Embed Size (px)
Citation preview

Defects of Blastogenesis: Counseling Dilemmas inTwo Families
Greetje de Jong1* and Patricia A. Kirby2
1Division of Human Genetics, University of Stellenbosch and Tygerberg Hospital, Tygerberg, South Africa2Department of Neuropathology, Tygerberg Hospital, South Africa
Three patients are described with defects ofblastogenesis and predominantly midlinedefects. Two were sibs of whom the first-born were female cephalothoracopagus-conjoined twins with multiple predomi-nantly midline defects initially thought tobe a sporadic occurrence. A subsequentbrother presented with severe hydrocepha-lus, rhombencephalosynapsis, conotruncaldefect, ambiguous genitalia, and unilateralpre-axial polydactyly; an autosomal reces-sive defect is postulated in this case. Patient3 had hydrocephalus, small cerebellum,cleft lip and palate, and a large sacrococcy-geal teratoma, the better differentiated partof which included ovarian tissue with pri-mordial follicles. The latter may occur inincomplete twinning as a defect of blasto-genesis. The mother had had a previous ter-mination of a fetus with hydrocephalusfrom a different relationship. Counselingwas difficult since no examinations weredone on the previous fetus and no furtherinvestigations of this family could be ob-tained, but a genetic origin is suspected.Most defects of blastogenesis are sporadic;however, some cases have a genetic causeand ultrasound examinations should be of-fered in subsequent pregnancies. Am. J.Med. Genet. 91:175–179, 2000.© 2000 Wiley-Liss, Inc.
KEY WORDS: blastogenesis; counseling;midline defects; spondylocos-tal defects
INTRODUCTION
Formation of the midline and of the mesoderm areimportant events in blastogenesis and the beginning ofgastrulation [Opitz, 1993]. Defects of blastogenesis in-clude severe malformations with high lethality andtwinning [Opitz, 1993; Martınez-Frıas, 1995]. In aSpanish epidemiological study, Martınez-Frıas [1995]reported no sex difference and a low recurrence risk inpatients with blastogenetic midline defects comparedto those without midline defects. Comparing mothers ofinfants with blastogenetic defects with mothers of chil-dren with nonblastogenetic defects showed that a his-tory of previous spontaneous abortions is more commonin the former group [Martınez-Frıas and Frıas, 1997].Chronic teratogenic exposure and genetic influencewere proposed as possible contributing factors. How-ever, blastogenetic defects have been described in fami-lies with autosomal dominant [de Meeus et al., 1997],autosomal recessive [Debrus et al., 1997], and severalwith X-linked inheritance patterns such as the patientsof Mathias et al. [1987] and Mikkila et al. [1994].
We report on clinical and autopsy data on three ba-bies/fetuses with multiple defects of blastogenesis. Inspite of differing clinical presentation, we think thatthe two sibs (family 1) may represent an autosomalrecessive mutation. A sporadic defect cannot be ex-cluded in patient 3, but a previous fetus who also hadhydrocephalus, but was not further examined, castsdoubt on this postulate.
CLINICAL REPORTSFamily 1
Patient 1. Routine ultrasound examination at 22weeks of gestation demonstrated female cephalothora-copagus-conjoined twins with a single head, two arms,two legs, two kidneys each, but a single heart. TheCaucasian parents were young (father 26 and mother25 years old), nonconsanguineous, and reported nofamily history of twinning. The mother had a step-brother with spina bifida occulta. There was no historyof teratogen exposure and the pregnancy had been de-scribed as normal. Pregnancy was terminated by pros-taglandin induction; the twins had a combined weightof 450 g and were joined at the metopic sutures. Onehad a cleft lip and for descriptive purposes will be re-
Presented at the 6th International Workshop on Fetal Geneticpathology, Dead Sea, Israel, March 14–19, 1999.
Current address for P.A. Kirby: Department of Pathology, Uni-versity of Iowa Hospitals and Clinics, Iowa City, Iowa.
*Correspondence to: Greetje de Jong, Division of Human Ge-netics, PO Box 19063, Tygerberg 7505, South Africa.
Received 27 April 1999; Accepted 30 November 1999
American Journal of Medical Genetics 91:175–179 (2000)
© 2000 Wiley-Liss, Inc.

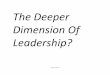
ferred to as twin 1, and the one to the right as twin 2(Fig. 1). Due to lateral rotation of the bodies, twin 1 wasto the left of twin 2. The abdominal walls between thetwo were not completely closed, exposing most of theabdominal contents of fetus 2. Both twins had tripha-langeal thumbs. Fetus 2 had unilateral pre-axial poly-dactyly. A deep cleft was present between one halluxand the other toes of twin 2. Twin 1 had moderatecervico-thoracic kyphoscoliosis and normal femalegenitalia. Twin 2 had marked cervico-thoracic kypho-scoliosis, a sacral spina bifida with covered myelome-ningocele, inverted feet, a cloaca, and uneven separa-tion of the labia majora. No blood could be obtained forchromosome analysis and fibroblast cultures were un-successful.
Autopsy. Both twins had well-developed skullbones. The dura was fused in the center above thebrains. A falx cerebri was present. The frontal lobeswere smaller than normal and separated by arachnoidonly. Each twin had two optic nerves but only one eyeto each face. Both had arhinencephaly with absence ofthe anterior fossa. The sella turcica of twin 1 containedno pituitary gland, but a tract that communicated withthe uncleft oropharynx-Rathke’s cleft. Twin 2 had asella turcica with pituitary gland. The rest of thebrains were appropriately developed. Each twin had a
trachea and anatomically normal but hypoplasticlungs. The pericardium was intact and the single hearthad four chambers. An atrial septal defect (ASD) waspresent. Pulmonary arteries originated from the leftaorta. There were two aortas, one arose from the rightventricle, then ran along the spine of twin 1 and even-tually fed into the umbilical cord. The other aorta arosefrom the left ventricle, ran along the spine of twin 2, itsdistal part becoming enmeshed in a hypoplastic mes-enteric plexus of vessels, which eventually also fed intothe umbilical cord. The veins of the cord predominantlycame from twin 1, but branches extended across fromtwin 2. The livers and biliary systems were normal andeach had a spleen and a thymus. Only one esophaguswas present, arising from both oropharynges. Theesophagus was patent and led into a single stomach.Most of the bowel belonged to twin 1, who had a patentanus. Twin 2 had a separate bowel consisting of thedistal ileum, appendix, and large intestine ending in ablind dilated pouch. Kidneys, ureters, bladder, and theinternal genitalia of twin 1 were normal. The kidneysof twin 2 were separated by a thin membrane only andwere tilted due to the severe kyphoscoliosis andcramped abdominal space so that the superior poleswere anteriorly oriented. The ureters were normal.Bladder and vagina formed a cystovaginocoele drainedby a tiny cloaca in the perineum. Attached to the cys-tovaginocoele were the (left) ovary and fallopian tube,while a right hypoplastic adnexal structure was at-tached to the pelvic wall. Deep to the separated labiamajora was a phallus-like structure with the cloaca atthe posterior end. Normal thyroid, adrenal and pancre-atic structures were present. The placenta appearednormal. No histologic study was done due to macera-tion.
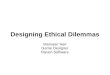
Patient 2. After a normal second pregnancy (nor-mal male), the mother presented in the third preg-nancy at 34 weeks of gestation with ultrasonographicevidence of “hydronephrosis” in the fetus. Third levelultrasonography showed severe hydrocephalus, normalcerebellum, no dilatation of the 4th ventricle, skin-covered vertebral defects, hydronephrosis, and am-biguous genitalia. Review of the photographs taken ofthe previous ultrasound examinations showed that hy-drocephalus had been developing since 20 weeks of ges-tation. The combination of anomalies was not like thatof any specific known syndrome, but acrocallosal, hy-drolethalus, Meckel, Smith-Lemli-Opitz syndromes,spondylocostal dysplasia, and Casamassina syndromewere considered. No history of exposure to teratogenswas reported and the mother did not have diabetesmellitus or a family history of the disease. The babywas delivered at 35 weeks of gestation by cesarean sec-tion due to hydrocephalus and previous cesarean sec-tion. The Apgar scores were 1, 2, 1 at 1, 5, and 10 min,respectively, and the baby died neonatally. The maleinfant weighed 2,810 g (<90th centile), measured 44 cmin length (>10th centile), had a head circumference of37.5 cm (>90th centile) and toe-heel length of 7.2 cm. Hehad a round head, hypertelorism, deep-set eyes andmicrognathia (Fig. 2). The sutures were widely sepa-rated. A third fontanel was present. There was pre-axial polydactyly of the right foot (seven toes, see Fig.Fig. 1. Patient 1: cephalothoracopagus-conjoined twins.
176 de Jong and Kirby

3). He had hypospadias and a deeply cleft median ra-phe with the appearance of labia majora. No spinalanomalies were visible.
Radiographs showed midthoracic spondylocostaldysostosis. He had 10 ribs on the right and 9 on the left.Distal sacral agenesis was observed. Chromosomeanalysis of fibroblasts showed a normal male comple-ment.
Autopsy. Asymmetry of the cerebral hemisphereswas present, with the left side larger than the right,caused by asymmetric enlargement of the respectivecerebral ventricles and especially the occipital horn ofthe left ventricle, which was hugely dilated, causingdistortion of the posterior fossa. The sinuses were pat-ent and the falx was thin. The gyri were diffusely flat-tened. Leptomeninges were congested. The medialtemporal lobes abutted against the small midbrain.Central herniation was present. The pons was elon-gated, the medulla smaller than normal, while the cer-ebellar vermis was absent with fusion of the hemi-
spheres in the midline (rhombencephalosynapsis) andalso fusion of the dentate nuclei. The fourth ventriclewas reduced in size. The cord appeared unremarkable.In removing the spinal cord a midthoracic spondylocos-tal dysostosis was noted.
The heart weighed 16 g (expected weight 19.5 g). Thepericardium was normal, while the anterior myocardi-al surface appeared pale. A type II truncus arteriosuscommunis with a right aorta was present. The left sub-clavian artery arose from the descending aorta. Carotidarteries branched from a common trunk that arosefrom the aortic arch. An ASD and a high membranousVSD were present. Both lungs were congested and un-aerated, but the rest of the respiratory system ap-peared normal, as did the gastrointestinal system. Theliver was normal and also the spleen (weight 4.6 g as toexpected weight of 6 g).
Bilateral hydronephrosis secondary to pelvi-uretericjunction stenosis was present. The bladder was normal.Hypospadias was present and the testes were in theinguinal canal. Adrenals were congested. Thyroid andpancreas were normal; no thymus tissue could be iden-tified. The lymph nodes were normal.
Histologic study showed congestion of the myocar-dium, spleen, lymph nodes, lungs, and placenta. Am-niotic fluid aspiration was found in the lungs togetherwith intraseptal hemorrhages. The renal cortex wascongested with interstitial hemorrhages. There was hy-dronephrosis without renal cysts and diffuse nephro-
Fig. 2. Patient 2: before autopsy.
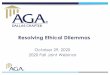
Fig. 3. Patient 2: radiograph of left foot showing pre-axial polydactylyand broad hallux.
Familial Blastogenesis Defects 177

blastema. Brain sections showed the fused dentatenucleus shaped around the fourth ventricle. The aque-duct was reduced in size.
Family 2
Patient 3. The 29-year-old Caucasian, healthymother presented at approximately 22 weeks of gesta-tion in her third pregnancy for ultrasound examinationdue to termination of her first pregnancy for hydro-cephalus, diagnosed ultrasonographically. Accordingto the mother, the female fetus had appeared normaland no further examinations were done in order to es-tablish the cause of the hydrocephalus. Her secondpregnancy resulted in a normal male from another re-lationship. The father of case 3 was healthy, noncon-sanguineous, Caucasian, with no family history of con-genital defects. There was no history of exposure toteratogens.
Ultrasonography demonstrated severe hydrocepha-
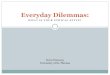
lus, a sacrococcygeal mass, probably a teratoma, andan abdominal cyst in a 22-week fetus. Parents electedtermination of pregnancy. The mother had a vaginaldelivery of a 660 g female fetus 3 days after prostaglan-din induction was commenced. The fetus had a bilat-eral cleft lip and palate, a flat midface and apparentlylow-set ears (Fig. 4). A multilocular cystic mass of 79 ×35 × 32 mm was present in the sacrococcygeal areawith solid areas. The distal cystic area displaced theanus anteriorly. The limbs were normal.
Radiographs showed midthoracic spondylocostaldyostosis with 10 pairs of ribs. Areas of calcificationwere present in the sacrococcygeal mass. Chromosomeanalysis of amniotic fluid showed a normal femalecomplement.
Autopsy confirmed the above clinical findings andshowed a small cerebellum, marked hydrocephalus,but no spinal cord abnormalities. The internal organswere normal, except for the thin-walled abdominal cyst62 mm in diameter, which had no connection to eitherthe sacrococcygeal mass nor the spinal column. Thegastrointestinal and urinary tracts were normal. Hy-drocolpos was present. The placenta, cord, and mem-branes were normal.
Microscopy showed the sacral mass to be an imma-ture teratoma. The cystic areas were lined with cuboi-dal, columnar, and mucinous cells, while more differ-entiated areas showed salivary glands, skin, andovarian tissue, the latter containing primordial fol-licles. Immature disorganized tissue formed the bulk ofthe mass with areas of degeneration and calcification.No abnormal mitosis was detected. The abdominal cystwas lined by transitional epithelium.
DISCUSSION
Conjoined twins are generally thought to representincomplete separation of identical twins. Midline de-fects are more common in monozygotic twins. Patient 1was therefore considered to be a defect of blastogenesisand, thus, was thought to be sporadic and have a lowrecurrence risk [Opitz, 1993; Martınez-Frıas, 1995].The multiple defects of patient 2 in the same family,not fitting a specific diagnosis and also representingdefects of blastogenesis, forced one to reconsider. Au-tosomal recessive inheritance would be a likely expla-nation. Autosomal recessive inheritance in 2 siblingswith different defects of blastogenesis, namely lateral-ization and midline defects, was described previouslyby Debrus et al. [1997], who postulated that a mutationof the connexin 43 gene could be responsible for these ofanomalies.
Absence of the thymus and the conotruncal defectssuggested DiGeorge syndrome, but the other findingswere not typical. Unfortunately, exclusion of the 22q11deletion by FISH was not feasible at the time andcurrently no tissue is available for further testing. Pa-tient 3 was interesting in that several anomalies pres-ent in patient 2 were observed, namely midthoracicspondylocostal dysostosis and hydrocephalus. Neitherof the two had an Arnold-Chiari type of malforma-tion, but both had cerebellar hypoplasia/dysplasia.The cleft lip and teratoma was reminiscent of patient
Fig. 4. Patient 3: lateral view showing abdominal distention due to theabdominal cyst and the position and relative size of the sacrococcygealteratoma.
178 de Jong and Kirby

1. Teratomas can originate from multipotential cells,but some are considered to be examples of incompletetwinning. Patient 3, with the teratoma containingovarian tissue with primordial follicles, could be clas-sified in the latter category. A defect of blastogenesis istherefore postulated to be the cause of the malforma-tions.
The mother of patient 3 had had a previous fetusby a different father with hydrocephalus. The ultra-sonographer had described the anomaly as enlargedlateral ventricles without any other observed defects.Several observers confirmed the absence of visible ad-ditional defects in this fetus. Although there aremany causes of hydrocephalus, two fetuses with thisabnormality born to the same healthy mother wouldbe unlikely to have a different cause. No consent couldbe obtained for radiological examination of the moth-er’s vertebral column or for a brain scan, in order toexclude possible autosomal dominant inheritance withvariable expression. Counseling is therefore more dif-ficult in patient 3 and neither a sporadic defect, anautosomal dominant single gene defect, gonadal mosa-icism, or even mitochondrial inheritance can be ex-cluded.
ACKNOWLEDGMENTSThe authors thank the ultrasound division of the De-
partment of Obstetrics and Gynecology for referral ofthe families and Prof. Kashula of the Department ofPathology, Red Cross Hospital, Cape Town, for autopsyof patient 3.
REFERENCESDebrus S, Sauer U, Gilgenkrantz S, Jost W, Jesberger H-J, Bouvagnet P.
1997. Autosomal recessive lateralization and midline defects: blasto-genesis recessive I. Am J Med Genet 68:401–404.
de Meeus A, Sarda P, Tenconi R, Ferriere M, Bouvagnet P. 1997. Blasto-genesis dominant I: a sequence with midline anomalies and heterotaxy.Am J Med Genet 68:405–408.
Martınez-Frıas M-L. 1995. Primary midline developmental field. I. Am JMed Genet 56:374–381.
Martınez-Frıas M-L, Frıas J. 1997. Are blastogenetic anomalies sporadic?Am J Med Genet 68:381–385.
Mathias RS, Lacro RV, Jones KL. 1987. X-linked laterality sequence: situsinversus, complex cardiac defects, splenic defects. Am J Med Genet28:111–116.
Mikkila SP, Janas M, Karikoski R, Tarkkila T, Simola KOJ. 1994. X-linkedlaterality sequence in a family with carrier manifestations. Am J MedGenet 49:435–438.
Opitz JM. 1993. Blastogenesis and the “primary field” in human develop-ment. In: Opitz JM, editor. Blastogenesis, normal and abnormal. NewYork: Wiley-Liss, BD:OAS XXIX (I):3–37.
Familial Blastogenesis Defects 179