Embed Size (px)
Citation preview
Defining End Stage CMP
Guillermo Torre-Amione MD, PhD
Defining what is End-Stage CMP
1. What is not end-stage
2. What is clearly end-stage
3. Dissecting the ambulatory high risk
1. What is not End stage

Heart Failure and Progression
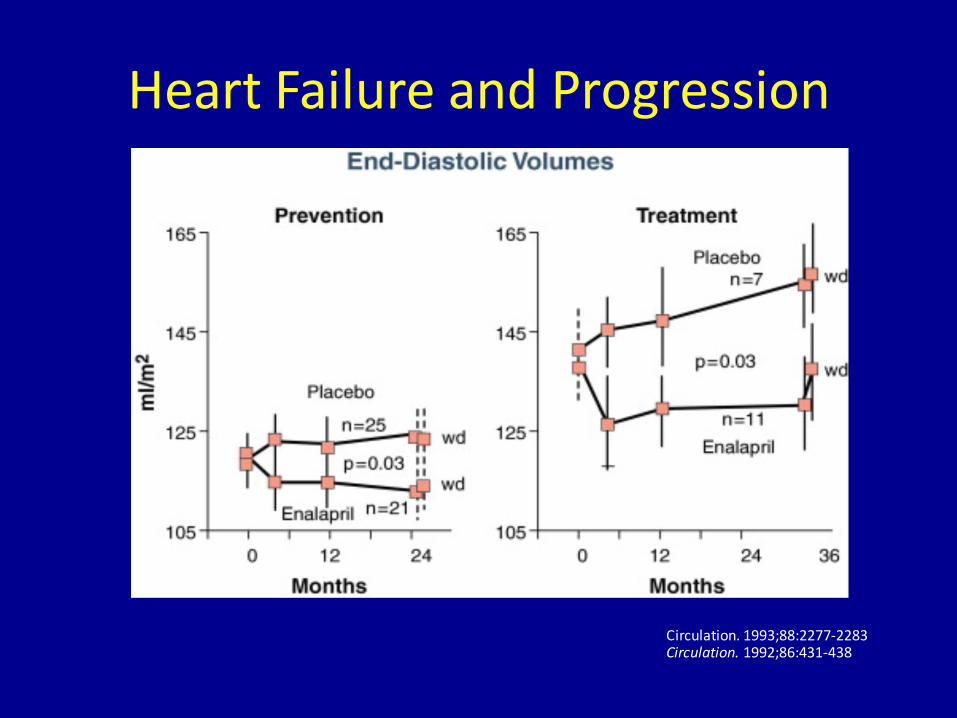
Heart Failure and Progression
Circulation. 1993;88:2277-2283Circulation. 1992;86:431-438
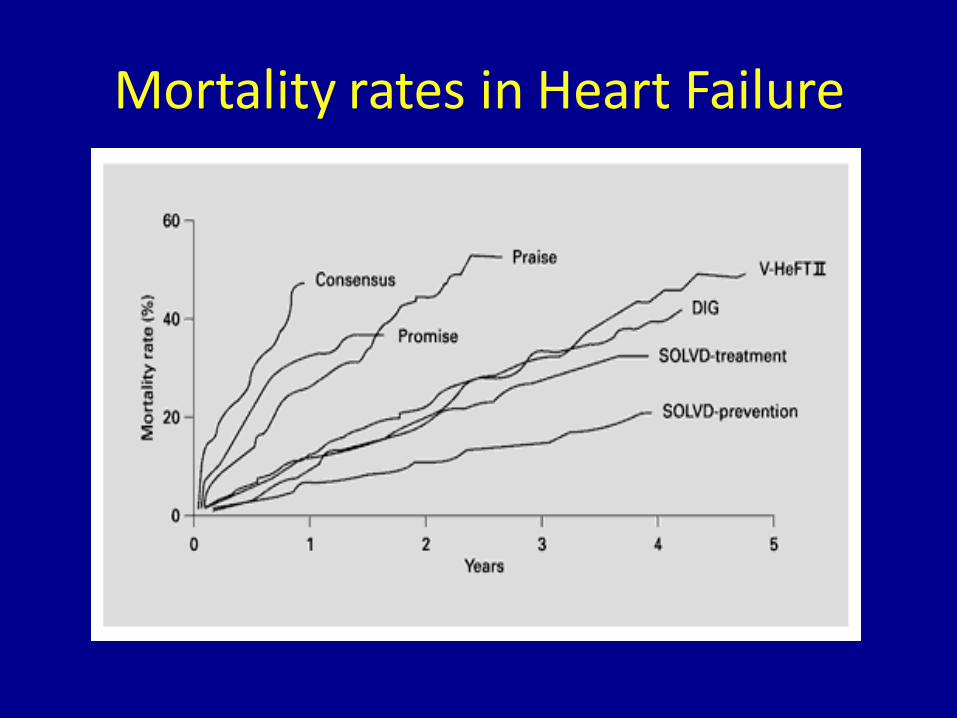
Mortality rates in Heart Failure
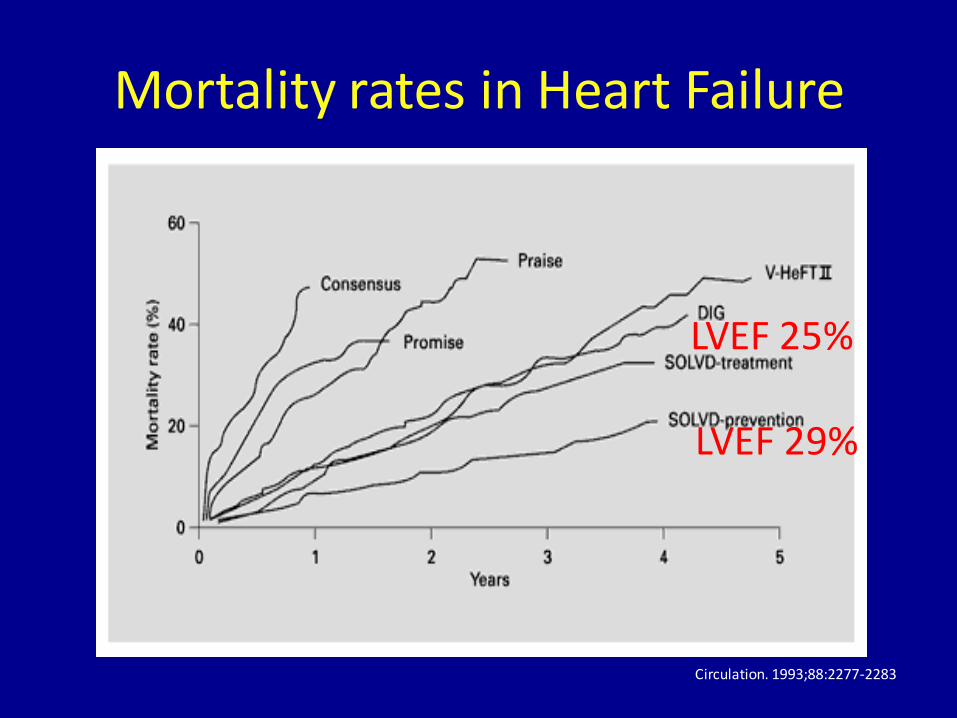
Mortality rates in Heart Failure
LVEF 25%
LVEF 29%
Circulation. 1993;88:2277-2283
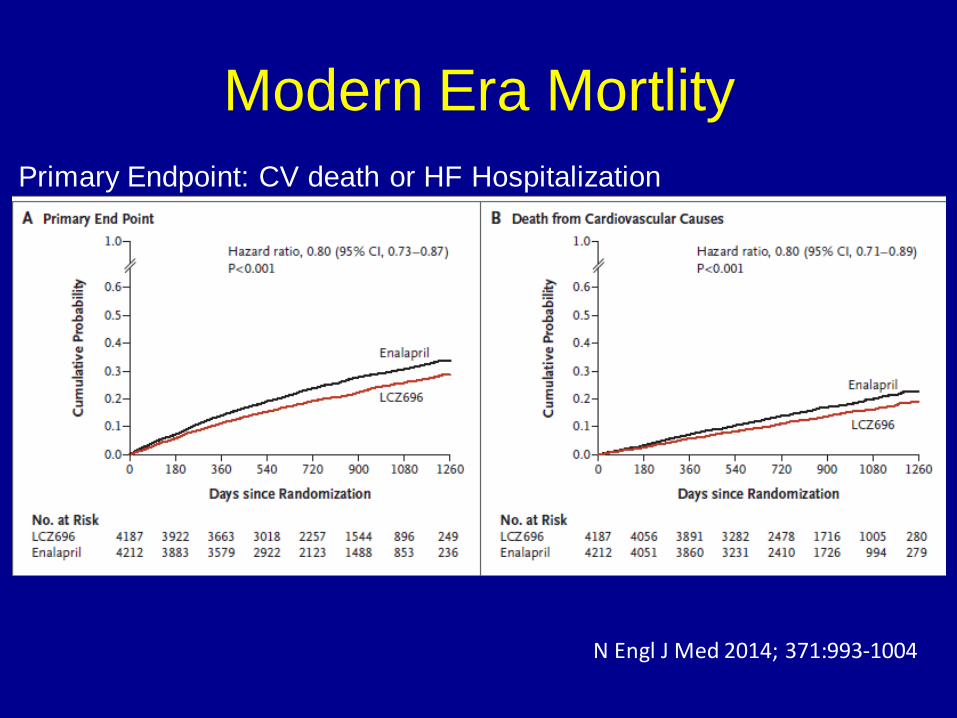
Modern Era Mortlity
Primary Endpoint: CV death or HF Hospitalization
N Engl J Med 2014; 371:993-1004
Mortality in asymptomatic untreated patients with LVD
20% at 4 years
SOLVD Prevention
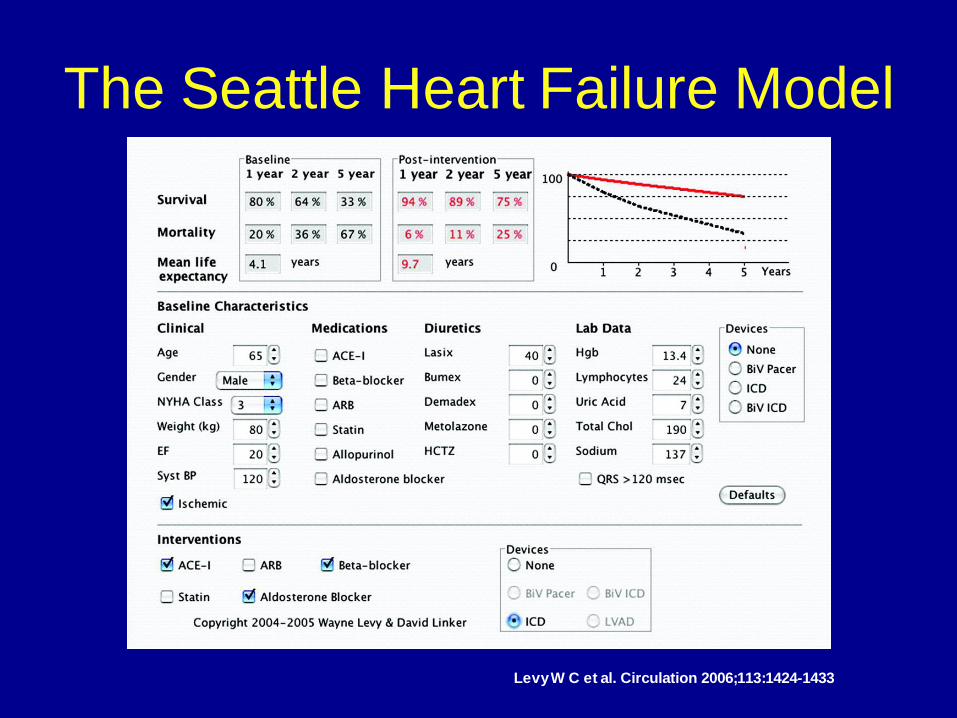
Levy W C et al. Circulation 2006;113:1424-1433
The Seattle Heart Failure Model
2. What is clearly end-stage
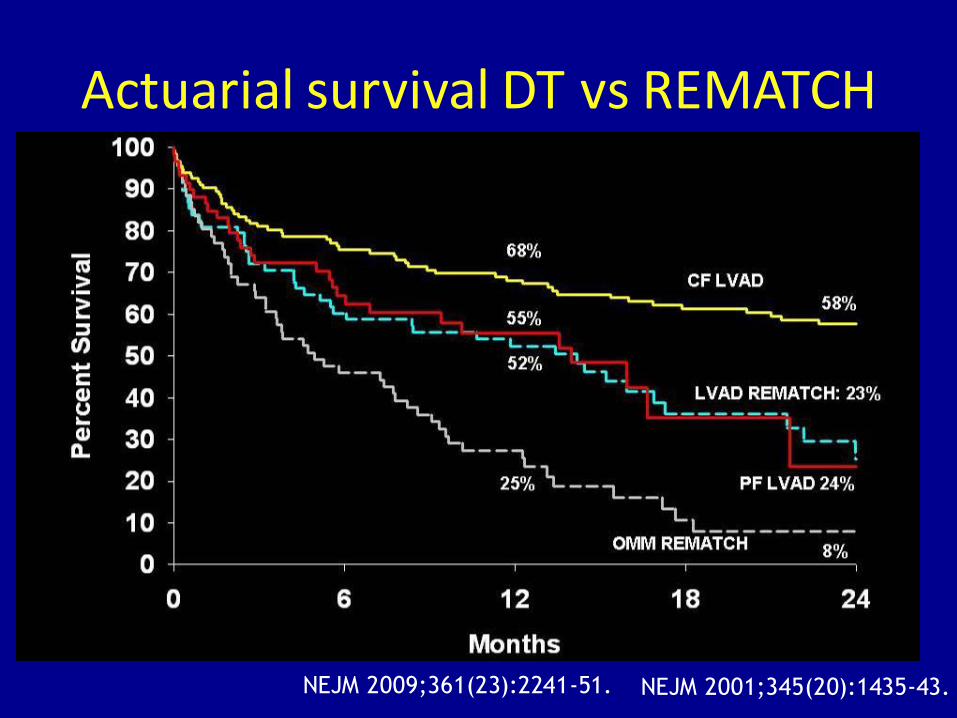
Actuarial survival DT vs REMATCH
NEJM 2009;361(23):2241-51. NEJM 2001;345(20):1435-43.
Inotrope dependent patient
VAD
3. Dissecting the high risk ambulatory patient
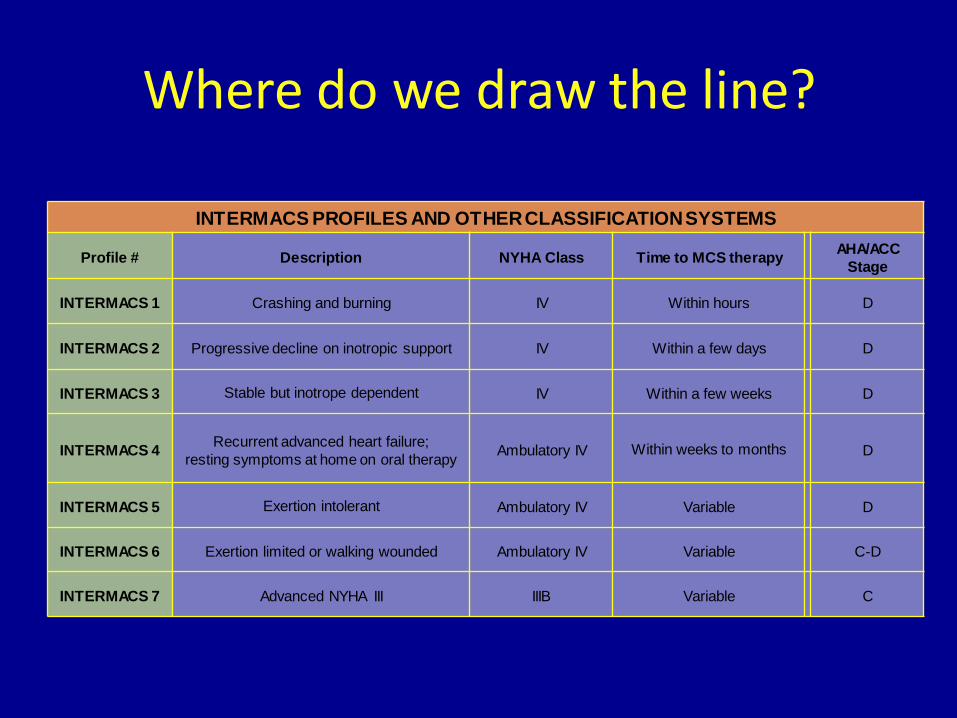
Where do we draw the line?
INTERMACS PROFILES AND OTHER CLASSIFICATION SYSTEMS
Profile # Description NYHA Class Time to MCS therapyAHA/ACC
Stage
INTERMACS 1 Crashing and burning IV Within hours D
INTERMACS 2 Progressive decline on inotropic support IV Within a few days D
INTERMACS 3 Stable but inotrope dependent IV Within a few weeks D
INTERMACS 4Recurrent advanced heart failure;
resting symptoms at home on oral therapyAmbulatory IV Within weeks to months D
INTERMACS 5 Exertion intolerant Ambulatory IV Variable D
INTERMACS 6 Exertion limited or walking wounded Ambulatory IV Variable C-D
INTERMACS 7 Advanced NYHA III IIIB Variable C
16
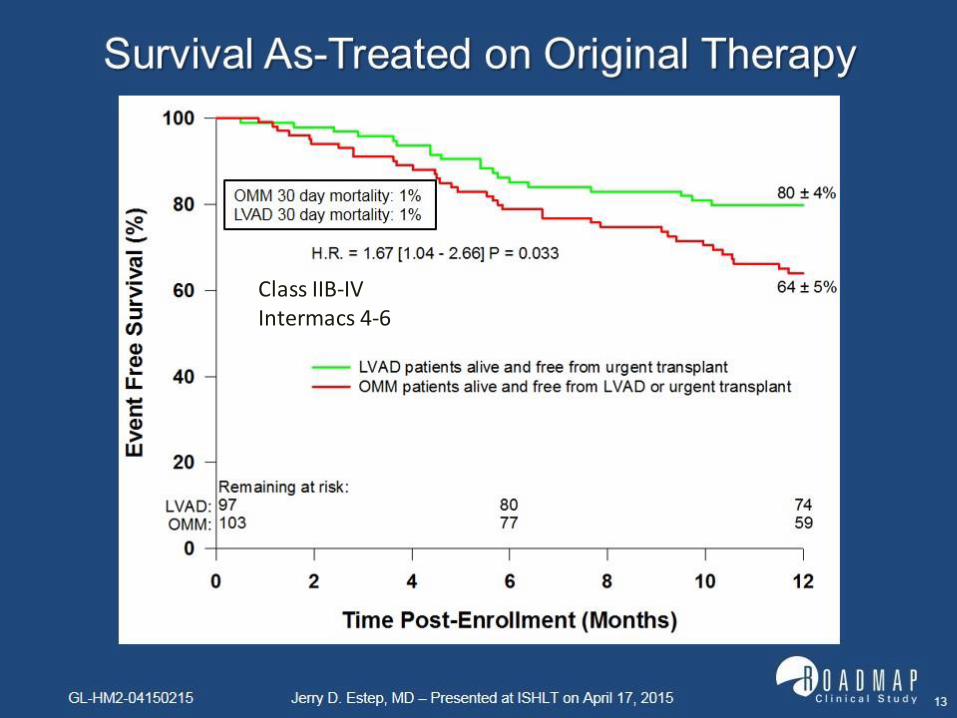
Class IIB-IVIntermacs 4-6
Biomarkers
• Cathecolamine levels
• Peristent BNP elevations
• Sodium
• Hemoglobin
• Uric Acid
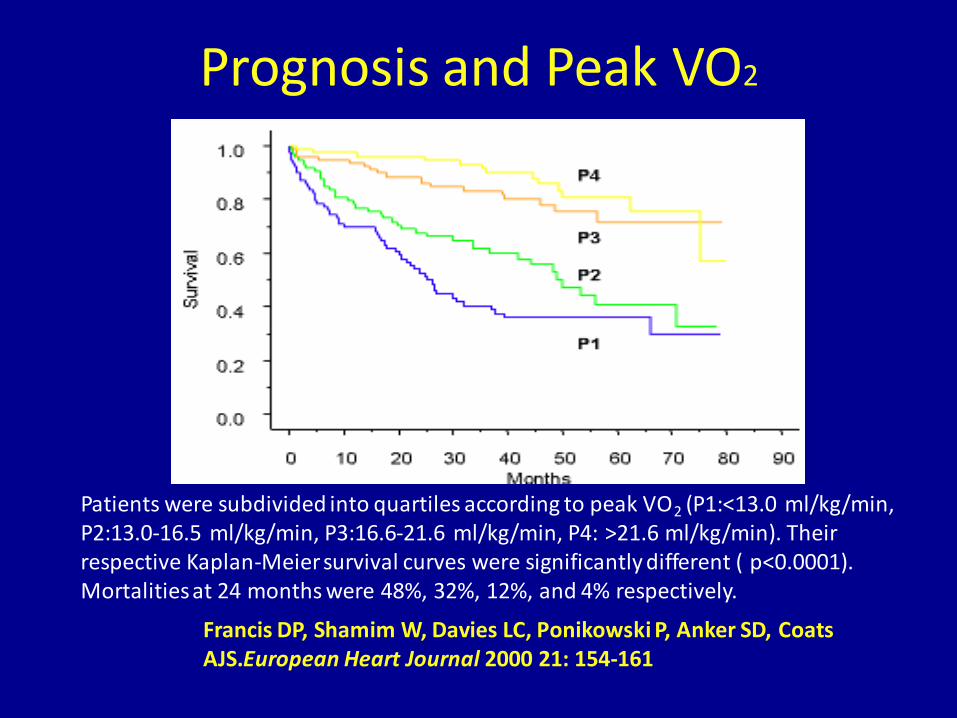
Prognosis and Peak VO2
Patients were subdivided into quartiles according to peak VO2 (P1:<13.0 ml/kg/min, P2:13.0-16.5 ml/kg/min, P3:16.6-21.6 ml/kg/min, P4: >21.6 ml/kg/min). Their respective Kaplan-Meier survival curves were significantly different ( p<0.0001). Mortalities at 24 months were 48%, 32%, 12%, and 4% respectively.
Francis DP, Shamim W, Davies LC, Ponikowski P, Anker SD, Coats AJS.European Heart Journal 2000 21: 154-161
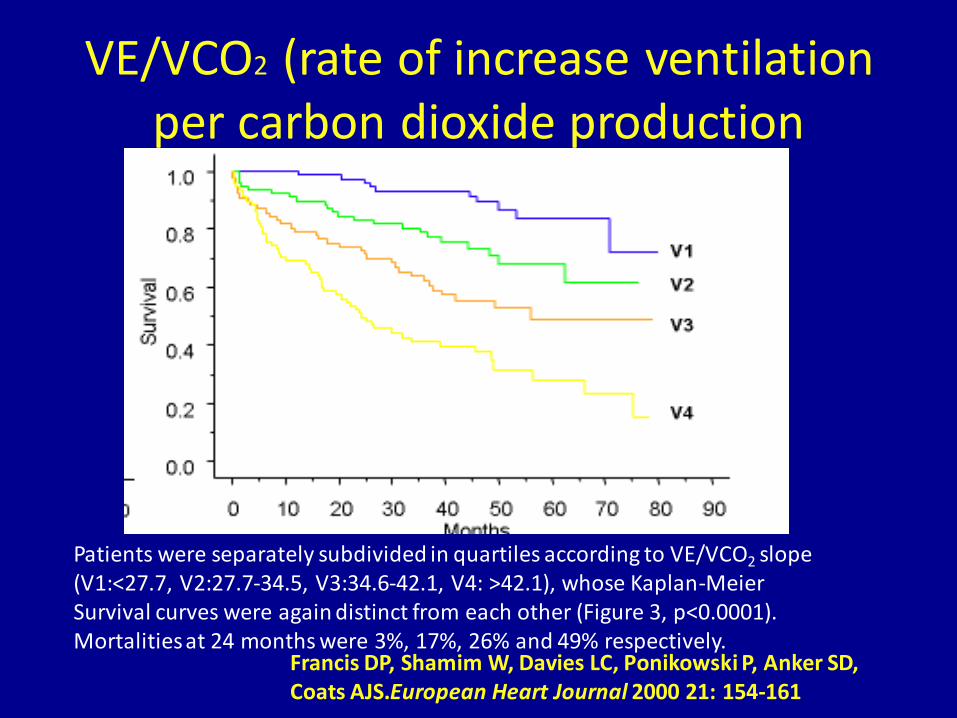
VE/VCO2 (rate of increase ventilation per carbon dioxide production
Patients were separately subdivided in quartiles according to VE/VCO2 slope (V1:<27.7, V2:27.7-34.5, V3:34.6-42.1, V4: >42.1), whose Kaplan-Meier Survival curves were again distinct from each other (Figure 3, p<0.0001). Mortalities at 24 months were 3%, 17%, 26% and 49% respectively.
Francis DP, Shamim W, Davies LC, Ponikowski P, Anker SD, Coats AJS.European Heart Journal 2000 21: 154-161
Evidence of end-organ damage
• Pulmonary Hypertension
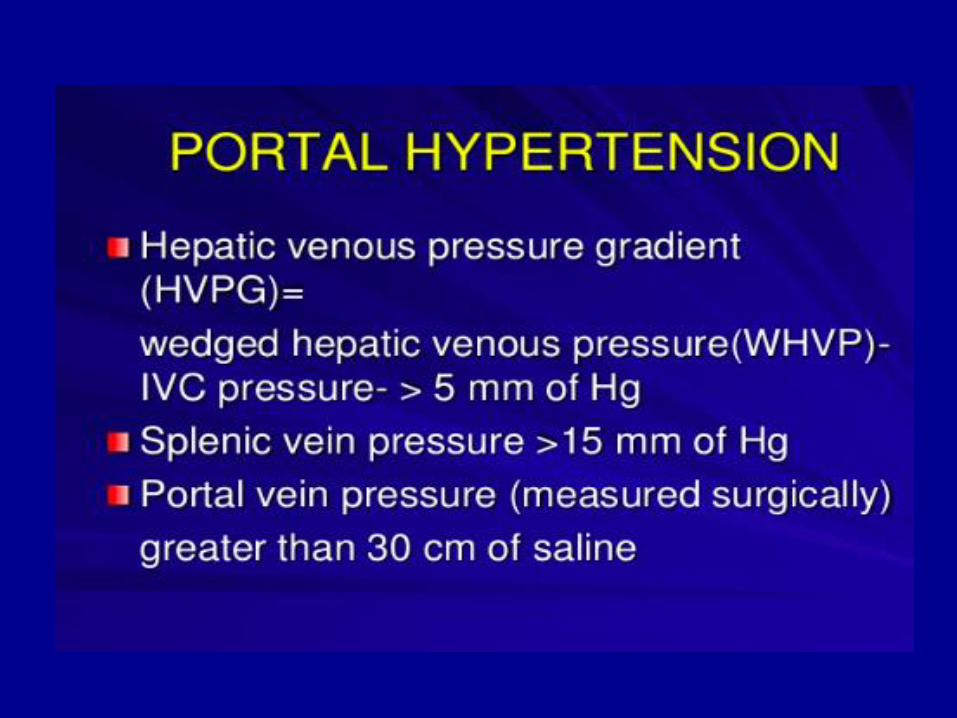
• Liver fibrosis/Cirrhosis
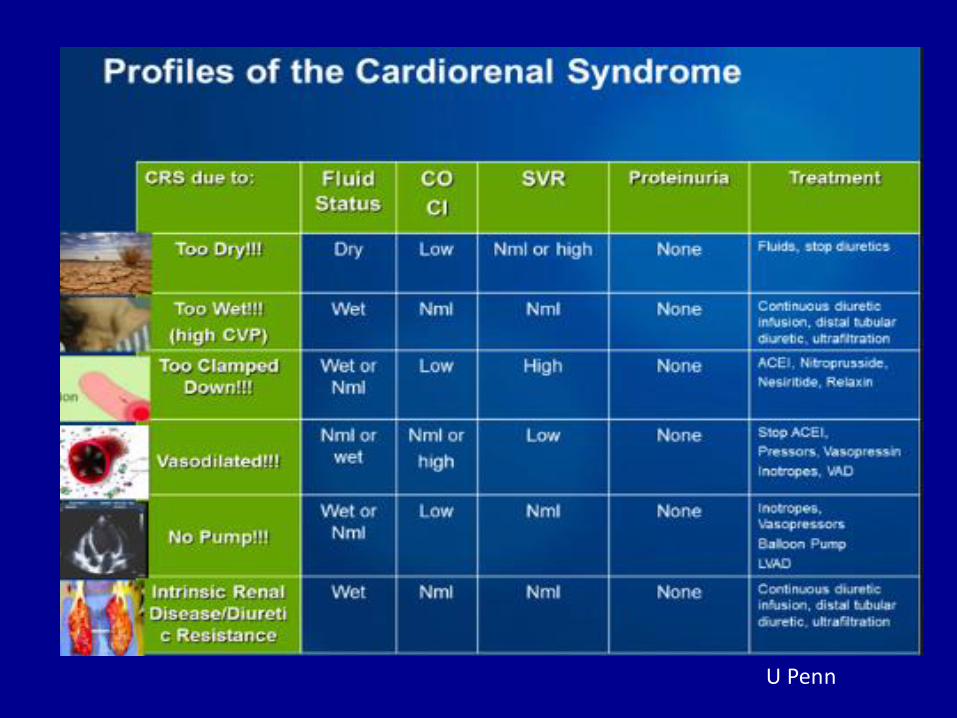
• Renal Failure
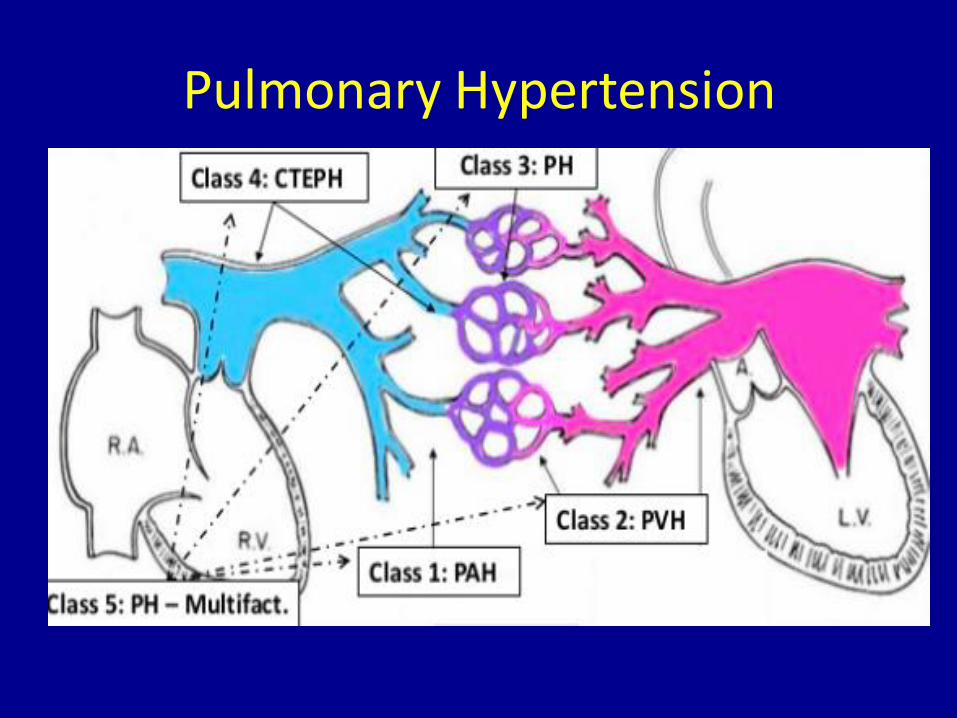
Pulmonary Hypertension
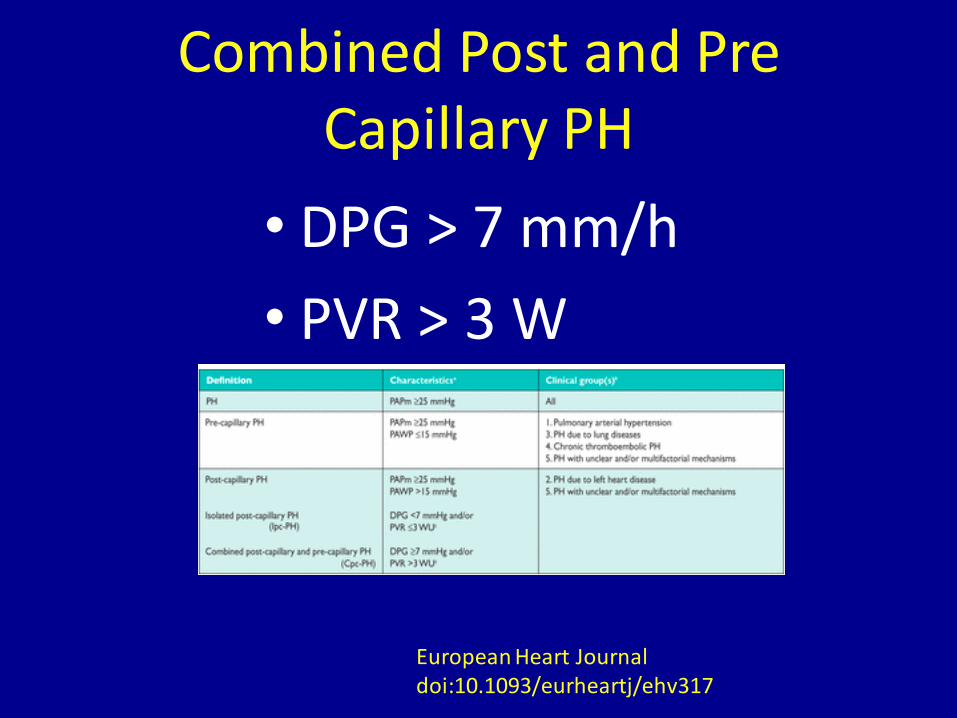
Combined Post and Pre Capillary PH
• DPG > 7 mm/h
• PVR > 3 W
European Heart Journal doi:10.1093/eurheartj/ehv317
“Fixed PAH”
• TPG >15 mmHg
• DPG (defined as diastolic PAP − mean PAWP) appears to best approach the characteristics required to determine pulmonary vascular disease. (ESC 2015 guidelines)
European Heart Journal doi:10.1093/eurheartj/ehv317
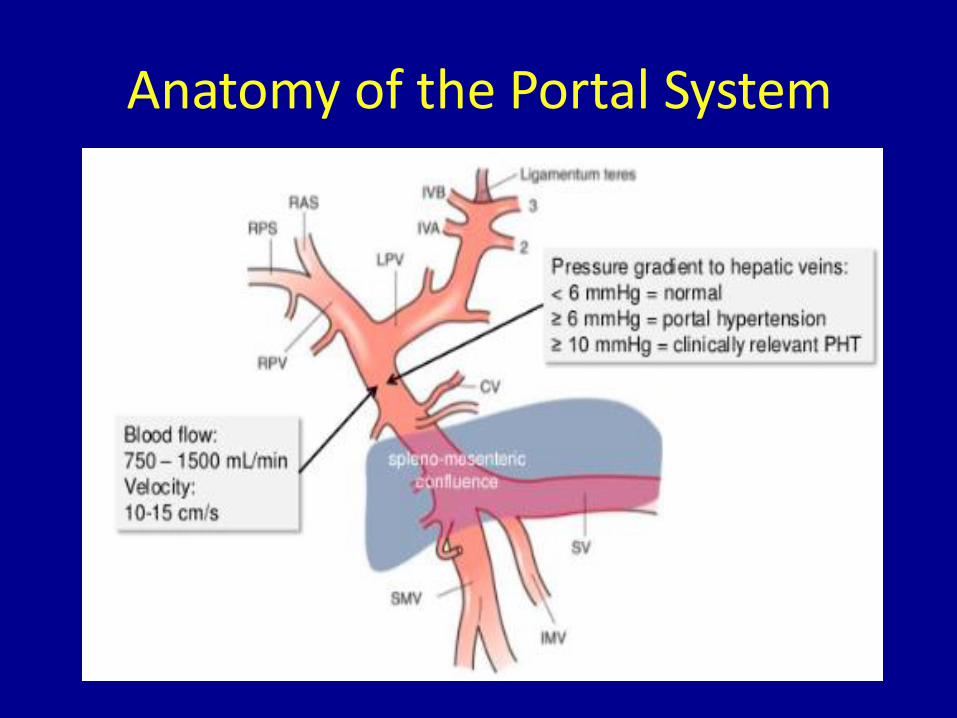
Anatomy of the Portal System
U Penn
Summary
• Ambulatory low EF: Long life
• Critically ill and needing Inotropes: Poor
• Ambulatory High risk: pulmonary hypertension, portal hypertension, renal dysfunction
• Ongoing registry studies will further define