Embed Size (px)
Citation preview
Declining value of alanine aminotransferase in screening of blood donors to prevent posttransfusion
hepatitis B and C virus infection
M.P. BUSCH, J.J. KORELITZ, S.H. KLEINMAN, S . R . LEE, J.P. AUBUCHON, G.B. SCHREIBER, AND THE RETROVIRUS EPIDEMIOLOGY DONOR STUDY
Background: Since the mid-1 98Os, blood banks in the United States have screened donors for elevated alanine aminotransferase (ALT) in an effort to prevent posttrans- fusion hepatitis. The present study was designed to quantitate the residual value of ALT screening following the implementation of hepatitis C virus (HCV) assays. Study Design and Methods: Two approaches were used. First, a database of 2.3 million donations made by 586,507 volunteer blood donors between 1991 and 1993 was used to compare the incidence of seroconversion to hepatitis B virus (HBV) and HCV marker positivity in donors with elevated ALT values and with normal ALT values. Second, the duration ofALT elevation prior to HBV and HCV seroconversion was determined from 34 well-documented cases of posttransfusion HBV and HCV; elevated-ALT window periods were multiplied by rates of HBV and HCV incidence in donors to project the yield of ALT screening. Predictive value and cost-effective- ness anal ses were also performed to compare the value of ALT screening before
Results: Both approaches indicate that ALT testing does not detect HBV in the win- dow phase but does currently identify approximately 3 HCV window-phase dona- tions per 1 million donations; this contrasts with ALT detection of approximately 1800 HCV-infectious units per 1 million donations prior to anti-HCV screening. Currently, only 8 in 10,000 donated units with elevated ALT (negative anti-HCV) are infected with HCV. The cost of continued ALT screening was estimated at $7,931,000 per
8 onciuslon: The yield, predictive value, and cost-effectiveness of ALT screening of blood donors have declined dramatically with the implementation of progressively improved anti-HCV assays. ALT screening of volunteer blood donors should be dis- continued.
and after L CV screening was implemented.
uality-adjusted year of life saved.
Abbreviations: ALT = alanine aminotransterase; EIA(s) = enzyme-linked Immunoassay(s); EIA-1 = tlrstgeneratlon EIA; EIA-2 = second generatlon EIA; EIA-3 = thirdgeneration EIA; HBc = hepatltls B core antlgen; HBsAg = hepatltls B surface antigen; HBV = hepatitis q virus; HCV= hepatitls C virus; QALY = quallty-adjusted life years; REDS = Retrovirus Epidemiology Donor Study.
IN 1986 AND 1987, United States blood banks intro- duced alanine aminotransferase (ALT) and hepatitis B core antibody (anti-HBc) tests as routine donor-screen- ing assays to reduce the risk of posttransfusion non- A,non-B hepatitis in blood recipients. This decision was based on findings from two prospective posttransfusion
From the Irwin Memorial Blood Centers and the University of 6%- fornia, San Francisco, California; Westat, Inc., Rockville, Maryland; Uni- versity of California, Los Angels., California; Ortho Diagnostics Systems, Raritan, New Jersey; and Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire.
Supported by contracts N01-HB-97077 (superseded by NOl-HB-
97081, and N01-HB-97082 from the National Heart, Lung, and Blood Institute.
Received for publication June 13, 1995; revision received July 24, 1995. and accepted August 7,1995.
TRANSFUSION 1995;35:90~910 .
471 14), N01-HB-97078, NOI-HB-97079, N01-HB-97080, NO1-HB-
hepatitis studies conducted in the late 1970s.’” These studies showed that the exclusion of donors with elevated ALT or anti-HBc would reduce the incidence of non- A,non-B hepatitis by 21 to 43 percent; the predicted effi- cacy of screening with both surrogate tests approached 50 percent. These predictions were later confirmed by studies conducted subsequent to the discovery of hepati- tis C virus (HCV) and determination that HCV is the major etiologic agent of non-A,non-B hepatitis4 For ex- ample, Donahue et al.5 and Nelson et a1.6 documented a 31-percent reduction in the per-unit risk of HCV infec- tion in transfusion recipients (from 52 to 36 serocon- versions/1000 units transfused) following the introduc- tion of non-A,non-B hepatitis surrogate tests. Similar results were recently reported by Blajchman et al.’ on the basis of a prospective randomized trial of ALT and anti-
903

904 BUSCH ET AL. TRANSFUSION V c d . 3 . No. I I-lYY5
HBc screening conducted in Canada. The utility of sur- rogate marker screening in the era before HCV screen- ing is also substantiated by the observation that, among contemporary first-time donors who were confirmed to be anti-HCV-positive, approximately 55 percent tested positive for one or both of these markers.8.'
In contrast, i t is unclear whether surrogate marker screening of volunteer donors continues to have signifi- cant value subsequent to the implementation of anti-HCV screening assays. Aach et al."' reanalyzed the implicated donor samples from the Transfusion-Transmitted Viruses Study from the 1970s, by using contemporary (second- generation) anti-HCV assays, and they concluded that surrogate marker screening would not have prevented transmissions of HCV that were not prevented by anti- HCV screening. Similarly, recent prospective posttrans- fusion hepatitis studies conducted in Canada and Spain, where surrogate marker screening was not implemented, have failed to establish any efficacy of ALT or anti-HBc screening since anti-HCV screening Finally, recent, well-controlled laboratory studies using polymer- ase chain reaction have failed to identify hepatitis B vi- rus (HBV) or HCV infection in hundreds of elevated- ALT12 or anti-HBc-reactiveI3 units that had tested negative for hepatitis B surface antigen (HBsAg) and anti- HCV markers.
Nonetheless, several arguments have been put forward in favor of retaining ALT in donor screening. The pri- mary concern relates to posttransfusion hepatitis due to blood from window-period donors who later serocon- verted for HBsAg or anti-HCV; analysis of HCV sero- conversion data suggests that a portion of such donations would likely be interdicted by ALT testing.l4-I6 Second, reports have appeared of persons with HBV or HCV in- fections (some of whom have elevated ALT) who are not identified by conventional serologic assay^.^^.'^ Third, there is preliminary evidence supporting the existence of at least one additional transfusion-transmissible hepati- tis virus, although the incidence of posttransfusion hepa- titis due to this virus appears to be low (compared to that of HBV and HCV), and there is no evidence that surro- gate markers would identify carriers of this virus."
In the present study, we use two approaches to mea- sure the value of ALT screening in the detection of win- dow-period HBV and HCV infections. The first approach involves direct comparisons of rates of seroconversion to HBV and HCV positivity among a large population of contemporary donors with elevated and normal ALT re- sults. The second, a two-step approach, involves estima- tion of the duration of the elevated-ALT window period preceding HBsAg and anti-HCV positivity on the basis of data from serial specimens from cases of posttrans- fusion hepatitis. The elevated-ALT window-period esti- mates are then multiplied by the observed rates of HBV and HCV seroconversion among donors to project the rate
of window-period HBV or HCV infections detectable by ALT screening. We also calculated the predictive value and cost-effectiveness of ALT screening of donors, both before and after the implementation of anti-HCV screen- ing.
Materials and Methods Incidence analysis by ALT level
The rates of seroconversion to HBV and HCV marker posi- tivity among donors with normal and elevated ALT were deter- mined by using the database of the National Heart, Lung, and Blood Institute Retrovirus Epidemiology Donor Study (REDS).2U This study involves five geographically separate blood centers in the United States (Irwin Memorial Blood Cen- ters, San Francisco, CA; Oklahoma Blood Institute, Oklahoma City, OK; and three American Red Cross Blood Services: Greater Chesapeake and Potomac Region, Baltimore, MD; Southeastern Michigan Region, Detroit, MI; and Southern Cali- fornia Region, Los Angeles, CA), which togethcr collect I . I million units of blood per year. The incidence analysis is based on donors who made two or more donations during the 3 years from January 1991 through December 1993.
For HBV markers, we examined rates of seroconversion to confirmed (neutrdlizabk) HBsAg positivity and anti-HBc re- activity over the entire study period. For HCV, we performed separate incidence rate analyses for the periods during which first- and second-generation anti-HCV enzyme immunoassays (EIA-1 and -2) were employed. The anti-HCV EIA-1 analysis period, within which the first donation was made, extended from June 1, 1991, when confirmatory (recombinant immunoblot assay) results were routinely available, and March 31, 1992, the date of transition to anti-HCV EIA-2. The anti-HCV EIA-2 analysis period extended from April 1, 1992, to December 31, 1993.
A set of intervals was produced for each donor on the basis of consecutive pairs of donation dates and test results. For do- nors who made two donations, one interval was formed. For donors who made three donations, two intervals were formed (based on donations 1 and 2 and donations 2 and 3); for donors who made more than three donations, intervals were produced on the same basis. An interval was included in the rate calcu- lation if the first donation of the interval was a transfusable do- nation (i.e., nonreactive on all serologic screening tests) or if the first donation was not transfusable only because of slightly elevated ALT. An incident HBV or HCV case was defined as one in which there was a change from nonreactive on the first donation of the interval to confirmed-positive (or repeatably re- active for anti-HBc) on the second donation of the interval. The incidence rate was calculated (separately for intervals in which the first donation had a normal ALT and slightly elevated ALT level) as the number of incident cases divided by the sum of the person-time ( k . , the sum of all days between the donation dates of the included intervals). We then multiplied the inci- dence rates by the length of the HCV preseroconversion win- dow, estimated as the time from transfusion to seroconversion in anti-HCV EIA-2, to project the risk of an infectious but seronegative donation for each period, with and without ALT screening.
Because donors with highly elevated ALT (2 2 x the cutoff) are notified of their results and deferred from subsequent do- nations, infected donors with highly elevated ALT are unlikely to return when they would demonstrate HBV or HCV sero- conversion. To avoid the bias that the absence of this group

TRANSFUSION 1 W5-Vol. 35. No. I I ALT SCREENING OF BLOOD DONORS 905
would create, we restricted the primary analysis to donors with normal and slightly elevated ALT (1-2 x cutoff). An adjustment was made to estimate the effect of including in the analysis donations with highly elevated ALT. This adjustment was based on the ratio of anti-HCV prevalence among units with highly elevated and slightly elevated ALT that were given by first-time donors (i.e., donors who had not previously been screened for anti-HCV). The observed incidence of anti-HCV in units with slightly elevated ALT was then multiplied by this prevalence ratio to estimate the incidence in units with highly elevated ALT. We determined the impact of eliminating ALT screening by computing the incidence rates for each of the three ALT groups (normal, slightly elevated, and highly elevated) and combining these according to their relative frequencies in the total REDS database of allogeneic donations (98.4% with normal ALT, 1.4% slightly elevated ALT, and 0.2% highly elevated ALT). A simi- lar approach was applied to adjust the observed predictive value estimates.
Elevated-ALT window-period analysis
To estimate the duration of ALT elevation preceding HBsAg or anti-HCV positivity, we examined data on the source of the blood in 13 cases of posttransfusion HBVZ' and 21 cases of posttransfusion HCVIb infection reported in the literature. The time between the first elevated-ALT donation and the first spe- cific marker-positive specimen was determined for each case. The average durations of the elevated-ALT preseroconversion windows were then calculated by summing the time for each case and dividing by the number of cases. The yield of ALT screening in the detection of window-phase HBV or HCV was then projected by multiplying the incidence of HBV and HCV observed among donors in the REDS study by the average du- ration of the elevated-ALT preseroconversion window period. For this purpose, we used an incidence for HCV seroconversion based on donors who were screened two or more times in the anti-HCV EIA-2 between April 1, 1992, and December 31, 1993.
Cost-effectiveness analysis
We utilized the data derived from this study in a modifica- tion of a previously published decision analysis mode122-24 to represent posttransfusion hepatitis outcomes in large, hypotheti- cal cohorts of patients undergoing transfusion with units of blood tested according to different protocols: ALT testing only, anti- HCV EIA-2 testing only, or both tests. The model calculates the net cost (/unit) of testing as the difference in average trans- fusion-related costs for recipients of tested and untested units. Similarly, the model calculates the net benefit of testing as the difference in quality-adjusted life expectancy for recipients of tested and untested units. Cost-effectiveness is then calculated as the ratio of net cost to net benefit.
In calculating net transfusion-related costs, the model incor- porates direct and indirect costs associated with testing as well as the costs of treating patients with transfusion-related hepa- titis and its complications. Indirect testing costs included those for notification of deferred donors, recruitment of replacement donors, publicity on testing decisions, and defense of associ- ated litigation. We estimated the direct and indirect incremen- tal costs of ALT testing to be $2.50 per unit and the public re- lations and legal costs of a decision not to test to be $0.25 per unit, although we varied the total testing-related costs widely in sensitivity analysis ($0-10) to reflect uncertainty in these estimates. We estimated the direct and indirect costs of anti- HCV testing to be $2.50 more than the costs of ALT testing.
The methods and data used to estimate the expected lifetime costs of treating posttransfusion hepatitis in both the acute and chronic phases have been described in detail in previous analy- ses.22-24 To simplify this quantitation and allow for consider- ation of new treatments, we increased to $l,OOO per case the estimated lifetime average incremental (present value) cost of the management and treatment of posttransfusion HCV in pa- tients with clinically evident disease to $20,000 per case and the cost of follow-up of patients with subclinical HCV infections.
The net benefit of ALT testing was calculated as the differ- ence in quality-adjusted life expectancy for hypothetical cohorts of recipients of tested or untested units. The transmission prob- abilities that were applied were those developed in this work: no testing for ALT or anti-HCV, 0.00448 (1/223); testing for ALT alone, 0.00278 (1/359); testing for anti-HCV EIA-2 alone, O.ooOo125 (1/80,257); and testing for both ALT and anti-HCV EIA-2, 0.0000097 (1/103,306). These incidences were tested over a broad range in sensitivity analysis. The probability that infection would lead to clinical disease was estimated as 0.5 percent.
We assumed that all recipients were at risk for development of acute and chronic sequelae of posttransfusion hepatitis. Post- transfusion longevity was reflected in the mean survival times assigned to patients receiving units tested in different protocols, which incorporated death due to underlying disease, hepatitis, and other causes. Mean survival after transfusion was estimated from published data as 10.7 years (with discounting) for all patients.z To estimate long-term survival in patients with chro- nic posttransfusion hepatitis, we initially used an excess mor- tality rate of 0.35 percent per year.22-24 In sensitivity analysis, we lowered the projected average posttransfusion longevity in the presence of posttransfusion hepatitis to as little as 1 year.
Discounting was performed at 5 percent per year to convert future costs and benefits to present value.% The effects of mor- bidity were included as quality adjustments of the extended l i f e ~ p a n ~ ~ - ~ ~ ; thus the benefits of testing are stated in quality- adjusted life years (QALY). We used software (Decision Maker, version 7.0, SG Pauker, Boston, MA) for modeling and analy- s ~ s . ~ ~ All costs were estimated in 1994 dollars.
Results During the 3-year analysis period, 2,962,229 units of allo-
geneic blood were collected at the five participating blood cen- ters. Of these, 2,318,356 were given by 586,507 multiple-time donors. There were 1,731,849 intervals for evaluation of sero- conversion rates.
HBV The rates of seroconversion to positivity for hepatitis B mark-
ers (HBsAg, anti-HBc) in donors with normal and slightly el- evated ALT values are given in Table l. None of the 33 donors identified as representing HBsAg incident cases had elevated ALT at the time of their preseroconversion donation. The HBsAg incidence rates were thus essentially identical for donors with normal ALT levels and for all donors (including those with slightly elevated ALT), with the latter reflecting the HBsAg incidence that would have occurred in the absence of screen- ing for slight ALT elevation. Similarly, the incidence of donor seroconversion to anti-HBc reactivity was essentially identical for donors with normal ALT, those with slightly elevated ALT, and all donors. Since the anti-HBc test is prone to nonspecificity and a confirmatory assay is not available, it is probable that a very high proportion of these cases of anti-HBc reactivity are unrelated to HBV exposure.

906 BUSCH ET AL. TKANS1:USION Vo1.3S. Nu. I l-l'llJS
Table 1. Relationship of donorALTstatus and incidence of HBsAgand anti-HBc HBsAg anti-HBc
Incident Person- Incidence Incident Person- Incidence ALT status cases years* Ratet (95% CI) cases years Rate (95% CI) Normal 33 801,553 4.12 (2.8-5.6) 4,170 799,450 522 (506-538) Slightly elevated 0 8,790 0 (0-34.1) 45 8,763 51 4 (374-675)
Total 33 810,343 4.07 12.8-5.6) 4.21 5 808.213 522 (506-537)
Person-time (days) times 365 days/year. t Incidence rates = seroconversion to marker positivity per 100,000 person-years. Because HBsAg is positive for only a brief period after
infection, the HBsAg incidence rate may underestimate total HBV incidence.
Table 2. Relationship of donor ALTstatus and incidence of HCVinfection HCV EIA-1 -screened donors HCV EIA-2-screened donors
ALT status of donation
Incident Person- Incidence cases* years Ratet (95% CI)
Incident Person- Incidence cases years Rate (95%CI)
Normal 159 227,352 69.9 (59.5-81.2) 14 324,355 4.3 (2.4-6.9) Slightly elevated 17 2,804 606.3 (352.3-928.7) 2 3,177 63.0 (5.9-1 80.5)
Total 176 230,156 76.5 (65.6-88.2) 16 327,532 4.9 (2.8-7.6)
* Nonreactive on anti-HCV EIA-1 followed by repeatable reactivity on anti-HCV EIA-2 and positivity on recombinant irnmunoblot assay. t Incident cases per 100,000 person-years.
This apparent failure of ALT testing to detect window-phase' donations from donors who seroconvert to HBV marker posi- tivity was supported by examination of ALT and HBsAg data on the donors in the 13 posttransfusion HBV cases. In all do- nors without a preexisting or concurrent HCV infection, ALT elevation was detected several weeks after detection of HBsAg. Thus, ALT screening appears to be of no value i n the early detection of HBV infection in donors.
HCV The rates of seroconversion to confirmed anti-HCV positivity
in donors with normal versus slightly elevated ALT are given in Table 2. Incidence rates were calculated separately for do- nation intervals in which the earlier donation screened as nega- tive in anti-HCV EIA-1 with the subsequent donation screened with anti-HCV EIA-2 and for donation intervals in which both donations were screenec! with anti-HCV EIA-2. Although there is a similar total of person-years of observation for the EIA- L - and EIA-2-screened donors, i t is notable that more than 10 times as many newly diagnosed HCV infections were observed among those who previously were negative i n EIA-I than among those who were negative in EIA-2 (176 vs. 16). Most of the appar- ently higher incidence in the EIA-1 screening period represents the enhanced sensitivity of the second-generation test for iden- tification of donors with chronic HCV infection (ix., donors identified as seropositive by EIA-2 who had tested false-nega- tive in the EIA-l), rather than true incident HCV cases. The
difference between the crude incidence rates i n the two scrcen- ing periods, 71.6 per 100,000 person-years, represents the rate of identification by HCV EIA-2 of HCV-seroposilive donors missed by HCV EIA-I; this result is consistent with findings i n studies that directly compared performance of the first- and second-generation ElAs in testing of large numbers of donor samples.'
With regard to ALT, donors with slightly elevated values were significantly more likely (pe0.001) than those with nor- mal ALT to seroconvert to anti-HCV positivity during both the EIA-1 and EIA-2 screening periods. However, the apparent incidence of HCV seroconversion in donors with slightly ele- vated ALT was 10 times greater during the EIA-1 screening period than during the EIA-2 period (606 vs. 63/100,11110 pcr- son-years). Note that the best estimate of HCV incidence dur- ing the EIA-2 screening period in all donors (equivalent to no screening for slight elevations of ALT) exceeds that i n the nor- mal ALT group by 14 percent (4.9 vs. 4.3, respectively); how- ever, the CIS overlap significantly because there were relatively few donations with slightly elevated ALT.
To estimate the impact of discontinuing ALT screening on the risk of HCV infection among recipients, we used the point estimates for HCV incidence among EIA-2-screened donors, with or without exclusion of units on the basis ofthe ALT level. These incidence rates were multiplied by an 81.9-day estimate of the duration of the HCV seroconversion window period,'" which yielded estimates for the probability of collecting ii unit from a donor in the preseroconversion window-phase of HCV
Table 3. Projected effect on HCVrisk ofdiscontinuing ALTscreening Incidence rate per Window period* Residual risk per
ALT screening 100,000 person-years (CI) Days (Years) rr,illion units (CI) Continue 4.3 (2.4-6.9) 81.9 (0.2242) 9.7 (5.3-1 5.4) Continue for highly elevated ALT levels only 4.9 (2.8-7.6) 81.9 (0.2242) 11 .O (6.2-17.0) Discontinuet 5.6 (3.2-8.6) 81.9 (0.2242) 12.5 (7.1-19.3)
Based on time from transfusion to anti-HCV EIA-2 positivity. t Adjustment assumes that the incidence rate in donations with highly elevated ALT level is 3.4 times greater than rate in donations with
slightly elevated ALT levels (see Table 5) and that, among all allogeneic donations, 98.4 percent have normal ALT, 1.4 percent have slightly elevated ALT, and 0.2 percent have highly elevated ALT (see Materials and Methods).
ALT SCREENING OF BLOOD DONORS TRANSRlSlON IIW5-Vtd 3.5. Nil. I I 907
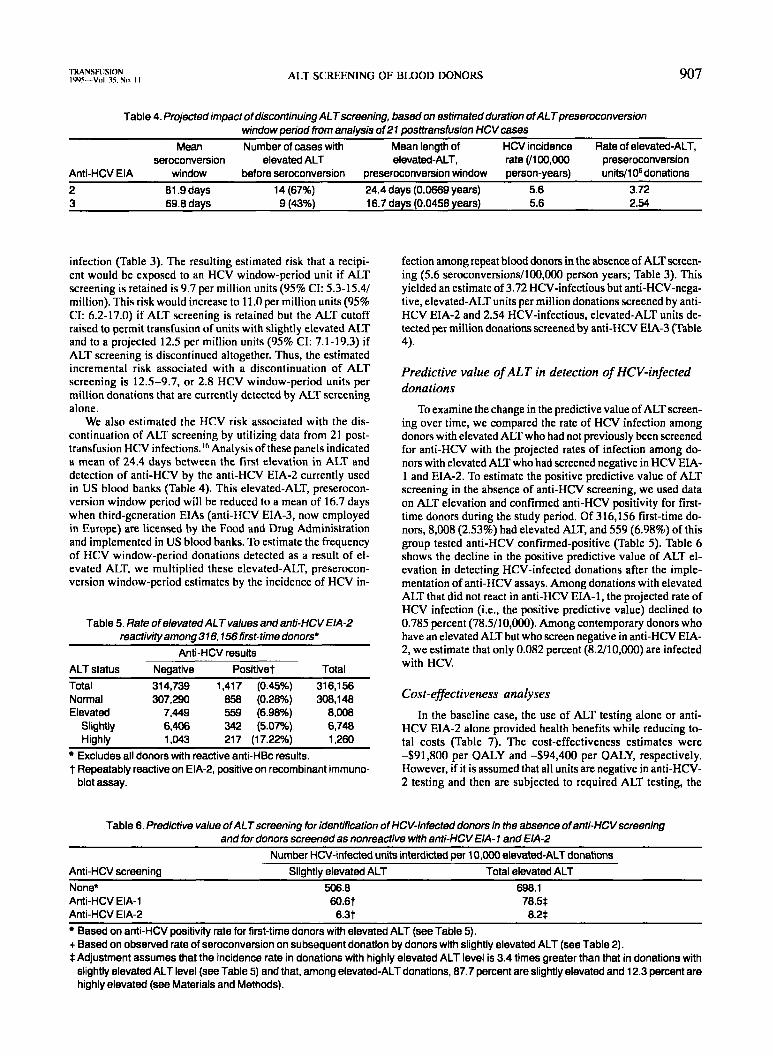
Table 4. Projected impact of discontinuing ALTscreening, based on estimatedduration ofALTpreseroconversion window period from analysis of 27 posttransfusion HCVcases
Mean Number of cases with Mean length of HCV incidence Rate of elevated-ALT, sermnversion elevated ALT elevated-ALT, rate (/1OO,OOO preseroconversion
Anti-HCV EIA window before sermonversion preseroconversion window person-years) unitdl 06 donations 2 81.9 days 14 (67%) 24.4 days (0.0669 years) 5.6 3.72 3 69.8 days 9 (43%) 16.7 days (0.0458 years) 5.6 2.54
infection (Table 3). The resulting estimated risk that a recipi- ent would be exposed to an HCV window-period unit if ALT screening is retained is 9.7 per million units (95% CI: 5.3-15.4/ million). This risk would increase to 11.0 per million units (95% CI: 6.2-17.0) if ALT screening is retained but the ALT cutoff raised to permit transfusion of units with slightly elevated ALT and to a projected 12.5 per million units (95% CI: 7.1-19.3) if ALT screening is discontinued altogether. Thus, the estimated incremental risk associated with a discontinuation of ALT screening is 12.5-9.7, or 2.8 HCV window-period units per million donations that are currently detected by ALT screening alone.
We also estimated the HCV risk associated with the dis- continuation of ALT screening by utilizing data from 21 post- transfusion HCV infections.Ih Analysis of these panels indicated a mean of 24.4 days between the first elevation in ALT and detection of anti-HCV by the anti-HCV EIA-2 currently used in US blood banks (Table 4). This elevated-ALT, preserocon- version window period will be reduced to a mean of 16.7 days when third-generation EIAs (anti-HCV EIA-3, now employed in Europe) are licensed by the Food and Drug Administration and implemented in US blood banks. To estimate the frequency of HCV window-period donations detected as a result of el- evated ALT. we multiplied these elevated-ALT, preserocon- version window-period estimates hy the incidence of HCV in-
Table 5. Rate ofelevatedALT values andanti-HCVEIA-2 reactivityamong376,756first-time donors*
Anti-HCV results ALT status Negative Positivet Total Total 31 4,739 1,417 (0.45%) 316,156 Normal 307,290 858 (0.28%) 308,148
Slightly 6,406 342 (5.07%) 6,748 Elevated 7,449 559 (6.98%) ~ , m
Highly 1,043 217 (17.22%) 1,260 Excludes all donors with reactive anti-HBc results.
t Repeatably reactive on EIA-2, positive on recombinant immuno- blot assay.
fection among repeat blood donors in the absence of ALT screen- ing (5.6 seroconversions/100,000 person years; Table 3). This yielded an estimate of 3.72 HCV-infectious but anti-HCV-nega- tive, elevated-ALT units per million donations screened by anti- HCV EIA-2 and 2.54 HCV-infectious, elevated-ALT units de- tected per million donations screened by anti-HCV EIA-3 (Table 4).
Predictive value of ALT in detection of HCV-infected donations
To examine the change in the predictive value of ALT screen- ing over time, we compared the rate of HCV infection among donors with elevated ALT who had not previously been screened for anti-HCV with the projected rates of infection among do- nors with elevated ALT who had screened negative in HCV EIA- 1 and EIA-2. To estimate the positive predictive value of ALT screening in the absence of anti-HCV screening, we used data on ALT elevation and confirmed anti-HCV positivity for first- time donors during the study period. Of 316,156 first-time do- nors, 8,008 (2.53%) had elevated ALT, and 559 (6.98%) of this group tested anti-HCV confirmed-positive (Table 5). Table 6 shows the decline in the positive predictive value of ALT el- evation in detecting HCV-infected donations after the imple- mentation of anti-HCV assays. Among donations with elevated ALT that did not react in anti-HCV EIA-1, the projected rate of HCV infection (ix., the positive predictive value) declined to 0.785 percent (78.5/10,MM). Among contemporary donors who have an elevated ALT but who screen negative in anti-HCV EIA- 2, we estimate that only 0.082 percent (8.2/10,000) are infected with HCV.
Cost-effectiveness analyses
In the baseline case, the use of ALT testing alone or anti- HCV EIA-2 alone provided health benefits while reducing to- tal costs (Table 7). The cost-effectiveness estimates were -$91,800 per QALY and -$94,400 per QALY, respectively. However, if it is assumed that all units are negative in anti-HCV- 2 testing and then are subjected to required ALT testing, the
Table 6. Predictive value ofALTscreening for identification of HCV-infected donors in the absence of anti-HCVscreening and for donors screened as nonreactive with anti-HCV EIA- 7 and EIA-2
Number HCV-infected units interdicted per 10,OOO elevated-ALT donations Anti-HCV screening Slightly elevated ALT Total elevated ALT None* 506.8 698.1 Anti-HCV EIA-1 60.6t 78.5$ Anti-HCV EIA-2 6.3t 8.2$
Based on anti-HCV positivlty rate for first-time donors with elevated ALT (see Table 5). + Based on observed rate of seroconversion on subsaquent donation by donors with slightly elevated ALT (see Table 2). $Adjustment assumes that the incidence rate in donations with highly elevated ALT level is 3.4 times greater than that in donations with
slightly elevated ALT level (see Table 5) and that, among elevated-ALT donations, 87.7 percent are slightly elevated and 12.3 percent are highly elevated (see Materials and Methods).

908 BUSCH El’ AL. ‘I‘KANSI’USION Vul.3S.Nt1 I I - IWS
Table 7. Cost-effectiveness ofALT and anti-HCVscreening, when performed alone or implemented serially
HCV cases per Cost per
ALT alone (pre-HCV) 0.00448 (1/223) 0.00278 (1/359) 1,698 491,800
Test Risk of HCV without test Risk of HCV with test million units QALY sawed
Anti-HCV (no ALT) 0.00448 (1/223) 0.0000125 (1/80,257) 4,470 -$94,400 Anti-HCV (added to ALT) 0.00278 (1/359) 0.0000097 (1/103,306) 2,775 -$87,900 ALT (added to anti-HCV) 0.00001 25 (1/80,257) 0.0000097 (1/103,306) 2.8 +$7,931,000
cost-effectiveness of ALT testing is estimated at +$7,931,000. This result is most sensitive to the probability of disease trans- mission, but the cost-effectiveness of ALT testing remains above $100,000 per QALY for probability estimates of transmission without ALT testing that are nine times greater than estimates from the data presented in this report and above $50,000 per QALY for probability estimates of transmission that are an or- der of magnitude above this study’s estimates. Although some studies have suggested that no excess mortality can be attrib- uted to transfusion-transmitted HCV in long-term follow-up of a large group of patients,w we elected to use a moderate mor- tality estimate in the model to allow for the consideration of a positive effect of testing on patient mortality. However, the cost- effectiveness estimate of ALT testing performed in addition to anti-HCV-2 testing remained above $155,000 per QALY even when the expected average effect on patient longevity after transmission of hepatitis exceeded 95 percent of the nominal posttransfusion longevity (data not shown). Variation i n the values of other variables iicross broad ranges did not result in substantial changes in the results of the model.
Discussion
The present study documents a marked decline in the yield of ALT as a screening test for posttransfusion hepa- titis and in the detection of HCV-infected blood donations in particular. Data from a variety of sources have estab- lished that, prior to anti-HCV EIA screening, ALT test- ing of donors prevented approximately one-third of post- transfusion HCV infections.’-8 On the basis of a decrease in the prevalence of HCV infection from 0.45 percent in all first-time donors to 0.28 percent in first-time donors with normal ALT, we estimated that 1700 HCV-infected units were interdicted as a result of ALT testing for every million units transfused in the period before anti-HCV screening. In contrast, using two separate approaches, we estimate that, in today’s setting of anti-HCV EIA-2 screening, only 2.8 to 3.7 infected units missed by spe- cific anti-HCV tests are detected by ALT screening for every million units screened. This represents a 99.8-per- cent decrease in yield with respect to the prevention of posttransfusion HCV infection. We further projected that the anti-HCV EIA-3 currently awaiting Food and Drug Administration approval will reduce the ALT presero- conversion window by approximately 8 days and conse- quently will reduce the already low residual value of ALT by another third.
The predictive value of elevated ALT €or detecting HCV infection has declined in parallel with the declin- ing yield of the test. Before anti-HCV screening was ini-
tiated, approximately 7.0 percent of donated u n i t s with elevated ALT were infected with HCV (Table 5), but now only 8 in 10,000 elevated-ALT units that test negativc for anti-HCV in EIA-2 actually are infected with HCV (Tdble 6). Thus, in the absence of anti-HCV screening, 1 HCV- infected unit was interdicted for every 13 elevated-ALT uni t s discarded, while, for anti-HCV EIA-2-screened donations, 1226 units are discarded for each HCV win- dow-period infection detected; this change represents a reduction of more than 98 percent in predictive value.
Despite this marked decline in predictive value, ALT testing does detect a small number of early HCV infec- tions. We estimated that the elimination of ALT screen- ing would result in transfusion of 2.8 to 3.7 additional HCV-infectious units per million units transfused, or 50 to 67 HCV-infected units per year. This would represent an approximately 30-percent increase in the risk of HCV infection from window-period donations (Table 3). Imple- mentation of the anti-HCV EIA-3 would partially offset, but not eliminate, this increased risk. Moreover, i t is possible that ALT testing may have some value i n idcn- tifying persons with atypical HBV or HCV infections who lack HBsAg, anti-HBc, or anti-HCV that is detectable by current assay^,'^^^^ as well as ii proportion of donors in- fected by putative additional hepatitis viruses that can be transmitted by transfusion. Evidence allowing quanti- tation of the value of ALT in the prevention of such in- fections is not available, and i t is likely that such benefit is small compared to the yield of ALT in detecting win- dow-period HCV infection documented in the present study.
The cost-effectiveness model constructed with the in - fection prevalence data derived in this study indicatcs that only a small health care benefit is associatcd with con- tinued use of ALT testing now that sensitive HCV anti- body tests are available. This benefit, at a cost of $7,931,000 per QALY, far exceeds the cost-effectiveness estimates of most other commonly accepted mcdical in- terventions, which are generally below $50,000 per QALY.2y-3z While cost-effectiveness determination is sen- sitive to the probabilities of disease transmission and hepatitis-related mortality used in the model, thc cost- effectiveness estimate far exceeded the $50,000 per QALY threshold when all plausible values were used for these variables. Thus, the cost-effectiveness analysis serves to quantify the extremely limited utility that ALT testing
TRANSFUSION IYYS-Vul. 35. Nu. I I ALT SCREENING OF BLOOD DONORS 909
currently offers. This extremely limited utility is in con- trast to the effect of ALT testing when anti-HCV was not available or of anti-HCV testing alone or in addition to ALT testing; these testing protocols provide increased longevity while reducing total costs.
In conclusion, our analysis shows a dramatic decline in the yield, predictive value, and cost-effectiveness of ALT screening of blood donors. On the basis of these data, both a National Institutes of Health consensus conference and a Food and Drug Administration advisory commit- tee recently recommended the discontinuation of ALT screening.” Blood organizations are now finalizing plans and procedures for discontinuing the test. This process exemplifies the ways in which critical analysis of test utility and cost-effectiveness should drive rational deci- sion making, even in an area as emotionally and legally charged as blood safety.
Acknowledgments
statistical work and Barbara Johnson for manuscript preparation. The authors thank Robin McEntire, PhD, of Westat for extensive
1.
2.
3.
4.
5 .
6.
7.
8.
9.
10.
11.
12.
References Aach RD, Szmuness W, Mosley JW, et al. Serum alanine amino- transferase of donors in relation to the risk of non-A, non-B hepatitis in recipients: the transfusion-transmitted viruses study. N Engl J Med 1981;304:989-94. Alter HJ, Purcell RH, Holland PV, Alling DW, Koziol DE. Do- nor transaminase and recipient hepatitis. JAMA 1981;246:630-4. Alter HJ, Holland PV. Indirect tests to detect the non-A, non-B hepatitis carrier state. Ann Intern Med 1984;101:859-61. Kuo G, Choo QL, Alter HJ, et al. An assay for circulating anti- bodies to a major etiologic virus of human non-A, non-B hepa- titis. Science 1989;244:362-4. Donahue JG, Mufioz A, Ness PM, et al. The declining risk of post-transfusion hepatitis C virus infection. N Engl J Med
Nelson KE, Ahmed F, Stambolis V, Ness PM, Yawn D, McAllister H. Incident hepatitis C virus (HCV) and hepatitis B virus (HBV) infections in transfused cardiac surgery patients: infection rates during different methods of donor screening. In: Proceedings of NIH Consensus Development Conference: infec- tious disease testing for blood transfusions. Bethesda: National Institutes of Health, 199557-9. Blajchman MA, Bull SB, Feinman SV. Post-transfusion hepati- tis: impact of non-A, non-B hepatitis surrogate tests. Lancet
Kleinman S, Alter H, Busch M, et al. Increased detection of hepatitis C virus (HCV)-infected blood donors by a multiple- antigen HCV enzyme immunoassay. Transfusion 1992;32:805- 13. Katkov WN, Friedman LS, Cody H, et al. Elevated serum ala- nine aminotransferase levels in blood donors: the contribution of hepatitis C virus. Ann Intern Med 1991;115:882-4. - Aach RD, Stevens CE, Hollinger FB, et al. Hepatitis C virus in- fection in post-transfusion hepatitis. An analysis with first- and second-generation assays. N Engl J Med 1991;325:1325-9. Esteban JI, Camps J, Genesca J, Alter HJ. Hepatitis C and B: new developments. In: Nance SJ, ed. Blood safety: current challenges. Bethesda: American Association of Blood Banks,
Sankary TM, Yang G, Romeo JM, et al. Rare detection of hepa- titis B and hepatitis C virus genomes by polymerase chain reac- tion in seronegative donors with elevated alanine aminotrans- ferase. Transfusion 1994;34:656-60.
1992;327:369-73.
1995;345:2 1-5,
1992:45-96.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
Douglas DD, Taswell HF, Rakela J, Rabe D. Absence of hepati- tis B virus DNA detected by polymerase chain reaction in blood donors who are hepatitis B surface antigen negative and anti- body to hepatitis B core antigen positive from a United States population with a low prevalence of hepatitis B serologic mark- ers. Transfusion 1993;33:212-6. Lelie PN, Cuypers HT, Reesink HW, et al. Patterns of serologi- cal markers in transfusion-transmitted hepatitis C virus infec- tion using second-generation HCV assays. J Med Virol
Courouce AM, Le Marrec N, Girault A, Ducamp S, Simon N. Anti-hepatitis C virus (anti-HCV) seroconversion in patients undergoing hemodialysis: comparison of second- and third- gen- eration anti-HCV assays. Transfusion 1994;34:790-5. Barrera JM, Francis B, Ercilla G, et al. Improved detection of anti-HCV in post-transfusion hepatitis by a third-generation ELISA. Vox Sang 1995;68:15-8. Lai ME, Farci P, Figus A, et al. Hepatitis B virus DNA in the serum of Sardinian blood donors negative for the hepatitis B surface antigen. Blood 1989;73:17-9. Alter MJ, Margolis HS, Krawczynski K, et al. Natural history of community-acquired hepatitis C in the United States. N Engl J Med 1992;327:1899-905. Alter HJ. Transfusion transmitted hepatitis C and non-A, non- B, non-C. Vox Sang 1994;67(Suppl3):19-24. Zuck TF, Thomson RA, Schreiber GB, et al. The Retrovirus Epi- demiology Donor Study (REDS): rationale and methods. Trans- fusion 1995;35:944-51. Mimms LT, Mosley JW, Hollinger FB, et al. Effect of concur- rent acute infection with hepatitis C virus on acute hepatitis B virus infection. Br Med J 1993;307:1095-7. Birkmeyer JD, Goodnough LT, AuBuchon JP, Noordsij PG, Littenberg B. The cost-effectiveness of preoperative autologous blood donation for total hip and knee replacement. Transfusion
Birkmeyer JD, AuBuchon JP, Littenberg B, et al. The cost-ef- fectiveness of preoperative autologous donation in coronary ar- tery bypass grafting. Ann Thorac Surg 1994;57:161-9. AuBuchon JP, Birkmeyer JD. Safety and cost-effectiveness of solvent-detergent-treated plasma. In search of a zero-risk blood
Vamvakas EC, Taswell HF. Mortality after blood transfusion. Transfus Med Rev 1994;8:267-80. Weinstein MC. Clinical decision analysis. Philadelphia: W.B. Saunders, 1980. Sonnenberg FA, Pauker SG. Decision Maker: an advanced per- sonal computer tool for clinical decision analysis. In: Proceed- ings of the Eleventh Annual Symposium on Computer Applica- tions in Medical Care. Washington: IEEE Computer Society Press, 1988. Seeff LB, Buskell-Bales Z, Wright EC, et al., and the NHLBl Study Group. Long-term mortality after transfusion-associated non-A, non-B hepatitis. N Engl J Med 1992;327:1906-11. Weinstein MC, Stason WB. Cost-effectiveness of coronary ar- tery bypass surgery. Circulation 1982;66(Suppl3):56-66. Evans RW. Cost-effectiveness analysis of transplantation. Surg Clin North Am 198666503-16. Stange PV, Sumner AT. Predicting treatment costs and life expectancy for end-stage renal disease. N Engl J Med
Etchason J, Petz P, Keeler E, et al. The cost effectiveness of preoperative autologous blood donations. N Engl J Med
NIH consensus statement on infectious disease testing for blood transfusion. Bethesda: National Institutes of Health, 1995.
1992;37:203-9.
1993i33544-5 1.
supply. JAMA 1994;272:1210-4.
1978;298:372-8.
1995;332:719-24.
Michael P. Busch, MD, PhD, Associate Professor in Residence, Department of Laboratory Medicine, University of California, San Francisco; and Vice-President, Research and Scientific Services, Irwin Memorial Blood Centers, 270 Masonic Avenue, San Francisco, CA 941 18. [Reprint requests]
James. J. Korelitz, PhD, Senior Study Director, Westat, Inc., Rock- ville, MD.

910 BUSCH ET AL. TRANSFUSION Vul.35.No. I I-IWS
Steven H. Kleinman, MD, Professor, Department of Pathology and Laboratory Medicine, and Co-Director, Transfusion Medicine, University of California, Los Angeles, CA.
Stephen R. Lee, PhD, Manager, Hepatitis Research and Devel- opmcnt, Ortho Diagnostics Systems, Raritan, NJ.
James P. AuBuchon, MD, Professor, Department of Pathology, Dartmouth-Hitchcock Medical Center, Lebanon, NH.
George B. Schreiber, DSc, REDS Principal Investigator, Westat, Inc., Rockville, MD.
The Retrovirus Epidemiology Donor Study (REDS Study Group) is presently the responsibility of the following persons: Blood Centers:
Potomac Region: A.E. Williams (Holland Laboratory), C.C. Nass American Red Cross Blood Services, Greater Chesapeake and
American Red Cross Blood Services, Southeastern Michigan
American Red Cross Blood Services, Southern California Region:
Irwin Memorial Blood Centers: E.L. Murphy (UCSF), M.P. Busch Oklahoma Blood Institute: R.O. Gilcher, J.W. Smith
Westat, Inc.: G.B. Schreiber, R.A. Thomson
Region: H.E. Ownby, D.A. Waxman
S.H. Kleinman (UCLA Medical Center), S. Hutching
Medical Coordinating Center:
National Heart, Lung, and Blood Institute: G.J. Nemo Steering Committee Chair: T.F. Zuck (Hoxworth Blood Center)














![CASE REPORT – OPEN ACCESS - COnnecting REpositories · ( -GTP), 587IU/L] and hepatic dysfunction [aspartate aminotrans-ferase (AST), 603U/L; alanine aminotransferase (ALT), 414U/L]](https://img.pdfslide.net/doc/110x75/5fe447d63616553e0750a168/case-report-a-open-access-connecting-repositories-gtp-587iul-and-hepatic.jpg)














