchange, leading to anincrease in Na+ in the cell. This in turn stimulates Na+/Ca2+ exchange, increasing theintracellular Ca2+ concentration, setting into motion a lot of harmful processes (section7.3).190
ROSParadoxically, hypoxia may also result in oxidative stress. The explanation is an elevatedproduction of ROS because of a lack of final electron acceptors in the ETC.11,32,41,103,105,108,132
McClintock et al.124 indeed found that a functional ETC was essential to initiate signalsthat regulate Bax/Bak to induce apoptosis after oxygen deprivation. Similarly, Chandelet al.30 reported that hypoxia failed to increase ROS production in cells without mito-chondrial DNA and a functional ETC.Alternative ways of generating ROS or RNS in hypoxia are activation of XO caused bythe metabolic stress a cell experiences when deprived of oxygen105 (section 4.1.2), andinduction of mitochondrial NOS103. It has to be stressed though, that these mechanismsrequire oxygen, and therefore cannot take place in anoxia.
HIF-1The response to hypoxia also involves transcription factors, such as activator protein-1(AP-1), nuclear factor-κB, and hypoxia-inducible factor-1 (HIF-1), to try to avoid severecell damage. HIF-1 is the most potent one, and is thought to be important in the generaloxygen homeostasis. Subunit HIF-1α is constitutively expressed, but its degradation isprevented in hypoxia through a PI-3K/Akt pathway (appendix B), resulting in increasedHIF-1α levels.132 Full activation of HIF-1 further necessitates suitable redox conditions,several coactivators and phosphorylation. Phosphorylation is probably carried out by
38

Cell death Hypoxia and cell death
Figure 7.3: The points at which hypoxia affects the damage pathways in the cell. (filled arrowsmean stimulation; thick perpendicular bars mean inhibition; large red oval in the middle repre-sents mitochondria; bottom left green oval represents nuclei; bottom right orange shape representsendoplasmic reticulum)
the ERK pathway (appendix B), which can be activated by mitochondrial ROS, influxof Ca2+, vascular endothelial growth factor (VEGF) or certain other growth factors, orNADPH oxidase.The result of HIF-1 transcriptional activity is enhanced expression of glycolytic en-zymes166, to increase the anaerobic ATP production, and VEGF, which stimulates neo-vascularization.132 The severity of the insult, and the extent to which a cell is able toadapt, determine whether a cell dies or survives.
MetabolismHypoxia stimulates glycolysis to compensate for the decreased rates of oxidative phos-phorylation. Malhotra et al.121 concluded that glycolysis was essential for the glucose-mediated protection against cytochrome c translocation, and cleavage and inactivationof PARP.
39

Cell death Ions and cell death
Furthermore, hypoxia induces glucose uptake through increasing the number of glucosetransporters.109 This protects against hypoxia-induced cell death, at least in vascularsmooth muscle cells, although no difference was found in ATP levels between cells over-expressing GLUT-1 and control cells during hypoxia.109
The TCA cycle and the ETC are also affected by hypoxia. Incubation of rat skeletalmuscle cells in hypoxia resulted in a decrease in several enzymes of this cycle, as well as incytochrome c oxidase from the ETC, without a change in the number of mitochondria.108
ApoptosisAccording to LeBlanc106, hypoxia might also induce the expression of proteins called in-hibitors of apoptosis (IAP)106 to avoid cell death. However, de Moissac et al.133 showeda three-fold increase in the number of apoptotic cardiac myocytes, a significant increasein active caspase-3 and cytosolic cytochrome c levels after only 1 hour of hypoxia (pO2
< 33mmHg (4.4 kPa)). This is confirmed by McClintock et al.124 who concluded froman oxygen deprivation-induced increase in cytochrome c and caspase-9 that apoptosis isexecuted via the intrinsic mitochondrial pathway under these conditions, and Brunelleet al.25, who report that fibroblasts lacking Bid, a key factor in the extrinsic apoptoticpathway (figure 7.1), still underwent apoptosis.However, Webster et al.190 indicated that hypoxia in itself was not a potent stimulatorof apoptosis in cardiac myocytes, while acidosis was, even in the absence of hypoxia.Replacement of the medium of cells subjected to hypoxia led to a clear decrease in theamount of apoptosis in comparison with a situation in which waste products, in particularprotons, accumulated in the medium.
7.3 Ions and cell death
Changes in the delicate balance between intracellular and extracellular ion concentra-tions may mediate or modify apoptosis or necrosis (figure 7.4).195,196 Necrosis is inducedupon severe loss of transmembrane ionic gradients leading to cell swelling and loss ofmembrane integrity.190
Ca2+
Lack of ATP results in decreased activity of the Ca2+ ATPase in the sarcolemma ande.r. membrane, as well as of the sarcolemmal Na+/K+ ATPase. A consequence of theformer ATPase inhibition is an increased intracellular Ca2+ concentration ([Ca2+]i), anda decreased Ca2+ concentration in the e.r., impairing proper protein synthesis.196
Slowing the latter ATPase decreases [K+]i, and increases [Na+]i, dissipating the steepNa+ gradient. This means that the driving force for the Na+/Ca2+ exchanger has dis-appeared, and that this exchange is impaired.15 Inhibition of the Na+/K+ pump alsoleads to depolarization of the cell membrane because of a net influx of cations, with con-comitant opening of voltage-dependent Ca2+ channels.15,135,190 Both these effects leadto a further increased [Ca2+]i (figure 7.4). The elevated [Na+]i also impairs Na+/H+
exchange, lowering the pH.135
Oxidative or nitrosative stress-induced damage to the e.r. membrane can also contributeto the unsettling of calcium homeostasis, as well as age-related mitochondrial dysfunc-tion and the accompanying inability to sequester cytosolic calcium.45
40

Cell death Ions and cell death
Figure 7.4: Role of ions in initiating cell damage: When the ATP level falls, ion pumps in thecell membrane can no longer function properly. A decrease in the Na+/K+ ATPase activityleads to an increased [Na+]i, and a decreased [K+]i. Diminished functioning of Ca2+ ATPaseresults in intracellular Ca2+ accumulation. All these changes in ionic concentrations have a lotof consequences for the cell. (filled arrows mean stimulation; large red oval in the middle repre-sents mitochondria; bottom left green oval represents nuclei; bottom right orange shape representsendoplasmic reticulum; curved blue line at the top represents the sarcolemma)
41

Cell death Ions and cell death
When intracellular Ca2+ levels are elevated, Ca2+ can be removed by pumping it outof the cell or into the endoplasmic reticulum, if ATP levels are sufficient and pumpsintact.145,181 Buffering by functional mitochondria is also an option, but excessive accu-mulation impairs oxidative phosphorylation, promotes the production of reactive oxygenspecies via the electron transport chain, and leads to the release of cytochrome c due toan increased permeability of the outer mitochondrial membrane.45 Mitochondrial volumecan no longer be controlled due to altered mitochondrial membranes.68
It was also reported that an elevated [Ca2+]i can contribute to increased susceptibilityto apoptosis via calpain-mediated caspase-12 activation and Bcl-XL inactivation.137
Another effect of increased Ca2+ concentration in the cell, is the activation of Ca2+-sensitive DNAses, proteases and phospholipases. Studies on the effects of venom phos-pholipases A2 on skeletal muscle report that focal disruption of the cell membrane leadsto a rapid efflux of CK, LDH, aspartate aminotransferase, myoglobin and creatine, anddepolarization of the membrane. The leakiness of the membrane also causes a rapid,large, and very harmful additional calcium influx leading among others to hypercontrac-tion, which in turn may promote further membrane damage through a mechanical effect.Ca2+-dependent activation of intracellular phospholipases induces or aggravates alreadyexisting membrane damage to all intracellular organelles.68
The activation of several Ca2+-dependent proteinases (mostly calpains) may degradeessential cytoskeletal proteins68, or convert XD into XO, which promotes superoxidegeneration (figure 7.5). Nitric oxide production is also stimulated by Ca2+, via stimula-tion of NOS (figure 7.5). Together, O2·− and NO· can react to form the very reactiveperoxynitrite (section 7.5).154 Both superoxide and peroxynitrite can be converted tothe hydroxyl radical (·OH).145
Sensitivity of muscle cells to Ca2+ accumulation could seem strange in view of the factthat Ca2+ levels are enormously elevated during contractions. But in that case, mostCa2+ will be bound to troponin to release the inhibition of formation of cross-bridgesbetween actin and myosin filaments.
K+
Increased ROS production can further impair Na+/K+ ATPase in the cell membrane.Because K+ is the predominant ion in the cell, loss of this ion from the cell might beimportant in apoptotic cell shrinkage.196 It has indeed been implicated in apoptosis inseveral cell types (although not in skeletal muscle cells).195 [K+]i falls in apoptotic cells,and is possibly associated with facilitation of caspase and nuclease activation, as well aschromatin condensation, DNA fragmentation, cytochrome c release, and mitochondrialdysfunction.195,196
Cl−
Changes in Cl− concentrations have also been associated with apoptosis. An elevationof extracellular Cl− was found to inhibit DNA fragmentation and apoptosis,196 possiblythrough cell volume reduction. Maeno et al.119 showed that cell shrinkage precededstaurosporine-induced apoptotic events like cytochrome c release, caspase-3 activation,and DNA laddering in several cell types although they did not use muscle cells. Fur-thermore, administering blockers of Cl− or K+ channels, thereby averting cell volumedecreases, prevented apoptosis, and they did indeed find that [Cl−]i was decreased inapoptotic cells.
42

Cell death Reactive oxygen species and cell death
7.4 Reactive oxygen species and cell death
The intracellular milieu is normally highly reducing, with more than 95% of the glu-tathione in the reduced form (GSH). When ROS are abundant, a large amount of GSHwill be in the oxidized form GSSG. However, in an oxidizing intracellular environment,caspases are inactivated, so apoptosis cannot occur.41 The redox state of the cell alsoinfluences the binding of several transcription factors that are thought to play a role inapoptosis, such as p53, AP-1 and NFκB.41,83
Besides being capable of destructing proteins and DNA, ROS and free radicals can alsoinitiate lipid peroxidation.59 They attack a polyunsaturated fatty acid, which then be-comes a carbon radical species setting into motion a chain reaction, generating moreand more harmful radicals that can continue the process of lipid peroxidation or attackmembrane proteins, eventually leading to loss of membrane function and disruption.59,182
Loss of membrane function may contribute to both apoptosis and necrosis, but mem-brane disruption implies necrosis.The possibility of ROS to react with nitric oxide and produce peroxynitrite leads to alot of additional harmful effects.
7.5 Reactive nitrogen species and cell death
NO· is a mediator of a lot of physiological processes. It is involved in muscle energeticsthrough stimulating glucose delivery with its vasodilatory effect, and promoting glucoseuptake.154 However, it down-regulates glycolysis24,88,154, inhibits CK154, and modulatesthe ETC and ATP-synthesis as well.24,88,103,154.Some of the actions of nitric oxide depend on its concentration, being anti-apoptotic atlow, physiological concentrations, while promoting cell death at high concentrations.88
Anti-death effectsNO· may prevent apoptosis through the induction of heat shock proteins41,88, or suppres-sion of Bax expression88. Furthermore, NO· can up-regulate the intracellular anti-oxidantsystem88, inhibit cytochrome c release through inhibition of PTP opening23,41, inacti-vate several caspases (caspase-311,41,88,148, caspase-8 and -141), modulate Bcl-2 proteinsto inhibit apoptosis41, and inhibit Ca2+ channels in the sarcoplasmic reticulum154 at lowconcentrations154.The main source of NO· is the vascular endothelium, where it acts as a vasodilator.2 Theearlier mentioned down-regulation of the electron transport chain and ATP synthesis byNO· may serve to have a larger region of well-oxygenated cells. In cells adjacent to ca-pillaries, the highest concentrations of NO· will be found, suppressing the ETC more,and saving oxygen, which can then migrate further away from the capillaries, into thetissue.23,178
Nitric oxide is also thought to be involved in protecting the proper functioning of ox-idative phosphorylation, by protecting the cell against H2O2-induced cytotoxicity23, andthrough suppressing the expression of uncoupling proteins23, which uncouple the electrontransport chain and the ATP generation through dissipation of the proton gradient.Inhibition of lipid peroxidation by NO· through scavenging of peroxyl radicals formedduring lipid peroxidation and capable of spreading the peroxidation, provides protection
43

Cell death Reactive nitrogen species and cell death
against damage to the cell membrane.23,41,59,108
Figure 7.5: Role of reactive oxygen and nitrogen species in cell death: Oxidative phosphorylationis the most important source of reactive oxygen species. The superoxide anion itself may exerta lot of deleterious effects, however, it can also combine with nitric oxide to form the harm-ful peroxynitrite. Nitric oxide itself has both pro-death and anti-death effects, depending on itsconcentration. (filled arrows mean stimulation; large red oval in the middle represents mitochon-dria; bottom left green oval represents nuclei; bottom right orange shape represents endoplasmicreticulum; curved blue line at the right represents the sarcolemma)
44

Cell death Reactive nitrogen species and cell death
Pro-death effectsIn contrast to its role as an anti-oxidant providing protection against ROS and preservingcross-bridge function at physiological levels, at high intracellular levels, NO· acts as anoxidizing agent.154 At moderate levels, inhibition of the electron transport chain by NO·leads to increased ETC-derived superoxide.148,154 At still higher levels, NO· reacts withthese superoxide molecules to form peroxynitrite.23,154
Among the other harmful effects of peroxynitrite are damage to proteins, cell membrane(lipid peroxidation193), endothelium, and nucleic acids, thereby activating PARP.145 Itcan decrease the GSH concentration in the cell and disturb the anti-oxidant system88,or stimulate the leakage of protons from mitochondria and interfere with the couplingbetween oxidative phosphorylation and ATP synthesis.23
Through stimulation of several Ca2+ channels, or activation of the e.r. stress response,NO· induces an increase in [Ca2+]i, leading to the effects discussed in section 7.3.35,41,154
Peroxynitrite as well as nitric oxide can also stimulate PTP-opening, and cytochrome crelease(figure 7.5), initiating the mitochondrial apoptotic pathway.103
NO· can also activate caspases, stimulate mitochondrial phospholipid oxidation, up-regulate pro-apoptotic gene expression, transcription factors such as NFκB, apoptosis-inducing ligands like FasL, and pro-apoptotic proteins like Bax, and down-regulate anti-apoptotic proteins.154
45

Chapter 8
Existing theoretical models
This chapter describes some of the existing models concerning metabolism, homeostasis,or tissue damage due to hypoxia, ischemia and reperfusion, impaired lymphatic drainage,or compression.
8.1 Energy metabolism
Ischemia and hypoxiaCabrera et al.28 developed a mathematical model to analyze and quantify the mecha-nisms that control lactate accumulation when oxygen availability to the muscle is low.They defined well-mixed interstitial fluid and tissue compartments, interconnected byan arterial and venous circulation. The tissue compartment was subdivided in muscletissue, splanchnic tissue, lungs and the rest. For each compartment, mass balance equa-tions were written for every metabolite including production, utilization, arterial supplyand venous drainage. Phosphorylation state (ATP/ADP), redox state (NADH/NAD+),and phosphocreatine levels were assumed to be the most important regulators of therates of the various metabolic processes. For oxygen consumption, they assumed simpleMichaelis-Menten kinetics, without regulation by phosphorylation or redox state.Their main finding was that muscle lactate production is very sensitive to muscle oxygenconcentration, while oxygen consumption remained fairly constant over a large range ofoxygen concentrations. Low oxygen concentrations however, lead to large NADH/NAD+
and ADP/ATP ratios, accelerating lactate formation.Again, like Yi et al.194, they did not take into account the subcellular compartmenta-tion of metabolic processes and distribution of metabolites. Another limitation of theirmodel is that it did not include ADP/ATP and NADH/NAD+ regulation of oxidativephosphorylation, and they did not do any simulations with oxygen concentrations lowenough to seriously decrease the oxygen consumption.Salem et al.161 used the model from Cabrera et al.28, and added some additional bio-chemical species and control metabolites. They solely modelled a cardiac compartmentto analyze cardiac energy metabolism under ischemia. The results showed that theNADH/NAD+ ratio increases during a 60% reduction in blood flow, being in part re-sponsible for the decreased pyruvate oxidation and increased pyruvate conversion to
46

Existing theoretical models Disturbed ion homeostasis
lactate. The model was not suitable for a more than 60% reduction in blood flow.Although Salem et al.161 admit that it is important to distinguish between extracellularspace, cytosol, sarcoplasmic reticulum and mitochondria, they did not do this.
Korzeniewski et al.94 made a detailed mathematical model of oxidative phosphoryla-tion alone, and they did include its dependence on ADP levels in contrast to Cabrera etal.28. Their simulations suggest a very strong hyperbolic dependence of ATP synthesison ADP concentration, which was only slightly enhanced increases in Pi concentrations.These Pi concentration changes were due to the incorporation of the CK system.They did not include glycolytic ATP production, nor hydrolysis of ATP to activate glu-cose or fatty acids for further breakdown and ATP generation. When they did this in alater study93 in a relatively simple way, they found that it significantly influenced the ki-netic properties of oxidative phosphorylation. A sudden collapse of oxygen consumptionand phosphorylation state appeared for very low oxidative phosphorylation activities.They suggested that this could be an energetic definition of cell death.
CompartmentationVendelin et al.184 developed a theoretical compartmentalized model for the regulation ofmitochondrial oxygen consumption. They used the FE method to solve reaction-diffusionequations on a 2D mesh consisting of a myofibril, myoplasm (muscle cytoplasm) and amitochondrion. CK and ATPase activity were spatially inhomogeneously distributedalong the myofibril on the basis of Wegman et al.’s experiments191, and they used Ko-rzeniewski’s92 description of oxidative phosphorylation. One of their findings was thatonly after making the diffusion coefficient for ADP 10-fold lower than that in water, the2D model gave different results than a 0D model.But since there is more and more support for limited diffusion due to structural organiza-tion61,89 and the existence of an intracellular convection or perfusion sytem6,77,78,86,192,it would be interesting to include this in the model. Furthermore, their model onlyconsisted of one cell without surroundings or neighbouring cells.
8.2 Disturbed ion homeostasis
Yi et al.194 developed a model to explain the changes in K+ concentrations and intra-cellular volume observed in hypoxia and ischemia in brain and cardiac tissues. Theirmodel consisted of 4 homogeneous compartments, namely damaged cells, damaged ex-tracellular space, a capillary compartment in the damaged region, and a healthy tissueregion. Water movement was made dependent on differences in osmotic pressure, butit was also assumed to be constrained by ecm collagen fibers. K+, Na+ and Cl− fluxeswere described with Hodgkin-Huxley-type currents79 and fluxes through the action ofthe Na+/K+ pump. They made the pump rate dependent on membrane potential and[K+]e and [Na+]i according to a formula from Luo et al.116, which they multiplied bythe ATP availability. For the latter term, they made a fit to experimental data on ATPlevels during ischemia in a dog heart to model ischemia and hypoxia as time-dependentdecreases in Na+/K+ activity.84 Ischemia was further simulated by setting the flow inthe capillary compartment to zero.Their results explained the large increase in intracellular volume during ischemia, and a
47

Existing theoretical models Perfusion
much smaller increase during hypoxia in brain tissue. Failure of the Na+/K+ pump leadsto a large Na+ influx and K+ efflux. Because the pump normally exchanges Na+ and K+
in a 3:2 ratio, the membrane depolarizes, modulating ion conductances, and the osmoticbalance between intra- and extracellular space is changed. The combined effect of thesechanges is cell swelling. In hypoxia however, the increased amount of extracellular K+
is washed away with the capillary flow, partly abolishing the effects seen in ischemia.Yi et al.194 assumed homogeneous compartments, not taking into account any spatialvariations, neither in the degree of ischemia, nor in ion and water transport. Anotherlimitation is that they assumed an ischemic region beforehand, but did not model indi-vidual cell death or spreading of the damage.
Ruppin et al.157 did simulate the propagation of damage from necrotic to healthy tissue.They made a theoretical model to predict the spreading of ischemic damage in braintissue based upon 2 different hypotheses.The first hypothesis was that K+ in the ecm increases as a result of membrane rup-ture or depolarization of necrotic cells. K+ then diffuses through the ecm, and causessurrounding cells to increase their Na+/K+ ATPase activity to reduce the extracellularK+ levels. If however, the energy generation in these surrounding cells is compromiseddue to ischemia, the increased ATPase activity may eventually deplete ATP, and lead tonecrosis.The second hypothesis was that damage would spread due to the release of some toxicsubstance from necrotic cells. This model was largely identical to the other one, exceptthat there are no homeostatic mechanisms for the toxic substance in the ecm, and theintactness of the tissue has changed from being proportional to the metabolic deficiencyto being proportional to the extracellular concentration of the toxic tissue. Despite thesimilarity, different damage propagation patterns were found for the 2 models.
8.3 Perfusion
There are a lot of numerical models describing skeletal muscle perfusion50,57,126,183, andalso many indicating hypoxic regions58,112,117,118,159. But the spatial and temporal evo-lution of damaged cells in a tissue as a result of compromised capillary perfusion has notbeen numerically evaluated as far as I know.We made an attempt at theoretically describing cellular damage due to external pressure-induced ischemia in a 2D representative skeletal muscle volume element.29 Partial cap-illary collapse changed oxygen supply, and when a cell had been hypoxic for too long, itwas assumed dead, increasing the oxygen availability for other cells.Although the FE model did not converge for large deformations, we concluded that thelocalization of capillaries and mitochondria were important for the subcellular oxygendistribution, and the hypoxia-induced cellular damage assessment.
8.4 Lymph flow
Reddy et al.152 developed a mathematical model of flow through the terminal lymphat-ics, in which the anchoring filaments are described as linear springs of which the length
48

Existing theoretical models Deformation
depends on the amount of interstitial fluid. This in turn, is determined by the differencebetween capillary filtration and flow into the terminal lymphatics. Capillary blood pres-sure and protein concentration form the upstream boundary conditions, and pressure inthe adjacent contractile lymphatic segment is the downstream boundary condition.Their results confirm that fluid absorption and flow through the terminal lymphaticsis due to periodic fluctuations in interstitial fluid pressure and suction of the adjacentcontractile lymphatics. Oedema, an accumulation of excess fluid in the interstitium, in-creased the lymph flow.152
Swartz et al.176 also developed a model to study the influence of edema on the me-chanics of lymphatic transport. Their model was a linear poroelastic description ofinterstitial fluid movement including lymphatic drainage. The pressure and fluid veloc-ity distributions were dependent on hydraulic conductivity of the tissue matrix, capillaryfluid reabsorption and lymphatic drainage, and elasticity of the tissue.They used microscopically observed lymph drainage in mice tails to estimate this bulktissue hydraulic conductivity, elasticity and resistance to lymphatic drainage, and theirchanges in mice tails made oedematous.Swelling caused an increase in the conductivity, but this was annihilated by the increaseddistensibility of the matrix, which reduced the driving force for fluid movement so muchthat fluid stagnation occurred.176 This is in contrast to the findings by Reddy et al.152,who reported an increase in lymph flow with oedema.
Both these models however did not consider the effects on tissue viability.
8.5 Deformation
Linder-Ganz et al.110 determined changes in mechanical properties of rat muscles ex-posed to prolonged mechanical loading. After certain combinations of magnitude andduration of pressure, muscle stiffening occurred, and this corresponded to histologicallyobserved necrosis. With an FE model of the rat limb, the determined the correspondinginternal stresses to derive a damage threshold for muscle stiffening.They applied these findings to FE models of human body parts vulnerable to pres-sure sores to analyze changes in stress distributions. In these models, local adaptationof muscle mechanical properties in high stress regions according to the experimentallyderived damage threshold, led to a widening area of high stress, exacerbating the vul-nerability.Although they did conclude that mechanical properties of striated muscle can be used asan indicator for compression injury, they did not prove a relation between the extent andlocalization of necrosis and high stresses in time. Furthermore, the change in stiffnessused locally in the model was derived from a uniaxial tension test of the complete muscle.Since they did not take into consideration muscle structure on the sub-tissue level andprocesses taking place there, they cannot make a distinction between contributions tothe damage from different damage-producing pathways such as ischemia, cellular defor-mation, or impaired lymph drainage.
Breuls et al.22 predicted local cell deformations in skeletal muscle tissue with a mul-
49

Existing theoretical models Deformation
tilevel FE approach. In this way, he was able to combine macroscopic muscle damagewith the damage initiating processes on the microlevel. Macroscopically, an externalpressure was applied to the muscle. Microscopically, this resulted in large differences inindividual cell deformations, which could be much larger than the macroscopic defor-mation. Moreover, the strains in the cells were found to be strongly influenced by themicroscopic architecture, suggesting that indirect mechanical interaction between neigh-bouring cells affects their deformation.22
Figure 8.1: Damage evolution in a mi-crostructure in the form of a pressure ver-sus time curve from the multilevel model ofBreuls20.
Figure 8.2: Experimental allowable exter-nal pressure versus time curves from dif-ferent studies: In the area above the lines,tissue breakdown will occur.20
Breuls20 extended his multilevel model with a damage law which stated that a cell diedwhen its accumulated strain energy density was above a certain critical value. This da-mage law was evaluated by comparing the simulation outcome with the experimentallymeasured accumulation of dead cells in a tissue-engineered in vitro model system (figure6.1).21 He constructed local damage plots that showed the amount of dead cells versustime for several external macroscopic loads. The exact shape and position depend on thelocation in the tissue and the microstructural properties. Combination of these curvesgives a new one with a certain bandwidth, which is determined by the microstructureand cell tolerance (figure 8.1). Breuls20 postulated that a critical damage curve will runsomewhere within this bandwidth, according to the amount of dead cells that corre-sponds to irreversible damage.In the past, there have been more numerical models concerned with tissue pressures,stresses and strains as a result of compression120,140,179,197, most of which tried to repro-duce experimentally observed critical pressure versus time curves without consideringthe underlying cellular processes (figure 8.2).
50

Chapter 9
Discussion
9.1 Summary
In the preceding chapters, the possible consequences of an external pressure on a tis-sue are discussed, with regard to their contributions to pressure ulcer aetiology. Themost adhered hypothesis regarding the development of these ulcers is that the externalcompression causes ischemia, either simply through collapse of capillaries or throughthe vascular waterfall mechanism. The latter mechanism is often used to explain ex-periments simulating the compartment syndrome, when the intramuscular pressure ishomogeneously elevated. This causes closure of the most compliant vessels, the venules,and consequent pressure build-up in the capillaries, decreasing the perfusion pressure.But whatever the mechanism is, ischemia will lead to damage if it lasts too long.Both skeletal muscle cells and vascular endothelial cells can be affected by a lack of oxy-gen. Injury to the latter cells can increase the permeability of the capillaries, hamperreperfusion upon load removal, and when it concerns the lymphatic endothelial cells, itcan impair lymphatic drainage. This might already be impaired due to high hydrostaticpressures in the tissue, and leads to disturbed volume regulation and waste removal,which is also hypothesized to be implicated in the aetiology of pressure ulcers.In all cells, hypoxia can raise the intracellular generation of reactive oxygen species, anddisturb the energy status of the cell. It forces the cell to rely on anaerobic glycolysiswith increased production of waste products and a less efficient ATP production.Ischemia is even worse than hypoxia, because it adds a reduced nutrient supply, andwaste removal to the oxygen lack, forcing the cell to use only endogenous substratesfor energy generation, and accelerating the accumulation of waste products resulting inacidosis.Instead of draining the tissue of all its accumulated waste products and delivering oxygenagain, reperfusion can deteriorate the status of the tissue. When perfusion is restored,inflammatory cells produce reactive oxygen and nitrogen species, but often, the ischemicperiod prevents reperfusion from occurring, and leaves the tissue with an increasing en-ergy shortage. That is why reperfusion is also hypothesized to be implicated in theaetiology of pressure ulcers.One of the consequences of the decreased ATP generation is failure of membrane ionpumps, and ion homeostasis can no longer be maintained. Especially Ca2+ accumula-
51

Discussion Conclusion
tion in the cytosol or mitochondria is very dangerous. It damages the mitochondrialmembrane and disturbs mitochondrial function. In the cytosol, it activates proteases,phospholipases, nucleases, and enzymes that catalyze the formation of reactive oxygenand nitrogen species.These ROS and RNS can initiate severe membrane damage through a process called lipidperoxidation. Besides being produced by the cells in the tissue, invading inflammatorycells during reperfusion add to the amount of ROS and RNS in the tissue. Membraneintegrity can further be compromised by the action of (Ca2+-activated) phospholipases.Obviously, the homeostatic imbalance is aggravated by the membrane disruptions.Too much membrane rupture or a too extensive homeostatic disturbance, both regard-ing redox state and ion concentrations, leads to necrosis. However, when the cell hassome ATP left, and some options to exert still some control over the cell’s destination,apoptosis can be executed. A cascade of caspases is set into motion, finally resulting inphagocytosis of the apoptotic bodies with intact membrane, without spilling of cellularcontents as is the case with necrosis.
However, it is known that pressure ulcers can develop in muscles within their ischemictolerance time. Also, cells can get damaged from deformation alone in the absence ofischemia or hypoxia. This suggests that deformation is somehow directly involved intissue degeneration in pressure ulcer formation.A constitutive level of membrane wounding exists in contracting muscles, with a sealingmechanism consisting of the insertion of intracellular lipid vesicles into the membranebreak, for which Ca2+ is necessary. Interestingly, the sarcolemma of people subjectedto bed rest appeared to be more vulnerable for rupturing when contracting than thatof ambulatory people. Furthermore, the lack of certain components connecting ecm andcytoskeleton also made muscles more sensitive to damage during contractions. In thesestudies, it was also assessed that Ca2+ was involved.The mechanism that leads to a decrease in cell viability when cells are passively deformedis still unsolved however.
9.2 Conclusion
Damage pathways following hypoxia, ischemia or reperfusion are extensively investigated,and a lot of mediating substances have been identified. There are complicated and in-terrelated processes going on in a cell once it starts to lose its homeostatic balance. Atthe cellular level, membrane integrity, ATP and Ca2+ are very important mediators ofinjury. Membrane integrity as well as ATP are discriminative factors between necrosisand apoptosis, and Ca2+ seems to play a pivotal role in the fate of the cell.But hypoxic, ischemic, and reperfusion injury are rather frequently occurring patho-logical processes, while direct deformation damage is more specific for pressure ulcerdevelopment. Till now, to my knowledge, no experiments or theoretical models havebeen published that try to couple deformation to a certain harmful process in the tissueto elucidate a damage pathway. Understanding it however, may not only provide waysfor therapeutic intervention, but also lead to the identification of substances or parame-ters to identify individuals with a high susceptibility for developing pressure ulcers.Therefore, the hypothesis is that pressure ulcer formation cannot be explained by is-
52

Discussion Future plans
chemia or ischemia/reperfusion alone, but that deformation somehow exacerbates thetissue damage. In this project, an attempt will be made to clarify which process is re-sponsible for damage directly related to deformation, and how is this related to the otherpressure ulcer aetiological factors.
9.3 Future plans
To achieve this aim, experimental and theoretical models at different levels of musclearchitecture will be combined.A. Stekelenburg is currently doing rat experiments at our university, in which she putsan indentor on the muscles in the rat hindlimb for 2 hours, and follows perfusion anddamage in time. In the near future, she will repeat these experiments with a cuff aroundthe rat’s thigh to see the difference in damage between a situation with and withoutdeformation of the muscle. MRI tagging experiments will add information about thesites of largest deformation.D. Gawlitta assesses apoptosis and necrosis in tissue engineered (TE) skeletal muscleconstructs, which she either deprives of oxygen, or deforms, or both. She will measurecertain damage markers in time, and compare outcomes in anoxia, compression, andanoxia under compression.Experiments with single cells in the compression device from Peeters142 can give answersto questions about what is going on geometrically in individual cells during prolongeddeformation. The time course of cell volume, cell shape and cell surface area can bemonitored with this set-up.
Since these experiments are performed on different levels, their outcomes cannot becompared easily. With a theoretical multi-level FE model, it will be attempted to applythe experimental results to the pressure ulcer situation, and couple the different levelsof the experiments.
There are a lot of conceivable pathways leading to damage directly due to cellular de-formation. An example is impedance of easy removal of waste products or diffusionof metabolites because of disorganization of the ecm. Deformation may also interferewith the osmotic balance in the tissue because of forced volume changes, and changesin membrane permeability. Another possibility is that deformation causes disruption ofthe connections that exist between ecm, cell membrane, and cytoskeleton, that are im-portant for cell shape and signalling. Cytoskeletal damage may also be the consequenceof pressure on the cells, leading to disorganization of intracellular communication andstability. Damage to intracellular organelles as a consequence of compression may leadto metabolic disturbances. But the hypothesis I want to start with is that deformationcauses membrane rupturing with a concomitant ingress of calcium.The phenomenon of membrane wounding and resealing has been studied quite exten-sively with regard to Duchenne’s muscular dystrophy, which can help to elaborate thishypothesis. Regions of highest strains in the membrane could be assumed to break,causing a calcium influx. Resealing can occur as long as the intracellular pool of phos-pholipids has not been depleted. But insertion of these phospholipid vesicles also insertscalcium channels in the membrane, opened by a local high calcium concentration. Some
53

Discussion Future plans
calcium sequestering may occur by the endoplasmic reticulum, but calcium will proba-bly accumulate and activate phospholipases that will further aggravate the membranedamage, eventually leading to irreversible membrane disintegration, and cell death.Validation of these hypothesized events should come from single cell experiments, prefer-ably compressing cells surrounded by other cells while monitoring cell shape and calciumconcentrations. It would also be very interesting to evaluate the permeability of thecell membranes, both in the undeformed and deformed state. This could possibly bedone with fluorescence recovery after photobleaching (FRAP) experiments. But also thecompression experiments on TE muscle constructs can give valuable information, espe-cially whether apoptosis or necrosis is the most widespread type of cell death followingsustained deformation.If the hypothesis of deformation-induced membrane breaks would be rejected, or provento be insufficient to explain the observed deformation damage, here are some suggestionsfor investigating the other hypotheses. Making a choice for one of them is of coursedependent on possible experimental observations pointing in a certain direction.
To investigate the often adhered hypothesis that ischemia is the main cause of pres-sure ulcers, a FE model of a representative volume element of skeletal muscle cells andthe capillaries between them has already been made. It has to be adapted to make itconverge for large deformations occurring in tissues developing pressure ulcers, to be ableto draw conclusions and make comparisons between the direct effect of deformation andthe indirect ischemic effect.Since previous results from this model already indicated that the subcellular distributionof mitochondria could change the hypoxic cell status, a good implementation of the sub-cellular distributions of some of the metabolic processes and substrates might be veryimportant.Including the ischemic model in the multi-level model from Breuls et al.20 should enablecomparisons between experimental and simulated perfusion patterns and the resultingdamage.
Finally, a combination of both ischemic and deformation damage should be simulatedwith the multi-level FE model. Simply summing the individual contributions of deforma-tion and ischemia to damage, might not be enough to predict the total damage outcome.Instead, deformation might make a cell more sensitive to oxygen shortages, or the otherway round, for example by deformation damage to metabolically important structures,or exacerbation of membrane damage by ischemic reactive oxygen species. In this regard,maintaining or disrupting membrane integrity, and the subcellular structural restrictionsand localizations of energy metabolism, seem to be the most important damage param-eters.The site of damage development at the tissue level is interesting because it could bedifferent for different damage pathways, and comparing the predicted site with the ex-perimentally observed site, could give information about the importance of a particularprocess in the pressure ulcer aetiology.
54

Bibliography
[1] European pressure ulcer advisory panel (1999) guidelines on pressure ulcer treat-ment.
[2] Abela C.B. and Homer-Vanniasinkham S. Clinical implications of ischaemia-reperfusion injury. Pathophysiology, 9:229–240, 2003.
[3] Adams V., Griffin L., Towbin J., Gelb B., Worley K., and McCabe E.R. Porininteraction with hexokinase and glycerol kinase: metabolic microcompartmenta-tion at the outer mitochondrial membrane. Journal of Muscle Research and CellMotility, 45(3), 1991.
[4] Akahane M., Ono H., Ohgushi H., and Tamai S. Viability of ischemia/reperfusedmuscles in rat: a new evaulation method by RNA degradation. Journal of Or-thopaedic Research, 19:559–564, 2001.
[5] Alderton J.M. and Steinhardt R.A. How calcium influx through calcium leakchannels is responsible for the elevated levels of calcium-dependent proteolysis indystrophic myotubes. Trends in Cardiovascular Medicine, 10:268–272, 2000.
[6] Andrienko T., Kuznetsov A.V., Kaambre4 T., Usson Y., Orosco A., Appaix F., Ti-ivel T., Sikk P., Vendelin M., Margreiter R., and Saks V.A. Metabolic consequencesof functional complexes of mitochondria, myofibrils and sarcoplasmic reticulum inmuscle cells. The Journal of Experimental Biology, 206:2059–2072, 2003.
[7] Arthur P.G., Giles J.J., and Wakeford C.M. Protein synthesis during oxygen con-formance and severe hypoxia in the mouse cell line c2c12. Biochimica et BiophysicaActa, 1475:83–89, 2000.
[8] Assuncao Guimaraes C.A. and Linden R. Programmed cell death: Apoptosis andalternative deathstyles. European Journal of Biochemistry, 271:1638–1650, 2004.
[9] Badhwar A., Dungey A.A., Harris K.A., Scott J.A., McCarter S.D., Scott J.R.,Phorbes T.L., and Potter R.F. Limitations in ischemic tolerance in oxidative skele-tal muscle: perfusion vs tissue protection. Journal of Surgical Research, 109:62–67,2003.
[10] Barnhart B.C., Alappat E.C., and Peter M.E. The CD95 type I / type II model.Seminars in immunology, 15:185–193, 2003.
55

BIBLIOGRAPHY BIBLIOGRAPHY
[11] Bisphoric N.H., Andreka P., Slepak T., and Webster K.A. Molecular mechanismsof apoptosis in the cardiac myocyte. Current Opinion in Pharmacology, 1:141–150,2001.
[12] Blaisdell F.W. The pathophysiology of skeletal muscle ischemia and the reperfusionsymdrome: a review. Cardiovascular Surgery, 10(6):620–630, 2002.
[13] Bogoyevitcha M.A., Boehma I., Oakleyc A., Kettermand A.J., and Barr R.K.Targeting the JNK MAPK cascade for inhibition: basic science and therapeuticpotential. Biochimica et Biophysica Acta, 1697:89101, 2004.
[14] Bonhuer J.A., Albadawi H., Patton G.M., and Watkins M.T. A noninvasivemurine model of hindlimb ischemia-reperfusion injury. Journal of Surgucal Re-search, 116:55–63, 2004.
[15] Boron W.F. and Boulpaep E.L. Medical Physiology. Saunders, 2003.
[16] Bosboom E.M.H. Deformation as a trigger for pressure sore related muscle damage.PhD thesis, Eindhoven, University of Technology, 2001.
[17] Bours G.J.J.W., Halfens R.J.G., Abu-Saad H.H., and Grol R.T.P.M. Prevalence,prevention, and treatment of pressure ulcers: descriptive study in 89 institutionsin the netherlands. Research in Nursing & Health, 25:99–110, 2002.
[18] Bouten C.V.C., Knight M.M., Lee D.A., and Bader D.L. Compressive deformationand damage of muscle cell subpopulations in a model system. Annals of BiomedicalEngineering, 29:153–163, 2001.
[19] Brand M.L., Roselino J.E.S., Piccinato C.E., and Cherri J. Mitochondiral alter-ations in skeletal muscle submitted to total ischemia. Journal of Surgical Research,110:235–240, 2003.
[20] Breuls R.G.M. Experimental and theoretical analyses of compression inducedmuscle damage: Aetiological factors in pressure ulcers. PhD thesis, Eindhoven,University of Technology, 2003.
[21] Breuls R.G.M., Bouten C.V.C., Oomens C.W.J., Bader D.L., and Baaijens F.P.T.Compression induced cell damage in engineered muscle tissue: An in vitro modelto study pressure ulcer aetiology. Annals of Biomedical Engineering, 31:1357–1364,2003.
[22] Breuls R.G.M., Sengers B.G., Oomens C.W.J., Bouten C.V.C., and Baaijens F.P.T.Predicting local cell deformations in engineered tissue constructs: a multilevel finiteelement approach. Journal of Biomechanical Engineering, 124:198–207, 2002.
[23] Brookes P.S., Levonen A-L., Shiva S., Sharti P., and Darley-Usmar V.M. Mito-chondria: regulators of signal transduction by reactive oxygen and nitrogen species.Free Radical Biology and Medicine, 33(6):755–764, 2002.
[24] Brown G.C. and Borutaite V. Nitric oxide inhibition of mitochondrial respirationand its role in cell death. Free Radical Biology and Medicine, 33(11):1440–1450,2002.
56

BIBLIOGRAPHY BIBLIOGRAPHY
[25] Brunelle J.K. and Chandel N.S. Oxygen deprivation induced cell death: An update.Apoptosis, 7:475–482, 2002.
[26] Brunori M. Nitric oxide moves myoglobin centre stage. Trends in BiochemicalSciences, 26(4):209–210, 2001.
[27] Burgess D.H., Svensson M., Dandrea T., Gronlund K., Hammarquist F., and Cotg-reave I.A. Human skeletal muscle cytosols are refractory to cytochrome c-dependentactivation of type-II caspases and lack APAF-1. Cell Death and Differentiation,6:256–261, 1999.
[28] Cabrera M.E., Saidel G.M., and Kalhan S.C. Role of O2 in regulation of lactatedynamics during hypoxia: mathematical model and analysis. Annals of BiomedicalEngineering, 26:1–27, 1998.
[29] Ceelen K.K. and Oomens C.W.J. Theoretical analysis of the role of ischemia inthe aetiology of deep pressure ulcers. internal report, February 2004.
[30] Chandel N.S., McClintock D.S., Feliciano C.E., Wood T.M., melendez J.A., Ro-driguez A.M., and Schumacker P.T. Reactive oxygen species generated at mito-chondrial complex III stabilize hypoxia-inducible factor-1α during hypoxia. TheJournal of Biological Chemistry, 275(33):25130–25138, 2000.
[31] Chang W.L. and Seireg A.A. Prediction of ulcer formation on the skin. MedicalHypotheses, 53(2):141–144, 1999.
[32] Clanton T.L., Zuo L., and Klawitter P. Oxidants and skeletal muscle function:physiologic and pathophysiologic implications. P.S.E.B.M. (Experimental Biologyand Medicine), 222:253–262, 1999.
[33] Clarke M.S.F., bamman M.M., and Feeback D.L. Bed rest decreases mechanicallyinduced myofiber wounding and consequent wound-mediated FGF release. Journalof Applied Physiology, 85(2):593–600, 1998.
[34] Claus-Walker J., DiFerrante N., Halstead L.S., and Tavella D. Connective tissueturnover in quadriplegia. American Journal of Physiology and Medical Rehabilita-tion, 61:130–140, 1982.
[35] Clementi E. Role of nitric oxide and its intracellular signalling pathways in thecontrol of Ca2+ homeostasis. Biochemical Pharmacology, 55:713–718, 1998.
[36] Coleman M.L. and Olson M.F. Rho GTPase signalling pathways in the morpholog-ical changes associated with apoptosis. Cell Death and Differentiation, 9(5):493–504, 2002.
[37] Coleman M.L., Sahai E.A., Yeo M., Bosch M., A. Dewar, and Olson M.F.Membrane blebbing during apoptosis results from caspase-mediated activation ofROCK − 1. Nature Cell Biology, 3:339–345, 2001.
[38] Constantin B., Imbert N., Besse C., Cognard C., and Raymond G. Cultured ratskeletal muscle cells treated with cytochalasin exhibit normal dystrophin expressionand intracellular free calcium control. Biology of the Cell, 85:125–135, 1995.
57

BIBLIOGRAPHY BIBLIOGRAPHY
[39] Cowled P.A., Leonardos L., Millard S.H., and Fitridge R.A. Apoptotic cell deathmakes a minor contribution to reperfusion injury in skeletal muscle in rat. EuropeanJournal of Vascular and Endovasular Surgery, 21:28–34, 2001.
[40] Cox M., Baaijens F.P.T., Oomens C.W.J., and A. Stekelenburg. Correlation be-tween muscle damage and local mechanics after sustained loading of the rat hindlimb: A dedicated FEM study. internal report, July 2004.
[41] Curtin J.F., Donovan M., and Cotter T.G. Regulation and measurement of oxida-tive stress in apoptosis. Journal of Immunological Methods, 265:49–72, 2002.
[42] Dalla Libera L., Sabbadini R., Renken C., Ravara B., Betto R., Angelini A., andVescovo G. Apoptosis in the skeletal muscle of rats with heart failure is associatedwith increased serum levels of TNF-α and sphingosine. Journal of Molecular andCellular Cardiology, 33:1871–1878, 2001.
[43] Daniel R.K. and Wheatley D.C. Etiologic factors in production pressure sores:experimental model. Archives of Physical Medicine and Rehabilitation, 62:492–498, 1981.
[44] Diegelmann R.F. Excessive neutrophils characterize chronic pressure ulcers. Woundrepair and Regeneration, 11:490–495, 2003.
[45] Dirks A.J. and Leeuwenburgh C. Aging and lifelong calorie restriction result inadaptations of skeletal muscle apoptosis represor, apoptosis-inducing factor, x-linked inhibitor of apoptosis, caspase-3 and caspase-12. Free Radical Biology andMedicine, 36(1):27–39, 2004.
[46] Dolken G., Leisner E., and Pette D. Immunofluorescent localization ofglycogenolytic and glycolytic enzyme proteins and of malate dehydrogenaseisozymes in cross-striated skeletal muscle and heart of the rabbit. Histochemistry,43(2):113–121, 1975.
[47] Donkelaar C.C. van, Huyghe J.M., Vankan W.J., and Drost M.R. Spatial inter-action between tissue pressure and skeletal muscle perfusion during contraction.Journal of Biomechanics, 34:631–637, 2001.
[48] Droin N.M. and Green D.R. Role of Bcl-2 family members in immunity and disease.Biochimica et Biophysica Acta, 1644:179188, 2004.
[49] Dzeja P.P. and Terzic A. Phosphotransfer networks and cellular energetics. TheJournal of Experimental Biology, 206:2039–2047, 2003.
[50] Eggleton C.D., Vadapalli A., Roy T.K., and Popel A.S. Calculations of intracap-illary oxygen tension distributions in muscle. Mathematical Biosciences, 167:123–143, 2000.
[51] Eisen A., Fisman E.Z., Rubenfire M., Freeimark D., McKechnie R., Tenenbaum A.,Motro M., and Adler Y. Ischemic preconditioning: nearly two decades of research.A comprehensive review. Atherosclerosis, 172:201–210, 2004.
58

BIBLIOGRAPHY BIBLIOGRAPHY
[52] Flogel U., Merx M.W., Godecke A., Decking U.K.M., and Schrader J. Myoglobin:A scavenger of bioactive NO. Proceedings of the National Academy of Sciences ofthe United States of America, 98:735–740, 2001.
[53] Fontaine E., Eriksson O., Ichas F., and Bernardi P. Regulation of the perme-ability transition pore in skeletal muscle mitochondria. The Journal of BiologicalChemistry, 273(20):12662–12668, 1998.
[54] Friedrich O., Kress K.R., Ludwig H., and Fink R.H.A. Membrane ion conductancesof mammalian akeletal muscle in the post-decompression state after high-pressuretreatment. Journal of Membrane Biology, 188:11–22, 2002.
[55] Gabai V.L., Meriin A.B., Yaglom J.A., Wei J.Y., Mosseri D.D., and ShermanM.Y. Suppression of stress kinase JNK is involved in Hsp72-mediated protection ofmyogenic cells from transient energy deprivation. Journal of Biological Chemistry,275(48):3808838094, 2000.
[56] Garrett R.H. and Grisham C.M. Biochemistry. Saunders College Publishing, 1995.
[57] Goldman D. and Popel A.S. A computational study of the effect of capilary networkanastomoses and tortuosity on oxygen transport. Journal of Theoretical Biology,206:181–194, 2000.
[58] Goldman D. and Popel A.S. A computational study of the effect of vasomotion onoxygen transport from capillary network. Journal of Theoretical Biology, 209:189–199, 2001.
[59] Gonzalez C., Sanz-Alfayate G., Agapito M.T., Gomez-Nino A., Rocher A., andObeso A. Significance of ROS in oxygen sensing in cel systems with sensitivity tophysiological hypoxia. Respiratory Physiology & Neurology, 132:17–41, 2002.
[60] Gonzalez-Serratos H., Rozycka M., Cordoba-Rodriguez R., and Ortega A. Mem-brane healing and restoration of contractility after mechanical injury in isolatedskeletal muscle fibers of the frog. Proceedings of the National Academy of Sciencesof the USA, 93:5996–6001, 1996.
[61] Graaf R.A. de, Kranenburg A. van, and Nicolay K. In vivo 31P-NMR diffusion spec-troscopy of ATP and phosphocreatine in rat skeletal muscle. Biophysical JournalVolume, 78:1657–1664, 2000.
[62] Graaff v.d. K.M. Human Anatomy. Wm.C. Brown Publishers, 1995.
[63] Grandmaison P.A., Nanowski T.S., and Vance J.E. Externalization of phos-phatidylserine during apoptosis does not specifically require either isoform of phos-phatidylserine synthase. Biochimica et Biophysica Acta, 1636:1 11, 2004.
[64] Graves J.D. and Krebs E.G. Protein phosphorylation and signal transduction.Pharmacology & Therapeutics, 82(2-3):111–121, 1999.
[65] Gray H. and Carter H.V. Anatomy: descriptive and surgical. Edison : ChartwellBooks, 1995.
59

BIBLIOGRAPHY BIBLIOGRAPHY
[66] Grisotto P.C., Santos dos A.C., Coutinho-Netto J., Cherri J., and Piccinato C.E.Indicators of oxidative injury and alterations of the cell membrane in the skeletalmuscle of rats submitted to ischemia and reperfusion. Journal of Surgical Research,92:1–6, 2000.
[67] Gustafsson U., Gidlof A., Povlsen B., and Sirsjo A. Skeletal muscle tissue oxygenpressure distribution during early reperfusion after prolonged ischaemia. EuropeanJournal of Vascular and Endovasular Surgery, 17:41–46, 1999.
[68] Gutierrez J.M. and Ownby C.L. Skeletal muscle degeneration induced by venomphospholipases A2: insights into the mechanisms of local and systemic myotoxicity.Toxicon, 42:915–931, 2002.
[69] Guyton A.C. and Hall J.C. Textbook of Medical Physiology. Saunders, 2000.
[70] Hamill O.P. and Martinac B. Molecular basis of mechanotransduction in livingcells. Physiological Reviews, 81(2):685–740, 2001.
[71] Hartsock L.A., O’Farrell D., Seaber A.V., and Urbaniak J.R. Effect of increasedcompartment pressure in the microcirculation of skeletal muscle. Microsurgery,18:67–71, 1998.
[72] Hatoko M., Tanaka A., Kuwahara M., Yurugi S., Iioka H., and Niitsuma K. Dif-ference of molecular response to ischemia-reperfusion of rat skeletal muscle as afunction of ischemic time: study of the expression of p53, p21(WAF-1), Bax pro-tein, and apoptosis. Annals of Plastic Surgery, 48(1):68–74, 2002.
[73] Hayse G., Romaschin S., Liauw abd A., and Walker P.M. Separation of reperfusioninjury from ischemia-induced necrosis. Surgical Forum, 6:152–157, 1988.
[74] He H., Lam M., McCormick T.S., and Distelhorst C.W. Maintenance of cal-cium homeostasis in the endoplasmic reticulum by Bcl-2. Journal of Cell Biology,138:1219–1228, 1997.
[75] Heinemann A., Tsokos M., and Puschel K. Medico-legal aspects of pressure ulcers.Legal Medicine, 5:S263–S266, 2003.
[76] Hochachka P.W. Intracellular convection, homeostasis and metabolic regulation.The Journal of Experimental Biology, 206:2001–2009, 1999.
[77] Hochachka P.W. The metabolic implications of intracellular circulation. Proceed-ings of the National Academy of Sciences, 96(22):12233–12239, 1999.
[78] Hochachka P.W. and Mossey M.K.P. Does muscle creatine phosphokinase haveaccess to the total pool of phosphocreatine plus creatine? Regulatory IntegrativeComputational Physiology, 43:868872, 1998.
[79] Hodgkin A.L. and Huxley A.F. A quantitative description of membrane currentand its application to conduction an excitation in nerve. Journal of Physiology,117:500–544, 1952.
[80] Homer-Vanniasinkam S., Rowlands T.E., Hardy S.C., and Gough M.J. Skeletalmuscle ischaemia-reperfusion injury: Further characterization of a rodent model.European Journal of Vascular and Endovasular Surgery, 22:523–527, 2001.
60

BIBLIOGRAPHY BIBLIOGRAPHY
[81] Houwing R., Overgoor M., Kon M., Jansen G., Asbeck van B.S., and HaalboomJ.R.E. Pressure-induced skin lesions in pigs: reperfusion injury and the effects ofvitamin E. Journal of Wound Care, 9(1):36–40, 2000.
[82] Jackson M.J., Papa S., Bolanos J., Bruckdorfer R., Carlsen H., Elliott R.M., FlierJ., Griffiths H.R., Heales S., Holst B., Lorusso M., Lund E., Moskaug J.O., MoserU., Di Paola M., Polidori M.C., Signorile A., Stahl W., Vina-Ribes J., and Ast-ley S.B. Antioxidants, reactive oxygen and nitrogen species, gene induciton andmitochondrial dysfunction. Molecular Aspects of Medicine, 23:209–285, 2002.
[83] Jang J-H. and Surh Y-J. Potentiation of cellular antioxidant capacity by Bcl-2:implications for its antiapoptotic function. Biochemical Pharmacology, 66:1371–1379, 2003.
[84] Jennings R.B. and Reimer K.A. The cell biology of acute myocardial ischemia.Annual Review of Medicine, 42:225–246, 1991.
[85] Junqueira L.C., Carneiro J., Kelley R.O., Wisse E., Nieuwenhuis P., and Ginsel L.Functionele Histologie. Elsevier, Maarssen, 2000.
[86] Kao H.P., Abney J.R., and Verkman A.S. Determinants of the translational mobil-ity of a small solute in cell cytoplasm. The Journal of Cell Biology, 120(1):175–184,1993.
[87] Kato M., Hayashi R., Tsuda T., and Taniguchi K. High pressure-induced changes ofbiological membrane; study on the membrane-bound Na+/K+-ATPase as a modelsystem. European Journal of Biochemistry, 269:110–118, 2002.
[88] Kiechle F.L. and Zhang X. Apoptosis: biochemical aspects and clinical implica-tions. Clinica Chimica Acta, 326:27–45, 2002.
[89] Kinsey S.T., Locke B.R., Penke B., and Moerland T.S. Diffusional anisotropy isinduced by subcellular barriers in skeletal muscle. NMR in Biomedicine, 12:1–7,1999.
[90] Knight K.R., Messina A., Hurley J.V., Zhang B., Morrison W.A., and Stewart A.G.Muscle cells become necrotic rather than apoptotic during reperfusion of ischaemicskeletal muscle. International Journal of Experimental Patholology, 80(3):169–175,1999.
[91] Knight S.L., Taylor R.P., Polliack A.A., and Bader D.L. Establishing predicitveindicators for the status of loaded soft tissues. Journal of Applied Physiology,90:2231–2237, 2001.
[92] Korzeniewski B. Regulation of ATP supply during muscle contraction: theoreticalstudies. Biochemical Journal, 330:1189–1195, 1998.
[93] Korzeniewski B. Influence of substrate activation (hydrolysis of ATP by first stepsof glycolysis and β-oxidation ) on the effect of enzyme deficiencies, inhibitors,substrate shortage and energy demand on oxidative phosphorylation. BiophysicalChemistry, 104:107–119, 2003.
61

BIBLIOGRAPHY BIBLIOGRAPHY
[94] Korzeniewski B. and Zoladz J.A. A model of oxidative phosphorylation in mam-malian skeletal muscle. Biophysical Chemistry, 92:17–34, 2001.
[95] Koseki T., Inohara N., Chen S., and Nunez G. ARC, an inhibitor of apoptosisexpressed in skeletal muscle and heart that interacts selectively with caspases.Proceedings of the National Academy of Sciences, 95:5156–5160, 1998.
[96] Kraft T., Hornemann T., Stolz M., Nier V., and Wallimann T. Coupling of cre-atine kinase to glycolytic enzymes at the sarcomeric I-band of skeletal muscle: abiochemical study in situ. Journal of Muscle Research and Cell Motility, 21:691–703, 2000.
[97] Krebs E.G. and Graves J.D. Interactions between protein kinases and proteasesin cellular signalling and regulation. Advances in Enzyme Regulations, 40:441–470,2000.
[98] Kunz W.S. Control of oxidative phosphorylation in skeletal muscle. Biochimica etBiophysica Acta, 1504:12–19, 2001.
[99] Kurose I., Anderrson D.C., and Miyasaka M. Molecular determinants ofreperfusion-induced leukocyte adhesion and vascular protein leakage. CirculationResearch, 74:336–343, 1994.
[100] Kyriakides C., Austen W., Wang Y., Favuzza J., Kobzik L., Moore F.D., andHechtman H.B. Skeletal muscle reperfusion injury is mediated by neutrophils andthe complement membrane attack complex. American Journal of Physiology - CellPhysiology, 46:C1263–C1268, 1999.
[101] Kyriakis J.M. and Avruch J. Mammalian mitogen-activated protein kinase sig-nal transduction pathways activated by stress and inflammation. PhysiologicalReviews, 81(2):807–869, 2001.
[102] Labbe R., Lindsay T., and Walker P.M. The extent and distribution of skeletalmuscle necrosis after graded periods of complete ischemia. Journal of VascularSurgery, 6(2), 1987.
[103] Lacza S., Puskar M., Figueroa J.P., Zhang J., Rajapakse N., and Busija D.W.Mitochondrial nitric oxide synthase is constitutively active and is functionally up-regulated in hypoxia. Free Radical Biology & Medicine, 31(12):1609–1615, 2001.
[104] Lambeth M.J. and Kushmerick M.J. A computational model for glycogenolysis inskeletal muscle. Anals of Biomedical Engineering, 30:808–827, 2002.
[105] Langen R.C.J., Corn S.H., and Wouters E.F.M. ROS in the local and systemicpathogenesis of COPD. Free Radical Biology & Medicine, 35(3):226–235, 2003.
[106] LeBlanc A.C. Natural inhibitors of apoptosis. Progress in Neuro-Psychologicalogyand Biological Psychiatry, 27:215–229, 2003.
[107] Leist M., Sinle B., Castoldi A.F., Kuhnle S., and Nicotera P. Intracellular adenosinetriphosphate (ATP) concentration: A switch in the decision between apoptosis andnecrosis. Journal of Experimental Medicine, 185(8):1481–1486, 1997.
62

BIBLIOGRAPHY BIBLIOGRAPHY
[108] Li C. and Jackson R.M. Reactive species mechanisms of cellular hypoxia-reoxygenation injury. American Journal of Physiology: Cell Physiology, 282:C227–C241, 2002.
[109] Lin Z., Weinberg J.M., Malhotra R., Merritt S.E., Holzman L.B., and BrosiusF.C. GLUT-1 reduces hypoxia-induced apoptosis and JNK pathway activation.American Journal of Physiology: Endocrinology and Metabolism, 278:E958–E966,2000.
[110] Linder-Ganz E. and Gefen A. Mechanical compression-induced pressure sores inrat hindlimb: muscle stiffness, histology, and computational models. Journal ofApplied Physiology, 96:2034–2049, 2004.
[111] Lindsay T.F., Liauw S., Romaschin A.D., and Walker P.M. The effect of is-chemia/reperfusion on adenine nucleotide metabolism and xanthine oxidase pro-duction in skeletal muscle. Jounral of Vascular Surgery, 12(1):8–15, 1990.
[112] Lo A., Fuglevand A.J., and Secomb T.W. Oxygen delivery to skeletal muscle finers:effects of microvascular unit structure and control mechanisms. American Journalof Physiology - Heart and Circulatory Physiology, 285:H955–H963, 2003.
[113] Lockshin R.A. and Zakerit Z. Caspase-independent cell deaths. Current Opinionin Cell Biology, 14:727733, 2002.
[114] Lorenzo H.K. and Susin S.A. Mitochondrial effectors in caspase-independent celldeath. FEBS letters, 557:14–20, 2004.
[115] Lu Y.T., Hellewel P.G., and Evans T.W. Ischemia-reperfusion lung injury: contri-butions of neutrophils and hydrostatic pressure. American Journal of Physiology- Lung Cellular and Molecular Physiology, 273:L46–L54, 1997.
[116] Luo C.H. and Rudy Y. A model of the ventricular cardiac action potential: depolar-ization, repolarization, and their interaction. Circulation Research, 68:1501–1526,1991.
[117] Lyabakh K.G. Mathematical modeling of oxygen transport to skeletal muscleduring exercise. Oxygen transport to tissue XXI Advances in experimental medicineand biology, 471:585–593, 1999.
[118] Lyabakh K.G. and Mankovskaya I.N. Oxygen transport to skeletal muscle workingat VO2max in acute hypoxia: theoretical predictions. Comparative Biochemistryand Physiology Part A, 132:53–60, 2002.
[119] Maeno E., Ishizaki Y., Kanaseki T., Hazama A., and Okada Y. Normotoxic cellshrinkage because of disordered volume regulation is an early prerequisite to apop-tosis. Proceedings of the National Academy of Sciences of the USA, 97(17):9487–9492, 2000.
[120] Mak A.F.T., Huang L., and Wang Q. A biphasic poroelastic analysis of the flowdependent subcutaneous tissue pressure and compaction due to epidermal loadings:issues in pressure sore. Journal of Biomechanical Engineering, 116:421–429, 1994.
63

BIBLIOGRAPHY BIBLIOGRAPHY
[121] Malhotra R. and Brosius F.C. Glucose uptake and glycolysis reduce hypoxia-induced apoptosis in cultured neonatal rat caridac myocytes. Journal of BiologicalChemistry, 274:12567–12575, 1999.
[122] Mars M. and hadley G.P. Raised intracompartmental pressure and compartmentsyndromes. Inujury, 29(6):403–411, 1998.
[123] Maxwell S.R.J. and Lip G.Y.H. Reperfusion injury: a review of the pathophys-iology, clinical manifestations and therapeutic options. International Journal ofCardiology, 58:95–117, 1997.
[124] McClintock D.S., Santore M.T., Lee V.Y., Brunelle J., Scott Budinger G.R., ZongW-X., Thompson C.B., Hay N., and Chandel N.S. Bcl-2 family members andfunctional electron transport chain regulate oxygen deprivation-induced cell death.Molecular and Cellular Biology, 22(1):94–104, 2002.
[125] McComas A.J. Skeletal Muscle, Form and Function. McMaster University, 1996.
[126] McGuire B.J. and Secomb T.W. A theoretical model for oxygen transport in skele-tal muscle under conditions of high oxygen demand. Journal of Applied Physiology,91:2255–2265, 2001.
[127] McNeil P.L. and Steinhardt R.A. Loss, restoration, and maintenance of plasmamembrane integrity. Journal of Cell Biology, 137(1):1–4, 1997.
[128] Mellander S. and Albert U. Effects of increased and decreased tissue pressure onhaemodynamic and capillary events in cat skeletal muscle. Journal of Physiology,481:163–175, 1994.
[129] Menger M.D., Rucker M., and Vollmar B. Capillary dysfunction in striated muscleischemia/reperfusion: on the mechanisms of capillary ”no-reflow”. Pathophysiology,8(1):2–7, 1997.
[130] Michel C.C. and Gollott H. Microvascular mechanisms in stasis and ischaemia. InBader D.L., editor, Pressure sores, clinical practice and scientific approach, pages153–163. Macmillan Press, 1990.
[131] Miller G.E. and Seale J. Lymphatic clearance during compressive loading. Lym-phology, 14:161–166, 1981.
[132] Minet E., Mottet M.D., Raes M., and Michiels C. Transduciton pathways involvedin hypoxia-inducible factor-1 phosphorylation and activation. Free Radical Biology& Medicine, 31(7):847–855, 2001.
[133] Moissac de D., Gurevich R.M., Zheng H., Singal P.K., and Kirshenbaum L.A. Cas-pase activaiton and mitochondrial cytochrome c release during hypoxia-mediatedapoptosis of adult ventricular myocytes. Journal of Molecular and Cellular Cardi-ology, 32:53–63, 2000.
[134] Mongin A.A. and Orlov S.N. Mechanisms of cell volume regulation and possiblenature of the cell volume sensor. Pathophysiology, 8:77–88, 2001.
64

BIBLIOGRAPHY BIBLIOGRAPHY
[135] Morin D., Hauet T., Spedding M., and Tillement J-P. Mitochondria as targets forantiischemic drugs. Advanced Drug Delivery Reviews, 49:151–174, 2001.
[136] Morishima N., Nakanishi K., Takenouchi H., Shibata T., and Yasuhiko Y. Anendoplasmic reticulum stress-specific caspase cascade in apoptosis. The Journal ofBiological Chemistry, 277(37):34287–34294, 2002.
[137] Nakagawa T., Zhu H., Morishima N., Li E., Xu J., Yankner B.A., and yuan J.Caspase-12 mediates ensoplasmic-reticulum-specific apoptosis and cytotoxicity byamyloid-β. Nature, 403:98–103, 2000.
[138] Nanobashvili J., Neumayer C., Fugl A., Punz A., Blumer R., Prager M.,Mittlbock M., Gruber H., Polterauer P., Roth E., Malinski T., and Huk I. Is-chaemia/reperfusion injury of skeletal muscle: Plasma taurine as a measure oftissue damage. Surgery, 133:91–100, 2003.
[139] Nola G.T. and Vistnes L.M. Differential response of skin and muscle in the experi-mental production of pressure sores. Plastic and Reconstructive Surgery, 66(5):728–735, 1980.
[140] Oomens C.W.J., Bouten C.V.C., Bressers O.F.J.T., Bader D.L., and BosboomE.M.H. Can loaded interface characteristics influence strain distributions in muscleadjacent to bony prominences.
[141] Paek R., Chang D.S., Brevetti L.S., Rollins M.D., Brady S., Ursell P.C., HuntT.K., Sarkar R., and Messina L.M. Correlation of a simple direct measurementof muscle pO2 to a clinical ischemia index and histology in a rat model of chronicsevere hindlimb ischemia. Jounral of Vascular Surgery, 39:172–179, 2002.
[142] Peeters E.A.G. Biomechanics of single cells under compression. PhD thesis, Eind-hoven, University of Technology, 2004.
[143] Peterson N.0., McConnaughey W.B., and Elson E.L. Dependence of locally mea-sured cellular deformability on position on the cell, temperature, and cytochalasinb. Proceedings of the National Academy of Sciences of the USA, 79:5327–5331111,1982.
[144] Petrasek P.F., Homer-Vanniasinkam S., and Walker P.M. Determinants of ischemicinjury to skeletal muscle. Journal of Vascular Surgery, 19(4), 1994.
[145] Pieper A.A., Verma A., Zhang J., and Snyder S.H. Poly (ADP-ribose) polymerase,nitric oxide and cell death. Trends in Pharmacological Sciences, 20:171–181, 1999.
[146] Plas D.R. and Thompson C.B. Cell metabolism in the regulation of programmedcell death. Trends in Endocrinology and Metabolism, 13:74–78, 2002.
[147] Poglazov B.F. and Livanova N.B. Interaction of actin with the enzymes of carbo-hydrate metabolism. Advances in Enzyme Regulation, 25:297–305, 1986.
[148] Proskuryakov S.Y., Konoplyannikov A.G., and Gabai V.L. Necrosis: a specificform of programmed cell death? Experimental Cell Research, 283:1–16, 2003.
65

BIBLIOGRAPHY BIBLIOGRAPHY
[149] Reddy N.P. Effects of mechanical stress on lymph and interstitial fluid flows. InBader D.L., editor, Pressure sores, clinical practice and scientific approach, pages203–219. Macmillan Press, 1990.
[150] Reddy N.P., Cochran G.V.B., and Krouskop T.A. Interstitial fluid lfow as a factorin decubitus ulcer formation. Journal of Biomechanics, 14:879–881, 1981.
[151] Reddy N.P., Palmieri V., and Cochran G.V.B. Subcutaneous interstitial fluid pres-sure during external tissue loading. American Journal of Physiology - RegulatoryIntegrative and Comparative Physiology, 240:R327–R329, 1981.
[152] Reddy N.P. and Patel K. A mathematical model of flow through the terminallymphatics. Medical Engineering Physiology, 17(2):134–140, 1995.
[153] Regula K.M., Ens K., and Kirshenbaum L.A. Mitochondria-assisted cell suicide: alicense to kill. Journal of Molecular and Cellular Cardiology, 35:559–567, 2003.
[154] Reid M.B. Role of nitric oxide in skeletal muscle: synthesis, distribution andfunctional importance. Acta Physiologica Scandinavica, 162:401–409, 1998.
[155] Reneman R.S., Slaaf D.W., Lindbom L., Tangelder G.J., and Arfors K-E. Muscleblood flow distirbances produced by simultaneous elevated venous and total muscletissue pressure. Microvascular Research, 20(6):307–318, 1980.
[156] Roach D.M., Fitridge R.A., Laws P.E., Millard S.H., Varelias A., and CowledP.A. Up-regulation of MMP-2 and MMP-9 leads to degradation of type IV colla-gen during skeletal muscle reperfusion injury; protection by the MMP inhibitor,doxycycline. European Journal of Endovascular Surgery, 23:260–269, 2002.
[157] Ruppin E., Ofer E., Reggia J.A., Revett K., and Goodall S. Pathogenic mechanismsin ischemic damage: a computational study. Computers in Biology and Medicine,29:39–59, 1999.
[158] Sacks A.H. Theoretical prediction of a time-at-pressure curve for avoiding pressuresores. Journal of Rehabilitation Research and Development, 26(3):27–34, 1989.
[159] Salathe E.P. and Gorman A.D. Modeling oxygen concentration in skeletal muscle.Mathematical and Computer Modeling, 26(4):91–102, 1997.
[160] Salcido R., Donofrio J.C., Fisher S.B., LeGrand E.K., Dickey K., Carney J.M.,Schosser R., and Liang R. Histopathology of pressure ulcers as a result of sequentialcomputer-controlled pressure sessions in a fuzzy rat model. Advances in WoundCare, 7(5):23–40, 1994.
[161] Salem J.E., Saidel G.M., Stanley W.C., and Cabrera M.E. Mechanistic model ofmyocardial energy metabolism under normal and ischemic conditions. Annals ofBiomedical Engineering, 30:202–216, 2002.
[162] Santore M.T., McClintock D.S., Lee V.Y., Scott Budinger G.R., and Chandel N.S.Anoxia-induced apoptosis occurs through a mitochondria-dependent pathway inlung epithelial cells. American Journal of Physiology - Lung Cellular and MolecularPhysiology, 282:L727–L734, 2002.
66

BIBLIOGRAPHY BIBLIOGRAPHY
[163] Sato M., Theret D.P., Wheeler L.T., Ohshima N., and Nerem R.M. Application ofthe micropipette technique to the measurement of cultured porcine aortic endothe-lial cell viscoelastic properties. Journal of Biomechanical Engineering, 112(3):263–168, 1990.
[164] Schlag M.G., Harris K.A., and Potter R.F. Role of leukocyte accumulation andoxygen radicals in ischemia-reperfusion-induced injury in skeletal muscle. AmericanJournal of Physiology - Heart Circulation Physiology, 280:H1716–H1721, 2001.
[165] Selman C. and Leeuwenburgh C.
[166] Semenza G.L. Hypoxia-inducible factor 1: master regulator of O2 homeostasis.Current Opinion in Genetics ad Development, 8:588–594, 1998.
[167] Sexton W.L., Korthuis R.J., and Laughlin M.H. Ischemia-reperfusion injury inisolated rat hindquarters. Journal of Applied Physiology, 68:387–392, 1990.
[168] Sharpe J.C., Arnoult D., and Youle R.J. Control of mitochondrial permeability byBcl-2 family members. Biochimica et Biophysica Acta, 1644:107–113, 2004.
[169] Shimizu S., Eguchi Y., Kamiike W., Waguri S., Uchiyama Y., Matsuda D., andTsujimoto Y. Retardation of chemical hypoxia-induced necrotic cell death by Bcl-2and ICE inhibitors: possible involvement of common mediators in apoptotic andnecrotic signal transductions. Oncogene, 12(10):2045–2050, 1996.
[170] Shrier I. and Magder S. Pressure-flow relationships in in vitro model of compart-ment syndrome. Journal of Applied Physiology, 79(1):214–221, 1995.
[171] Stevens A.S. and Lowe J.S. Human histology. Mosby, London, 1997.
[172] Suarez R.K. Shaken and stirred: muscle structure and metabolism. Journal ofExperimental Biology, 206:2021–2029, 2003.
[173] Sundin B.M., Hussein M.A., Glasofer S., El-Falaky M.H., Abdel-Aleem S.M.,Sachse R.E., and Klitzman B. The role of allopurinol and deferoxamine in prevent-ing pressure ulcers in pigs. Plastic and Reconstructive Surgery, 105(4):1408–1421,2000.
[174] Suzuki Y., Imai Y., Nakayama H., Takahashi K., Takio K., and Takahashi R. Aserine protease, HtrA2, is released from the mitochondria and interacts with XIAP,inducing cell death. Molecular Cell, 8(3):613–621, 2001.
[175] Swartz M.A. The physiology of the lymphatic system. Advanced Drug DeliveryReviews, 50:3–20, 2001.
[176] Swartz M.A., Kaipainen A., Netti P.A., Brekken C., Boucher Y., Grodzinsky A.J.,and Jain R.K. Mechanics of interstitial-lymphatic fluid transport: theoretical foun-dation and experimental validation. Journal of Biomechanics, 32:1297–1307, 1999.
[177] Toth A., Ivanics T., Ruttner Z., Slaaf D.W., Reneman R.S., and Ligeti L. Quanti-tative assessment of [Ca2+]i levels in rat skeletal muscle in vivo. American Journalof Physiology - Heart Circulation Physiology, 44:H1652–H1662, 1998.
67

BIBLIOGRAPHY BIBLIOGRAPHY
[178] Thomas D.D., Liu X., Kantrow S.P., and Lancaster J.R. The biological lifetime ofnitric oxide: Implications for the perivascular dynamics of NO and O2. Journal ofthe Neurological Sciences, 179:1–33, 2000.
[179] Todd B.A. and Thacker J.G. Three-dimensional computer model of the humanbuttocks, in vivo. Journal of Rehabilitation Research and Development, 31(2):111–119, 1994.
[180] Torres C. de, Munell F., Roig M., Revento J., and Macaya A. Naturally occurringcell death during postnatal development of rat skeletal muscle. Muscle & Nerve,26:777–783, 2002.
[181] Trump B.F. and Berezesky I.K. The role of altered [Ca2+]i regulation in apoptosis,oncosis, and necrosis. Biochimica et Biophysica Acta, 1313:173–178, 1996.
[182] Urso M.L. and Clarkson P.M. Oxidative stress, exercise, and antioxidant supple-mentation. Toxicology, 189:41–54, 2003.
[183] Vankan W.J. A finite element model of blood perfused skeletal muscle. PhD thesis,Eindhoven, University of Technology, 1996.
[184] Vendelin M., Kongas O., and Saks V. Regulation of mitochondrial respirationin heart cells analyzed by reaction-diffusion model of energy transfer. AmericanJournal of Physiology - Cell Physiology, 278:C747–C764, 2000.
[185] Vlahakis N.E., Schroeder M.E., Pagano R.E., and Hubmayr R.D. Role ofdeformation-induced lipid trafficking in the prevention of plasma membrane stressfailure. American Journal of Respiratory and Critical Care Medicine, 166:1282–1289, 2002.
[186] Vollmar B., Westermann S., and Menger M.D. Microvascular response to com-partment syndrome-like external pressure elevation: An in vitro fluorescence mi-croscopic study in the hamster striated muscle. The Journal of Trauma: Injury,Infection, and Critical Care, 46(1):91–96, 1999.
[187] Wang W.Z., Anderson G., Maldonado C., and Barker J. Attenuation of vasospasmand capillary no-reflow by ischemic preconditioning in skeletal muscle. Micro-surgery, 17:324–329, 1996.
[188] Wang W.Z., Guo S.Z., Anderson G.L., and Miller F.N. The initiating factors oflate preconditioning in skeletal muscle. Journal of Surgical Research, 99:92–99,2001.
[189] Wang Y.N., Bouten C.V.C., Lee D.A., and Bader D.L. Compression induceddamage in a muscle cell model in vitro. 2004.
[190] Webster K.A., Discher D.J., Kaiser S., Hernandez O., Sato B., and Bisphoric N.H.Hypoxia-activated apoptosis of cardiac myocytes requires reoxygenation or a pHshift and is independent of p53. The Journal of Clinical Investigation, 104:239–252,1999.
68

BIBLIOGRAPHY BIBLIOGRAPHY
[191] Wegmann G., Zanolla E., Eppenberger H.M., and Wallimann T. In situ compart-mentation of creatine kinase in intact sarcomeric muscle: the acto-myosin overlapzone as a molecular sieve. Journal of Muscle Research and Cell Motility 1992Aug;13(4):420-35, 13(4):420–435, 1992.
[192] Wheatley D.N. Diffusion theory, the cell and the synapse. BioSystems, 45:151163,1998.
[193] White B.C., Sullivan J.M., DeGracia D.J., ONeil B.J., Neumar R.W., GrossmanL.I., Rafols J.A., and Krause G.S. Brain ischemia and reperfusion: molecularmechanisms of neuronal injury. PNAS, 98(1):355–360, 2001.
[194] Yi C-S., Fogelson A.L., Keener J.P., and Peskin C.S. A mathematical study of vol-ume shifts and ionic concentration changes during ischemia and hypoxia. Journalof Theoretical Biology, 220:83–106, 2003.
[195] Yu S.P. Na+, K+-ATPase: the new face of an old player in pathogenesis andapoptotic/hybrid cell death. Biochemical Pharmacology, 66:1601–16909, 2003.
[196] Yu S.P., Canzoniero L.M.T., and Choi D.W. Ion homeostasis and apoptosis. Cur-rent Opinion in Cell Biology, 13:405–411, 2001.
[197] Zhang J.D., Mak A.F.T., and Huang L.D. A large deformation biomechanicalmodel for pressure ulcers. Journal of Biomechanical Engineering, 119:406–408,1997.
[198] Zong W-X, Li C., Hatzivassiliou G., Lindsten T., Yu Q-C., Yuan J., and ThompsonC.B. Bax and Bak can localize to the endoplasmic reticulum to initiate apoptosis.The Journal of Cell Biology, 162(1):59–69, 2004.
69

Appendix A
Muscle structure
Skeletal muscles consist of fascicles, bundles of muscle fibres, that are each surroundedby a layer of connective tissue, the perimysium (figure A.1). Muscle fibres in turn, areembedded in a very thin layer of connective tissue, the endomysium, which is not morethan 1µm125 thick. The fibres contain multiple peripheral nuclei from the individualcells that are fused to form the final muscle cell with a diameter ranging from 10 to100µm.65,85 The cell is composed of multiple myofibrils, the contractile elements, and itis surrounded by its cell membrane, the sarcolemma (figure A.2). A myofibril in turn,consists of sarcomeres, which are repetitive units of myosin and actin filaments between2 Z discs (figure A.3). The highly structured organization of these sarcomeres gives askeletal muscle its cross-striated appearance. Protruding from the Z discs are the actinfilaments, which partly overlap with the myosin filaments. The total dark region of over-lap is called the A band, the center of the sarcomere where only myosin is found, is calledthe H band, and the light bands adjacent to the Z discs are A bands, containing onlyactin.Multiple capillaries run through the endomysium, branched off from arteries in the pe-rimysium. There are several capillaries that supply one fibre of nutrients and oxygen.The precise capillary density varies from one muscle type to another, being largest inslow oxidative (type I) muscles, because these are more dependent on oxygen for theirmetabolism than fast glycolytic (type II) muscle fibres.171
70

Muscle structure
Figure A.1: Skeletal muscle structure: The entire muscle is surrounded by the epimysium, whichcontinues as perimysium covering the fascicles, and finally as endomysium, which surrounds theindividual muscle fibers. Capillaries run between the individual fibres.65
Figure A.2: The composition of one cell: It is covered by the sarcolemma, and consists of manymyofibrils.62
Figure A.3: The structure of a sarcomere: pink lines are actin filaments, and blue lines myosinfilaments.
71

Appendix B
Signalling molecules in apoptosis
There are numerous molecules influencing the processes going on after cell injury, someof which will be briefly discussed below.
MAPK signal transduction pathways
Mitogen-activated protein kinase (MAPK) signal transduction pathways are activatedby a wide variety of stimuli, both physiological and pathological. The MAPK pathways,in turn, lead to coordinated activation of gene transcription, protein synthesis, cell cyclemachinery, cell death, and differentiation.101
The core of this signal transduction pathway consists of three kinases, of which thefirst, MAPK-kinase-kinase (MAP3K, MAPKKK or MEKK) activates MAPK-kinase(MAPKK, MAP2K, MEK or MKK), which in turn activates MAPK.101 MAPKs aresubdivided into three groups. The first group consists of extracellular signal-regulatedkinases (ERKs) that respond to growth factor stimulation and are anti-apoptotic. c-junN-terminal kinases (JNKs or stress-activated protein kinases SAPKs), and p38 kinasesare the second and third group, and they are triggered after exposure of cells to environ-mental stress.24,83 They are major components of the stress-induced apoptotic pathway,which can be activated by ischemia, oxidative stress, DNA damage, or TNF cytokines(TNF, interleukin-1, Fas ligand, receptor activator of NF-κB etc.101).101,148 Recruit-ment of JNK and p38 kinase activate transcription factors such as AP-1.82,101 JNK mayalso phosphorylate mitochondrial substrates, leading to the activation of Bax-dependentapoptosis.13
Further, JNK and p38 might be indirect targets of caspases, and they might then acti-vate caspases again in a positive feedback loop.64,97
The observation that inhibition of JNK decreased necrotic cell death in myogenic cellsafter transient energy deprivation, indicates that JNK is also involved in necrosis. Forother pro-apoptotic (p38) and anti-apoptotic (Akt, ERK) kinases, similar conclusionswere drawn.55,148
72

Signalling molecules in apoptosis
Pro-apoptotic molecules
Bax and Bak Bax and Bak are pro-apoptotic Bcl-2 family members that exert theireffect depending on their subcellular localization. When attached to the endoplasmicreticulum, they activate caspase-9 via activated caspase-12, but when in contact withmitochondria, they help initiate PTP opening and stimulate caspase-9 activation via theapoptosome.25,153,198
omi/HtrA2 and Smac/Diablo Another pro-apoptotic molecule is the serine pro-tease omi/HtrA2, which is released from the mitochondria together with cytochrome cand Smac/Diablo.8 Both omi/HtrA2 and Smac/Diablo can suppress the action of in-hibitor of apoptosis proteins (IAPs), thereby sensitizing the cell to apoptosis.8,10,45,106,114,153,168
Omi/HtrA2 can also induce cell death in a caspase-independent way.174
TNF-α Tumor necrosis factor-α (TNF-α) is an inflammatory cytokine that can initi-ate apoptosis through the extrinsic pathway, contributing to the formation af a DISC.Furthermore, it causes activation of phospholipase A282, provokes a rise in ROS produc-tion by mitochondria41,82, and induces the expression of the inducible NOS41.TNF-α also stimulates NF-κB activity, thereby increasing IAP expression, which is ac-tually an anti-apoptotic effect.106 However, one of the IAPs may also have some pro-apoptotic effect in accelerating the TNFR-mediated activation of caspase-8.106
Dalla Libera et al.42 demonstrated that the level of plasma TNFα was correlated withthat of extracellular sphingosine, a second messenger able to increase the number ofapoptotic cells without involving TNF receptors of which they claim that they are nothighly expressed on skeletal muscle cells, but with activation of caspases-3 and 9.
AIF Upon its release from the mitochondrial intermembrane space, apoptosis induc-ing factor (AIF) translocates to the nucleus to cause DNA condensation and fragmen-tation.10,106,114 Besides its effect on the nucleus, it may also provoke caspase-9 releasefrom the mitochondria, and it has been associated with both free-radical scavenging andproduction. Which of the two is executed probably depends on the subcellular localiza-tion of AIF, scavenging when in the mitochondria, and generating free radicals when inthe cytosol.114
EndoG and CAD Endonuclease G (EndoG) is another molecule that is released fromthe mitochondrial intermembrane space after PTP opening. It is involved in caspase-independent DNA degradation into oligonucleosomal fragments10,114, comparable to theaction of caspase-activated DNAse (CAD).
IκB Caspase-mediated cleavage of IκB leads to its binding to NF-κB, and suppres-sion of the activity of NF-κB. When IκB has already been phosphorylated and henceinactivated, it has become insensitive to caspase cleavage.97
73

Signalling molecules in apoptosis
Anti-apoptotic molecules
Bcl-2 Bcl-2 has several anti-apoptotic effects. Associated with mitochondria, Bcl-2may prevent PTP-opening and the resulting release of mitochondrial molecules, for ex-ample by stabilizing the outer mitochondrial membrane or disruption of the interactionof Bax/Bak with PTP components.153 Direct interaction with APAF-1 prevents forma-tion of the apoptosome, and enabling IAP activity also inhibits apoptotic activities.106
Bcl-2 has also been found to maintain Ca2+ homeostasis by inhibiting Ca2+ release fromthe e.r. , preventing Ca2+ overload.74
Furthermore, there is some evidence that the pro-apoptotic members of the Bcl-2 fam-ily are involved in the anti-oxidant system, probably by modulating GSH metabolism.41
Among others, over-expression of Bcl-2 leads to higher levels of antioxidant enzymes andGSH, creatineg a more reducing environment. Bcl-2 also induces relocation of GSH fromcytosol to nucleus, where it upregulates the transcription of NF-κB, AP-1 and p53, andactivates antioxidant protective genes.41,83
Bcl-XL Bcl-XL is an anti-apoptotic Bcl-2 family member. McClintock et al.124 foundthat Bcl-XL prevented oxygen-deprivation-induced apoptosis through inhibiting cytochromec release from the mitochondria. Prevention of Bax/Bak activation is proposed as themechanism of action.25,48
IAP Inhibitor of apoptosis proteins (IAPs) can directly interact with caspases-3, 7 and9 or degrade them to inhibit their activities.45,106,153 They also activate the Akt survivalpathway, JNK expression and NF-κB.106
TNF-α, TRAIL, the Akt survival pathway and NF-κB all up-regulate IAPs.106
ARC Apoptosis repressor with CARD (caspase recruitment domain) (ARC) is a pro-tein specifically expressed in skeletal muscle and heart. It is known to translocate fromcytosol to mitochondria under oxidative stress.45 This repressor prevents the release ofcytochrome c from mitochondria45. It also inhibits apoptosis induced by stimulation ofTNFRs and Fas receptors, possibly through interaction with initiator caspase-2 and -8.95
Hsp Heat shock proteins (Hsps) can protect cells from apoptosis as well as necrosisinduced by various stimuli, such as oxidative stress and ischemia/reperfusion.148 Throughinteraction with APAF-1 and cytosolic cytochrome c, procaspase-3, or AIF, they preventthe formation of a functional apoptosome, caspase activation, or the caspase-independentcell death pathway respectively.106,148
Hsps also exhibit anti-necrotic effects apparently through protection of mitochondria.148
Akt Procaspase-9 can be inactivated by Akt (also called protein kinase B), which isactivated upon binding of certain growth factors to their receptors, activation of PI3K,or in response to NO·.25,41,97 But caspases can also inactivate Akt through cleavage.97
Akt can also exert its anti-apoptotic effect through inactivation of Bad, a pro-apoptoticBcl-2 family member, controlling the activation of NFκB, or stimulating hexokinase, a
74

Signalling molecules in apoptosis
key regulator of the overall rate of glycolysis.25,146 An additional effect of hexokinase isthat upon binding to VDAC in the mitochondrial membrane, it blocks binding of Baxand thus PTP opening.25
PARP Poly(ADP-ribose)polymerase (PARP) is one of the targets of caspase-3, and isa DNA repair enzyme that uses nicotinamide dinucleotide (NAD).133,145 ResynthesizingNAD requires ATP, explaining the energy depletion upon massive stimulation of PARP.Cleavage by caspases leads to inactivation with concomitant prevention of ATP depletion,enabling apoptosis and avoiding necrosis.145,148
NF-κB Nuclear factor-κB is a transcription factor that promotes cell survival. It isconstitutively expressed in the cytosol in an inactive complex that can be activated withthe help of Bcl-2, IAP and MAPKs.106 Once active, it regulates the transcription of cellsurface receptors and cytokines among others.82 IAPs are also under control of NF-κB.45
Also, transcription of antioxidant enzymes catalase, SOD, and GPx is partially mediatedby NF-κB, as well as AP-1. Synthesis of GSH, which also prevents accumulation of ROS,is under control of NF-κB and AP-1 as well.83 ROS have also been implicated in theactivation of NF-κB, while NO· appears to be inhibitory.82
p53 The cellular redox state, cellular stress, or DNA damage activate transcriptionfactors p53, which can signal to the cell to allow DNA repair or to enter apoptosis.25,82
Among the target genes of p53 are the pro-apoptotic Bax and Bid.48
AP-1 Activation of AP-1 is mediated by JNK, p38 kinase, and cellular redox state,which also influences DNA-binding of AP-1.82,101 AP-1 then regulates the expression ofgenes associated with growth, differentiation, neuronal excitation, and stress.82
75