Embed Size (px)
Citation preview
“ Dan Setlacec” Center of General Surgery and Liver Transplantation, Fundeni Clinical Institute, Bucharest
Dr. Simona Olimpia Dima
Diabetul zaharat post-rezectie pancreatica, preventie si atitudine
Background
• The number of patients undergoing pancretic surgery is increasing:
– Early diagnosis of premalignant lesions
– Referral of patients affected by surgical pancreatic disease to high-volume centers.1,2
• Life expectancy of patients undergoing pancreatectomy has increased in recent years
• Post-resection diabetes is now atracting attention as a factor influencing quality of life and life expectancy of patients who have undergone this procedure
1Balzano G. Et al. Br. J. Surg.2008;95:357-362; 2Lemmens VE. Et al. Br. J Surg. 2011; 98:1455-1462/ 3Balzano G. Et al. Ann Surg. 2013; 258:210-218
Classification of Diabetes
• Type 1 diabetes
– β-cell destruction
• Type 2 diabetes
– Progressive insulin secretory defect
• Other specific types of diabetes
– Genetic defects in β-cell function, insulin action
– Diseases of the exocrine pancreas
– Drug- or chemical-induced
• Gestational diabetes mellitus (GDM)
ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S11.

2-3 % of the type 3c DM are patients who underwent pancreatectomy1, 2
1Ewald N et al. Diabetes Met Res Rev. 2011;28: 338-42 2 Hardt PB e al. Diab. Care 2008; 31 Suppl 2: S165-169
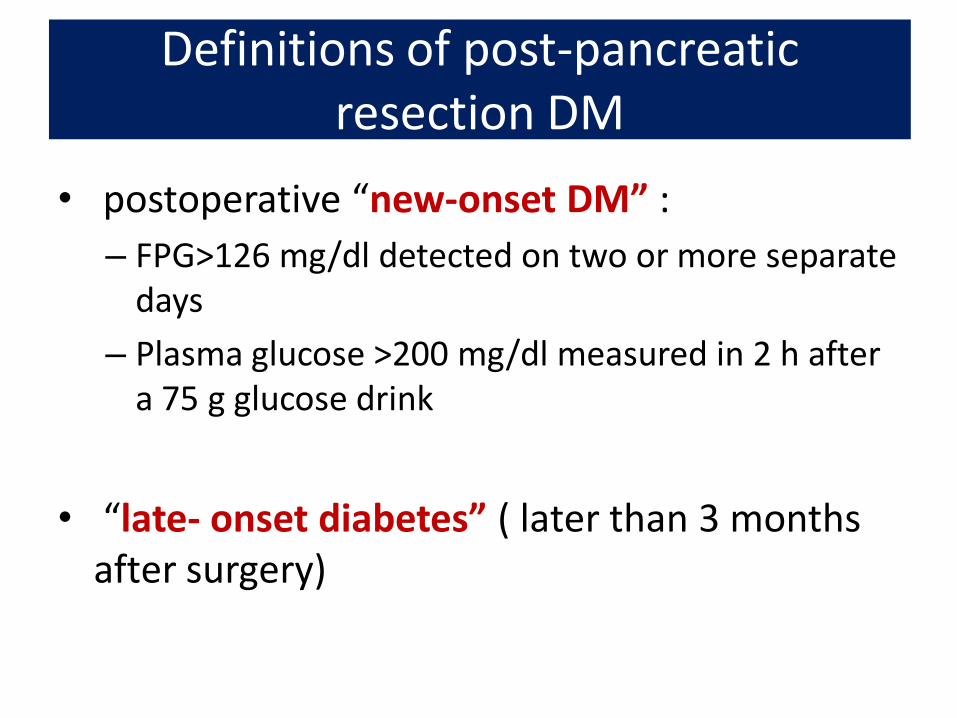
Definitions of post-pancreatic resection DM
• postoperative “new-onset DM” :
– FPG>126 mg/dl detected on two or more separate days
– Plasma glucose >200 mg/dl measured in 2 h after a 75 g glucose drink
• “late- onset diabetes” ( later than 3 months after surgery)
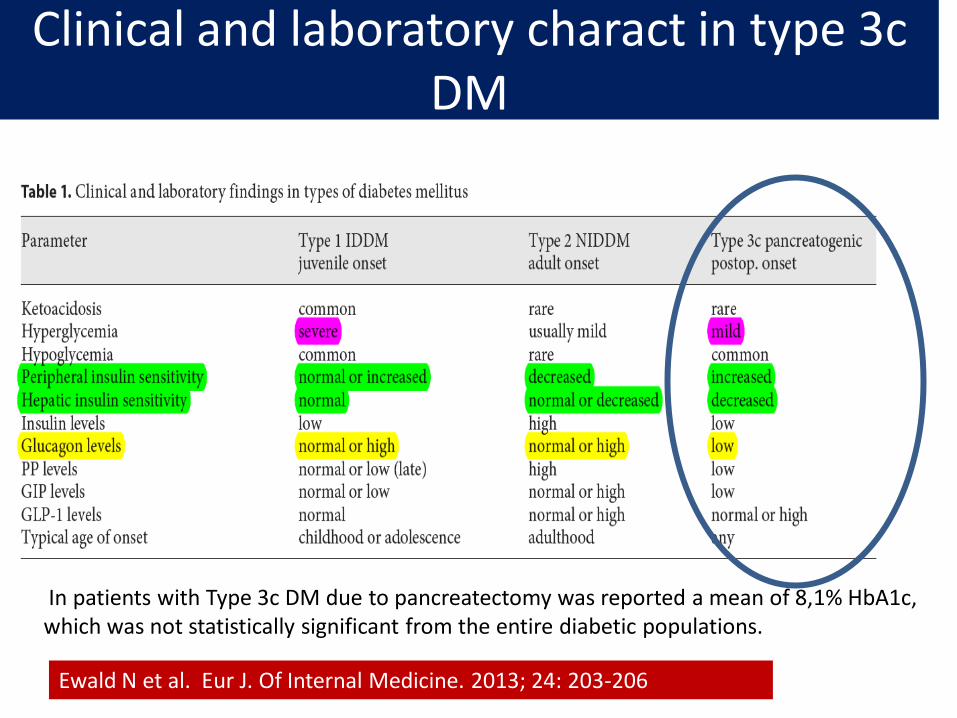
Clinical and laboratory charact in type 3c DM
In patients with Type 3c DM due to pancreatectomy was reported a mean of 8,1% HbA1c, which was not statistically significant from the entire diabetic populations.
Ewald N et al. Eur J. Of Internal Medicine. 2013; 24: 203-206
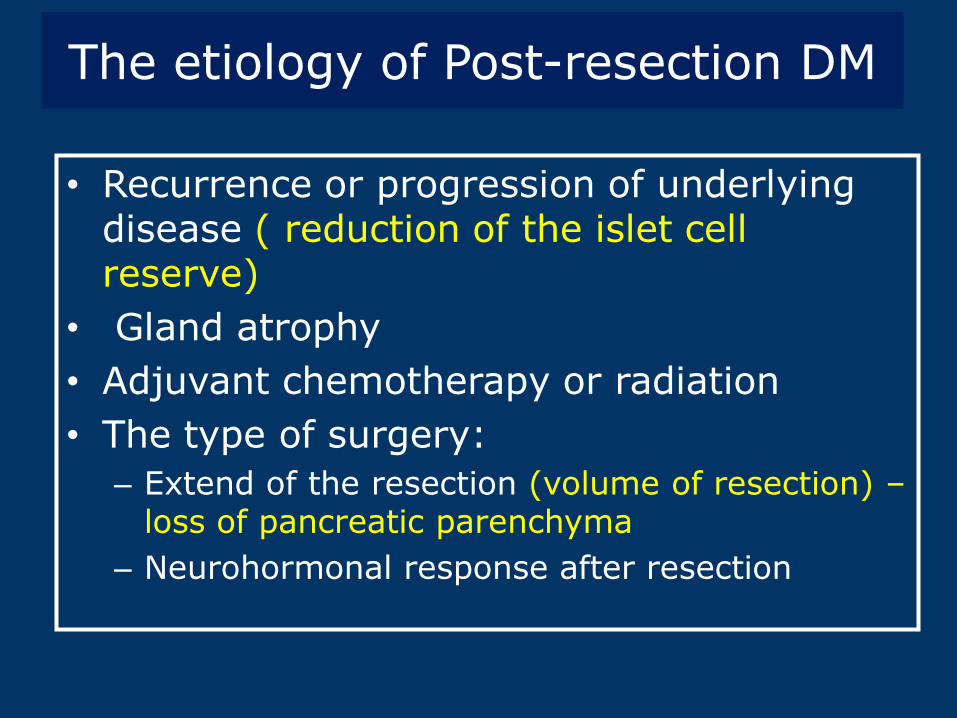
The etiology of Post-resection DM
• Recurrence or progression of underlying disease ( reduction of the islet cell reserve)
• Gland atrophy
• Adjuvant chemotherapy or radiation
• The type of surgery:
– Extend of the resection (volume of resection) – loss of pancreatic parenchyma
– Neurohormonal response after resection
Post-resection DM- incidence ranging from 0% to 50%3
- 4.8 to 38% of patients after DP ( distal pancreatecomy) - 20% of the patients after pancreaticoduodenectomy
1Ewald N et al. Diabetes Met Res Rev. 2011;28: 338-42 2 Hardt PB e al. Diab. Care 2008; 31 Suppl 2: S165-169; 3 Ferrara M et al.cHBP 2013, 15: 170-174.
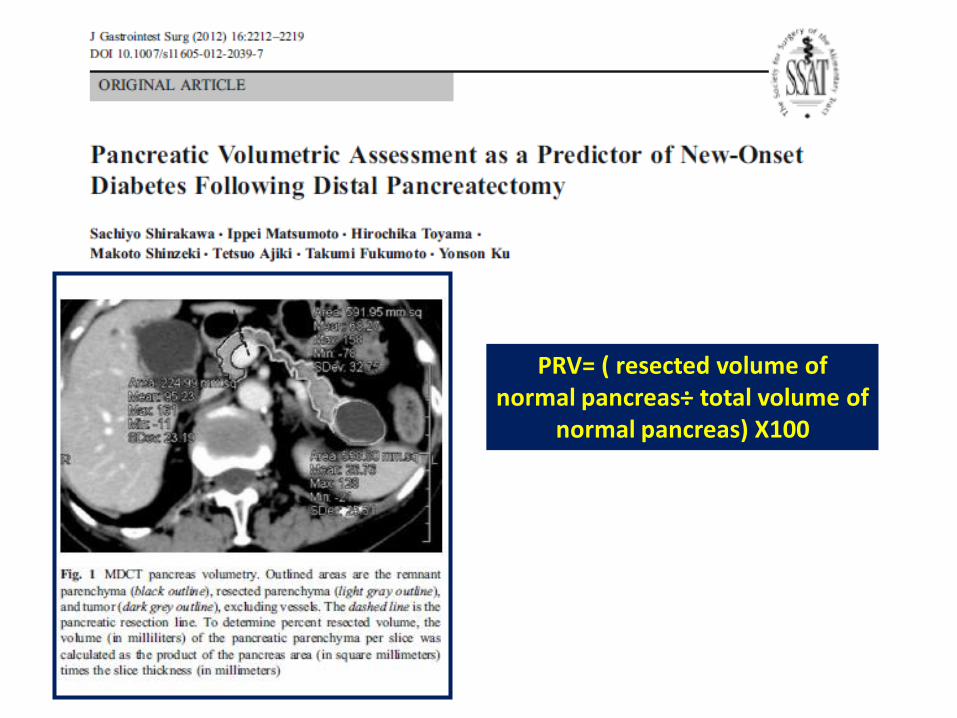
PRV= ( resected volume of normal pancreas÷ total volume of
normal pancreas) X100
The volume reduction of the pancreatic parenchyma– risk factor for diabetes The mean PRV for the new-onset groupwas 49% vs 32 % for the non-diabetic group PRV >44%- indepedent risk factor for postoperative new onset diabetes Using the PRV – offer specific information about individual risk of the postoperative DM
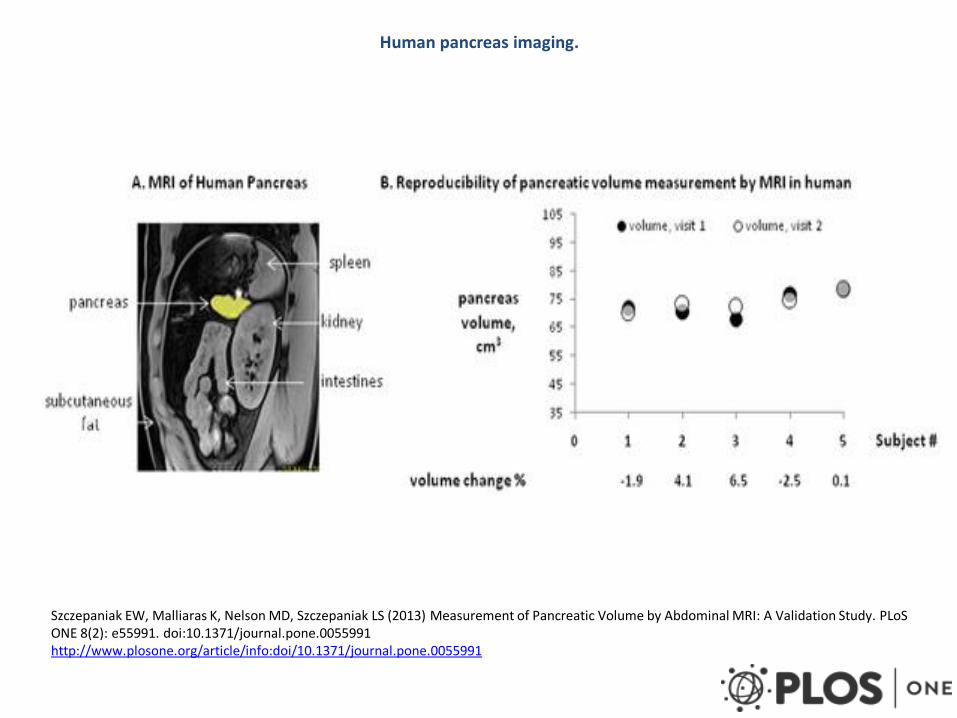
Human pancreas imaging.
Szczepaniak EW, Malliaras K, Nelson MD, Szczepaniak LS (2013) Measurement of Pancreatic Volume by Abdominal MRI: A Validation Study. PLoS ONE 8(2): e55991. doi:10.1371/journal.pone.0055991 http://www.plosone.org/article/info:doi/10.1371/journal.pone.0055991
PANCREATIC CANCER (PDAC) AND DM
Incidence of DM after pancreatic resection in PDAC
1. Distal pancreatectomy
• Between 40% to 80% of the pancreas is removed, depending on the indication for surgery- location of the tumor)1,2
• The rate of new-onset DM after DP in patients with remaining normal parenchyma is low comparative with CP- 5-9%3
1Slezak L.A. Et al. World J. Surg. 2001; 25, 452–460; 2Maeda H, Hanazaki K. Pancreatology 2011; 11:268-276 3Lillemoe KD et al. Ann Surg. 1999; 693-698; King J et al. Ann Surg 2008; 12: 1548-1553
2. Pancreticoduodenectomy (PD)
• The rate of new-onset DM after PD in patients with PDAC
• Amelioration of the diabetes state has been often observed after PD for PDAC
Incidence of DM after pancreatic resection in PDAC
Xiang Yi He et al. suggests that nearly half of newly diagnosed PDAC patients have DM.
71.1 % of these patients have new-onset DM (\2 years) and
65 % of new-onset DM are resolved post-radical resection.
Diabetogenic influence of PC
The mechanisms responsible for resolution of DM:
- Surgical resection- associated anatomical changes
Local effects: removal of the:
- diabetogenic factors secreted by the adenocarcinoma cells
- local inflammation due to obstructive lesions ( cause insuline resistance)
Menge BA et al. Diabetologia 2009; 52:306-317/ Ohtsuka T et al. Pancreas 2009; 38: 700-705
Postoperative outcome after pancreatectomy in patients with preoperative DM
The effect of preoperative DM on pancreatic fistula is cntroversial
Mathur et al. – DM offer a protective benefit against pancreatic fistula
- The patients developed pancreatic fistula were less likely to have diabetes. (p<0.05)
1,2 Mathur A. Et al. 2007 Ann Surg.
Postoperative outcome after pancreatectomy in patients with preoperative DM
• Pre-existing DM may have prognostic implications after resection for PDAC1,2
• Patients with preoperative DM – higher risk of any type of pancreatic fistula than those witout DM (10.3% vs 3,7%)
• the risk for ISGPS type B and C is similar (p=0.8)
• No significant difference in the rate of postoperative mortalities between two groups
1,2 Chu CK et al. Ann Surg. Oncol.2010; 17:502-513 / Sperti C. Br J Surg83: 625-631 3Nakata B et al. International Journal of Surgery 2013: 1-5
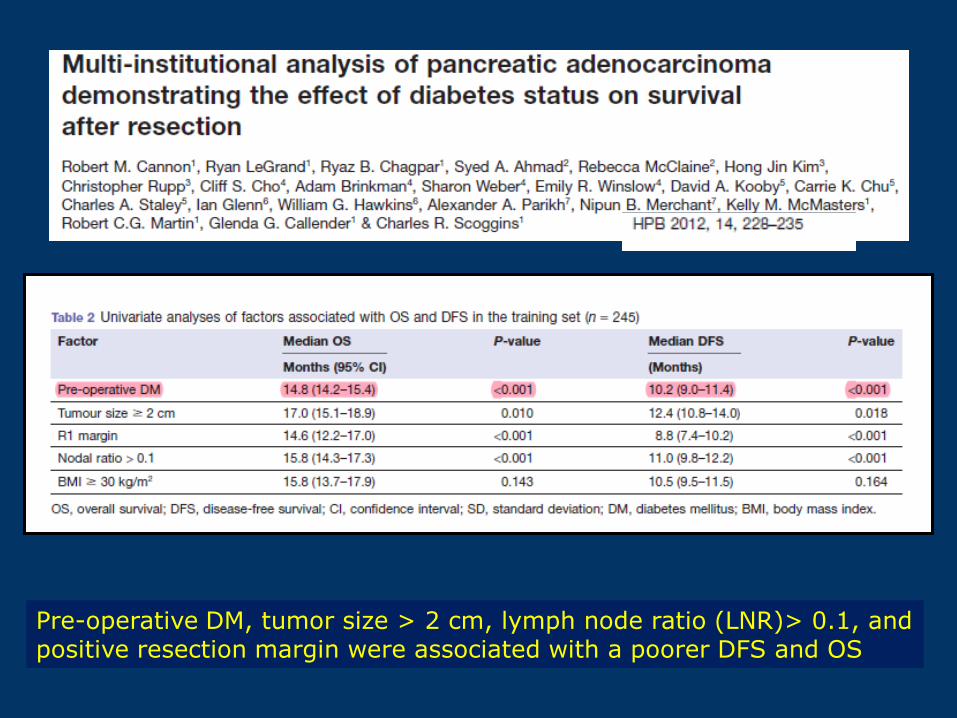
Pre-operative DM, tumor size > 2 cm, lymph node ratio (LNR)> 0.1, and positive resection margin were associated with a poorer DFS and OS

SOLUTION FOR MANAGEMENT
Management of the
1. Glycemic control
1. Treatment of additional comorbidities (maldigestion, qualitative malnutrition)
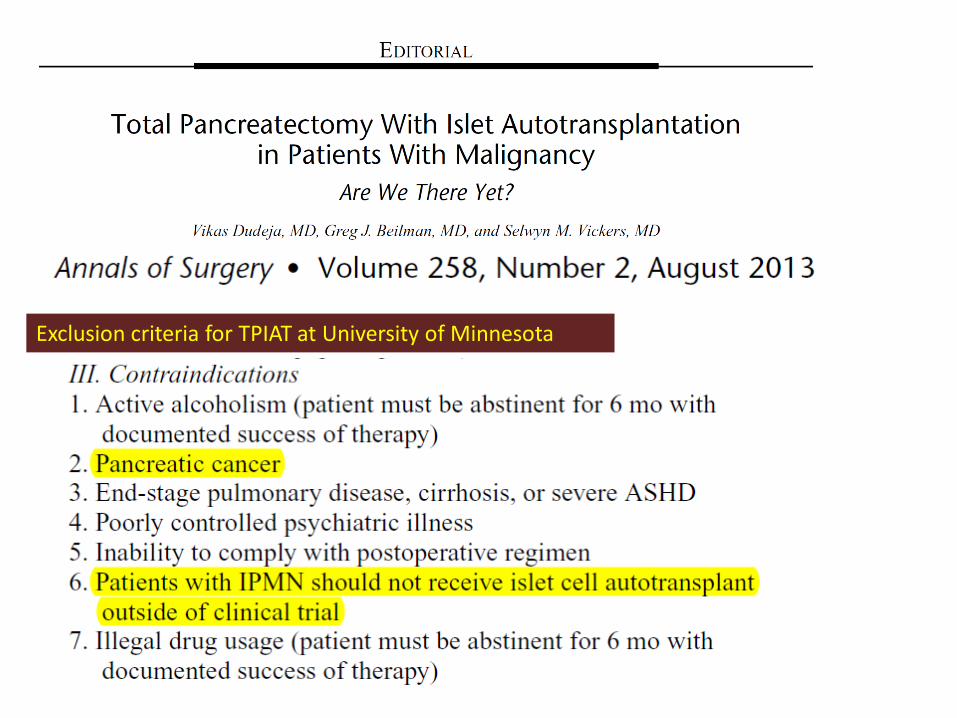
Exclusion criteria for TPIAT at University of Minnesota
Why malignancy or concern for malignancy remains a clear exclusion for TPIAT?
• The islet isolation process enriches islets, but does not totally eliminate ductal cells (cell of origin for pancreatic ductal adenocarcinoma)
• Multifocality has been described in pancreatic cancer
Concern for the use of islet preparation contaminated with ductal cells in patients with malignancy

BENIGN AND LOW GRADE MALIGNANT LESIONS AND DM
28
What is chronic pancreatitis ?
• Chronic pancreatitis is a progressive
inflammatory disease implying destroyed
secretory pancreatic parenchyma and
replacement with fibrous tissue, that could
lead to both exocrine and endocrine
insufficiency (i.e. malnutrition and
diabetes)
Braganza JM, Lancet, 2011
29
Treatment goals
• Relieve pain / prevent recurrent attacks
• Manage complications
• Correct metabolic consequences such as
diabetes or malnutrition
30
Whipple procedure - 72 patients
Pylorus preserving PD - 24 patients
Duodenum preserving pancreatic head resections in 10
patients
•Beger procedure - 6 patients
•Frey procedure – 4 patients
Distal pancreatectomy
• with splenectomy - 38 patients
• spleen preserving - 4 patients
Total pancreatectomy - 2 patients
Resection procedures: 150 between 1995 and 2008
DM after pancreatic resection in CP-Distal pancreatectomy
• For patients with CP the incidence of post-resection DM may reflect the underlying disease progression in addition to the effects of resection. 1
• 25-50% of patients with CP have risk of developing DM after DP2
1 Ferrara M et al.cHBP 2013, 15: 170-174
2Maeda H, Hanazaki K. Pancreatology 2011; 11:268-276
Hutchins RR. et al.Ann Surg. 2002;236(5):612-8
32
RESECTION in chronic pancreatitis
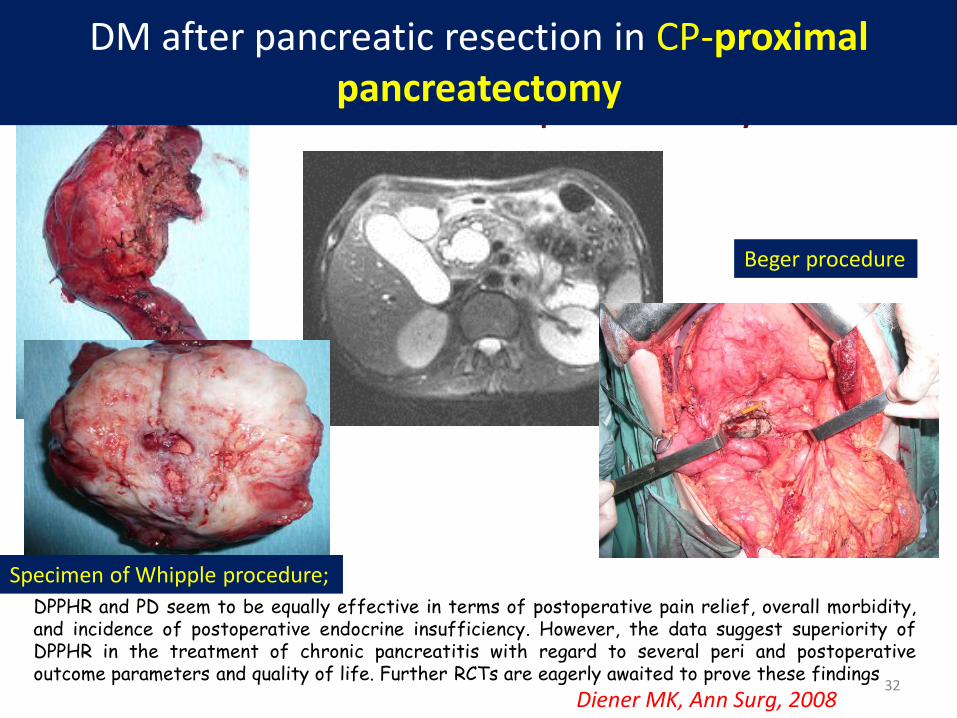
DPPHR and PD seem to be equally effective in terms of postoperative pain relief, overall morbidity, and incidence of postoperative endocrine insufficiency. However, the data suggest superiority of DPPHR in the treatment of chronic pancreatitis with regard to several peri and postoperative outcome parameters and quality of life. Further RCTs are eagerly awaited to prove these findings
Diener MK, Ann Surg, 2008
Proximal pancreatectomy
Beger procedure
Specimen of Whipple procedure;
DM after pancreatic resection in CP-proximal pancreatectomy
Proximal pancreatectomy
• Büchler et al. compared endocrine function following pylorus preserving partial pancreaticoduodenectomy or duodenum-preserving pancreatic head resection (DPPHR, or “Beger” procedure) performed for chronic pancreatitis
The observation that the DPPHR (Beger) procedure was superior to pylorus-preserving pancreaticoduodenectomy with respect to glucose metabolism suggests that preservation of the duodenum (or the pancreatic polypeptide- and insulin-containing tissue in the ventral pancreas) was responsible for improved glucose tolerance postoperatively.
Büchler et al. Am. J. Surg. 169:65, 1995; Slezak L.A. Et al. World J. Surg. 2001;
DM after pancreatic resection in CP-Distal pancreatectomy
34
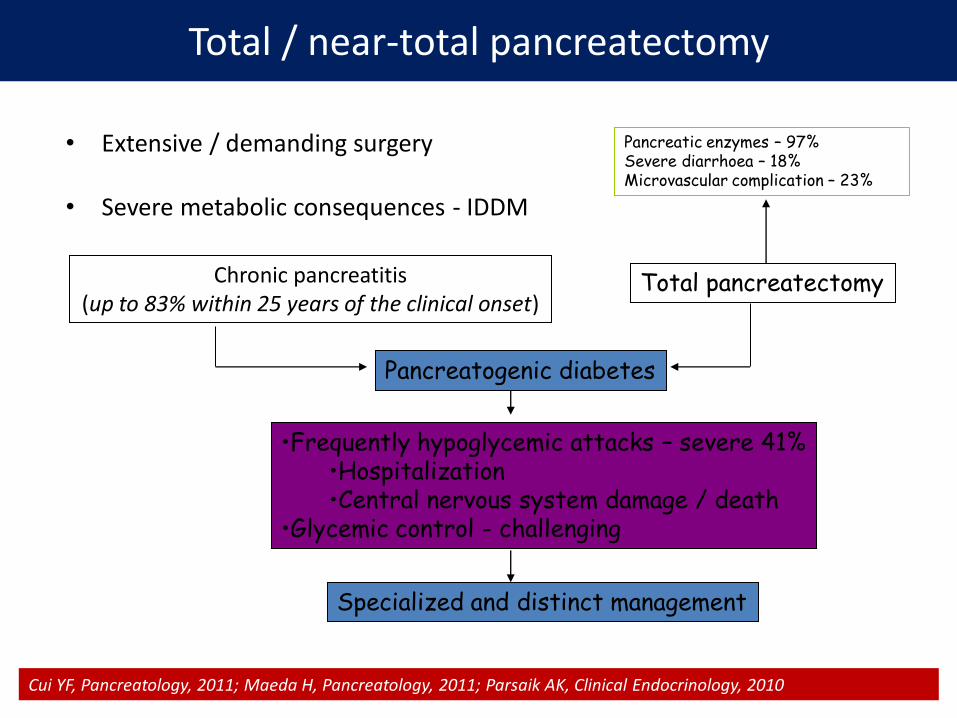
Total / near-total pancreatectomy
• Extensive / demanding surgery
• Severe metabolic consequences - IDDM
Pancreatogenic diabetes
Chronic pancreatitis (up to 83% within 25 years of the clinical onset)
Cui YF, Pancreatology, 2011; Maeda H, Pancreatology, 2011; Parsaik AK, Clinical Endocrinology, 2010
•Frequently hypoglycemic attacks – severe 41% •Hospitalization •Central nervous system damage / death
•Glycemic control - challenging
Total pancreatectomy
Specialized and distinct management
Pancreatic enzymes – 97% Severe diarrhoea – 18% Microvascular complication – 23%
35
Total pancreatectomy
Total pancreatectomy should no longer be generally avoided, because it is
a viable option in selected patients.
Mortality decreased from 22% to 3%, but hypoglycemia continues to be a problem
Parsaik AK, Clinical Endocrinology, 2010
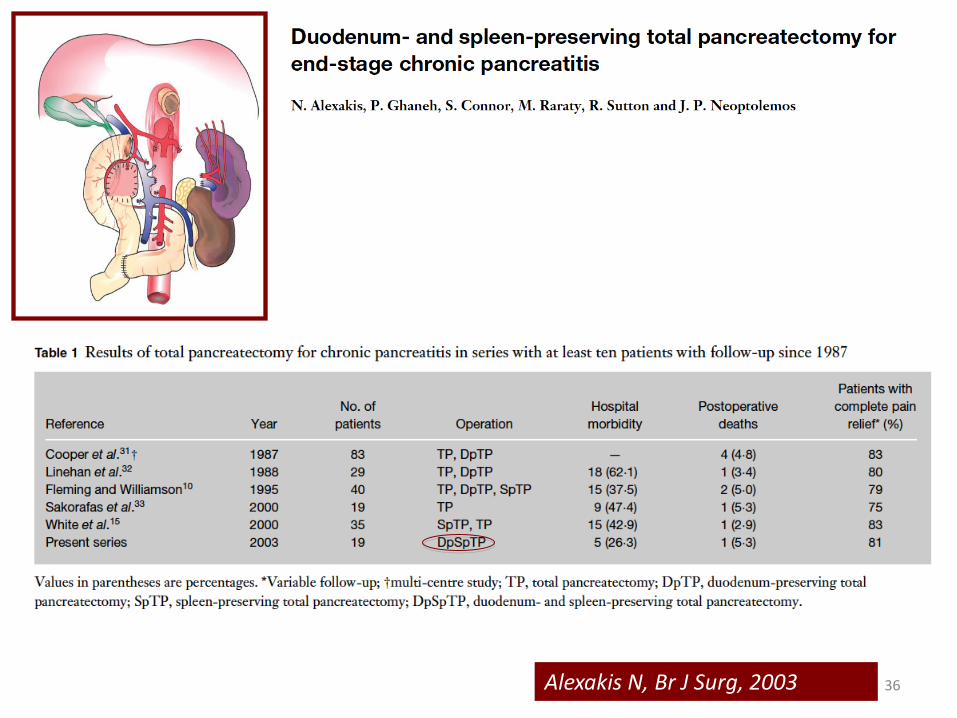
36 Alexakis N, Br J Surg, 2003
37
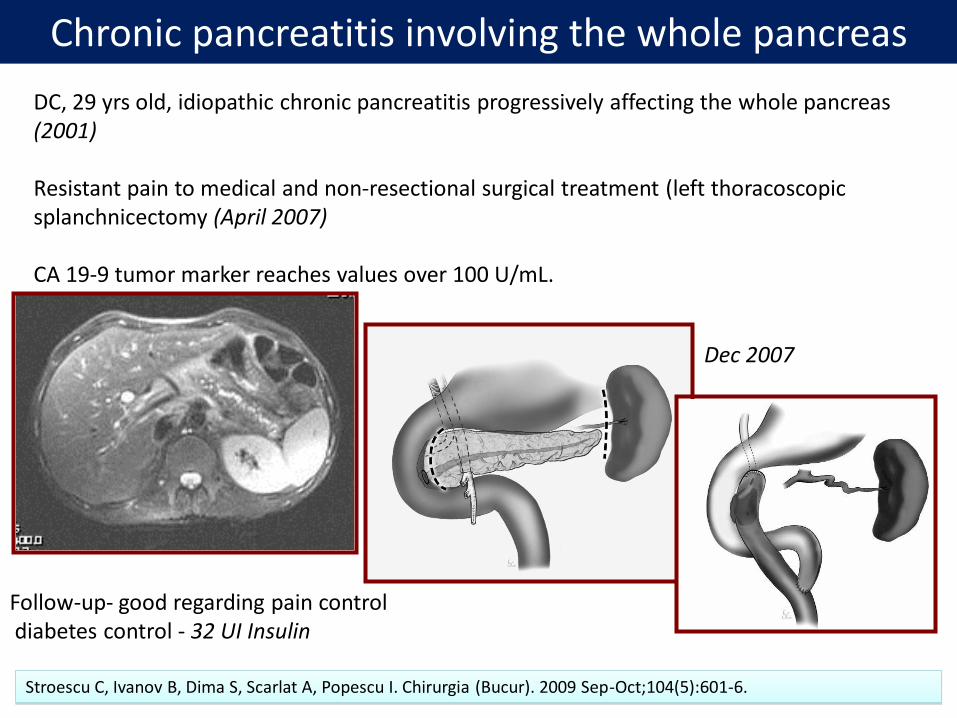
DC, 29 yrs old, idiopathic chronic pancreatitis progressively affecting the whole pancreas (2001) Resistant pain to medical and non-resectional surgical treatment (left thoracoscopic splanchnicectomy (April 2007) CA 19-9 tumor marker reaches values over 100 U/mL.
Follow-up- good regarding pain control diabetes control - 32 UI Insulin
Stroescu C, Ivanov B, Dima S, Scarlat A, Popescu I. Chirurgia (Bucur). 2009 Sep-Oct;104(5):601-6.
Chronic pancreatitis involving the whole pancreas
Dec 2007

SOLUTION FOR MANAGEMENT
-Parenchyma sparing procedures -Islet autotransplantation
Central pancreatectomy
Parenchyma sparing surgery
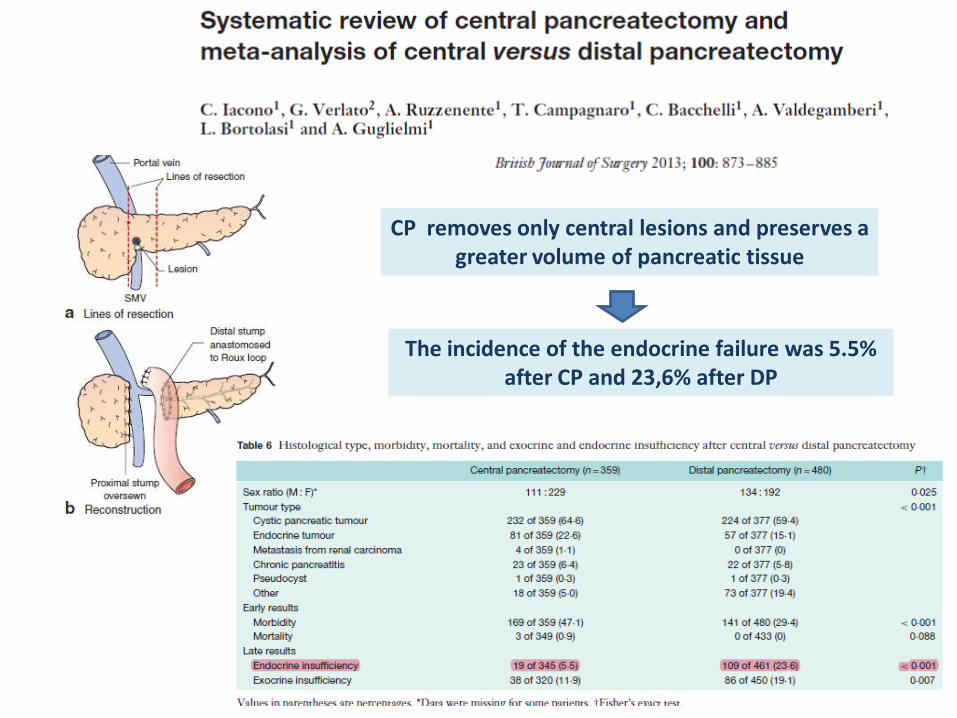
CP removes only central lesions and preserves a greater volume of pancreatic tissue
The incidence of the endocrine failure was 5.5% after CP and 23,6% after DP
42
Chronic pancreatitis - total pancreatectomy and autologus islet transplants
PAIN IDDM
TOTAL PANCREATECTOMY
AUTOLOGUS ISLET TRANSPLANTS
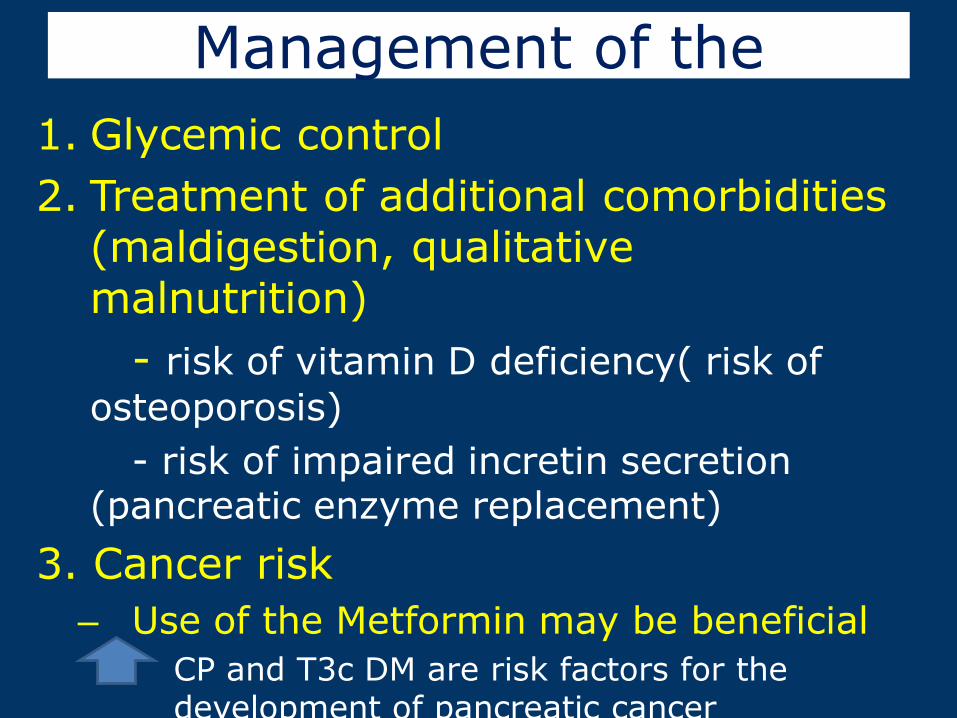
Management of the
1. Glycemic control
2. Treatment of additional comorbidities (maldigestion, qualitative malnutrition)
- risk of vitamin D deficiency( risk of
osteoporosis)
- risk of impaired incretin secretion (pancreatic enzyme replacement)
3. Cancer risk
– Use of the Metformin may be beneficial
• CP and T3c DM are risk factors for the development of pancreatic cancer
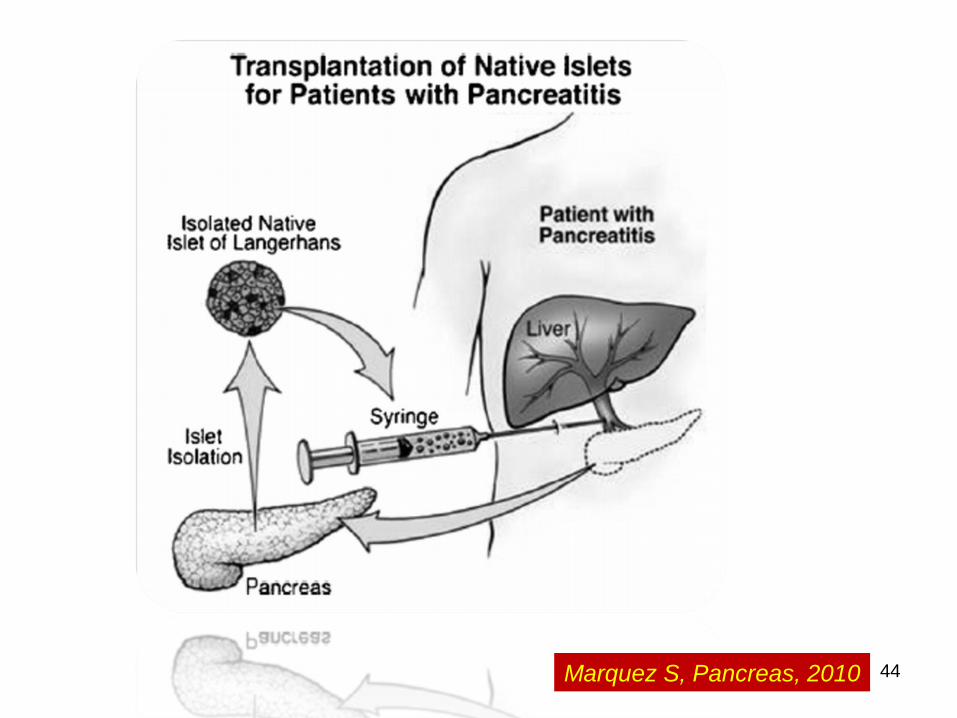
44 Marquez S, Pancreas, 2010
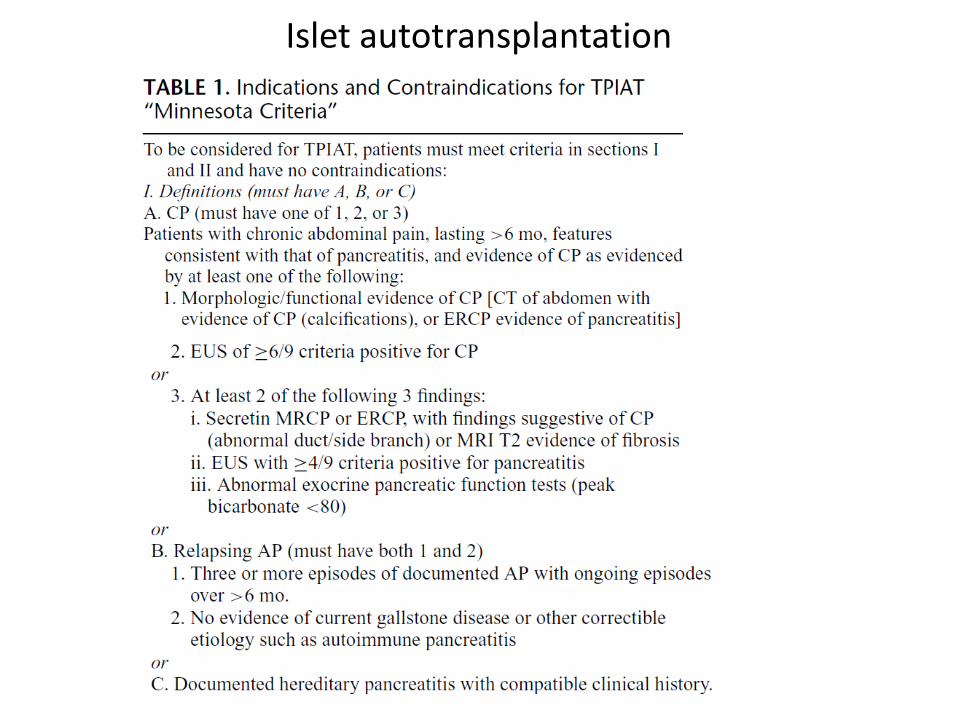
Islet autotransplantation
46
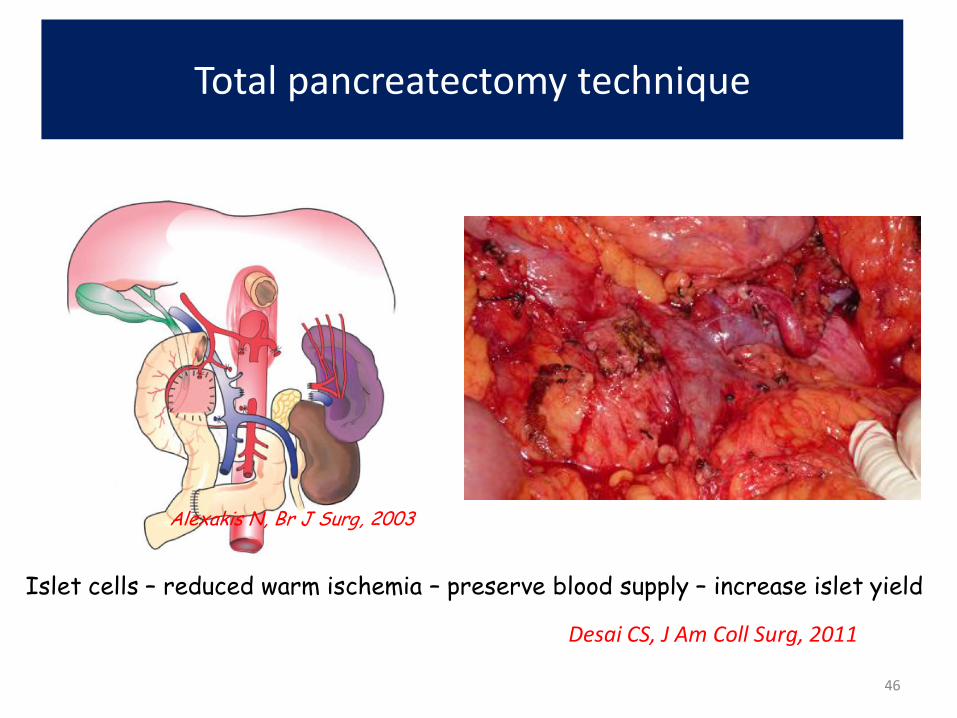
Total pancreatectomy technique
Islet cells – reduced warm ischemia – preserve blood supply – increase islet yield
Desai CS, J Am Coll Surg, 2011
Alexakis N, Br J Surg, 2003
47
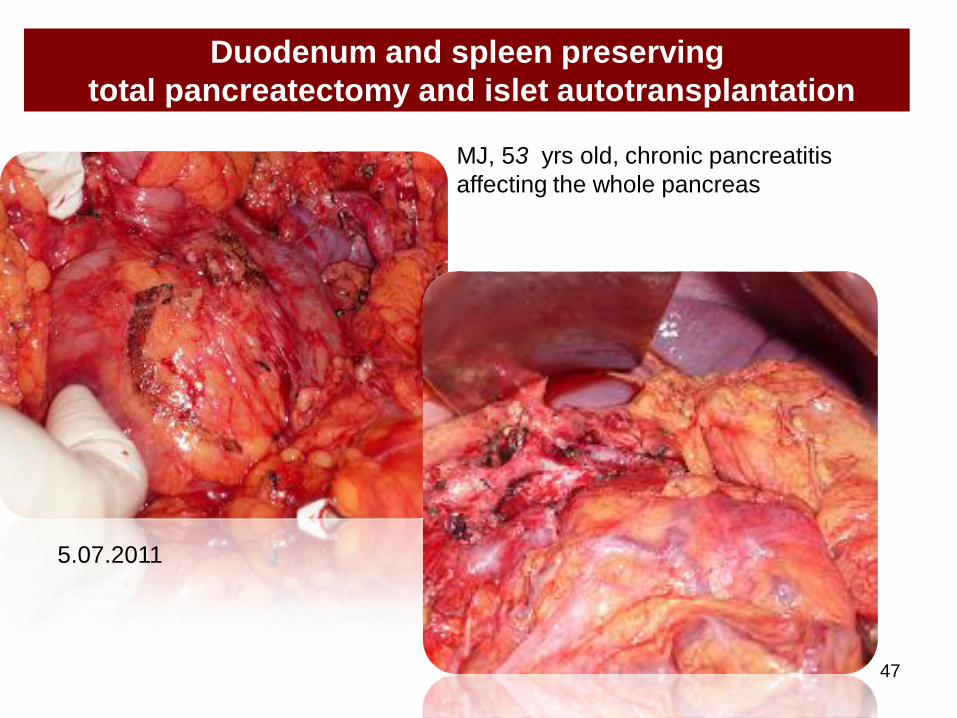
Duodenum and spleen preserving
total pancreatectomy and islet autotransplantation
5.07.2011
MJ, 53 yrs old, chronic pancreatitis
affecting the whole pancreas
48
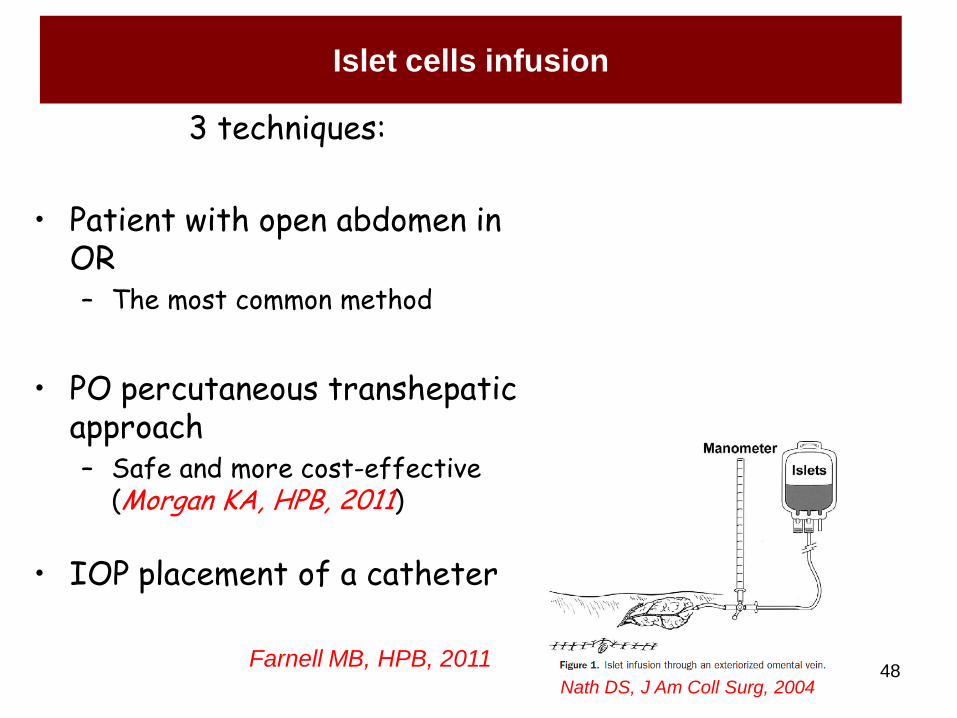
Islet cells infusion
3 techniques:
• Patient with open abdomen in OR – The most common method
• PO percutaneous transhepatic approach – Safe and more cost-effective
(Morgan KA, HPB, 2011)
• IOP placement of a catheter
Farnell MB, HPB, 2011 Nath DS, J Am Coll Surg, 2004
49
Results of total pancreatectomy and autoislet
transplant
• Complications: 6% to 42% • Ris F, Transplantation, 2011; Morgan KA, HPB, 2011; Desai CS, J Am Coll Surg, 2011
• Insulin independence: – at 1 year: 47% - 95%
• Ris F, Transplantation, 2011; Sutherland DER, Transplantation, 2008; Wahoff SC, Ann Surg, 1995
– at 10 year: 76% • Sutherland DER, Transplantation, 2008
• Pain relief in chronic pancreatitis: 82% • White SA, Am J Surg, 2000
50
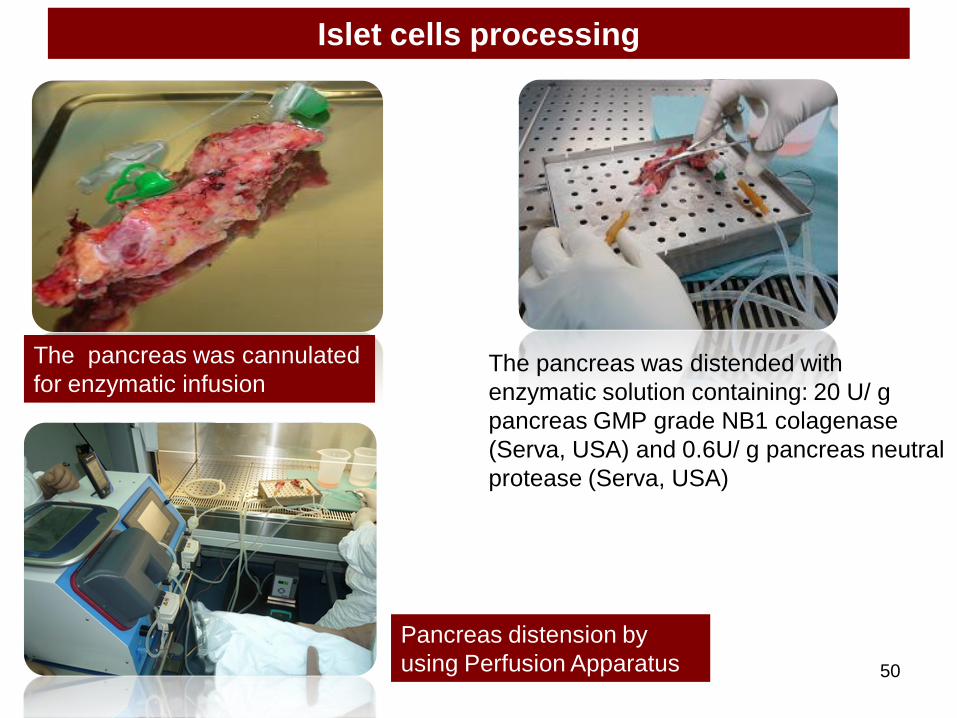
Islet cells processing
The pancreas was distended with
enzymatic solution containing: 20 U/ g
pancreas GMP grade NB1 colagenase
(Serva, USA) and 0.6U/ g pancreas neutral
protease (Serva, USA)
The pancreas was cannulated
for enzymatic infusion
Pancreas distension by
using Perfusion Apparatus
51
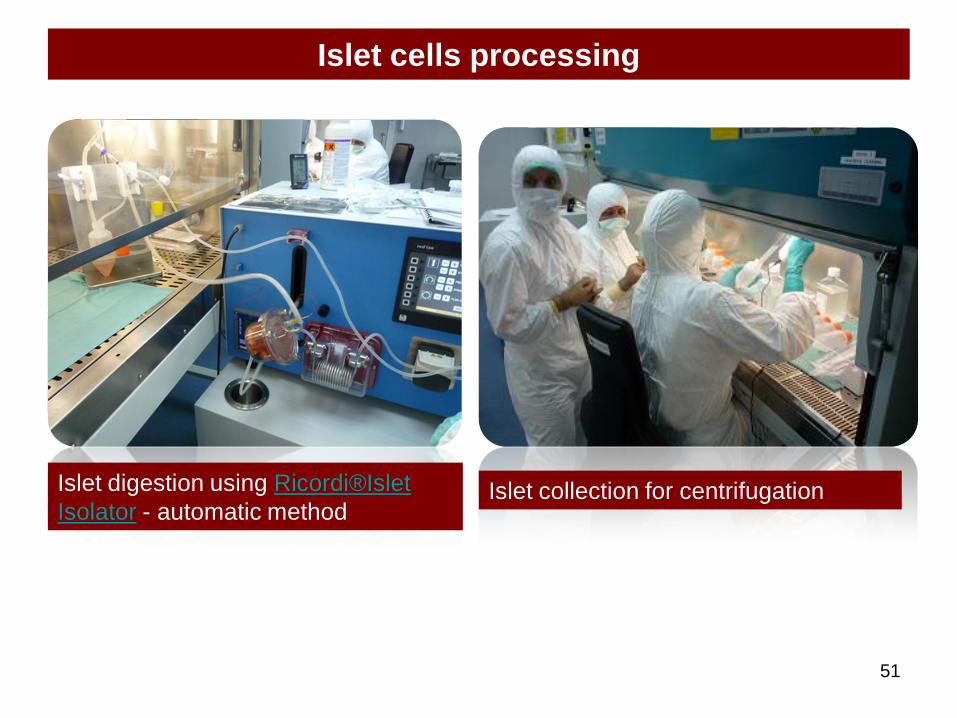
Islet cells processing
Islet digestion using Ricordi®Islet
Isolator - automatic method Islet collection for centrifugation
52
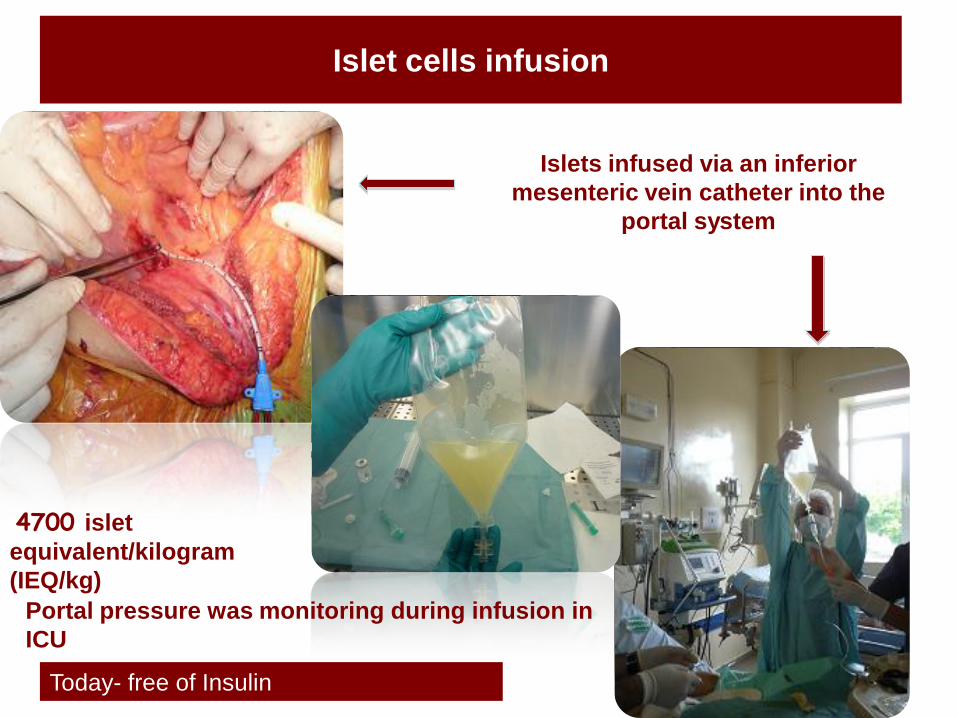
Islet cells infusion
Islets infused via an inferior
mesenteric vein catheter into the
portal system
Portal pressure was monitoring during infusion in
ICU
4700 islet
equivalent/kilogram
(IEQ/kg)
Today- free of Insulin
Conclusions
53
- the postoperative incidence of diabetes is directly
related to the extent of the pancreatic resection
- those patients who require only distal pancreatectomy or
limited excavation of the pancreatic head develop diabetes
far less frequently than those who require
pancreaticoduodenectomy or near-total or total
pancreatectomy