Embed Size (px)
Citation preview
DECLARATION OF CONFLICT OF INTEREST

CONFLICT OF INTEREST
No conflict of interest relevant
to this talk

Cardiovascular MRI, analysis of safety
and image quality in patients with
implantable cardiac arrhythmia devices
Author Block
B. Igual*†, MJ. Sancho-Tello†, F. Buendía†, A. Maceira*, O. Cano†‡, J.
Estornell*, JM. Sánchez†, J. Olagüe†, A. Salvador†
† Servicio Cardiología Hospital Universitari i Politècnic La Fe, Valencia
* ERESA. Unidad Imagen Cardíaca. Valencia, Spain.
‡ Instituto Investigación Sanitaria La Fe, Valencia
Animal experiments showing significant heating effects of over 15ºC
At least 17 pacemaker patient deaths worldwide thought to be
attributable to MRI
Martin ET. et al. Cur Cardiol Reports 2007;9:63-71.
Background
Adverse Events During MRI in Pacemaker Patients Evidence Against Performance of MRI in Patients with ICADs
Ferris RJ. et al. Am J Roentgenol 2007;188:1388-1394.
More than 500 patients with ICADs have undergone MRI at 1.5T
without severe complications
Background
Evidence Favoring Performance of MRI in Patients with ICADs
- Shinbane JS. J. Cardiovasc Magn Reson. 2007;9:5-13
- Sommer T, et al. Circulation. 2006;114:1277-1284
- Martin ET, et al. J Am Coll Cardiol. 2004;43:1315-1324
- Nazarian S, et al. Circulation. 2006;114:1277-1284
Previously reported pacemaker patient deaths only with “old
generation” pacemakers (< year 2000) and in the absense of adequate
monitoring and supervision
Cardiovascular MRI in this setting can be technically
demanding and the signal loss and magnetic field inhomogeneity
induced by the device may limit the diagnostic yield of this
imaging technique
Background
Cardiovascular MRI in patients with ICADs
Little data available in the literature
Background
We hypothesized that specific cardiovascular
MRI in patients with pacemakers or ICDs can
be safely performed

Objective
To evaluate the safety, feasibility and
diagnostic utility of cardiovascular MRI in
patients with ICADs not specifically designed
for the MRI enviroment

Consecutive patients with PM/ICDs from September 2007 to January
2011 referred for medically necessary cardiovascular MRI
MRI system: Siemmens Magneton-Avanto MR-2004-V 1.5T
Devices should be in place for at least 6 weeks
Epicardial and abandoned leads excluded
Systematic safety protocol (pre-, during and post-MRI)
Methods

Adverse events, symptoms
Changes in electrical parameters
Variables
Device weight and volume
Change of MRI acquisition protocol to avoid device artifacts
Signal Loss Area (SLA)
Safety and Feasibility
Effects on Image Quality
Indication for cardiovascular MRI
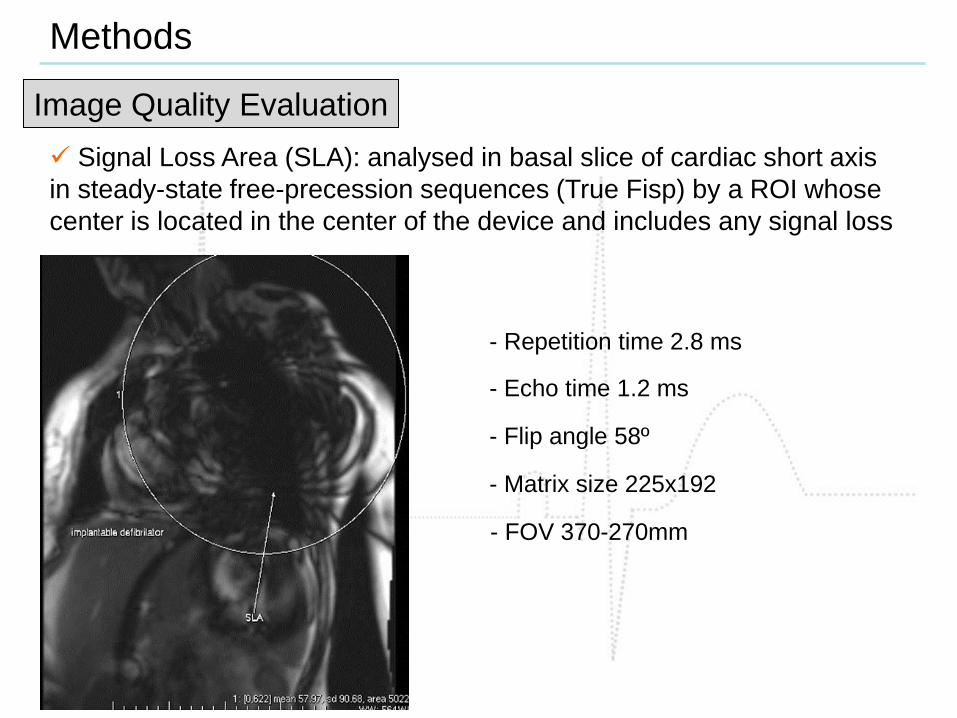
Signal Loss Area (SLA): analysed in basal slice of cardiac short axis
in steady-state free-precession sequences (True Fisp) by a ROI whose
center is located in the center of the device and includes any signal loss
Methods
Image Quality Evaluation
- Repetition time 2.8 ms
- Echo time 1.2 ms
- Flip angle 58º
- Matrix size 225x192
- FOV 370-270mm
Empirically if a great SLA was observed:
Methods
Protocol Change
1. Change of sequences: True Fisp for Turbo Flash sequences (spoiled
gradient echo sequence)
2. Use of magnetic field homogenitation tools (SHIM)
MRI was considered non-conclusive when it failed to solve the clinical
questions raised for each individual patient.
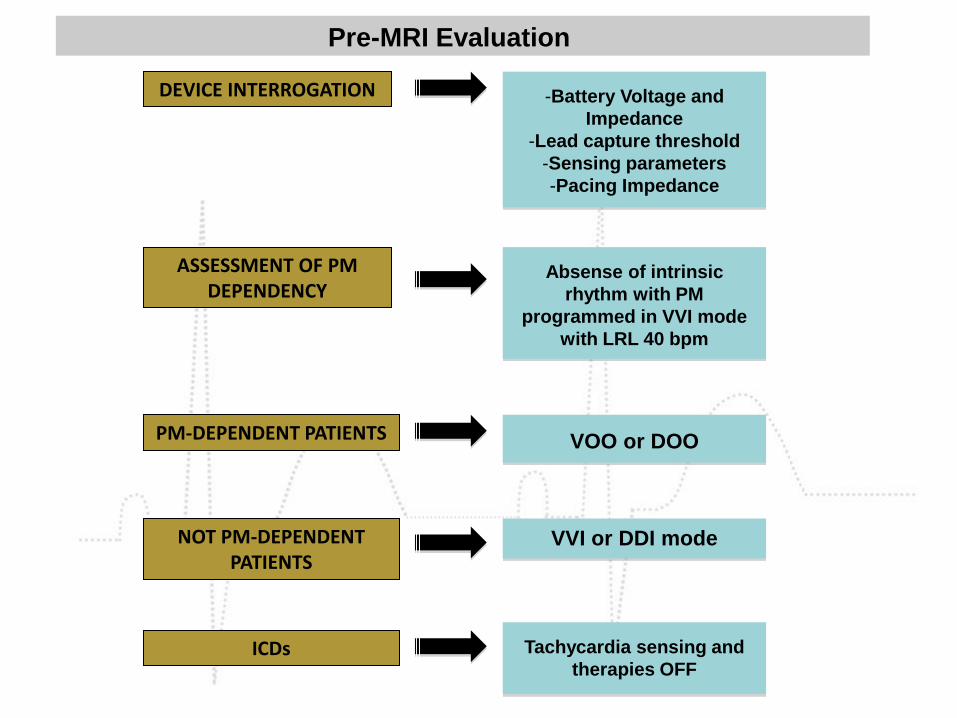
DEVICE INTERROGATION -Battery Voltage and
Impedance
-Lead capture threshold
-Sensing parameters
-Pacing Impedance
Pre-MRI Evaluation
Absense of intrinsic
rhythm with PM
programmed in VVI mode
with LRL 40 bpm
ASSESSMENT OF PM DEPENDENCY
PM-DEPENDENT PATIENTS
NOT PM-DEPENDENT PATIENTS
VOO or DOO
VVI or DDI mode
ICDs Tachycardia sensing and
therapies OFF

HEART RATE AND O2 SATURATION MONITORING
MR compatible optically
encoded ECG and
pulse oximetry
(Invivo® 3155MVS)
Evaluation During-MRI
CONTINOUS AUDIO CONTACT
EXPERIENCED CARDIOLOGIST PRESENT
DURING THE SCAN
FULL RESUSCITATION EQUIPMENT
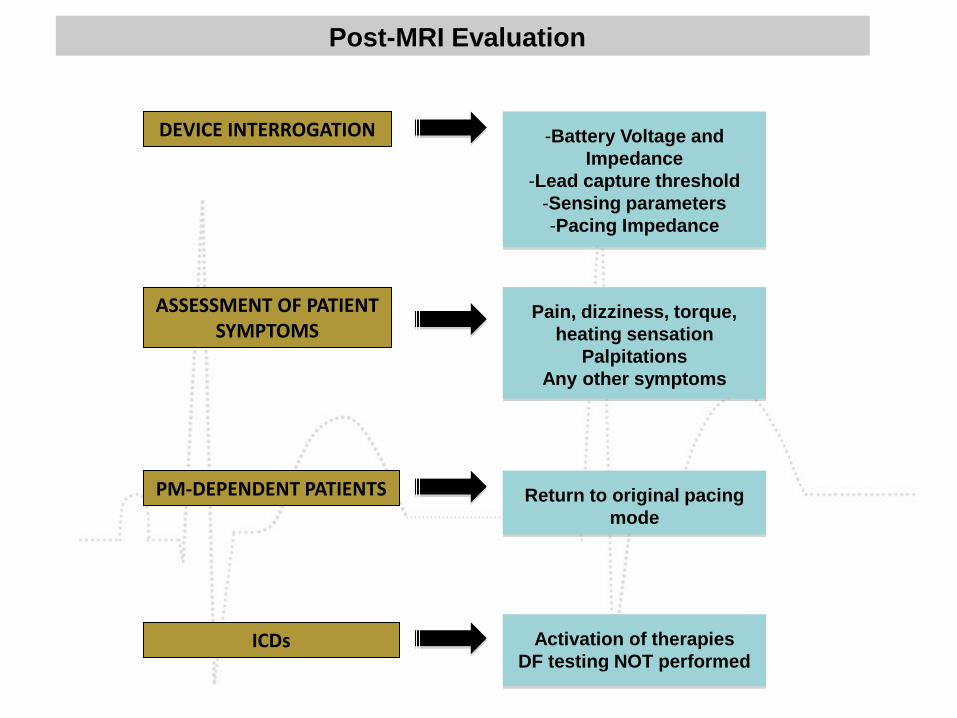
DEVICE INTERROGATION -Battery Voltage and
Impedance
-Lead capture threshold
-Sensing parameters
-Pacing Impedance
Post-MRI Evaluation
Pain, dizziness, torque,
heating sensation
Palpitations
Any other symptoms
ASSESSMENT OF PATIENT SYMPTOMS
PM-DEPENDENT PATIENTS Return to original pacing
mode
ICDs Activation of therapies
DF testing NOT performed

Results
Baseline characteristics of the population sample
42 cardiovascular MRI were performed in 41 patients (35 PM and 7 ICDs)
11 patients were PM-dependent
No serious MRI-related adverse events occurred in any patient
All the scans were completed

Results
Baseline characteristics of the population sample

Results
Baseline characteristics of the population sample

Results
Electrical Parameters Pre- and Post-MRI
Maximal AP threshold increase 0.12V in 1 patient
Maximal VP threshold increase 0.25V in 1 patient
Results
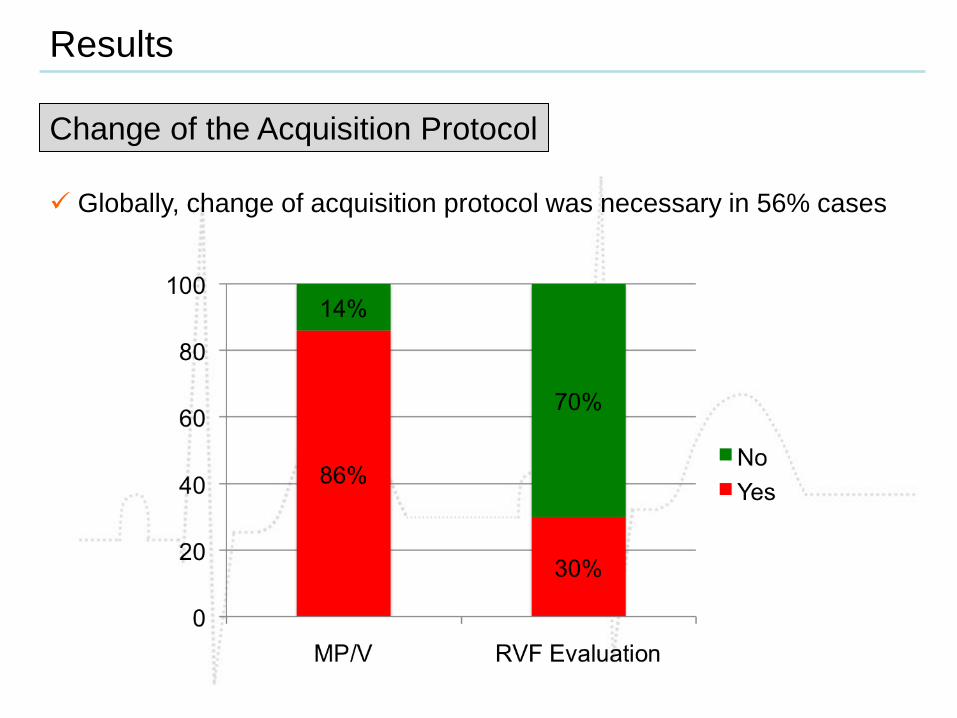
Change of the Acquisition Protocol
Globally, change of acquisition protocol was necessary in 56% cases
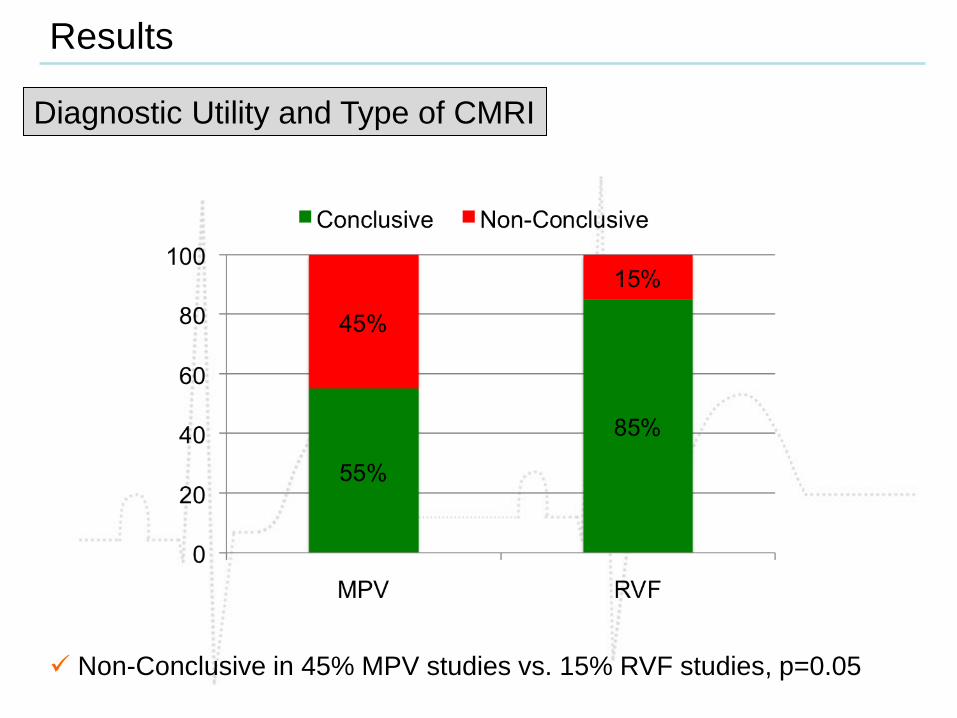
Diagnostic Utility and Type of CMRI
Non-Conclusive in 45% MPV studies vs. 15% RVF studies, p=0.05
Results
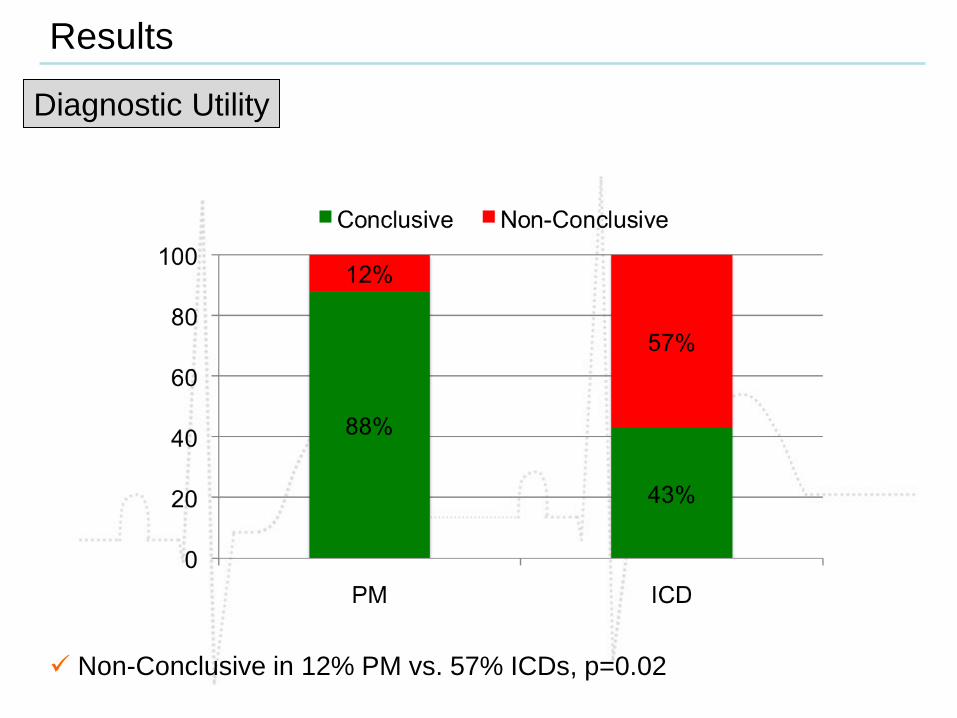
Diagnostic Utility
Results
Non-Conclusive in 12% PM vs. 57% ICDs, p=0.02

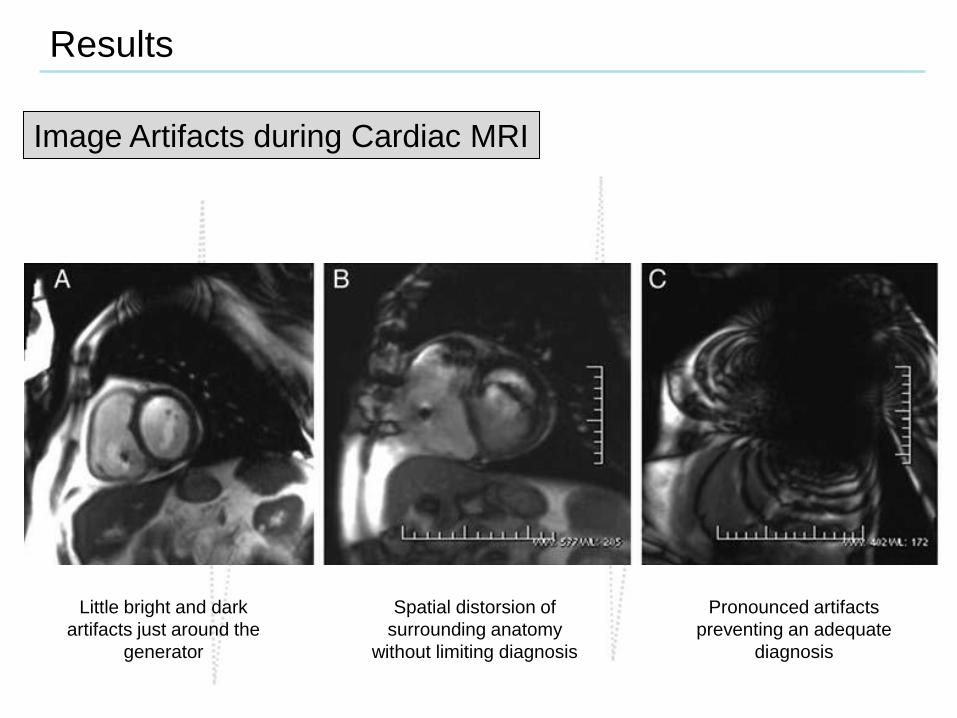
Image Artifacts during Cardiac MRI
Results
Results
Image Artifacts during Cardiac MRI
Spatial distorsion of
surrounding anatomy
without limiting diagnosis
Pronounced artifacts
preventing an adequate
diagnosis
Little bright and dark
artifacts just around the
generator
Cardiovascular MRI can be safely performed in patients with PM or ICD
No significant MRI-related complications occurred during or after MRI
Electrical parameter changes were minimal and comparable pre- and
post-MRI examinations
Conclusions
Myocardial perfusion/viability MRI scans in patients with high volume
devices should not be advised, due to the high incidence of non-
conclusive scans
Diagnostic utility depends on the device (ICD vs PM) and the clinical
indication of the MRI