Embed Size (px)
Citation preview

Decreased fetal erythropoiesis Kell hemolytic anemia
and hemolysis in
Carl P. Weiner, MD, and J o h n A. Wiriness, MD
Iowa City, Iowa
OBJECTIVE: Lower changes in optical density (450 nm) measurements have been reported in fetuses with anti-Ketl anemia compared with those with anti-D anemia. The purpose of this investigation was to determine if hemolysis and erythropoiesis differ between anti-Kell and anti-D hemolytic disease. STUDY DESIGN" Ninety-three pregnancies complicated by either anti-D or anti-Kell alloimmunization were evaluated. Fetal blood samples obtained at the first cordocentesis were tested for the red blood cell antigen type, hemoglobin, hematocrit, reticulocyte count; nucleated red blood cells, total serum bilirubin concentration, umbilical venous respiratory blood gases, serum erythropoietin level, and strength of the direct Coombs test. To determine the evolution of hemolytic anemia in the two antigen groups, these laboratory parameters were repeated on the fetal blood samples triggering the decision to perform a fetal intravascular transfusion (hematocrit <30%). RESULTS: A total of 65 of 93 fetuses were antigen positive (11 for Kell and 54 for RhD). The mean gestational age and laboratory measurements of antigen-positive, nonanemic fetuses at first blood sampling did not differ significantly between groups. There was a strong inverse relationship observed between the hemoglobin concentration and reticulocyte count independent of gestational age in the anti-D group but not in the anti-Kell group. Eight (73%) fetuses with anti-Kell antibodies and 37 (69%) with anti-D antibodies underwent intravascular transfusion. At the cordocentesis when the decision for transfusion was made, anti-Kell anemic fetuses had lower reticulocyte counts and total bilirubin concentrations. The strong inverse relationship between the hemoglobin and reticulocyte count was again seen only in the anti-D group. In both groups, fetal erythropoietin increased significantly between the first and last blood samplings and in each group were negatively correlated with hemoglobin independent of gestational age. CONCLUSION: Anti-Kell anemic fetuses have lower reticulocyte counts and total serum bilirubin levels than do comparable anti-D anemic fetuses. This finding argues in favor of fetal blood sampling rather than amniotic fluid analyses for the management of fetal hemolytic disease resulting from Kell antibodies. Unlike RhD alloimmunized fetuses, these fetuses do not manifest an inverse relationship between hemoglobin concentration and reticulocyte count. We speculate that, compared to anti-D fetal anemia, anti-Kell anemia is associated with increased hemolysis of nonhemoglobinized or incompletely hemoglobinized erythroid precursors. (AM J OBsrEr GYNECOL 1996;174:547-51 .)
Key words: Pregnancy, Rh disease, cordocentesis
Several investigators have observed that women with
Kell a l lo immuniza t ion and an affected fetus have lower
amniot ic fluid changes in optical density (450 nm) mea-
surements than do comparable women with D al loimmu-
nization. 1' ~ More recently Vaughan et al? r epor t ed that,
in addit ion to having significantly lower changes in opti-
cal density measurements , anemic Kel l -a l loimmunized
b¥om the Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, and the Division of Neonatology, Department of Pedi- atrics, University of Iowa College of Medicine. Supported in part by United States Public Health Service grants No. HL49041 (C.P. V~), HL51735 (C.P.W.), and HL46925 ff.A. W.). Received for publication February 10, 1995," revised May 23, 1995; accepted June 5, 1995. Reprint requests': Carl P. Weiner, MD, Department of Obstetrics and Gynecology, University of Iowa College of Medicine, Iowa City, IA 52242. Copyright © 1996 by Mosby-Year Book, fne. 0002-9378/96 $5.00 + 0 6/1/66801
fetuses have lower reticulocyte counts compared with fe-
tuses with D al loimmunizat ion. Al though the fetal biliru-
bin concentra t ions measured in stored samples f rom Kell
fetuses were also lower, the difference did no t reach sta-
tistical significance. The authors at tr ibuted their findings
to rapid equil ibrat ion of bi l irubin across the placenta.
However, normal fetal serum bil irubin concentra t ions
are significantly h igher than maternal bi l i rubin concen-
trations. 4 Because erythropoie t in concentra t ions were
no t measured in this or pr ior studies, it is no t possible to
de te rmine whether the low reticulocyte counts in anti-
Kell anemic fetuses are due to increased fetal hemolysis
or to an inadequate response of the fetus to the anemia.
We h)q~othesized that anti-Kell anemic fetuses would have
significantly lower reticulocyte counts and bil irubin levels
than would comparable anti-D anemic fetuses. On the
basis of exper ience with the evaluation of fetal hemolytic
547

548 Weiner and Widness February 1996 AmJ Obstet Gynecol
Table I. Character is t ics ( m e a n + SD) of fetuses with D a n d Kell a l l o i m m u n i z a t i o n at first cordocentes i s where
h e m a t o c r i t was >30%
anti-D anti-Kell
Gestational age (wk) Hemoglobin (gm/dl) Hematocrit (%) Reticulocytes (% red blood cells) Absolute reticulocytes (xl0~/lal) Nucleated red blood cells (per 100 white blood cells) Total bilirubin (mg/dI) Erythropoiedn (mU/ml)
27-+4 (41) 25-+3 (7) 11.8 -+ 2.4 (41) 12.5 -+ 1.9 (7)
36-+7 (41) 38-+6 (7) 9.5-+7 (37) 11.5-+4 (7)
250 -+ 104 (37) 345 -+ 114 (7)* 15.4-+21 (41) 22.5-+9 (7)
2.4-+0.9 (28) 2.1-+0.7 (5) 9.1 -+ 4 (28) 8.0 + 3 (7)
Values in parentheses indicate number of fetuses studied. Comparisons exclude fetuses with hematocrit <30% at first cordocentesis; these may be found in Table II.
*p < 0.05. However, normalized for gestational age, there is no difference in absolute reticulocyte count between groups. Mean reticulocyte counts in both groups are above 97.5th percentile of mean for healthy, control fetuses of same gestational age. 6
Table II. Character is t ics ( m e a n + SD) of fetuses with D a n d Kell a l l o i mmu n i za t i o n at cordocen tes i s d ic ta t ing
n e e d for t rans fus ion
anti-D anti-Kell
Gestational age (wk) Hemoglobin (gm/dl) Hematocrit (%) Reticulocytes (% red blood cells) Absolute reticulocytes (xl0~/pl) Nucleated red blood cells (per 100 white blood cells) Total bilirubin (mg/dl) Erythropoietin (mU/ml)
28.8-+5 (37) 27.2+6 (8) 7 .7+3 (37) 6.0_+4 (8)* 23-+8 (37) 18-+11 (8)*
13.6-+7 (37) 5.7-+4 (8)+ 218-+106 (37) 91 -+91 (8)?
28.4 -+ 72 (35) 3.2 -+ 4 (8) 4.1-+2 (21) 2.7+_1 (5)t
32.6 -+ 31 (37) + 40.2 -+ 44 (8) +
Values in parentheses indicate number of fetuses studied. Comparisons exclude fetuses with hematocrit <30% at first cordocentesis.
*p < 0.10, p > 0.05 from anti-D group. t p < 0.05 from anti-D group. ++p < 0.05 from first blood sample (excludes fetuses whose first sample revealed hematocrit <30%).
disease with fetal b lood sampling, 5 we specu la ted tha t
these d i f fe rences would no t be p r e s e n t be fore the onse t
of anemia . Thus the pu rpose of the c u r r e n t invest igat ion
was to d e t e r m i n e w h e t h e r hemolysis a n d e ry thropoies i s
differ be tween fetuses with anti-Kell and anti-D hemoly t ic
anemia . To accompl i sh this, we c o m p a r e d m e a s u r e m e n t s
of fetal p l a sma e r y t h r o p o i e t i n c o n c e n t r a t i o n , fetal s e r u m
b i l i rub in , a n d o t h e r hema to log i c p a r a m e t e r s be fore a n d
af ter the d e v e l o p m e n t of fetal anemia .
Methods
Nine ty - th ree p r egnanc i e s compl i ca t ed by e i t he r anti-D
or anti-Kell a l l o i m m u n i z a t i o n were evaluated in the Uni-
versity of Iowa Fetal Diagnosis a n d T r e a t m e n t Uni t , as
previously descr ibed. 4' 5 T h e h e m o g l o b i n concen t r a t i o n ,
hematoc r i t , re t iculocyte c o u n t (bo th p e r c e n t a g e of the
total r ed b l o o d cells a n d the absolu te n u m b e r ) , n u c l e a t e d
r ed b l o o d cells, total s e r u m b i l i rub in concen t r a t i o n , um-
bilical b l o o d gases a n d pH, s e r u m e r y t h r o p o i e t i n level,
a n d s t r eng th of the d i rec t C o o m b s test for each fetus were
m e a s u r e d in b l o o d samples o b t a i n e d at the first co rdo-
centesis. Sixty-five of the 93 fetuses (70%) were ident i f ied
as an t i g en positive (anti-D, n = 54; anti-Kell, n = 11) a n d
compr i se the study popu la t ion .
Ant igen-posi t ive fetuses were ass igned a p a t t e r n of risk
for deve lop ing severe hemoly t ic a n e m i a an tena ta l ly o n
the basis of the results of the first cordocentes is . ~ This
p a t t e r n was used to d e t e r m i n e if a n d w h e n the nex t
cordocen tes i s was to be p e r f o r m e d . Trans fus ion the rapy
was in i t ia ted w h e n the fetal h e m a t o c r i t level dec l ined to
<30%. This value is below the 2.5th pe rcen t i l e for all
ges ta t ional ages af ter 20 weeks. ~ Excep t for the d i rec t
C o o m b s test, these same l abora to ry p a r a m e t e r s were
m e a s u r e d again in the fetal b l o o d sample, which trig-
ge red the decis ion to p e r f o r m a fetal in t ravascular t rans-
fusion. Amnio t i c f luid optical densi ty m e a s u r e m e n t s were
n o t ob ta ined .
T h e t e c h n i q u e s used for cordocen tes i s a n d intravascu-
lar t rans fus ion a n d the i r compl i ca t ion rates have b e e n
desc r ibed previously. 6' 7 Each p r o c e d u r e used a h i g h - r e s o -
lu t ion sector or cu rved l inear u l t r a s o n o g r a p h y t rans-
d u c e r with an a t tached , f ixed ang le -need le guide (Civco
Medical In s t rumen t s , Kalona, Ia.).
T h e f indings are p r e s e n t e d as the m e a n +_ 1 SD. Analy-

Volume 174, Number 2 Weiner and Widness 549 AmJ Obstet Gynecol
ses inc luded Pearson correlat ion, stepwise mult iple l inear
regression, i n d e p e n d e n t t test, analyses of variance, and
Kruskal-Wallis one-way analysis of variance for the non-
parametrical ly distr ibuted e ry thropoie t in data. Because
of the l imited sample volume, no t all laboratory values
were available for all fetuses. A corre la t ion or difference
yielding p < 0.05 was accepted as indicat ing significance.
R e s u l t s
~rhen the hematocr i t was >30%, there were no signifi-
cant differences between the two groups in any study
variable (Table I). The re was a strong inverse relat ionship
be tween hemog lob in concent ra t ion and reticulocyte
count in the D-a l lo immunized fetuses that was indepen-
den t of gestational age ( r = - 0 . 7 3 , p < 0.0001). This in-
verse relat ionship was no t seen with the anti-Kell g roup
( r= 0.52, p = 0.10). The loss of this relat ionship suggests
that fewer reticulocytes are en te r ing the per iphera l circu-
lation f rom the marrow. The 17 fetuses who had a hemat-
ocrit <30% at the first b lood sample were placed in the
pretransfusion group (Table II) for the purpose of statis-
tical analyses (see below).
Forty-five fetuses of the 65 (69%) antigen-posit ive fe-
tuses (8 with anti-Kell and 37 with anti-D) had anemia
severe e n o u g h to unde rgo one or more fetal intravascular
transfusions. The percen tage o f fetuses with Kell and D
a l lo immuniza t ion requir ing transfusion did no t differ sig-
nificantly (anti-Kell 73%; anti-D 69%).
At the cordocentesis when the decision for intravascu-
lar transthsion was made, anti-Kell anemic fetuses had
significantly lower reticulocyte counts (both percen t and
absolute) and total bi l i rubin concentra t ions (Table II and
Figs. 1 to 3). Umbil ical venous pH and b lood gas values
did no t differ be tween the two groups. In both groups the
fetal e ry thropoie t in concent ra t ions increased signifi-
cantly (p < 0.05) between the first and last b lood sam-
plings and were negatively corre la ted with hemoglob in
i n d e p e n d e n t of gestational age (anti-D, r = - 0 . 6 1 , p =
0.0004; anti-Kell, r= -0.79, p = 0.05). Nine of the 45 had
hematocr i t levels at or jus t above 30% when the intravas-
cular transfusion was planned. These n ine had shown a
steadily d ropp ing hematocr i t over the course of our
evaluation, leading us to the predict they would soon have
a hematocr i t <30%. That predic t ion was correct in all
instances. Each fetus had a hematocr i t <30% at transfu-
sion. The m e a n interval between this "dec is ion" sample
and the actual transfusion was 4 days for the anti-D group
and 1 day for the anti-Kell g roup (not significant).
The strong inverse relat ionship no ted at the t ime of the
first sample between the hemog lob in concent ra t ion and
reticulocyte count i n d e p e n d e n t of gestational age in the
D-a l lo immunized fetuses persisted in the sample ob-
ta ined when the decision to transfuse was made
( r= -0.62, p < 0.0001) (Fig. 4). Again, it was no t s e e n in
Hematocrit (%)
50
40
30
20
10
o" O•o %
®
o ~
• IP
0 I I I
® • anti D O anti K e l l
I I i I I 1 I ._ . . I
18 20 22 24 26 28 30 32 34 36 38 40
G e s t a t i o n (weeks)
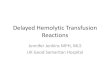
Fig. 1. Fetal hematocrit of antigen-positive fetuses at cordocen- tesis when decision for fetal intravascular transfusion was made plotted against 95% confidence interval for population of nor- mal fetuses (shaded area). Solid circles, Anti-D fetuses; open circles, anti-Kell fetuses.
the Kel l -a l loimmunized group ( r= 0.12, p = 0.64) (Fig.
5). The loss of this expected relat ionship in the anti-Kell
anemic fetuses is consistent with their significantly lower
reticulocyte counts.
C o m m e n t
The cur ren t investigation demonstra tes that there are
intrinsic differences in the hemolytic pat tern associated
with RhD and Kell a l lo immune anemia. Consistent with
the repor t o fVaughan et al., ~ we find that Kell a l loimmu-
nization is, in contrast to RhD, associated with the loss of
the anticipated inverse relat ionship between hemoglob in
and reticulocyte count. This suggests e i ther an inappro-
priate response by the Kel l -a l loimmunized fetus to ane-
mia or the destruct ion of the reticulocytes before or after
they en ter the per iphera l circulation. Also consistent with
the findings of Vaughan et al. was our f inding that anti-
Kell fetal anemia is associated with lower reticulocyte
counts than in comparable anemic fetuses with anti-D
at loimmunizat ion. This f inding is even more remarkable
when it is cons idered that both the mean hematocr i t and
the gestational age of the Kell g roup before transfusion
t ended to be somewhat lower than in the D group. Low
hematocr i t and early gestational age would both be ex-
pected to increase, not decrease, the reticulocyte count.
In contrast to Vaughan et al., 3 who found no significant
difference in total bil irubin between anti-Kell and D
groups, we found that fetuses with anti-Kell hemolytic
anemia have significantly lower total bi l i rubin measure-
ments compared with those with anti-D hemolytic ane-
mia. We suggest the lower total bi l i rubin accounts for the
reports of low measurements of del ta optical density at

550 Weiner and Widness February 1996 AmJ Obstet Gynecol
Reticulocytes (% RBC)
28
21
14
• anti D O anti Kell
0 0 •
O •
I ° I I • I ° I • 1 20.5 23.5 26.5 29.5 32.5 >34
Gestation (weeks)
Fig. 2. Fetal reticulocyte counts (percent red blood cells [RBCs]) of antigen-positive fetuses at cordo- centesis when decision for fetal intravascular transfusion was made plotted against 95% confidence interval of mean from normal fetuses (shaded area). Solid circles, Anti-D fetuses; open circles, anti-Kell fetuses.
T . B .
m g / d L
10.0
8.0
6.0 f • anti D O anti Kell
o• • 4 , 0 • • • • O • •
2.0
0 I I I I I I I I 20 22 24 26 28 30 32 34 36
Gestation (weeks)
Fig. 3. Fetal total bilirubin (T.B.) (in milligrams per deciliter) of antigen-positive fetuses at cordocentesis when decision for fetal intravascular transfusion was made plotted against 95% confidence interval for population of normal fetuses (shaded area). Solid circles, Anti-D fetuses; open circles, anti-Kell fetuses.
450 nm in Kell-sensitized pregnancies manifest ing pro-
found fetal anemia. This f inding also argues in favor of
fetal b lood sampling ra ther than amniot ic fluid analysis
for the m a n a g e m e n t of fetal hemolytic disease caused by
Kell a l loimmnnizat ion. The f inding that the reticulocyte
counts in fetuses with Kell a l lo immunizat ion are no t dif-
fe ren t than in those with D a l lo immuniza t ion before the
deve lopmen t of anemia indicates that the a lgor i thm u s e d
to assign risk in a l lo immunized pregnancies n e e d no t be
changed. 5 We note that Vaughan et al. measured biliru-
bin in samples that had been stored for several months
and observed a nonsignif icant t rend toward lower biliru-
bin levels in the Kell group. No informat ion is provided regarding storage conditions. Because bi l i rubin is pho to-
degraded, this factor a lone likely accounts for the dis-
crepancy with the cur ren t study.
There are several possible explanat ions for the low
reticulocyte counts and serum bi l i rubin in fetuses with
anti-Kell anemia. First, there may be inadequa te release
of e ry thropoie t in by the anemic fetus in response to the
associated hypoxemia. Our f inding of increasing serum
erythropoie t in concent ra t ion in both RhD and Kell
groups as anemia developed effectively eliminates this
possibil i ty. In point, the mean ery thropoie t in level in
Kel l -a l loimmunized fetuses t ended to be h igher than in
the D-a l lo immunized fetuses when the decision for trans-
fusion was made. This f inding is consis tent with the ob-
servation that the Kell g roup ' s pretransfusion hemoglo -
bin and hematocr i t levels were slightly, but no t signifi-
cantly, lower than the RhD group. Second, anti-Kell
hemolyt ic anemia may be associated with inadequate
erythroid stem cell response to the appropriately in-
creased ery thropoie t in levels. This hypothesis cannot cur-
rently be tested in vivo. Third, Vaughan et al? suggested
that the Kell antibody might in terfere with erythroid
growth or different iat ion because the Kell ant igen pro-

t i "Volume 174, Number 2 We,net and Wm~ness gg4 Am J Obstet Gynecol
35
30
o o z, A
8 ' ~ 10 & c£
A t~
5 t a
0 I r I I I I I ~ .
0 5 10 15 20 25 30 35
Hematocrit %
I
4 0
Fig. 4. Relationship between fetal hematocrits and reticulocyte counts of D antigen-positive fetuses when decision for fetal intravascular transfusion was made. Regression line, Simple linear regression.
35
E g o
g- o
rr"
30
25
20
15
10
5
0 0
A
g~
2 I I I I I l l
5 10 15 20 25 30 35 40
Hemat0crit %
Fig. 5. Relationship between fetal hematocrits and reticulocyte counts of Kell antigen-positive fetuses when decision for fetal intravascular transfusion was made. Regression line, Simple linear regression.
rein s t ruc tu re resembles tha t of the zinc neu t r a l en-
dopep t idases 8 involved in the b i n d i n g of a variety of pep-
t ide h o r m o n e s . This testable hypothes is cou ld exp la in the
low ret iculocyte coun t s a n d total b i l i rub in at the t ime of
a n e m i a bu t if t rue shou ld also be associated with a low
ret iculocyte c o u n t be fo re the onse t of anemia . T h e l a t t e r
was n o t f o u n d in the c u r r e n t study. Four th , hemoly t ic ane-
mia may be associated with inc reased hemolysis of n o n h e -
m o g l o b i n i z e d or i ncomple t e ly h e m o g l o b i n i z e d e ry th ro -
cyte p r e c u r s o r cells in the m a r r o w w h e n c o m p a r e d with
a n e m i a caused by anti-D. T h e obse rva t ion tha t Kell anti-
gens are expressed o n the i m m a t u r e K562 e ry th ro leuke -
mia cell l ine suggests t ha t Kell is expressed early in r ed
b l o o d cell deve lopmen t f l We favor the f o u r t h hypothes is
because it accoun t s for all of the f indings in the c u r r e n t
study (i.e., Kell af fected fetuses with lower ret iculocyte
counts , lower b i l i rub in levels, e levated s e r u m ery th ropo i -
e t in levels, a n d n o inverse r e l a t ionsh ip be tween h e m o g l o -
b in c o n c e n t r a t i o n a n d ret iculocyte count) . In conclus ion ,
fetal re t iculocyte coun t s a n d b i l i rub in levels in fe tues with
Kell a l l o i m m u n e a n e m i a are lower t h a n in fetuses with
RhD a l l o i m m u n e a n e m i a in spite of appropr ia te ly in-
c reased fetal p lasma e r y t h r o p o i e t i n levels in b o t h groups.
These f ind ings a rgue in favor of fetal b l o o d sampl ing
r a t h e r t h a n amnio t i c f luid analysis for the m a n a g e m e n t of
fetal hemoly t ic disease caused by Kell a l lo immuniza t ion .
We t h a n k R o b e r t L. Sch mi d t for p e r f o r m a n c e of the e r y t h r o p o i e t i n rad io immunoassay .
R E F E R E N C E S
1. Caine ME, Mueller-Heubach E. Kell sensitization in preg- nancy. AM.J OBSTET GYNECOL 1986;154:85-90.
2. Berkowitz RL, Beyth Y, Sadovsky E. Death in utero due to Kell sensitization without excessive elevation of the delta OD 450 value in amniotic fluid. Obstet Gynecol 1982;60:746-9.
3. VaughanJl, Warwick R, Letsky E, Nicolini U, Rodeck CH, Fisk NM. Erythropoietic suppression in fetal anemia because of Kell alloimmunization. AM j OBSTET OYNECOL 1994;171:247- 52.
4. Weiner CR Human fetal bilirubin and fetal hemolytic disease. A~IJ OBSTET G~ECOL 1992;116:1449-54.
5. Weiner CP, Williamson RA, Wenstrom KD, Sipes SL, Grant SS, WidnessJA. Management of fetaI hemolytic disease by cordo- centesis, I: prediction of fetal anemia..&,a J OBSTET G~ECOL 1991;165:546-53.
6. Weiner CR Williamson RA, Wenstrom KD, et al. Management of fetal hemolytic disease by cordocentesis, II: outcome of treatment. ~&~aJ OBSTET G~ECOL 1991;165:1302-7.
7. Weiner CP, Wenstrom KD, Sipes SL, Williamsom RA. Risk factors for cordocentesis and fetal intravascular transfusion. AMJ OBSTET G~ECOL 1991;165:1020-5.
8. Lee S, Zambas ED, Marsh ~ , Redman CM. Molecular clon- ing and primary structure of Kell blood group protein. Proc Natl Acad Sci U S A 1991;88:6353-7.
9. McGinniss MH, Dean A. Expression of red cell antigens by K562 human teukaemia lines before and after induction of haemoglobin synthesis by hemin. Transfusion 1985;25: 105-9.




![Delayed-Onset Hemolytic Anemia in Patients with Travel ... · Delayed-onset anemia (herein referred to as postartesunate delayed-onset hemolysis [PADH] pattern of anemia) has been](https://img.pdfslide.net/doc/110x75/5e6bfc5b26d5f27b322eef74/delayed-onset-hemolytic-anemia-in-patients-with-travel-delayed-onset-anemia.jpg)