Embed Size (px)
Citation preview

Criminal Justice and Substance Abuse Treatment
David FarabeeIntegrated Substance Abuse ProgramsUCLA Department of Psychiatry & Biobehavioral Sciences

Disclosure InformationCriminal Justice & Substance Abuse TreatmentDavid Farabee, PhD
Continuing Medical Education committee members and those involved in the planning of this CME Event have no financial relationships to disclose.
David Farabee, PhD
I have no financial relationships to disclose-and
I will not discuss off label use and/or investigational use in my presentation

Prevalence of Drug Use Among Offenders

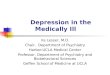
Past-Month Drug Use among Probationers and Non-Probationers
Illicit Drug Use (Past Mo)
Illicit Drug Dependence
(Past Yr)
Alcohol Abuse/Dep
(Past Yr)
AOD Dep/Abuse (Past Yr)
0
5
10
15
20
25
30
35
40
45
31.1
18.4
33.8
41.7
13.5
4.6
13.615.9
Probationers General Population(SAMHSA, 2009)

ADAM (UA) Results Use of any drug among arrestees in
2010 ranged from 52% in Washington, D.C. to 83% in Chicago.
Marijuana was most common; Cocaine is on the decline.
Opiates showed the greatest increases over the past 5 years: Portland: 10% to 22% Sacramento: 6% to 11% Indianapolis: 5% to 11%

Routes of Influence
Economic-CompulsiveIntentional crime that results from drug users engaging in an economically oriented crime to support their own addiction.
Pharmacological Crimes that occur as a result of
the excitability, paranoia, or poor impulse control associated with use of certain drugs.
SystemicCrimes associated with drug manufacturing and distribution.
(Goldstein (1985). JDI, 15, 493-506 )

Violence: The Big Picture
Most alcohol and drug use occurs among persons who are not violent.
Individual histories of aggression and violence are key to predicting whether drug use will increase these behaviors.
Alcohol is more closely related to murder, rape, and assault than any other substance (Parker & Rebhun, 1995).
For a review, see Boles & Miotto (2003). Aggression & Violent Behavior, 8, 155-174. For a review, see Boles & Miotto (2003). Aggression & Violent Behavior, 8, 155-174.

Public Health and Safety Consequences
IDU accounts for 7% of new HIV cases among males; 14% of cases among females (CDC, 2009);
Prevalence of HCV among IDUs is 35% (Amon et al.,
2008); Over the course of an addiction career, periods of
elevated narcotics use are associated with commensurate increases in both property crime and drug dealing (Anglin & Speckart, 1988);
The risk of death among parolees 2 weeks following release is ~ 13 times > than that of the general population, with drug overdose being the leading cause (Binswanger et al., 2007).

Assessing Drug Use and Treatment Needs Among Offenders

Stages of Risk Assessment
Professional judgment Evidence-based tools Evidence-based and dynamic Systematic and comprehensive
Andrews et al. (2006) Crime & Delinquency, 52, 7-27.

Value of Actuarial Approaches
Clinical Versus Statistical Prediction: A Theoretical Analysis and a Review of the Evidence (Meehl, 1954/1996);
20 published studies comparing the predictive efficacy of informal clinical judgments with that of standardized assessments;
In every one of these comparisons, the actuarial approaches performed as well as or better than the subjective approaches.

Two Studies
Validate COMPAS Needs Scales Concurrent validity (with relevant LSI-R
scales) Validate Treatment Effectiveness
Assessment (TEA) Compare with ASI Examine concordance with UA results

Overlapping Constructs of the COMPAS and LSI-R Assessments
COMPAS LSI-RCriminal Involvement Criminal HistoryHistory of Non Compliance History of Violence Current Violence Criminal Associates/Peers CompanionsSubstance Abuse Alcohol/Drug ProblemsFinancial Problems/Poverty FinancialVocational/Education Problems Education/EmploymentCriminal Thinking Attitudes/OrientationFamily Criminality Family/MaritalSocial Environment Problems Leisure and Recreation Leisure/RecreationResidential Instability AccommodationSocial Adjustment Problems Socialization Failure Criminal Opportunity Criminal Personality Social Isolation

Four Yes/No Questions:
Do you need substance abuse treatment?
Do you need help earning a high school diploma/GED?
Do you need help learning skills that will help you find employment?
Do you need help finding a safe place to live?

% of “High-Need” Inmates Identified Using Single Item (N=75)
Substance Abuse
Financial Housing Educ/Voc0
10
20
30
40
50
60
70
80
90
100
COMPASLSI-R

Correlations with TABE Reading Score
COMPAS LSI-R Single Item TABE
COMPAS 1.0 .41*** .23* -.31**
LSI-R 1.0 .40*** -.16
Single Item 1.0 -.34**
TABE 1.0

TEA vs ASI
Treatment Effectiveness Assessment (Ling et al., 2013) Please rate your drug use on a 0-10
scale (0=problematic - 10=doing well) Addiction Severity Index
13 questions combined using a weighting scheme, computer scored.
R=-.34 (p <.001; N=300)

Comparisons of TEA/ASI Scores by UA Result (N=300)
UA - UA+ Sig.
ASI .17 (SD=.10)
.23 (SD=.10)
P <.001
TEA 4.6 (SD=2.9)
3.4 (SD=2.2)
P <.001

6-Mo. RTC by Motivation for and Receipt of Treatment (N=800)
Treated Untreated0
5
10
15
20
25
30
35
4038
21
2731
No Desire for TreatmentDesire for Treatment%
RTC

Interventions for AOD-Involved Offenders

Drug Courts
Testing and Sanctions
Pharmacotherapies

Drug Courts

Overview of Drug Courts
First established in Florida in 1989 Nearly 1,700 drug courts currently
exist in the U.S. Emphasis on treatment, regular
court hearings, frequent testing, and graduated sanctions

Baltimore City Drug Court—A Randomized Comparison (3 Yrs)
% Rearrested % Reconvicted0
102030405060708090
100 78
58
88
64
Treatment (n=139) Control (n=96)
Gottfredson et al. (2006)

GAO Review (2005)
117 drug court evaluations between May 1997 and January 2004 27 were selected
Must have comparison group Must have recidivism, drug use, or
completion outcome 8 of the studies provided cost-benefit
data

GAO Findings
Typical program lasts about 1 year Completion rates range from 27% to 66% Drug court participants were less
criminally active than non-participants (both during and after treatment)
Drug test results showed lower use among drug court participants while in treatment, self reported levels did not differ
Cost savings ranged from $1,000-$15,000 per participant

“[W]e were unable to find conclusive evidence that the specific drug court components, such as the behavior of the judge, treatment provided, level of supervision, and sanctions for noncompliance affect the participants’
[outcomes]” (GAO, 2005; p.6)

Testing & Sanctions

Testing & Sanctions
Regular, random drug testing Swift and certain consequences for
positive tests No a priori assumption of the need
for treatment

Superior Court Drug Intervention Program—Design
Random assignment to— Sanctions docket [graduated
sanctions, random testing, judicial monitoring]
Treatment docket [weekly drug testing and intensive day treatment]
Standard docket [weekly drug testing, monitoring, and encouragement to enter treatment]

Superior Court Drug Intervention Program—Results
Sanctions Treatment Standard0
5
10
15
20
25
30
19
26 2727
22
11ArrestsAll clean UAs
%
Harrell et al., 2000

The HOPE Program
Warning hearings H.O.P.E. hotline > 1 weekly random drug testing (6x per
mo) Every violation (e.g., dirty UA or missed
appointment) leads to an immediate arrest and sanction
Short terms, typically 2 days (served on weekend if employed). Terms increase for repeat violations.

RCT Outcomes
Outcome HOPE Control
No-shows for probation appointments
(average of appointments per
probationer)
9% 23%
Positive urine tests (average of tests
per probationer)
13% 46%
New arrest rate (probationers
rearrested)
21% 47%
Revocation rate (probationers
revoked)
7%* 15%
Incarceration (days sentenced) 138 days* 267 days

Treatment Provider Perceptions of Why Prop 36 Cients Did Not Complete Treatment
63%
74%
18%
30%
17%19%
0
10
20
30
40
50
60
70
80
Transportation Work schedule Housing Familyresponsibilities
Unwilling tocomply
Motivation
Perc
en
t
Notes: Data are from the 2007 Proposition 36 Treatment Provider Survey. The results reflect responses from randomly selected Proposition 36 Treatment Providers (n = 87).

Providers’ Perceptions – Would Jail Sanctions for Non-compliance Improve Treatment Outcomes?
19%
1%
80%
0
20
40
60
80
100
No Maybe Yes
Per
cen
t
Notes: Data are from the 2007 Prop 36 Treatment Provider Survey. The results reflect responses from randomly selected Prop 36 Treatment Providers (n = 87).

Behavioral Triage Model

Behavioral Triage Model (BTM)
Treatment decisions based on probationers’ revealed behavior
Allocates treatment resources more efficiently Under diversion programs many
probationers mandated to treatment do not have a diagnosable substance abuse disorder, wasting scarce treatment resources and displacing self-referrals in greater need of care.

Distribution of Positive Drug Tests
0 1 2 3 4 5 60%
10%
20%
30%
40%
50%
60%
51%
28%
12%
5%2% 1% 1%
Number of positive drug tests
Perc
en
tage

Pharmacotherapies for Opiate-Dependent Offenders
Referral to community-based counseling (usually OP)—inexpensive but insufficient.
Methadone & buprenorphine can be effective, but partial agonists are unpopular among CJ administrators.
Oral opioid antagonists are more acceptable, but adherence (as with psychosocial treatments) is low.
Long-acting opioid antagonists Overcome the problem of non-compliance (at least for
monthly segments); Eliminate concerns about potential diversion; Can still be coupled with psychosocial treatment; and A single dose provides protection during the period of
highest risk for relapse and overdose—the first 2-3 weeks following release.

What is the Evidence for Evidence-Based Offender Programs?

National Registry of Evidence-based Programs and Practices (NREPP)
Managed and funded by SAMHSA Began in 1997 Purpose: “[T]o assist the public in
identifying approaches to preventing and treating mental and/or substance abuse disorders that have been scientifically tested and that can be readily disseminated to the field.” (NREPP, 2009)

Types of Interventions Included in This Study (N=31)
17
8
6
Substance AbuseMental HealthHybrid

NREPP Review Criteria Quality of research is reported results
using the following six criteria: Reliability of measures Validity of measures Intervention fidelity Missing data and attrition Potential confounding variables Appropriateness of analysis
Reviewers use a scale of 0.0 to 4.0, with 4.0 being the most favorable.

Distribution of NREPP Quality and Dissemination Readiness Scores (N=31)
<1.0 1.0-1.4
1.5-1.9
2.0-2.4
2.5-2.9
3.0-3.4
3.5-4.0
0
2
4
6
8
10
12
QualityDissemination
Score
Fre
qu
en
cy

Ratings by Program Type (N=31)
Program Type Quality Dissemination
Substance Abuse (n=17)
Mean=2.8 (SD=0.52)Range=1.7-3.8
Mean=2.6 (SD=0.87)Range=0.8-4.0
Mental Health (n=8) Mean=3.0 (SD=0.37)Range=2.2-3.5
Mean=2.7 (SD=0.92)Range=1.3-4.0
Hybrid (n=6) Mean=3.00 (SD=0.49)Range=2.1-3.5
Mean=3.17 (SD=0.82)Range=1.5-3.9
One third of the EBPs had not been replicated.

Developers as Evaluators
Total (N=123)
Hybrid (N=32)
Mental Health (N=27)
Substance Abuse (N=64)
0 10 20 30 40 50 60 70 80 90 100
52
38
56
58
%

Summary: Prevalence
Illicit drug use and dependence is approximately 2-5 times more common among offenders than the general population.
50%-80% of arrestees test positive for at least one illicit drug.
Cocaine use is declining; opiate use is increasing.

Summary: Assessment
Studies of the added value of more complex assessments over that of single-item questions suggest that some offender needs (esp. drug problems) can be assessed using single items with binary responses
70%-90% of those identified as needing AOD, financial, or housing assistance on the COMPAS or LSI-R were also identified with the single-item measures.
Likewise, compared to the ASI drug-use composite measure, the TEA score was as predictive of UA results as the ASI composite score.

Summary: Interventions
Drug court approach can be effective but not a panacea.
BTM may be a useful alternative that helps practitioners focus on those with most severe problems.
Depot medications for opiate dependence address many of the problems associated with offender treatment (e.g., CJS resistance, poor adherence, risk of diversion, high post-release mortality rates).

Summary: Evidence-Based Programs
There is tremendous variation in the quality/dissemination readiness of the CJ-focused NREPP studies.
Lack of evaluator independence undermines confidence in findings.
Inhibits innovation in a field that desperately needs it.

Questions
1. Rates of opiate use among offenders have stabilized over the past 5 years.
a. Trueb. False

Questions
2. Good risk/needs assessment cannot be accomplished without an in-depth client. interviewa. Trueb. False

Questions
3. Many offenders with serious drug problems can quit when subjected to frequent, random drug tests coupled with mild sanctions.a. Trueb. False