Embed Size (px)
Citation preview

Dave Woods, PharmDChief Pharmacy Officer
San Francisco Health Network

Statement of Conflicts of Interest David Woods, PharmD has no actual or potential conflict of interest in relation to this presentation

Today’s Agenda What is the San Francisco Community Clinic Consortium?
Pre‐Audit Strategy HRSA Audit Process Follow up and Lessons Learned

San Francisco Community Clinic Consortium (SFCCC) A group of community‐based, non‐profit health clinics Clinics pool their collective resources to address the needs and interests of their patients
San Francisco’s Outpatient Safety Net Healthy SF (HSF) Program‐ Provides access to universal, comprehensive, affordable healthcare to uninsured adults
Includes pharmacy benefit

Tom Waddell Health Center (and child sites) Covered entity: Tom Waddell Health Center Child sites: #18 (#15‐ SF DPH, #3 independent clinics) # eligible (uninsured) patients: 50,000 # of Providers: 4,109 # of Pharmacies: 9 # of Rx’s: > 400,000 claims/year $ 340B Purchases: $12 million /year
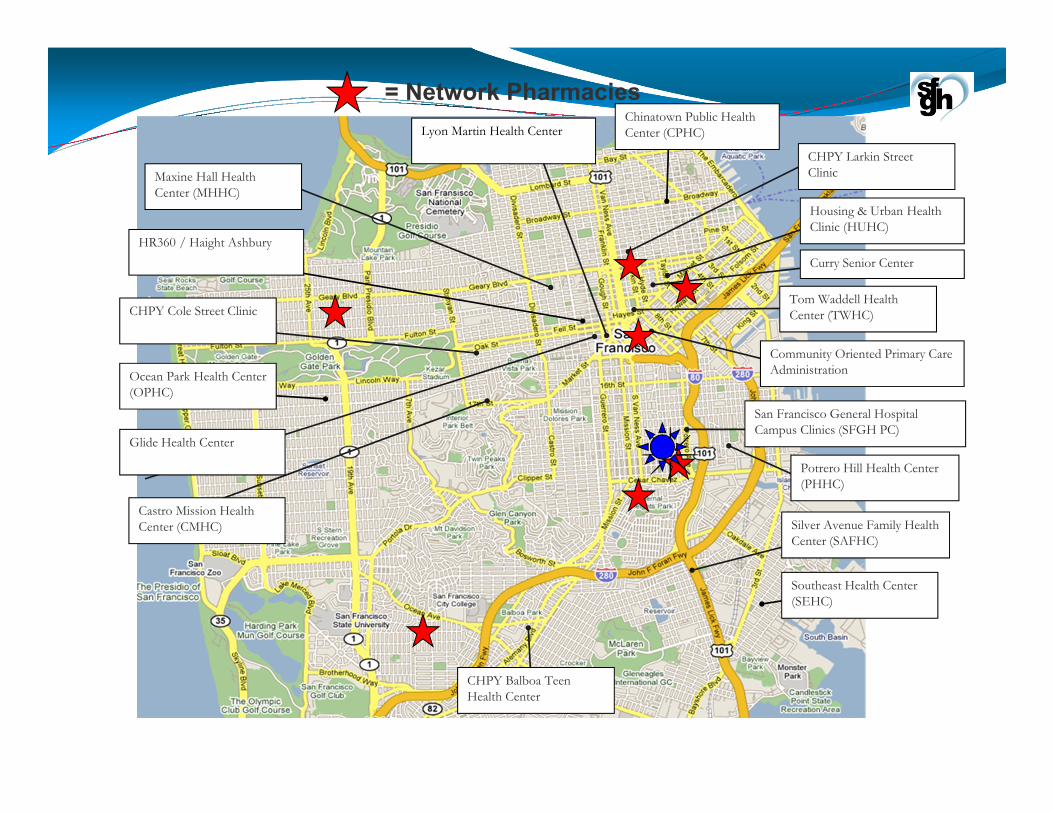
Glide Health Center
Potrero Hill Health Center (PHHC)
Silver Avenue Family Health Center (SAFHC)
Southeast Health Center (SEHC)
Tom Waddell Health Center (TWHC)
Chinatown Public Health Center (CPHC)
Ocean Park Health Center (OPHC)
Maxine Hall Health Center (MHHC)
Housing & Urban Health Clinic (HUHC)
Curry Senior Center
Community Oriented Primary Care Administration
CHPY Cole Street Clinic
CHPY Balboa Teen Health Center
CHPY Larkin Street Clinic
HR360 / Haight Ashbury
Castro Mission Health Center (CMHC)
Lyon Martin Health Center
San Francisco General Hospital Campus Clinics (SFGH PC)
= Network Pharmacies
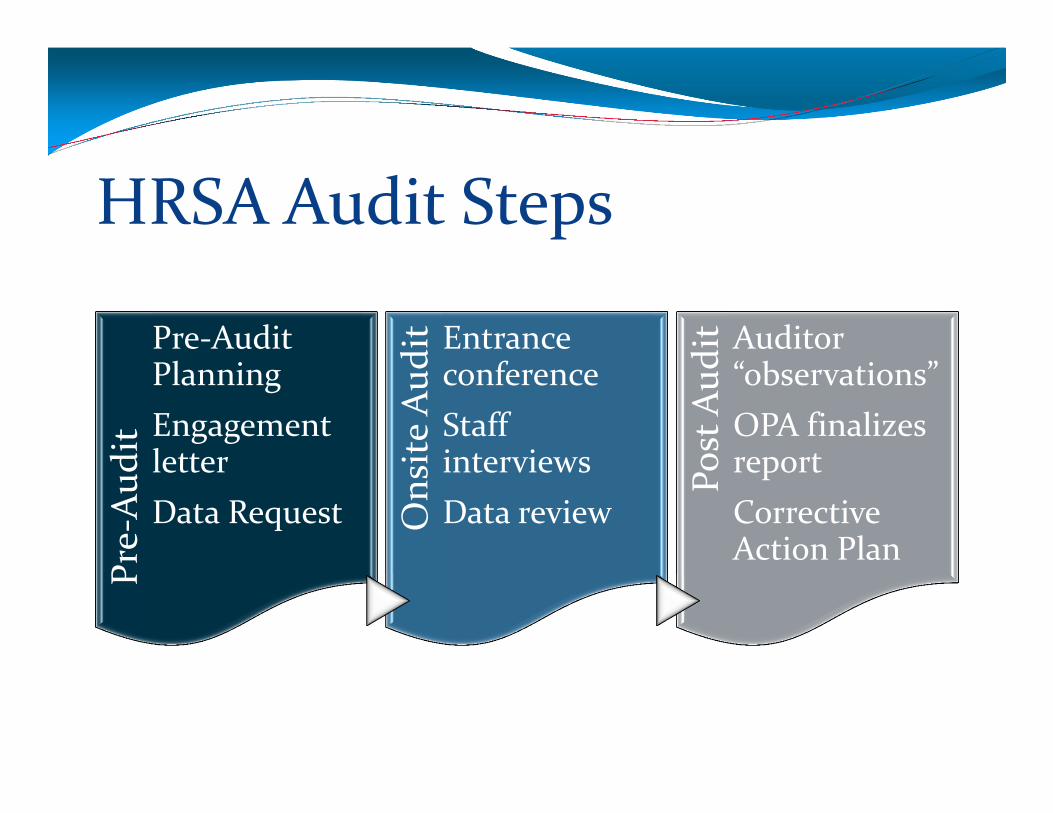
HRSA Audit StepsPre‐Aud
it
Pre‐Audit PlanningEngagement letterData Request O
nsite Aud
it Entrance conferenceStaff interviewsData review
Post Aud
it Auditor “observations”OPA finalizes reportCorrective Action Plan

Pre‐Audit Preparation Identify persons needed for the audit Develop plans for auditor logistics Arrange entrance conference with key management and clinical staff
Prepare participants for questions Alert pharmacies of the audit Re‐check OPA website for accuracy

HRSA Standard Data Request All 340B P&P’s, including vendors Current Medicare Cost Reports Listing of all dispensed prescriptions (6 month period) Eligible provider list Inventory listing and reports (including $ balance) Contract Pharmacy list (and contracts) Monitoring of contract pharmacies‐ data $ value of 340B purchases (purchasing info is used for high cost drug sample)

Logistical Requirements Enclosed, lockable working space to meet and review records
Internet access Access to copy machine Staff to assist with data reviews

HRSA Onsite Audit Entrance conference Escorts Data sample review (electronic vs hard copy)
30 prescription samples were selected from the data submitted for a detailed compliance review
Breakdown of sample Clinic: random cross section High cost drug Rx’s: 5 Providers: 28 selected for audit
340B staff interviews

Data Request 340B Policies and Procedures MOU’s (verify clinic ownership & contracts) Clinic eligibility (verified scope of services, eligibility of each child site, trace to grant funding to verify 340B eligibility)
Patient eligibility Provider eligibility and verification Drug eligibility

Clinic EligibilityVerified that all child sites are eligible for 340BHow child sites tie to the grant fundingReviewed master agreements for each entityReviewed sub‐agreements for each entityBreakdown of contractual costs by clinic

Patient EligibilityVerified:The Covered Entity has an established relationship with patient (medical record review)
Range of services is consistent with grant fundingProvider arrangement with Covered Entity

Prescription EligibilityDocumentation of Rx/order in medical record with associated date of serviceDocumentation of eligible providerDocumentation of eligible locationDocumentation of treatment for the condition the drug is used forDocumentation of outpatient status at the time of order

Provider EligibilityRequested: Hard copy of credentialing file for each provider To see “affiliation” agreement with affiliated medical center for treating physicians to show that the clinic has arrangement for services
Medical Residents‐ validated “active” status when the Rx was written

Referral PrescriptionsOnce the “clinic” refers a patient to a specialist, the clinic’s provider must maintain oversight of the patients care.Prescribing physician is an eligible providerReferral is documented in the medical recordDocumentation of treatment by prescribing physician noted in the medical record

Pharmacy EligibilityReviewed Covered Entity contract/MOU with each pharmacy
On‐site pharmacy visit Visited two pharmacies

Clinic Medication SuppliesRequested invoices of all clinic drug purchasesIf clinics keep 340B drugs on premises, checked for “auditable records of dispensing”
Options: Clinic does not maintain floor stock / med suppliesor Clinic keeps an auditable record of administrations and dispenses
or Purchase from non 340B (WAC) account

Medicaid: Duplicate Discounts & Carve‐0ut Medicaid / Managed Care Medicaid: Clinics “carve‐out” Medicaid prescriptions
In CA, DSH hospitals are required to “carve‐in” Medicaid (Medi‐Cal prescriptions) and bill Medicaid at the 340B cost

Lessons Learned Prepare: Utilize tools and examples offered by Apexus, SNHPA and others
Actively engage team/leadership Identify point person for HRSA communication Audit process appears standardized, but is dynamic Complexity of multiple data sets & medical records Floor stock / clinic medication supplies “Observations” provided, not guidance

Additional Questions?Dave Woods, PharmDChief Pharmacy Officer
San Francisco Dept of Public Health
Phone: (415) 206‐[email protected]





























