Embed Size (px)
Citation preview

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
AnticoagulationAnticoagulation
Debbie L. Cardell, MDDebbie L. Cardell, MDAsst. Clinical Prof of MedicineAsst. Clinical Prof of Medicine
Medical Director UHC-D Medical Director UHC-D Anticoagulation ClinicAnticoagulation Clinic

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Today’s TopicsToday’s Topics
• Diagnoses for which anticoagulation is Diagnoses for which anticoagulation is necessarynecessary
• Duration of therapyDuration of therapy
• INR goalINR goal
• Starting warfarinStarting warfarin
• Sources of evidenced based medicineSources of evidenced based medicine
• Drug/Drug interactionsDrug/Drug interactions
• System wide protocolSystem wide protocol
• Work up of PE/DVTWork up of PE/DVT

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Diagnoses requiring Diagnoses requiring warfarinwarfarin• Atrial fibrillation - sometimesAtrial fibrillation - sometimes
• Valvular Heart DiseaseValvular Heart Disease
• Prosthetic heart valvesProsthetic heart valves
• DVTDVT
• PEPE
• Hypercoagulable States - sometimesHypercoagulable States - sometimes
• THR, TKA, hip fracture repairTHR, TKA, hip fracture repair
• Pulmonary HypertensionPulmonary Hypertension

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
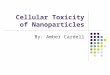
Copyright ©2001 American Heart Association
Fuster, V. et al. Circulation 2001;104:2118-2150
Antithrombotic therapy for prevention of stroke (ischemic and hemorrhagic) in patients with nonvalvular AF: adjusted-dose warfarin compared with
placebo

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Case 1Case 1
• 46 y.o. male continuity patient with 46 y.o. male continuity patient with allergic rhinitis, found on exam to allergic rhinitis, found on exam to have irregular pulse. No other have irregular pulse. No other medical problems.medical problems.
• Pulse irreg. 76 bpm, BP 132/76Pulse irreg. 76 bpm, BP 132/76
• EKG shows a-fibEKG shows a-fib

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 1 Question 1
• Does the patient need Does the patient need anticoagulation?anticoagulation?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Answer Answer
• NoNo
• Provide proof for your answerProvide proof for your answer

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Atrial FibrillationAtrial Fibrillation
• CHADS2 score is an easy to use clinical CHADS2 score is an easy to use clinical tool for determining who needs warfarintool for determining who needs warfarin
• C – CHF- 1 point C – CHF- 1 point
• H – treated HTN - 1 pointH – treated HTN - 1 point
• A – age >75 – 1 pointA – age >75 – 1 point
• D – diabetes – 1 pointD – diabetes – 1 point
• S – prior history of stroke or TIA-2 pointsS – prior history of stroke or TIA-2 points

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
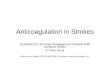
CHADS2 score and risk of CHADS2 score and risk of strokestroke
ScoreScore Risk of Stroke per 100 patient Risk of Stroke per 100 patient yearsyears
00 1.91.9
11 2.82.8
22 4.04.0
33 5.95.9
44 8.58.5
55 2.52.5
66 18.218.2

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
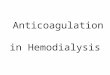
Interpreting the CHADS2 Interpreting the CHADS2 scorescore
ScoreScore RiskRisk AnticoaguAnticoagulation lation TherapyTherapy
ConsideraConsiderationstions
00 LowLow AspirinAspirin 325 mg 325 mg likely to likely to offer most offer most benefitbenefit
1-21-2 ModerateModerate Aspirin or Aspirin or WarfarinWarfarin
INR goal INR goal 2-32-3
33 HighHigh WarfarinWarfarin INR goal INR goal 2-32-3

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Exception to CHADS2Exception to CHADS2
• Although a patient with a prior stroke Although a patient with a prior stroke and no other risk factors would only and no other risk factors would only have a score of 2 and calculates out have a score of 2 and calculates out as a moderate risk, they are truly as a moderate risk, they are truly high risk and should be treated with high risk and should be treated with warfarin in the absence of warfarin in the absence of contraindications.contraindications.

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Case 2Case 2
• 54 y.o. man with HTN well controlled 54 y.o. man with HTN well controlled on HCTZ and metoprolol, found to on HCTZ and metoprolol, found to have irregular pulsehave irregular pulse
• EKG shows a-fibEKG shows a-fib
• Echo one year ago EF 60%Echo one year ago EF 60%

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 2Question 2
• Does this patient need warfarin?Does this patient need warfarin?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Interpreting the CHADS2 Interpreting the CHADS2 scorescore
ScoreScore RiskRisk Anticoag-Anticoag-ulation ulation TherapyTherapy
ConsideraConsidera-tions-tions
00 LowLow AspirinAspirin 325 mg 325 mg likely to likely to offer most offer most benefitbenefit
1-21-2 ModerateModerate Aspirin or Aspirin or WarfarinWarfarin
INR goalINR goal
2-32-3
33 HighHigh WarfarinWarfarin INR goal INR goal
2-32-3

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Valid contraindications to Valid contraindications to warfarinwarfarin
• Patient refusalPatient refusal
• Non-compliance with INR monitoringNon-compliance with INR monitoring
• Alcohol consumptionAlcohol consumption
• Bleeding diathesisBleeding diathesis
• History of major bleedingHistory of major bleeding

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 3Question 3
• 56 y.o. woman with MVP admitted 4 56 y.o. woman with MVP admitted 4 mos ago for TIAmos ago for TIA
• Does she need warfarin?Does she need warfarin?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Answer Answer
• Only if she is an ASA failureOnly if she is an ASA failure
• MVP with h/o stroke or TIA –ASA dose MVP with h/o stroke or TIA –ASA dose of 50-160mg dailyof 50-160mg daily
• If fails ASA – then warfarinIf fails ASA – then warfarin

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Valvular DiseaseValvular Disease
• MVP with h/o stroke or embolization – ASA MVP with h/o stroke or embolization – ASA 50-160 mg50-160 mg
• MVP with ASA failure – warfarin – long-MVP with ASA failure – warfarin – long-term range 2-3term range 2-3
• Rheumatic heart disease – mitral valve – Rheumatic heart disease – mitral valve – with a-fib and/or prior history of stroke – with a-fib and/or prior history of stroke – lifetime use of warfarin with a goal of 2-3lifetime use of warfarin with a goal of 2-3
• Rheumatic Mitral Valve disease and NSR Rheumatic Mitral Valve disease and NSR with Left Atrial size >5.5 cm – lifetime with Left Atrial size >5.5 cm – lifetime warfarin goal 2-3warfarin goal 2-3

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 4Question 4
• 60 y.o. man with prosthetic aortic 60 y.o. man with prosthetic aortic valve, echo shows nl EF. He has valve, echo shows nl EF. He has never had a stroke or TIA. He has a never had a stroke or TIA. He has a bi-leaflet valve.bi-leaflet valve.
• What is his INR goal?What is his INR goal?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Prosthetic Heart ValvesProsthetic Heart Valves
• GoalsGoals– Aortic position – NSR, NL LA size, bi-leaflet or Aortic position – NSR, NL LA size, bi-leaflet or
tilting disc prosthesis - INR 2.0-3.0tilting disc prosthesis - INR 2.0-3.0– Aortic position – other risk factors* INR 2.5-3.5Aortic position – other risk factors* INR 2.5-3.5– Mitral position – 2.5-3.5Mitral position – 2.5-3.5
• Duration – lifetime if mechanical, 12 weeks Duration – lifetime if mechanical, 12 weeks post surgery if bio-prosthetic (porcine)post surgery if bio-prosthetic (porcine)

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
AVR + Other Risk Factors = AVR + Other Risk Factors = INR 2.5-3.5INR 2.5-3.5
• Atrial FibrillationAtrial Fibrillation
• Myocardial infarctionMyocardial infarction
• Left atrial enlargement > 5.5cmLeft atrial enlargement > 5.5cm
• Endocardial damageEndocardial damage
• Low ejection fractionLow ejection fraction
• Caged ball or caged disc valveCaged ball or caged disc valve

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 5Question 5
• Patient with AVR tells you his brother Patient with AVR tells you his brother just had an MI at 49y.o. He picked just had an MI at 49y.o. He picked up a new habit, smoking, since you up a new habit, smoking, since you last saw him.last saw him.
• Would you start ASA for primary Would you start ASA for primary prevention of CV disease?prevention of CV disease?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
AnswerAnswer
• YesYes

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Aspirin Plus Warfarin?Aspirin Plus Warfarin?
• When?When?
• Only proven benefit is in patients Only proven benefit is in patients with Prosthetic Valves and increased with Prosthetic Valves and increased CV risk or previous MICV risk or previous MI– WARIS IIWARIS II– ASPECT 2ASPECT 2
• Dose should be 81mgDose should be 81mg

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Next CaseNext Case
• 28 y.o. woman presents to the ER on 28 y.o. woman presents to the ER on one of your call days with a unilateral one of your call days with a unilateral swollen legswollen leg
• Doppler reveal a DVTDoppler reveal a DVT
• History reveals she just had breast History reveals she just had breast reduction surgery 2 weeks agoreduction surgery 2 weeks ago

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 6Question 6
• What is her INR goal?What is her INR goal?
• How long would you treat her?How long would you treat her?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Deep Vein ThrombosisDeep Vein Thrombosis
• INR goal is 2.0-3.0INR goal is 2.0-3.0
• Duration depends on clinical scenarioDuration depends on clinical scenario

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Classifying PatientsClassifying Patients
• First-episode DVT secondary to a transient First-episode DVT secondary to a transient risk factor risk factor
• First-episode DVT and concurrent cancerFirst-episode DVT and concurrent cancer• First-episode idiopathic DVT First-episode idiopathic DVT • First-episode DVT associated with a First-episode DVT associated with a
prothrombotic genotype prothrombotic genotype • Recurrent DVT Recurrent DVT
CHEST 2003CHEST 2003

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
11stst DVT, Transient Risk DVT, Transient Risk FactorFactor
• Treat to INR 2-3 for 3 monthsTreat to INR 2-3 for 3 months
• Transient Risk factors includeTransient Risk factors include– SurgerySurgery– PregnancyPregnancy– HospitalizationHospitalization– TraumaTrauma– FractureFracture

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Next CaseNext Case
• 67 y.o. male continuity patient 67 y.o. male continuity patient seeing you after hospital discharge, seeing you after hospital discharge, comes to clinic for follow up. He was comes to clinic for follow up. He was admitted for a UE DVT. During admitted for a UE DVT. During admission he was found to have admission he was found to have widely metastatic liver cancer.widely metastatic liver cancer.
• What is your anticoagulant of choice?What is your anticoagulant of choice?
• How long do you treat him?How long do you treat him?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
DVT in the setting of CancerDVT in the setting of Cancer
• LMWH is recommended the in CHEST LMWH is recommended the in CHEST guidelines for the first 3-6 months of long guidelines for the first 3-6 months of long term therapyterm therapy
• LMWH is recommended for advanced and LMWH is recommended for advanced and metastatic cancersmetastatic cancers
• LMWH is recommended LMWH is recommended during during chemotherapychemotherapy
• In select patients with localized disease, In select patients with localized disease, warfarin can be consideredwarfarin can be considered

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Next CaseNext Case
• 37 y.o. man in your clinic comes in 37 y.o. man in your clinic comes in acutely complaining of leg pain and acutely complaining of leg pain and swelling.swelling.
• He denies, travel, recent surgery, He denies, travel, recent surgery, hospitalization, prolonged hospitalization, prolonged immobilization.immobilization.
• You are able to obtain dopplers. You are able to obtain dopplers.
• He has a DVTHe has a DVT

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 7Question 7
• What is his INR goal?What is his INR goal?
• How long do you treat him?How long do you treat him?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
First Idiopathic VTEFirst Idiopathic VTE
• At least 6 months (6-12 months)At least 6 months (6-12 months)– PREVENT trial – after 3 months of PREVENT trial – after 3 months of
anticoagulation, 508 patients randomized to anticoagulation, 508 patients randomized to continuation of warfarin (INR 1.5-2.0) vs. placebo. continuation of warfarin (INR 1.5-2.0) vs. placebo. Trial stopped after 4.3 years when there was a Trial stopped after 4.3 years when there was a significantly lower rate of recurrent VTE in the significantly lower rate of recurrent VTE in the warfarin group (2.6 versus 7.2 per 100 patient-warfarin group (2.6 versus 7.2 per 100 patient-years, hazard ratio [HR] 0.36, 95% CI 0.19-0.67) years, hazard ratio [HR] 0.36, 95% CI 0.19-0.67)
– ELATE – after 3 months of INR 2.0-3.0, 738 ELATE – after 3 months of INR 2.0-3.0, 738 patients randomized low dose warfarin INR 1.5-patients randomized low dose warfarin INR 1.5-1.9 vs. 2.0-3.0. f/u 2.4 yrs. Recurrent VTE was 1.9 vs. 2.0-3.0. f/u 2.4 yrs. Recurrent VTE was significantly lower in the higher dose warfarin significantly lower in the higher dose warfarin group (1.9 versus 0.7 per 100 patient-years, HR group (1.9 versus 0.7 per 100 patient-years, HR 2.8, 95% CI 1.1-7.0). 2.8, 95% CI 1.1-7.0).

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
After six monthsAfter six months
• Risks and benefits need to be reviewed Risks and benefits need to be reviewed with the patientwith the patient– Risk of minor bleeding with continued Risk of minor bleeding with continued
anticoagulation 12.8 per 100 pt years, major anticoagulation 12.8 per 100 pt years, major bleeding is 2.7 per 100 patient-years, with a bleeding is 2.7 per 100 patient-years, with a case fatality rate of 9.1 percent (95% CI 2.5-case fatality rate of 9.1 percent (95% CI 2.5-22) 22) Ann Intern Med 2003 Dec 2;139(11):893-900. Ann Intern Med 2003 Dec 2;139(11):893-900.
– Risk of recurrent VTE on no warfarin 7.2-8.4 Risk of recurrent VTE on no warfarin 7.2-8.4 per 100 pt years in PREVENT and THRIVE III per 100 pt years in PREVENT and THRIVE III trials, low dose warfarin 1.9-2.6 per 100 pt trials, low dose warfarin 1.9-2.6 per 100 pt years (ELATE and PREVENT), and .7 episodes years (ELATE and PREVENT), and .7 episodes per 100 pt years on full dose warfarin (ELATE)per 100 pt years on full dose warfarin (ELATE)

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Case ContinuedCase Continued
• His 6 months of warfarin therapy are His 6 months of warfarin therapy are overover
• You discuss the risks and benefits of You discuss the risks and benefits of treating him for a year vs. stopping nowtreating him for a year vs. stopping now
• He opts to stop the warfarinHe opts to stop the warfarin• Should you test him for acquired and Should you test him for acquired and
hereditary thrombophilias?hereditary thrombophilias?• Are there any other tests to determine Are there any other tests to determine
his individual risk?his individual risk?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Screening for Screening for ThrombophiliasThrombophilias• Controversial – there is no consensusControversial – there is no consensus
• Arguments against screening – Arguments against screening – – excessive, not cost effective, does not impact excessive, not cost effective, does not impact
treatmenttreatment
• Arguments for screening – Arguments for screening – – some patients (1-2%) have very high risk some patients (1-2%) have very high risk
profiles, knowledge could help manage risky profiles, knowledge could help manage risky situations such as surgery and pregnancysituations such as surgery and pregnancy
– Helps in screening of family membersHelps in screening of family members

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Inherited ThrombophiliasInherited Thrombophilias
• Require life long anticoagulation only in the Require life long anticoagulation only in the following cases:following cases:– Two or more spontaneous thromboses or one Two or more spontaneous thromboses or one
spontaneous thrombosis in the case ofspontaneous thrombosis in the case of antithrombinantithrombin deficiency or the antiphospholipid syndrome deficiency or the antiphospholipid syndrome
– One spontaneous life-threatening thrombosis (e.g., near-One spontaneous life-threatening thrombosis (e.g., near-fatal pulmonary embolism; cerebral, mesenteric, or fatal pulmonary embolism; cerebral, mesenteric, or portal vein thrombosis) portal vein thrombosis)
– One spontaneous thrombosis at an unusual site (e.g., One spontaneous thrombosis at an unusual site (e.g., mesenteric or cerebral vein) mesenteric or cerebral vein)
– One spontaneous thrombosis in the presence of more One spontaneous thrombosis in the presence of more than a single genetic defect predisposing to a than a single genetic defect predisposing to a thromboembolic event thromboembolic event
UpToDateUpToDate

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Consider screeningConsider screening
• In Strongly Thrombophilic patients –In Strongly Thrombophilic patients –
– First idiopathic VTE prior to 50 y.o.First idiopathic VTE prior to 50 y.o.– History of recurrent thrombotic episodesHistory of recurrent thrombotic episodes– First-degree relative with thrombotic First-degree relative with thrombotic
episode prior to the age of 50episode prior to the age of 50

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
When not to screenWhen not to screen
• Recent major surgery, trauma, or Recent major surgery, trauma, or immobilization immobilization
• Active malignancy Active malignancy • Systemic lupus erythematosus Systemic lupus erythematosus • Inflammatory bowel disease Inflammatory bowel disease • Myeloproliferative disorders Myeloproliferative disorders • Heparin-induced thrombocytopenia with Heparin-induced thrombocytopenia with
thrombosis thrombosis • Preeclampsia at term Preeclampsia at term • Retinal vein thrombosis Retinal vein thrombosis

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Individual Risk AssessmentIndividual Risk Assessment
• D-dimer testing – 4 studies have D-dimer testing – 4 studies have shown an increased risk of recurrent shown an increased risk of recurrent VTE in patients with elevated D-dimers VTE in patients with elevated D-dimers after 3 months of anticoagulation HR after 3 months of anticoagulation HR 2-2.52-2.5– One of the studies showed only 5 patients One of the studies showed only 5 patients
out of 186 with a normal D-dimer with a out of 186 with a normal D-dimer with a recurrent VTE, this give a negative recurrent VTE, this give a negative predictive value of >96%. predictive value of >96%.
Thromb Haemost 2002 Jan;87(1):7-12.Thromb Haemost 2002 Jan;87(1):7-12.

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Recurrent VTERecurrent VTE
• Trials are ongoing to determine the Trials are ongoing to determine the optimal duration of treatment, but for optimal duration of treatment, but for now recommendations say now recommendations say “indefinite” unless there is a “indefinite” unless there is a reversible causereversible cause
• If reversible cause – then treat until If reversible cause – then treat until the risk factor is no longer an issuethe risk factor is no longer an issue

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Upper Extremity ThrombosisUpper Extremity Thrombosis
• General consensus is that this General consensus is that this represents a more thrombogenic represents a more thrombogenic patientpatient
• No randomized controlled trials to No randomized controlled trials to determine the most appropriate determine the most appropriate length of therapylength of therapy
• If a reversible cause – can treat for 3-6 If a reversible cause – can treat for 3-6 monthsmonths
• If not – long term anticoagulationIf not – long term anticoagulation

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Next CaseNext Case
• You are called to the ER to see one of your You are called to the ER to see one of your clinic patients. She is 42 y.o. c/o SOB for 1 clinic patients. She is 42 y.o. c/o SOB for 1 day, she is breathing rapidly and is day, she is breathing rapidly and is tachycardic, her O2 sats are 88%. CXR is tachycardic, her O2 sats are 88%. CXR is negative. WBCs are normal. She is not negative. WBCs are normal. She is not hypotensive.hypotensive.
• You order a PE protocol CT. It is positive.You order a PE protocol CT. It is positive.
• How long will this patient need to be How long will this patient need to be treated for her PE?treated for her PE?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Treatment for PETreatment for PE
• Treatment goals are the same as Treatment goals are the same as DVTDVT
• Duration the same as DVTDuration the same as DVT
• Exception is “massive PE” which is Exception is “massive PE” which is defined as “shock” or requiring defined as “shock” or requiring pressors – this would constitute a pressors – this would constitute a reason for lifelong anticoagulationreason for lifelong anticoagulation

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Other ConsiderationsOther Considerations
• Compression Stockings should be prescribed at Compression Stockings should be prescribed at 30-40mm Hg at the ankle in all patients with 30-40mm Hg at the ankle in all patients with DVT within a month after Dx and continued for DVT within a month after Dx and continued for 1-2 years. This has been proven to reduce the 1-2 years. This has been proven to reduce the incidence of post-thrombotic syndrome by 50% incidence of post-thrombotic syndrome by 50% LancetLancet 1997;3491997;349,759-762,759-762
• Patients should be on “ambulation as Patients should be on “ambulation as tolerated”tolerated”
• NSAIDs are not recommended during the acute NSAIDs are not recommended during the acute treatment of DVTtreatment of DVT

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Total Hip ReplacementTotal Hip Replacement
• Low Molecular Weight Heparin Low Molecular Weight Heparin (LMWH)(LMWH)
oror
• Warfarin with a target INR of 2.0-3.0Warfarin with a target INR of 2.0-3.0
oror
• Fondaparinux 2.5 mg dailyFondaparinux 2.5 mg daily
• Duration: 28-35 daysDuration: 28-35 days

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Hip Fracture SurgeryHip Fracture Surgery
• Same recommendations as Total Hip Same recommendations as Total Hip ReplacementReplacement

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Total Knee Arthroplasty Total Knee Arthroplasty (TKA)(TKA)
• LMWH at high risk dosesLMWH at high risk doses
oror
• Warfarin with INR goal 2.0-3.0Warfarin with INR goal 2.0-3.0
oror
• FondaparinuxFondaparinux
• Duration: 10 daysDuration: 10 days

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Next CaseNext Case
• 62 y.o. female with Pulmonary 62 y.o. female with Pulmonary Hypertension secondary to COPDHypertension secondary to COPD
• She is in NSRShe is in NSR
• Her last echo showed an EF of 50%Her last echo showed an EF of 50%

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 8Question 8
• Does she need warfarin?Does she need warfarin?
• Does your recommendation change if Does your recommendation change if her EF was 20%?her EF was 20%?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Pulmonary HypertensionPulmonary Hypertension
• INR goal of 2.0 forINR goal of 2.0 for– Pulmonary Hypertension secondary to Pulmonary Hypertension secondary to
chronic thromboembolic diseasechronic thromboembolic disease– PulmHTN with afibPulmHTN with afib– Idiopathic Pulmonary HypertensionIdiopathic Pulmonary Hypertension– Familial Pulmonary HypertensionFamilial Pulmonary Hypertension– Pulmonary Hypertension with severe left Pulmonary Hypertension with severe left
heart failureheart failure

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Starting DoseStarting Dose
• Start with 5mg of warfarin (CHEST)Start with 5mg of warfarin (CHEST)
• Consider a lower dose in very elderlyConsider a lower dose in very elderly
• Get a baseline INRGet a baseline INR
• Follow a nomogramFollow a nomogram

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
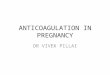
NomogramNomogram
• One can be found in the AnnalsOne can be found in the Annals– Annals of Internal Medicine Annals of Internal Medicine
2003;138:7142003;138:714

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Kovacs, M. J. et. al. Ann Intern Med 2003;138:714-719
5-mg Warfarin Initiation Nomogram

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Initiation CaseInitiation Case
• Your previous DVT patient is started Your previous DVT patient is started on 5mg warfarin (following CHEST on 5mg warfarin (following CHEST guidelines)guidelines)
• His baseline INR is 1.1His baseline INR is 1.1
• You start him on 1mg/kg of You start him on 1mg/kg of enoxaparin BIDenoxaparin BID
• He comes back on day three with an He comes back on day three with an INR of 1.4INR of 1.4

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Question 9Question 9
• What dose do you tell him to take?What dose do you tell him to take?
• When do you tell him to come back?When do you tell him to come back?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Follow upFollow up
• Arrange for appointments as per the Arrange for appointments as per the nomogramnomogram
• INR check on days 3,4,5,6,INR check on days 3,4,5,6,
• Then twice weekly for two weeksThen twice weekly for two weeks
• Weekly for two more weeksWeekly for two more weeks
• IfIf stable, then every 4 weeks stable, then every 4 weeks

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Initiation of anticoagulationInitiation of anticoagulation
• How many days of enoxaparin should How many days of enoxaparin should you write for?you write for?
• What are the instructions for What are the instructions for stopping the enoxaparin?stopping the enoxaparin?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
AnswerAnswer
• Write for a minimum of five days of Write for a minimum of five days of enoxaparin enoxaparin
• INR should be therapeutic for two INR should be therapeutic for two days in a row before stopping days in a row before stopping enoxaparinenoxaparin

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
MonitoringMonitoring
• After the initial 2 weeks, INRs usually After the initial 2 weeks, INRs usually become more stablebecome more stable
• Maintenance nomograms may be Maintenance nomograms may be utilized to help in decision makingutilized to help in decision making
• An experienced clinician is An experienced clinician is equivalent to a nomogramequivalent to a nomogram

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Maintenance CaseMaintenance Case
• 65 y.o. woman with A-fib, DM and 65 y.o. woman with A-fib, DM and hyperlipidemia had to switch her hyperlipidemia had to switch her statin from atorvastatin to simvastatin statin from atorvastatin to simvastatin for insurance coverage purposes.for insurance coverage purposes.
• Her repeat INR after med change Her repeat INR after med change shows the INR is 3.6shows the INR is 3.6
• What adjustment do you make?What adjustment do you make?• When should she follow up?When should she follow up?

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
INR changes while on INR changes while on maintenancemaintenance
• Worsening CHFWorsening CHF
• New medicationNew medication
• Stopped a medicationStopped a medication
• Stopped or started smokingStopped or started smoking
• Increased or decreased physical activityIncreased or decreased physical activity
• InfectionInfectionThis is why an experienced clinician performs as well as a nomogram or This is why an experienced clinician performs as well as a nomogram or calculatorcalculator

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Anticoagulation Clinic vs. Anticoagulation Clinic vs. PCPPCP
• Anticoagulation Clinic saves moneyAnticoagulation Clinic saves money• Decreases hospitalizations (related Decreases hospitalizations (related
to anticoagulation)to anticoagulation)• Decreases INRs outside of rangeDecreases INRs outside of range• Decreases anticoagulation related Decreases anticoagulation related
complicationscomplications• Am J Hosp PharmAm J Hosp Pharm 985:42,304-308, 985:42,304-308, PharmacotherapyPharmacotherapy
10=995:15,732-739, 10=995:15,732-739, Drug Intell Clin PharmDrug Intell Clin Pharm 1985;19,575- 1985;19,575-580, 580, Arch Intern MedArch Intern Med 1998:158,1641-1647, 1998:158,1641-1647, ChestChest 2005:127,1515-1522.2005:127,1515-1522.

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Drug InteractionsDrug Interactions
• Safest to assume all drugs interact Safest to assume all drugs interact with warfarinwith warfarin
• Check Check allall new medications in new medications in epocrates or a similar programepocrates or a similar program
• Don’t forget about herbals and over Don’t forget about herbals and over the counter medsthe counter meds

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Common Bad ActorsCommon Bad Actors
• AcetataminophenAcetataminophen
• Trimethoprim/sulfamethoxazoleTrimethoprim/sulfamethoxazole
• FluoroquinolonesFluoroquinolones
• Antibiotics in generalAntibiotics in general
• GemfibrozilGemfibrozil
• AspirinAspirin
• ClopidogrelClopidogrel
• PrednisonePrednisone

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
When ForcedWhen Forced
• If you must use one of these If you must use one of these medications, recheck the INR in 3 medications, recheck the INR in 3 daysdays
• OR look on MicroMedex and see how OR look on MicroMedex and see how strong the interaction isstrong the interaction is
• For Bactrim, decrease weekly For Bactrim, decrease weekly warfarin dose by 30% and recheck in warfarin dose by 30% and recheck in 3 days3 days

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
System Based Protocol System Based Protocol GoalsGoals
• Uniformity of treatmentUniformity of treatment
• Encourage the use of evidence based Encourage the use of evidence based guidelinesguidelines
• Create a patient registryCreate a patient registry
• Uniformity of dose adjustment and Uniformity of dose adjustment and follow upfollow up
• Provide seamless care Provide seamless care

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
ResourcesResources
• CHADS2 scoreCHADS2 score
• Wells score for DVT and PEWells score for DVT and PE
• Warfarin initiation nomogramWarfarin initiation nomogram
• Warfarin maintenance calculatorWarfarin maintenance calculator
• CHEST guidelinesCHEST guidelines
• Patient information in English and Patient information in English and SpanishSpanish

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Referring PatientsReferring Patients
• From inpatient setting – use Consult From inpatient setting – use Consult upon discharge option upon discharge option
• Anticoagulation referralAnticoagulation referral• Tell patient to go to ExpressMed at the Tell patient to go to ExpressMed at the
hospital in 2-3 days (follow protocol)hospital in 2-3 days (follow protocol)• Order INR in SunriseOrder INR in Sunrise
– Stat patient waitingStat patient waiting– Give paper to patientGive paper to patient

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
Referring PatientsReferring Patients
• From Outpatient settingFrom Outpatient setting– Use Outpatient Consult or Anticoagulation Use Outpatient Consult or Anticoagulation
ConsultConsult– In pull down menu, select anticoagulationIn pull down menu, select anticoagulation– Tell patient to go to ExpressMed clinic in Tell patient to go to ExpressMed clinic in
2-3 days (follow protocol)2-3 days (follow protocol)– Order INR from within SunriseOrder INR from within Sunrise
•Stat patient waitingStat patient waiting•Hand the paper to the patientHand the paper to the patient

Debbie L. Cardell, MDDebbie L. Cardell, MDDiv Gen Med UTHSCSADiv Gen Med UTHSCSA 2/29/082/29/08
QuestionsQuestions