-
Please note, these are the actual video-recorded proceedings
from the live CME event and may include the use of trade names and
other raw, unedited content. Select slides from the original
presentation are omitted where Research To Practice was unable to
obtain permission from the publication source and/or author. Links
to view the actual reference materials have been provided for your
use in place of any omitted slides.
-
David Jablons, M.D.Professor and Chief, Section of General
Thoracic SurgeryAda Distinguished Professor and Program
LeaderThoracic Oncology Laboratory Helen Diller Family
Comprehensive Cancer CenterUniversity of California, San
FranciscoLarge-Scale International Validation of a qPCR-Based
Genetic Assay Prognostic of Survival in Resected Non-Squamous Cell
NSCLC
-
A practical genomic prognostic assay361 stage I-IV non-squamous
FFPE samples(UCSF Training Cohort)Measure expression of 14 cancer
pathways + reference genes(CLIA-certified Laboratory)
-
A practical genomic prognostic assay361 stage I-IV non-squamous
FFPE samples(UCSF Training Cohort)Measure expression of 14 cancer
pathways + reference genes(CLIA-certified Laboratory)L2-penalized
Cox Proportional Hazards Modeling
-
A practical genomic prognostic assay361 stage I-IV non-squamous
FFPE samples(UCSF Training Cohort)Measure expression of 14 cancer
pathways + reference genes(CLIA-certified Laboratory)L2-penalized
Cox Proportional Hazards Modeling
-
A practical genomic prognostic assay361 stage I-IV non-squamous
FFPE samples(UCSF Training Cohort)Measure expression of 14 cancer
pathways + reference genes(CLIA-certified Laboratory)L2-penalized
Cox Proportional Hazards ModelingIndependent ValidationKaiser
Northern California433 stage IChina Clinical Trials Consortium1006
stage I-III
-
A practical genomic prognostic assay361 stage I-IV non-squamous
FFPE samples(UCSF Training Cohort)Measure expression of 14 cancer
pathways + reference genes(CLIA-certified Laboratory)L2-penalized
Cox Proportional Hazards ModelingIndependent ValidationKaiser
Northern California433 stage IChina Clinical Trials Consortium1006
stage I-IIIparaffin-tissues
-
A practical genomic prognostic assay361 stage I-IV non-squamous
FFPE samples(UCSF Training Cohort)Measure expression of 14 cancer
pathways + reference genes(CLIA-certified Laboratory)L2-penalized
Cox Proportional Hazards ModelingIndependent ValidationKaiser
Northern California433 stage IChina Clinical Trials Consortium1006
stage I-IIIqPCRparaffin-tissues
-
A practical genomic prognostic assay361 stage I-IV non-squamous
FFPE samples(UCSF Training Cohort)Measure expression of 14 cancer
pathways + reference genes(CLIA-certified Laboratory)L2-penalized
Cox Proportional Hazards ModelingIndependent ValidationKaiser
Northern California433 stage IChina Clinical Trials Consortium1006
stage I-IIIqPCRparaffin-tissuesblinded
-
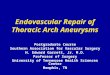
Study Cohorts (n=1800)
UCSF Training CohortKaiser Validation CohortChina Validation
CohortEligible Patients3614331006Successful RNA recovery337
(93.4%)420 (97.0%)967 (96.1%)
Age at Resection67.4 (10.5)66.6(9.3)58.3(10.8)Females200
(59.3%)229 (54.5%)366 (37.9%)Smoking HistoryYes224 (66.5%)355
(84.5%)492 (48.9%)No57 (16.9%)36 (8.6%)403 (40.1%)Unknown56
(16.6%)29 (6.9%)72 (7.2%)Median follow-up
(months)46.470.037.8Deaths at 5 years139 (41.2%)179 (42.6%)406
(42.0%)HistologyAdenocarcinoma278 (82.5%)325 (77.4%)881
(87.6%)Large Cell17 (5.0%)15 (3.6%)17 (1.7%)Mixed10 (3.0%)15
(3.6%)46 (4.6%)NSCLC NOS32 (9.5%)65 (15.5%)23 (2.3%)AJCC StageI223
(66.2%)420 (100%)471 (46.8%)II41 (12.2%)0222 (22.1%)III58
(17.2%)0266 (26.4%)IV9 (2.7%)00Undetermined6 (1.8%)08 (0.8%)Cohort
Mean (Standard Deviation)
-
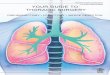
Algorithm Development UCSF CohortOverall survival (%):80% versus
35%, based on 14 cancer-related oncogenes
-
Blinded Assay ValidationKaiser Cohort (n = 420)China Cohort (n =
967) Overall Survival75% versus 48% 80% versus 45%
-
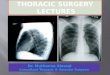
Stage Independence (China)Stage I disease (low risk = 83.0%
[73.889.1]; intermediate risk = 67.7% [54.877.7]; high risk = 64.6%
[57.970.5])Stage II disease (low risk = 54.2% [30.173.2];
intermediate risk = 45.8% [26.263.4]; high risk = 38.1%
[29.446.8])Stage III disease (low risk = 53.3% [32.670.3];
intermediate risk = 43.3% [27.258.5]; high risk = 24.0%
[17.530.9])
-
Multivariate ModelsKaiser cohort (n = 420)China cohort(n =
967)
PredictorHR95% CILR test p-valueHigh Risk
Category*1.931.23-3.040.010Female Sex0.650.48-0.870.004Age
(years)1.041.02-1.06
-
China stage I-IIA (n=540)New TNMM Staging
TNM StageMulti-Gene AssayNew TNMM StageIALow RiskTNMM IAIBLow
Risk
IAIntermediate + High RiskTNMM IBIBIntermediate + High
RiskIIALow Risk
IIAIntermediate + High RiskTNMM IIA
-
Conventional StagingNo data support the use of adjuvant
treatment in patients with stage IA tumors as defined by
conventional criteriaUse of such treatment in patients with stage
IB disease is lent support by only controversial evidence
-
New TNMM StagingThe addition of the molecular assay gave better
risk discrimination than did NCCN risk criteria alone
-
Genetic Assay Outperforms Conventional Methods The molecular
assay was the strongest predictor of 5 year mortality compared with
standard criteria (sex, age, smoking status, etc)Outperformed the
NCCN guidelines used to identify high-risk patients with stage I
disease
-
ConclusionsThere is a clear need to improve NSCLC stagingA
robust, practical assay prognostic of survival after resection has
been developed using qPCR and paraffin-tissuesThis multi-gene assay
has been independently validated in two large international
cohortsThe multi-gene assay can outperform conventional risk
factors / staging and may lead to personalized therapies for
patients with early stage non-squamous NSCLC
-
Thank youUCSF Thoracic Oncology LaboratoryDavid JablonsMichael
MannPatrick PhamMike MulvihillMarc SegalRoshni RayKirk JonesDan
RazZhidong XuThierry JahanBiao HeKaiser Northern CaliforniaStephen
Van Den EedenCharles QuesenberryLaurel HabelChina Clinical Trials
ConsortiumJianxing HeZhi-Hua ZhuWen GaoHuanrong ZhangBo SuQiuhua
DengZongfei WangJiangfen ZhouHuiling LiMei-Chun HuangChe-Chung
YehPinpoint GenomicsDavid BerrymanJerry HurstFatemeh Zaiei
-
Sunday, February 12, 2012Hollywood, FloridaCo-ChairsRogerio C
Lilenbaum, MDMark A Socinski, MDCo-Chair and ModeratorNeil Love,
MDFaculty Walter J Curran Jr, MDDavid Jablons, MDMark G Kris,
MDSuresh Ramalingam, MDAlan B Sandler, MD
************************