Embed Size (px)
Citation preview
AD-A 191I654 FILL Wp C
AD-A191 654 USAARL Report No. 87-13
Dark Adaptation and Recoveryfrom Light Adaptation:
Smokers versus Nonsmokers
By
Roger W. Wiley DTICSELECTE: P-MAR2 4I
Sensory Research DivisionVisual Sciences Branch
September 1987
Approvsd for public release; distribution unlimited.
88 3 22 070A A % W"
NOTICE
Qualified Requesters
Qualified requesters may obtain copies from the Defense TechnicalInformation Center, Cameron Station, Alexandria, Virginia, 22314.Orders will be expedited if placed through the librarian or other persondesignated to request documents from the Defense Technical InformationCenter.
Change of Address
Organizations receiving reports from the U.S. Army AeromedicalResearch Laboratory on automatic mailing lists should confirm correctaddress when corresponding about laboratory reports.
Disposition
Destroy this report when it is no longer needed. Do not return itto the originator.
Di scl aimer
The views, opinions, and/or findings contained in this report arethose of the authors and should not be construed as an official Departmentof the Army position, policy, or decision, unless so designated by otherofficial documentation. Citation of trade names in this report does notconstitute an official Department of the Army endorsement or approval ofthe use of such commercial items.
Human Use
Human subjects participated in these studies after giving free andinformed voluntary consent. Investigators adhered to AR 70-25 andUSAMRDC Reg 70-25 on Use of Volunteers in Research.
Reviewed:
BRUCE C. LEIBRECHT, Ph.D.LTC, MSDirector, Sensory Research Division
j~r D. LaMbTHE rhD. DUDLEY R. P CE
COL, MS Colonel, M7Chairman, Scientific Review Commanding
Committee
!_
UNCLASSIFIED
SECURITY CLASSIFICATION OF THIS PAGE"Form Appoved
REPORT DOCUMENTATION PAGE OMB No. O4.0 In
Ia. REPORT SECURITY CLASSIFICATIONb lb RESTRICTIVE MARKINGSUnclassified
2a. SECURITY CLASSIFICATION AUTHORITY 3, DISTRIBUTION /AVAILABILITY OF REPORT
2b. DECLASSIFICATION / DOWNGRAC.ING SCI-EDULE
4. PERFORMING ORGANIZATION REPORT NUMBER(S) 5. MONITORING ORGANIZATION REPORT NUMBER(S)
USAARL Report: No. 87-13
(a. NAME OF PERFORMING ORGANIZATION 6b. OFFICE SYMBOL 7a. NAME OF MONITORING ORGANIZATIONU.S. Army Aeromedical Research (If applicable) U.S. Army Medical Research andLaboratory SGRD-UAS-VS Development Command
16c. ADDRESS (City, State, and ZIPCode) 7b. ADDRESS (City, State, and ZIP Code)
P.O. Box 577 Ft. DetrickFt. Rucker, AL 36362-5292 Frederick, MD 21701-5012
Ba. NAME OF FUNDING /SPONSORING 18b. OFFICE SYMBOL 9. PROCUREMENT INSTRUMENT IDENTIFICATION NUMBERORGANIZATION (If applicable)
Sc. ADDRESS (City, State, and ZIP Code) 10. SOURCE OF FUNDING NUMBERSPROGRAM PROJECT A TASK WORK UNITELEMENT NO. NO. NO. CCESSION NO.
I 62777A 3EI62777A871 BG 16411. TITLE (Include Security Classification)
Dark Adaptation and Recovery from Light Adaptation: Smokers Versus Non-Smokers12. PERSONAL AUTHOR(S)
Roger W. Wiley13a. TYPE OF REPORT 13b. TIME COVERED 14. DATE OF REPORT (Year, Mc. nth,Dy) 15. PAGE COUNT
FROM TO September 1967 2516. SUPPLEMENTARY NOTATION
17. COSATI CODES 18. SUBJECT TERMS (Continue on reverse if nereuarry an identify& by block number)FIELD GROUP SUB-GROUP
06/041"7- 09/0519,"'BSTRACT (Continue on reverse if necessary and identify by block number)
`-Since the published data concerning the effects of smoking on visual sensitivity atnight are inconsistent, a new study was initiated to investigate this question. ThirtyArmy aviators between the ages of 19 and 39 volunteered to participate in this study. Ofthese subjects, 15 smoked and 15 were non-smokers. Each subject was seated in a light-controlled room and exposed to a standardized bright light for 5 minutes. Immediatelyafter the bright light was extinguished, the subject's visual sensitivity was tested bygradually increasing the intensity of a test light until the subject could see it. This
- was continued over a period of 35 minutes by which time the subjects had reached theirmaximum light sensitivity. Each subject then wore a pair of AN/PVS-5 Night Vision Gogglesfor 5 minutes after which his visual sensitivity again was tested for 20 minutes. Our datado not show any differences in visual sensitivity between aviators who smoke and those whodo not smoke. Blood samples were analyzed to compare serum levels of nicotine, cotinineand carboxyhemoglobin with the visudl data. Again, no correlation exists between, ,,
20. DISTRIBUTION /AVAILABILITY OF ABSTRACT 21. ABSTRACT SECURITY CLASSIFICATION0 UNCLASSIFIED/UNLIMITED [3 SAME AS RPT. 0 DTIC USERS
22a. NAME OF RESPONSIBLE INDIVIDUAL 22b. TELEPHONE (Include Area Code) 22c. OFFICE SYMBOLR2aeI W. Wilev (205) 255-6810 SGRD-UAS-VS00 Form 1473, JUN 86 Previous edtions are obsolete. SECJRITY CLASSIFICATION OF THIS PAGE
OD~orn 173.
19. ABSTRACT Continued
sensitivity and blood measures related to smoking. Aviators who smoke reach the samelevel of sensitivity to light as non-smokers and they do so in the same amolnt of time.Visuel recovery after wearing the Night Vision Goggles also followed the same timecourse regardless of smoking history The conclusion from these data is that lightsensitivity, the ability to see the mmest lights at night, is independent of smokinghi story.
I~o*
Table of Contents
Introduction . . . . . . . . . . . . . . . . . . .. . 3
Materials and methods . . . . . . . . . . . . . . . . .. 4
Results. .. . .a * e - e * * . .*. . . .% a .e. * * a * 6
Discussion . . . . . . . . . . . . .. . . . . . . * 6 0 10
Conclusions . . . . . . . . . . . . . . . 12
References . . . . . . . . . . . . . . . . . . 13
Accesir," For
NTIS CRA&IDTIC TABUriannounced -
ByJ..... ..................Distr ibu tion I
Avaitsbl~ity CodesAv•il ao•dor
Dist Special
This page left blank intentionally.
Introduction
The possible biological effects of smoking tobacco productshave been studied intensively from a variety of differentaspects. However, despite many efforts, the reported changes invisual sensory functions are inconsistent. The earlier reportsindicated subjects who smoke cigarettes demonstrated reducedvisual thresholds. For example, McFarland and coworkers (1944,1953, 1970) reported a loss in visual sensitivity associated withsmoking cigarettes. They used, as a measure of visualsensitivity, discrimination thresholds, i.e., the ability todetect light stimuli presented against backgrounds of variousbrightnesses. These authors stated that they could detect achange in the discrimination threshold if the subject smoked justone cigarette. Since no change in threshold was reported if thesubjects did not inhale the smoke, the authors concluded thatcarboxyhemoglobin saturation was the cause of reduced visualsensitivity. They reached this conclusion after considering thatnicotine still reaches the blood even without inhaling the smokewhile carboxyhemoglobin saturation is not present withoutinhalation. In partial support of this conclusion, Sheard (1946)reportad that the immediate effect of inhaling smoke was areduction of from 0.25 to 0.75 log units in absolute lightsensitivity. However, he ascribed his results to nicotine sincehis data indicated no effect if the nicotine was filtered fromthe smoke. These early reports have not remained unchallenged.
In contrast to the previous reports, Troemel, Davis andHendley (1951) found that nicotins actually facilitated thecourse of dark adaptation in their subjects. Johansson andJansson (1964) used a visual discrimination threshold and arepeated measures design to assess smoking effects and failed toshow any change in thresholds after their subjects smokedcigarettes. Calissendorff (1977) also used a repeated measuresdesign and reported a slight reduction in mesopic, but notscotopic, light sensitivity when measured after his subjectssmoked cigarettes. Durazzini, Zazo, and Bertoni (1975) attemptedto correlate the presence of thiocyanates in the urine secondaryto smoking with several measures of visual function. Theseauthors reported about half of their subjects demonstrated areduction in absolute visual sensitivity thresholds after smokingcigarettes. In comparison to these investigations which haveaddressed primarily scotopic or mesopic function, Fine andKobrick (1987) studied the effects of smoking on visual contrastsensitivity which is primarily subserved by the photopic system.No differences in contrast sensitivity were found in their testsubjects pre- and postcigarette smoking. However, habitualsmokers had slightly lower contrast sensitivities to certainspatial frequencies.
3
While many of the above investigations have used only alimited number of subjects or examined either the scotopic orphotopic system using psychophysical procedures, Luria and McKay(1979a, b) used both psychophysical and eleotrophysiologicaltechniques to assess the effects of carbon monoxide exposure onsmokers and nonsmokers. Using age-matched subjects (40 smokersand 40 nonsmokers), they tested scotopio sensitivity, reactiontime, color vision, visually evoked cortical potentials, andEEGs. As a group, the smokers had a poorer scotopic sensitivityscore and a slower reaction time. The remaining tests in theirbattery did not show any differences between the two groups,Further, their results did not demonstrate any trends to indicatethat a history of smoking caused a cumulative decrement in visualsensory function.
There is a growing body of evidence to indicate that smokin2cigarettes can cause many different physical infirmities (USSurgeon General Report, 1979). However, the effects of smokingon visual sensory function are equivocal. A review of thepublished evidence presents a confusing picture. Cigarettesmoking does, or possibly does not, cause a change in visualperceptual processes; if visual processes are changed, they mightbe enhanced or reduced. Finally, if a change occurs, thephotopic, mesopic, and/or sootopic systems might be affected.
The objective of the present investigation is to determineif there are changes in scotopic sensitivity and its recoverywhich possibly could be attributable to chronic tolacco use. Toassess this, we measured absolute scotopic sensitivity usingstandardized clinical testing procedures in a group of Armyaviators who smoke cigarettes and compared those results with anage-matched group of aviators who do not smoke. Additional datawere obtained to determine if differences exist between the twogroups in recovery of absolute scotopic sensitivity after viewinga military electro-optical device (AN/PVS-5 night visiongoggles).
Materials and methods
Subjects
Thirty Army aviator volunteers served as subjects for thisstudy. Of these, 15 subjects did not smoke or use any tobaccoproducts and 15 smoked cigarettes. All among the smoking grouphad smcked for more than I year with 11 of them having smoked formore than 10 years. Daily usage ranged from about 10 cigarettesto more than 40. The ages among the smokers ranged between 28and 38 years (mean = 32.87 years) and among the nonsmokersbetween 19 and 39 years (mean = 30.20 years).
4
Procedures
Since the purpose of this study was to investigate thecumulative rather than immediate effects of cigarettes, noattempt was made to control the subjects' mucking prior to datacollection. However, the testing procedures requiredapproximately 2 hours during which the subjects were not allowedto smoke. The testing schedule required complete data collectionon two subjects daily, and subjects from the smoking andnonsmoking groups were interspersed.
An identical test procedure was followed on every subject.When the individual arrived at the laboratory, he was thoroughlybriefed on the purpose of the experiment and trained on theobservations required of him. He then sat in a dimly illuminatedroom (5.12 footcandles) for 5 minutes. Following this period,all lights were extinquished in the specially prepared dark roomand the subject remained in the dark for 3 minutes. During thistime, his left eye was occluded, and he positioned himselfcomfortably in front of the hemispherical gansfeld of a clinicalGoldmann/Weekers Adaptometer. The instrument then was turned onand the subject was light adapted by staring at the uniformlyilluminated hemisphere having a brightness of 312 footlamberts.In accordance with standard clinical testing procedure, thisperiod of light adaptation lasted for 5 minutes, after which thehemisphere lighting was extinguished and the fixation lightbecame visible. Testing light sensitivity thresholds startedimmediately.
An ascending method of limits was used to measure thethreshold with the subject indicating when the test stimulusbecame visible by tapping on the instrument table. The angularsubtense of the test stimulus was 10 degrees and it stimulated aportion of the retina --pproximatley 10 degrees below the fovea.During the first 15 minutes of dark adaptation, the threshold wasmeasured every 15 seconds. Measurements were made every 30seconds during the remainder of the 35 minutes.
After completing the 35 minutes of threshold testing, thesubject donned a pair of AN/PVS-5 night vision goggles (NVOs).He was instructed simply to observe objects in the darkened testroom using the infra-red source incorporated into the NVGs toilluminate them. The goggle output tubes provide a brightness of0.098 footlambert and the subject was exposed to this- brightnessfor 5 minutes. Following the 5 minute NVG exposure, the subjectimmediately positioned himself in the Dark Adaptometer again andthreshold testing was resumed for an additional 20 minutes toassess the speed with which he recovered his absolutesensitivity.
When the psychophysical testing had been completed, the
5
subject was allowed to light adapt and a medical technician,using standard medical laboratory techniqut, took two venousbluod samples. A 15 ml sample was forwarded to the AlabamaReference Laboratory which had been contracted to analyse eachsample for nicotine and cotinine levels. A 7 ml sample wasanalyzed immediately to determine the percentage ofcarboxyhemoglobin (COHb).
Results
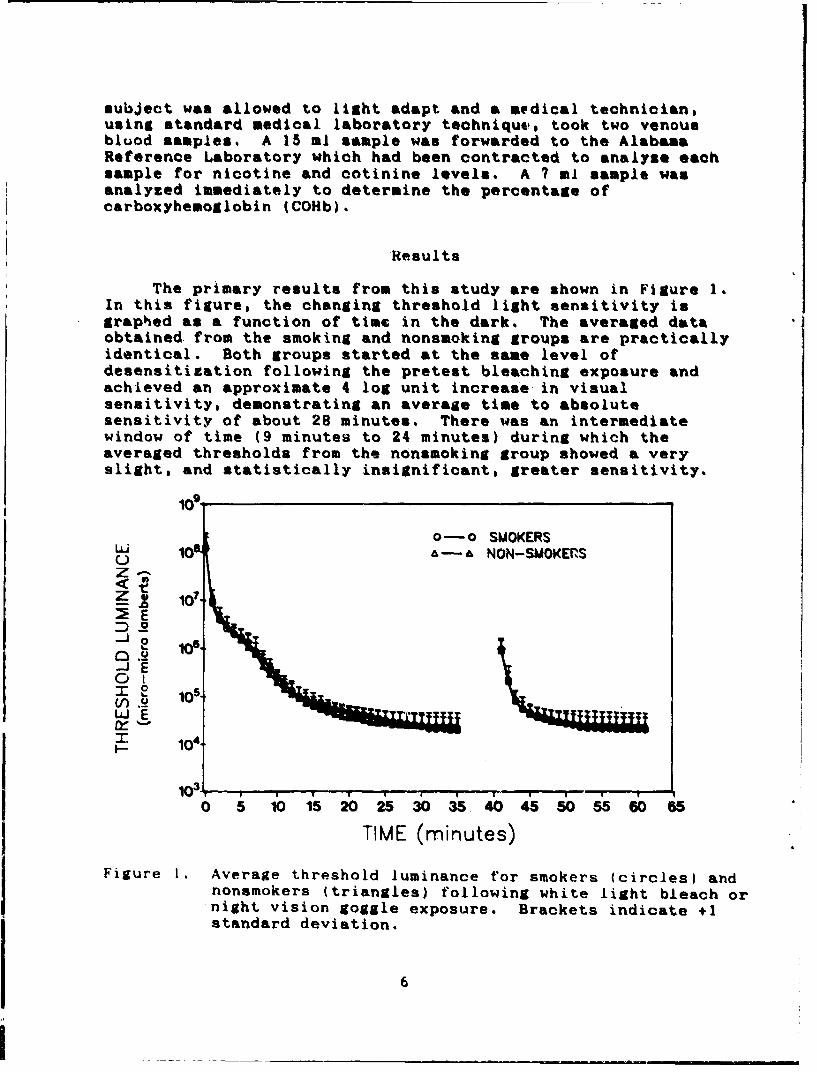
The primary results from this study are shown in Figure 1.In this figure, the changing threshold light sensitivity isgraphed as a function of time in the dark. The averaged dataobtained from the smoking and nonsmoking groups are practicallyidentical. Both groups started at the same level ofdesensitization following the pretest bleaching exposure andachieved an approximate 4 log unit increase in visualsensitivity, demonstrating an average time to absolutesensitivity of about 28 minutes. There was an intermediatewindow of time (9 minutes to 24 minutes) during which theaveraged thresholds from the nonsmoking group showed a veryslight, and statistically insignificant, greater sensitivity.
0-0 SMOKERS
S10a && • NON-SMOKERSZ•
•E0 .zz o
SE
104"
05 1 ,0 1 202 5 30' 35, 40 45 50 556.5
TIME (minutes)
Figure 1. Average threshold luminance for smokers (circles) andnonsmokers (triangles) following white light bleach ornight vision goggle exposure. Brackets indicate +1standard deviation.
6
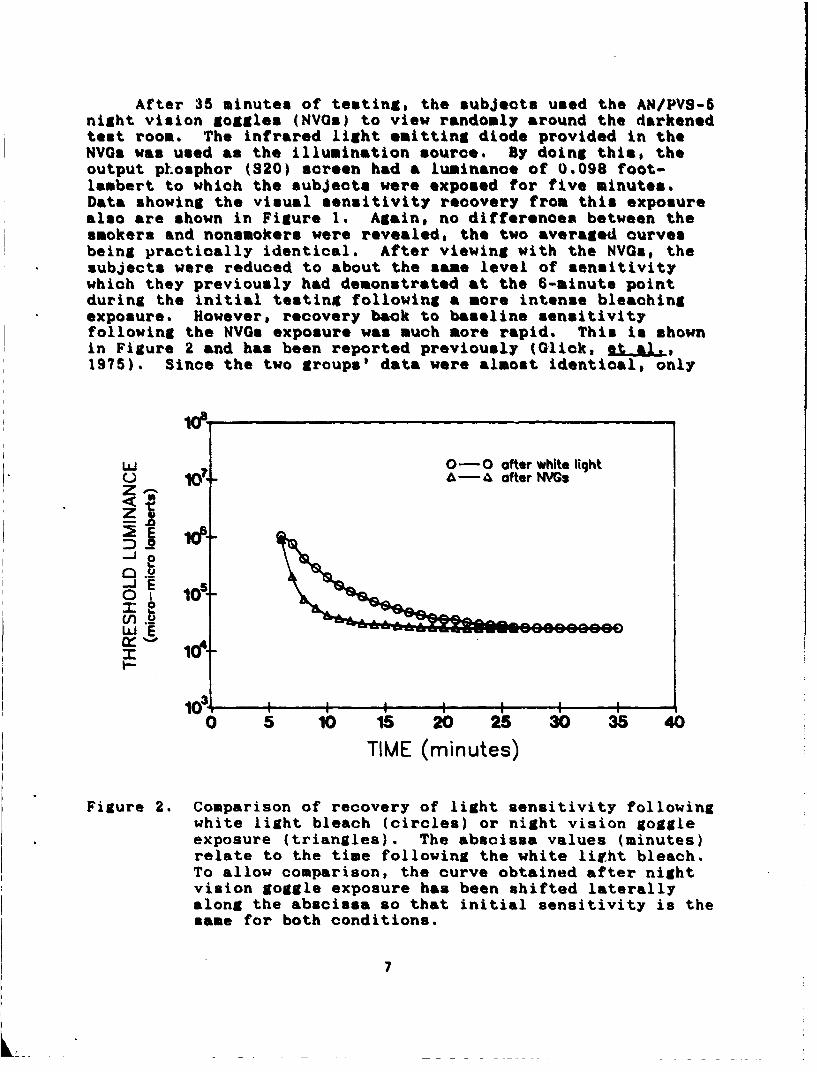
After 35 minutes of testing, the subjects used the AN/PVS-5night vision goggles (NVQs) to view randomly around the darkenedtest room. The infrared light emitting diode provided in theNVGs was used as the illumination source. By doing this, theoutput phosphor (S20) screen had a luminance of 0.098 foot-lambert to which the subjects were exposed for five minutes.Data showing the visual sensitivity recovery from this exposurealso are shown in Figure 1. Again, no differences between thesmokers and nonsmokers were revealed, the two averaged curvesbeing practically identical. After viewing with the NVOs, thesubjects were reduced to about the same level of sensitivitywhich they previously had demonstrated at the 6-minute pointduring the initial testing following a more intense bleachingexposure. However, recovery back to baseline sensitivityfollowing the NVGs exposure was much more rapid. This is shownin Figure 2 and has been reported previously (Glick, et al.,1975). Since the two groups' data were almost identical, only
W 0- 0 ofter white lightU A-A ofter NVGZ•
.2
WE
10 1 i 1 i0 5 10 15 20 25 30 35 40
TIME (minutes)
Figure 2. Comparison of recovery of light sensitivity followingwhite light bleach (circles) or night vision goggleexposure (triangles). The abscissa values (minutes)relate to the time following the white litht bleach.To allow comparison, the curve obtained after nightvision goggle exposure has been shifted laterallyalong the abscissa so that initial sensitivity is thesloe for both conditions.
7
the smokers' data are shown. In Figure 2p the initial thresholddata are plotted from 6 minutes until 32 minutes. As statedpreviously# maximum sensitivity was reached by the 28th iinute oftesting. For comparison, the threshold recovery data followingexposure with the NVYs also are shown in the figure. In thislatter condition, threshold recovery is much more rapid,approaching the maximum sensitivity within 5 minutes afterremoving the NVYs.
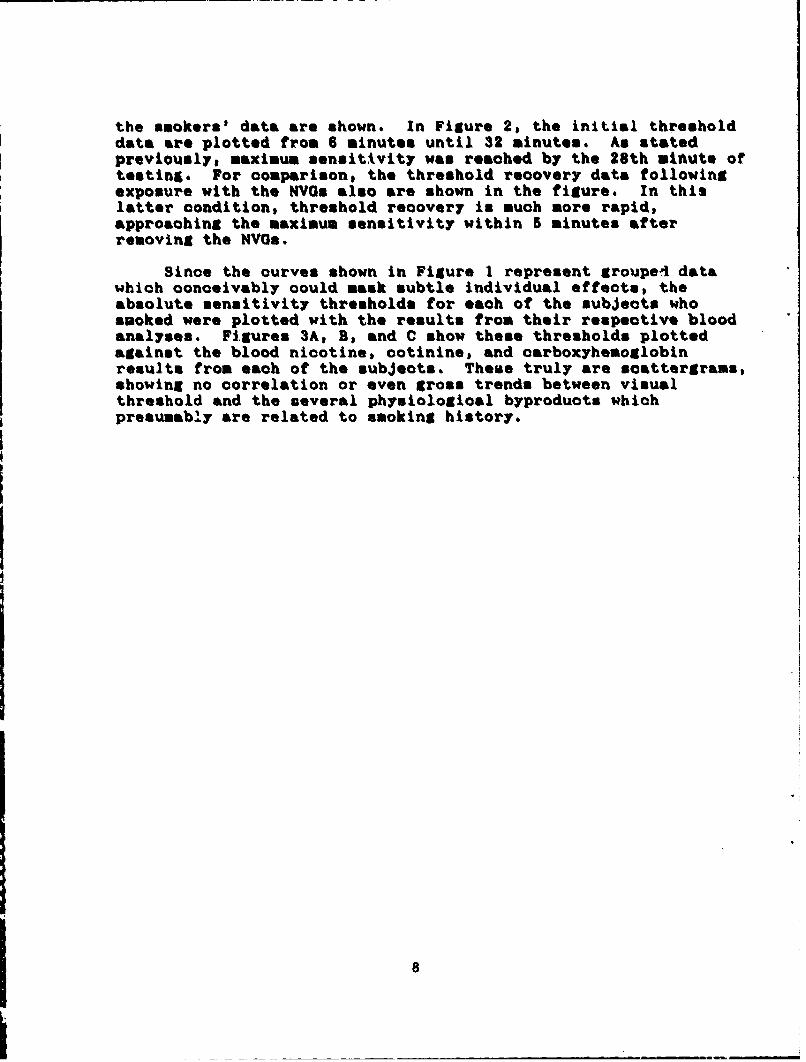
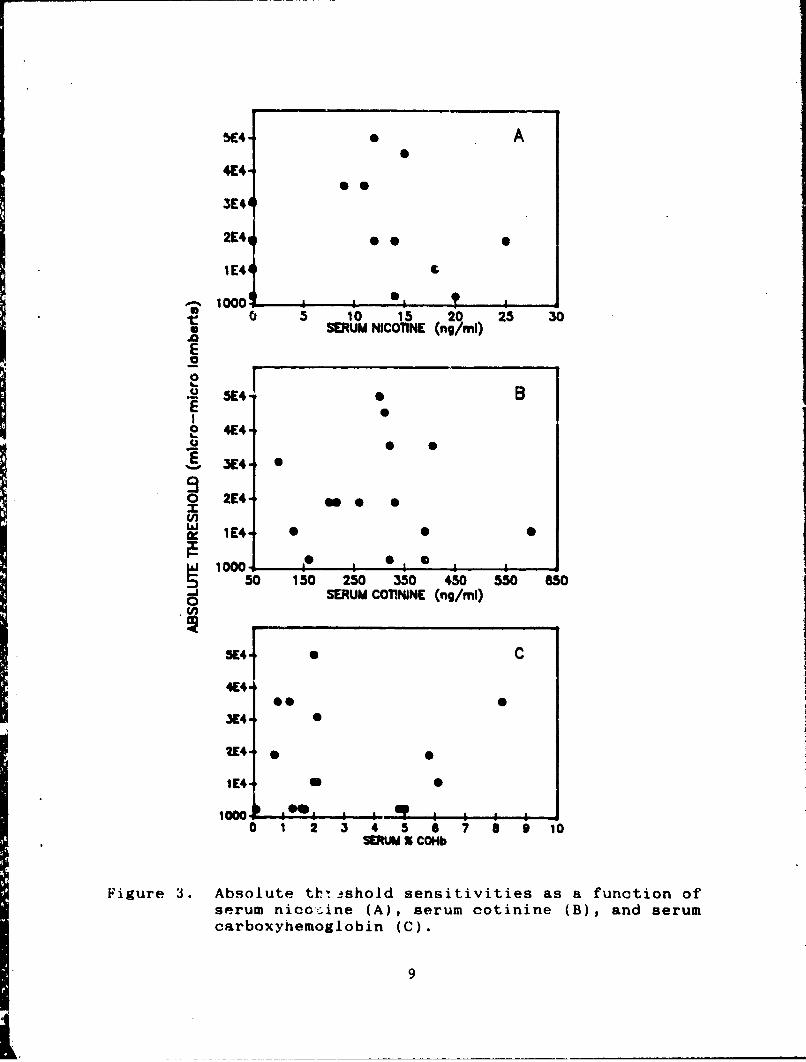
Since the curves shown in Figure 1 represent groupel datawhich conceivably could mask subtle individual effects, theabsolute sensitivity thresholds for each of the subjects whosmoked were plotted with the results from their respective bloodanalyses. Figures 3A, B, and C show these thresholds plottedagainst the blood nicotine, cotinine, and carboxyhemoglobinresults from each of the subjects. These truly are scattergrams,showing no correlation or even gross trends between visualthreshold and the several physiological byproducts whichpresumably are related to smoking history.
8
SE4 A
4E4-
3E4
2E4
1E4
__1000' I *I0 3 10 15 20 25 30
SEUM NICOTINE (ng/ml)
SE0. E
xI2 !4
S2E4-o
100 0 250 350 450 550 650
SERUM COTININE (ng/ml)
3E4 S C
4E41
3E4-
2E4*
1E4 U S
100010 1 2 3 4 5 6 7 8 9 10
SERUM X COHb
Figure 3. Absolute thtishold sensitivities as a function ofserum nico-ine (A), serum cotinine (B), and serumcarboxyhemoglobin (C).
9
Discussion
The impetus for this investigation has been provided byconsiderations at the Department of the Army staff level tobroaden the restrictions on smoking among Army aviators. Atpresent, smoking is not allowed in Army aircraft during flight.A further restriction under consideration would be to not allowany smoking by Army aviators at any time, both off ioial andpersonal. By this restriction, smoking tobacco could be thebasis for nonselection for aviation training or removal fromflight status if already rated.
A restriction on tobacco products would significantly impactthe personal lives and professional careers of the affectedaviators. Such a restriction should not be taken precipitouslywithout clear indications that the use of tobacco productsnegatively affect military performance or endanger missionaccomplishment. There are many precedents for prohibition basedupon potentially compromising performance. Almost simultaneouswith the dawn of aviation, the use of alcohol along with or priorto operating an aircraft has been forbidden. However, theadverse sensory and motor effects of alcohol are well-documented(Collins, et al., 1987). That is not the case with tobacco. Asdiscussed previously, the visual sensory effects of tobacco arecontradictory. Several investigations have reported a reductionin absolute light sensitivity with smoking while others havefailed to show any change in threshold or even showed afacilitation. Among the investigations which have reported avisual change, the visual change has been variously photopic,mesopic, or scotopic and the effect has been attributed tonicotine or carboxyhemoglobin.
The results from the present investigation which are shownin Figure 1 support previous reports of no change in visualthreshold secondary to tobacco use. The average sensitivityprofiles are practically identical over the course of darkadaptation for the two test groups. 1n addition, exposure by theAN/PVS-5 NVGs subsequent to reaching absolute light sensitivitycaused the same average visual desensitization in the smoking andnon-smoking groups and the measured recovery of sensitivityoccurred at the same rate. The data shown in Figure 2 aresimilar to comparison curves reported previously by Glick, et al.(1974).
As shown in Figure 2, recovery of visual threshold followingexposure to the light output from the NVGs is much faster thanrecovery following the white light initial bleaching. Asmentioned in the earlier report, the more rapid recovery from NVGexposure possibly can be attributed to the narrower wavelength
10
band of the NVG output (S20 phosphor). While this would notaffect rod function, separate cone populations might bedifferentially influenced. Although the NVO output is quite dim(0.098 footlambert), it is definitely photopic as evidenced bythe green uolor perception resulting. However, an equallyacceptable explanation is provided by a consideration of neuralversus photochemical adaptation. It is possible that the visualdesensitization after exposure to the dim NVG tube is caused by achange in the neural gain of the visual system rather than achange in the bleached versus unbleached retinal photopigments.By this reasoning, the recovery would be faster because of themore rapid neural recovery rather than a change in photopigmentstate.
Realizing that grouped %&ta analyses might fail to revealsubtle threshold changes among the smokers and that self-reportsof smoking history would not be sufficiently reliable orquantitative, venous blood samples were taken from each subject.These samples were used to analyze sera concentrations of severalcontaminants resulting from tobacco use. Both carboxyhemoglobinand nicotine previously have been considered to be implicated inchanges in visual function. Unfortunately, both of these haverelatively short plasma half-lives and our subjects wereprevented from smoking for at least two hours during the study.Therefore, we also measured cotinine, a major metabolite ofnicotine, which has a much longer life (Pojer, et al., 1984).However, the results shown in Figure 3 indicate that there was nocorrelation between any of these products and absolute thresholdin our subjects.
a1
L _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Conclusions
Our data indicate that there is no difference in visualfunction between smokers and nonsmokers when the measures ofvisual function are absolute light sensitivity and rate ofrecovery of sensitivity after light exposure. There is a growingbody of evidence that use of tobacco products has a variety ofnegative health effects. Also* the immediate physiologioalconsequences of smoking may or may not degrade visual perception.The present data show that there are no cumulative effects ofsmoking which degrades light sensitivity. Therefore, changes invisual function related to chronic cigarette smoking do notappear to provide a useful basis for prohibiting cigarette use.
12
REFERENCES
Calissendorff, B. 1977. Effects of repeated smoking on darkadaptation. Acta Ophthalmologica. 55:261-268.
Collins, W.E., Mertens, H.W., and Higgins, E.A. 1987. Someeffects of alcohol and simulated altitude on complexperformance scores and breathalyzer readings. Aviation.Siace. and Environmental Medicine. 58:328-332.
Durazzini, G., Zazo, F., and Bertoni, G. 1975. The importanceof the dosage of thiocyantes in urine and blood of flyingpersonnel for the prevention of diseases of visual function.In G. Perdriel (Ed). Medical reguirements and examinationprocedures in relation to the tasks of today's airorew,p.A7.1-5. London: NATO Advisory Group for AerospaceResearch and Development.
Fine, B.J. and Kobrick, J.L. 1987. Cigarette smoking, field-dependence and contrast sensitivity. Aviation. Snace. andEnvironmental Medicine. 58:777-782.
Glick, D.D., Wiley, R.W., Moser, C.E., Park, C.K. 1974. Darkadaptation changes associated with use of the AN/PVS-5 NightVision Goggle. USAARL-LR-75-2-7-2. US Army AeromedicalResearch Laboratory, Fort Rucker, Alabama.
Luria, S.M. and McKay, C.L. 1979a. Effects of low levels ofcarbon monoxide on vision of smokers and nonsmokers.Archives O9f Environmental Health. 34:38-44.
Luria, S.M. and McKay, C.L. 1979b. Visual processes of smokersand nonsmokers at different ages. Archives ofEnvironmental Health., 34:449-454.
McFarland, R.A., Roughton, F.J.W., Halperin, M.H. and Niven, J.I.1944. The effects of carbon monoxide and altitude on visualthresholds. Journal of Aviation Medicine. 15:381-394.
McFarland, R.A. 1953. Tobacco and efficiency. In Human factorsin air transportation. ocoupational health and safety,p.299-307. McGraw-Hill Book Company, New York.
McFarland, R.A. 1970. The effects of exposure to smallquantities of carbon monoxide on vision. Annals of the NewYork Academy of Science. 174:301-312.
13
Pojer, R., Whitfield, J.B., Poulos, V., Eckhard, I.F., Richmond,R., and Hensley, W.J. 1984. Carboxyhemoglobin, cotinine,and thiocyanate assay compared for distinguishing smokersfrom nonsmokers. Clinical Chemistry. 30:1377-1380.
Sheard, C. 1946. The effects of smoking on the dark adaptationof rods and cones. Federation Proceedings. 5:94.
Troemel, R.G., Davis, R.T., and Hendley, C.D. 1951. Darkadaptation as a function of caffeine and nicotineadministration. Proceedings of the South Dakota Academy ofSciences. 30:979-985.
US Surgeon General Report. 1979. Smokins and Health. USGovernment Printing Office. Washington, D.C.
14
Initial distribution
CommanderUS Army Natick Research and Development CenterATTN: Documents LibrarianNatick, MA 01760
CommanderUS Army Research Institute of Environmental MedicineNatick, MA 01760
Naval Submarine Medical Research LaboratoryMedical Library, Naval Sub BaseBoX 900Groton, CT 05340
US Army Avionics Research and Development ActivityATTN: SAVAA-P-TPFort Monmouth, NJ 07703-5401
Commander/DirectorUS Army Combat Surveillance and Target Acquisition LaboratoryATTN: DELCS-DFort Monmouth, NJ 07703-5304
US Army Research and Development Support ActivityFort Monmouth, NJ 07703
Commander10th Medical LaboratoryATTN: AudiologistAPO NEW YORK 09180
Chief, Benet Weapons LaboratoryLCWSL, USA ARRADCONATTN: DRDAR-LCB-TLWatervliet Arsenal, NY 12189
CommanderNaval Air Development CenterBiophysics LabATTN: G. KyddCode 60BIWarminster, PA 18974
15
CommanderNan-Machine Integration SystemCode 602Naval Air Development CenterWarminster, PA 18974
Naval Air Development CenterTechnical Information DivisionTechnical Support DetachmentWarminster, PA 18974
CommanderNaval Air Development CenterATTN: Code 6021 (Mr. Brindle)Warminster, PA 18974
Dr. E. HendlerHuman Factors Applications, Inc.29t West Street RoadWarminster, PA 18974
Commanding OfficerNaval Medical Research and Development CommandNational Naval Medical CenterBethesda, MD 20014
Under Secretary of Defense for Research and EngineeringATTN: Military Assistant for Medical and Life SciencesWashington, DC 20301
DirectorArmy Audiology and Speech CenterWalter Reed Army Medical CenterWashington, DC 20307-5001
COL Franklin H. Top, Jr., MDWalter Reed Army Institute of ResearchWashington, DC 20307-5100
CommanderUS Army Institute of Dental ResearchWalter Reed Army Medical CenterWashington, DC 20307-5300
HQ DA (DASG-PSP-O)Washington, DC 20310
16
Naval Air Systems CommandTechnical Air Library 950DEm 278, Jeffersorn Plaza I1Department of the NavyWashington, DC 20361
Naval Research Laboratory LibraryCode 1433Washington, DC 20375
Naval Research Laboratory LibraryShock and Vibration Information CenterCode 5804Washington, DC 20375
Harry Diamond LaboratoriesATTN: Technical Information Branch2800 Powder Mill RoadAdelphi, MD 20783-1197
DirectorUS Army Human Engineering LaboratoryATTN: Technical LibraryAberdeen Proving Ground, ND 21005-5001
US Army Materiel Systems Analysis AgencyATTN: Reports ProcessingAberdeen Proving Ground, ND 21005-5017
CommanderUS Army Test and Evaluation CommandATTN: ANSTE-AD-HAberdeen Proving Ground, ND 21005-5055
US Army Ordnance Center and School LibraryBldg 3071Aberdeen Proving Ground, ND 21005-5201
Director (2)US Army Ballistic Research LaboratoryATTN: DRXBR-OD-ST Tech ReportsAberdeen Proving Ground, ND 21005-5066
US Army Environmental Hygiene Agency LaboratoryBldg E2100Aberdeen Proving Ground, ND 21010
17
CommanderUS Army Medical Research Institute of Chemical DefenseATTN: SGRD-UV-AOAberdeen Proving Ground, MD 21nl0-5425
Technical LibraryChemical Research and Development CenterAberdeen Proving Ground, MD 21010-5423
Commander (5)US Army Medical Research and Development CommandATTN: SGRD-RMS (Mrs. Mad: ;an)Fort Detrick, Frederick, ,- 21701-5012
CommanderUS Army Medical Research Institute of Infectious DiseasesFort Detrick, Frederick, MD 21701
CommanderUS Army Medical Bioengineering Research and Development LatoratoryATTN: SGRD-UBZ-IFort Detrick, Frederick, MD 21701
Director, Biological Science& DivisionOffico of Naval Research600 North Quincy StreetArlington, VA 22217
Defense Technical Information CenterCameron StationAlexandria, VA 22314
CommanderUS Army Materiel CommandATTN: AMCDE-3 (CPT Broadwater)5001 Eisenhower AvenueAlexandria, VA 223!3
US Army Foreign Science and Technology CenterATTN: MTZ220 7th Street, NECharlottesville, VA 22901-5396
CommandantUS Army Aviation Logistior- SchoolATTN: ATSQ-TDNFort Eustis, VA 23604
18
Director, Applied Technology LaboratoryUSARTh-AVSCONATTN: Library, Bldg 401Fort Bustin, VA 23604
US Army Training and Doctrine CommandATTN: ATCD-ZXFort Monroe, VA 23651
US Army Training and Doctrine Command (2)ATTN: SurgeonFort Monroe, VA 23651-5000
Structures Laboratory LibraryUSARTL-AVSCOMNASA Langley Research CenterMail Stop 266Hampton, VA 23665
Aviation Medicine ClinicTMC #22, SAAFFort Bragg, NC 28305
Naval Aerospace Medical Institute LibraryBldg 1953, Code 102Pensacola, FL 32508
US Air Force Armament Development and Test CenterEglin Air Force Base, FL 32542
Command SurgeonUS Central CommandMacDill Air Force Base, FL 33608
US Army Missile CommandRedstone Scientific Information CenterATTN: Documents SectionRedstone Arsenal, AL 35898-5241
Air University Library(AUL/WE)Maxwell AFB, AL 36112
US Army Research and Technology Labortories (AVSCOM)Propulsion Laboratory MS 302-2NASA Lewis Research CenterCleveland, OH 44135
19
AFAXRWHEXWri•hlt-Patterson AFBR OH 45433
US Air Force Institute of Technology(AFIT'D'!...E)Bldg 6-), Area BWright-Patterson AFB, OH 45433
University of MichiganNASA Center of Excellence in Nan-Systems ResearchATTN: R.G. Snyder, DirectorAnn Arbor, NX 48109
Henry L. TaylorDirector, Institute of AviationUniversity of Illinois--Willard AirportSavoy, IL 61874
John A. Dellinger, MS, ATPUniversity of Illinois--Willard AirportSavoy, IL 61874
CommanderUS Army Aviation Systems CommandATTN: MRSAV-WS4300 Goodfellov BlvdSt Louis, NO 63120-1798
Project OfficerAviation Life Support EquipmentATTN: AMCPO-ALSE4300 Goodfellow BlvdSt Louis, NO 63120-1798
CommanderUS Army Aviation Systems CommandATTN: SGRD-UAX-AL (NMJ Lacy)Bldg 105, 4300 Goodfellow BlvdSt Louis, NO 63120
CommanderUS Army Aviation Systems CommandATTN: DRSAV-ED4300 Goodfellow BlvdSt Louis, NO 63120
US Army Aviation Systems CommandLibrary and Information Center BranchATTN: DRSAV-DIL4300 Goodfellow BlvdSt Louis, MO 63120
20
___________________________________________......___.......__
Commanding OfficerNaval Diodynamics LaboratoryP.O. Box 24907New Orleans, LA 70189
Federal Aviation AdministrationCivil Aeromedical InstituteCAMI Library AAC 64D1P.O. Box 25082Oklahoma City, OK 73125
US Army Field Artillery SchoolATTN: LibrarySnow Hall, Room 14Fort Sill, OK 73503
CommanderUS Army Academy of Health SciencesATTN: LibraryFort San Houston, TX 78234
CommanderUS Army Health Services CommandATTN: HSOP-SOFort Sam Houston, TX 78234-6000
CommanderUS Army Institute of Surgical ResearchATTN: SGRD-USN (Jan Duke)Fort Sam Houston, TX 78234-6200
Director of Professional ServicesAFMSC/GSPBrooks Air Force Base, TX 78235
US Air Force School of Aerospace MedicineStrughold Aeromedical LibraryDocuments Section, USAFSAM/TSK-4Brooks Air Force Base, TX 78235
US Army Dugway Proving GroundTechnical LibraryBldg 5330Dugway, UT 84022
Dr. Diane DemosDepartment of Human FactorsISSN, USCLos Angeles, CA 90089-0021
21
US Army Yma Proving Groundtechnical LibraryYuma, AZ 85364
US Army White Sands Missile RangeTechnical Library DivisionWhite sands Missile Range, NM 68002
US Air Force Flight Test CenterTechnical Library@ Stop 238Edwards Air Force Base, CA 93523
US Amy Aviation Engineering Flight ActivityATTN: SAVTE-N (Tech Lib) Stop 217Edwards Air Force Bases CA 93523-5000
CommanderCode 3431Naval Weapons CenterChina Lake, CA 93555
US Army Combat Developments Experimental CenterTechnical Information CenterBldg 2925Fort Ord, CA 93941-5000
Aeromechanics LaboratoryUS Army Research and Technical LaboratoriesAmen Research Center, N/S 215-1Moftfett Field, CA 94035
ComnanderLatterman Army Institute of ResearchATTN: Medical Research LibraryPresidio of San Francisco, CA 94129
Sixth US ArmyATTN: SAAPresidio of San Francisco, CA 94129
DirectorNaval Biosciences LaboratoryNaval Supply Center, Bldg 844Oakland, CA 94625
22
CommanderUS Army Aeromedical CenterFort Rucker, AL 36362
CommanderUS Army Aviation Center and Fort RuckerATTN: ATZQ-CDRFort Rucker, AL 36362
Directorate of Combat DevelopmentsBldg 507Fort Rucker, AL 36362
Directorate of Training DevelopmentBldg 502Fort Rucker, AL 36362
ChiefArmy Research Institute Field UnitFort Rucker, AL 36362
ChiefHuman Engineering Laboratory Field UnitFort Rucker, AL 36362
Commandc -7US Army Safety CenterFort Rucker, AL 36362
CommanderUS Army Aviation Center and Fort RuckerATTN: ATZQ-T-ATLFort Rucker, AL 36362
US Army Aircraft Development Test ActivityATTN: STEBG-MP-QACairns AAF, Fort Rucker, AL 36362
PresidentUS Army Aviation BoardCairns AAF, Fort. Rucker, AL 36362
23
Distribution to foreign addressees
ChiefDefence and Civil Institute of Environmental MedicineP.O. Box 2000ATTN: Director RtLSDDownsview, Ontario Canada M3M 3B9
USDAO-AMLO, US EmbassyBox 36FPO New York 09510
Staff Officer, Aerospace MedicineRAF Staff, British Embassy3100 Massachusetts Avenue, NWWashington, DC 20008
Canadian Society of Aviation Medicinec/o Academy of Medicine, TorontoATTN: Ms. Carmen King288 Bloor Street WestToronto, Canada M55 1V8
Canadian Airline Pilot's AssociationMAJ (Retired) J. Soutendam1300 Steeles Avenue EastBrampton, Ontario, Canada L6T IA2
Canadian Forces Medical Liaison OfficerCanadian Defence Liaison Staff2450 Massachusetts Avenue, NWWashington, DC 20008
Commanding Officer404 Squadron CFB GreenwoodGreenwood, Nova Scotia, Canada BOP INO
Officer CommandingSchool of Operational and Aerospace MedicineDCIEM P.O. Box 20001133 Sheppard Avenue WestDownsview, Ontario, Canada M3M 3B9
National Defence Headquarters101 Colonel J3y DriveATTN: DPHOttowa, Ontario, Canada KIA 0K2
24
commanding officerHeadquarters, RAAP BasePoint Cook Victoria, Australia 3029
Canadian Army Liaison OfficeBldg 602Fort Rucker., AL 36362
Netherlands Army Liaison OfficeBldg 602Fort Rucker,, AL 36362
German Army Liaison OfficeBldg 602Fort Rucker,, AL 36362
British Army Liaison OfficeBldg 602Fort Rucker,, AL 36362
French Army Liaison OfficeBldg 602Fort Rucker,, AL 36362
25





























