Embed Size (px)
Citation preview

ARTICLE
Delayed Neurologic Sequelae Resulting from EpidemicDiethylene Glycol Poisoning
Sam Alfred, M.B.B.S., F.A.C.E.M.Division of Clinical Toxicology, Department of Emergency Medicine, Westmead Hospital,
Westmead, Australia
Patrick Coleman, M.B., M.R.C.P.I., F.R.C.A.P. and David Harris, M.B.B.S., F.R.A.C.P.Centre for Transplantation and Renal Research, Millenium Institute, Westmead, Australia
Tim Wigmore, B.A., M.A., B.M., B.Ch., F.R.C.A. andEdward Stachowski, M.B.B.S., F.A.N.Z.C.A., F.J.F.I.C.M.Department of Intensive Care Medicine, Westmead Hospital, Westmead, Australia
Andis Graudins, M.B.B.S., Ph.D., F.A.C.E.M. F.A.C.M.T.Clinical and Experimental Toxicology Unit, Department of Emergency Medicine,
Prince of Wales Hospital, Prince of Wales Clinical School, University of New South Wales,
Randwick, Australia
Background. Diethylene glycol (DEG) is a well-knownmetabolic and renal toxin usually ingested accidentally as anethanol substitute or as a contaminant in various medicinals. Todate, most poisonings have occurred in third-world countrieswhere early death from renal failure is very common. We reporta series of seven patients presenting with epidemic DEGpoisoning from a correctional facility with varying degrees ofmetabolic acidemia and acute renal impairment responding toemergent hemodialysis (HD). Significantly, three patients de-veloped delayed neurologic toxicity which has not been wellcharacterized in the past. Case Series. Seven male patients (agerange 19–55) presented over a 36 h period following ingestion ofvarying quantities of DEG. Initially three patients, ingesting thelargest quantities of DEG, presented more than 24 h postingestionwith severe metabolic acidemia (pH range 6.8–7.1) and anuricacute renal failure requiring HD. All three remained dialysis-dependent and developed significant cranial neuropathies withbulbar palsy in the second week postingestion. One patient diedwith cerebral oedema and a progressive encephalopathy. Twofurther patients presented within 24 h of ingestion with normalrenal function and a moderate metabolic acidemia (pH range7.2–7.28) requiring HD. They remained well. Finally, two furtherpatients presented with a history of trivial DEG ingestion and didnot require any therapy. Neurologic signs in the two survivinginitial presenters improved over 4–6 months although they
remained dialysis-dependent. Conclusion. Unrecognized DEGpoisoning may present with metabolic acidemia and anuric acuterenal failure. Established renal impairment may predict subse-quent delayed neurologic toxicity.
Keywords Diethylene glycol; Poisoning; Acute renal failure;
Bulbar palsy; Delayed toxicity
INTRODUCTION
Diethylene glycol (DEG) is an alcohol formed by the
condensation of two ethylene glycol molecules with an ether
bond. It was first isolated in 1869, and found its initial
commercial application as an industrial solvent in 1928. Since
then it has been increasingly employed as a cleaning and
softening agent in a variety of processes. Unfortunately, its
low cost of production has resulted in usage beyond the
industrial sphere. Despite documented toxicity in humans
(1–5), the pleasant smell and sweet taste of DEG have
resulted in its repeated use as an ethanol substitute and as a
vehicle for medical elixir preparations. Eight mass poisonings
involving DEG ingestion in humans have occurred within the
last 65 years with typical features of toxicity including
metabolic acidemia and acute renal failure (3,6–11).
Epidemic outbreaks of DEG poisoning have primarily
occurred in developing countries where the ability to diagnose
and adequately treat its toxicity is limited. Consequently, early
mortality and morbidity are high in cases of epidemic DEG
toxicity, with most deaths occurring within the first 2 weeks
Address correspondence to Dr. Sam Alfred, M.B.B.S., F.A.C.E.M.,Division of Clinical Toxicology, Department of Emergency Medicine,Westmead Hospital, Westmead, NSW, 2145, Australia; Fax: 61-2-9633-4296; E-mail: [email protected]
155
Clinical Toxicology, 43:155–159, 2005
Copyright D Taylor & Francis Inc.
ISSN: 0731-3810 print / 1097-9875 online
DOI: 10.1081/CLT-200057875
Order reprints of this article at www.copyright.rightslink.com
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
th C
arol
ina
Stat
e U
nive
rsity
on
11/0
7/13
For
pers
onal
use
onl
y.

post exposure secondary to acute renal failure (3,6–11). A
small number of cases of neurologic impairment have been
reported following exposure to DEG (6,11–13). We report a
series of seven patients from a correctional facility who
presented to our health service 24 h after the recreational
ingestion of DEG. Despite rapid recognition and treatment of
systemic acidemia and acute renal failure, delayed neurologic
complications were observed in the second week post-
ingestion. These included cranial and peripheral neuropathies,
mental status changes, and recurrent seizures.
CASE SERIES
Over a 28 h period a total of seven correctional services
inmates presented to our tertiary referral center and an
associated district hospital following exposure to a cleaning
fluid which had been diluted with water and ingested for
recreational purposes. Situational constraints made formal
identification of the cleaning agent impossible; however DEG
was identified as the toxicological agent by gas chromatog-
raphy and mass spectrometry (GCMS) performed on samples
acquired from the drinking container used. Subsequent clinical
and biochemical progress was consistent with DEG exposure.
The initial two male patients aged 19 [P1] and 25 [P2]
years and previously well, presented to the affiliated district
hospital 28 h postingestion. Both complained of nausea and
vomiting and on examination exhibited Kussmaul respiration
at 30 breaths/min. They were alert, hemodynamically stable,
and anuric. Subsequent biochemical analysis revealed severe
metabolic acidosis with elevated anion and osmolar gaps, as
well as acute renal failure as evidenced by elevation of the
serum creatinine (Table 1). In view of the history of potential
toxic alcohol ingestion, intravenous ethanol therapy com-
menced. Patient-1 was transferred to our institution for urgent
hemodialysis while patient-2 initially remained at the
peripheral hospital where continuous veno-venous hemodial-
ysis (CVVHD) commenced prior to transfer to another tertiary
institution for intermittent hemodialysis.
Two hours later a 52-yr-old male patient [P3], with a
history of chronic obstructive pulmonary disease and epilepsy,
presented to our institution with an identical history of solvent
ingestion 30 h earlier. On arrival, he was agitated and
confused with a Glasgow coma score of 12. He suffered a
prolonged generalized tonic-clonic seizure requiring sedation,
intubation, and ventilation. Biochemical analysis revealed a
similar severe metabolic acidosis with elevated anion and
osmolar gaps (Table 1). He was also anuric with elevated
serum creatinine (Table 1). Ethanol therapy was initiated and
hemodialysis commenced.
The following day another two previously healthy male
patients, aged 27 [P4] and 20 [P5] years, presented to our
institution 21 h postingestion of the same liquid. Both
complained of nausea. They were alert and hemodynamically
stable with Kussmaul respiration. Both demonstrated a
metabolic acidosis with elevated anion and osmolar gaps.
Serum creatinine was normal in both cases. Ethanol and
haemodialysis were commenced.
Finally, two further previously well male patients aged 21
[P6] and 26 [P7] years presented to our facility stating that
they had ingested the same cleaning fluid, although in a dilute
form and smaller volumes. They were asymptomatic and
systemically well with normal acid base balance and no
osmolar gap. Serum creatinine levels were also normal. They
were observed for 6 h and were subsequently transferred back
to prison after repeat biochemical markers remained normal.
Patient-1 remained dialysis-dependent and anuric, but was
otherwise well until day 10 postingestion when he abruptly
developed hearing and visual impairment. These progressed
over the ensuing 24 h to complete hearing loss and blindness
and were associated with the development of a bulbar palsy
and a rapidly declining level of consciousness that required
endotracheal intubation and ventilatory support. Cranial CT
scan revealed no abnormality. Cerebral MRI showed high-
intensity signals suggestive of foci of oedema or infarction
within the left parietal and occipital lobes, and both cerebellar
hemispheres. His neurological state did not improve, and on
day 19 postingestion he developed severe cerebral oedema and
died. A limited autopsy found no evidence of central de-
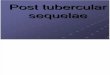
myelination. Renal biopsy showed diffuse cortical necrosis
consistent with DEG toxicity (see Fig. 1).
Patient-2 was managed at a separate tertiary institution as
our acute hemodialysis capabilities had been overwhelmed.
He was managed in a manner identical to our patients. Initially
he showed improvement symptomatically with stabilization of
his acid-base status, but remained dialysis dependent. Renal
biopsy demonstrated near total cortical necrosis. During the
second week of his admission he also developed a bulbar
palsy with associated lower limb weakness suggestive of a
peripheral neuropathy. EMG and nerve conduction studies
confirmed a sensory-motor neuropathy involving the lower
limbs, which did not progress. His neurological signs im-
proved over time but did not resolve completely, He remains
dialysis-dependent.
Patient-3 had a turbulent clinical course, requiring re-
intubation on two occasions due to uncontrolled seizures. He
developed aspiration pneumonia with respiratory failure
complicated by significant pleural and pericardial effusions.
Fourteen days postingestion he developed a bulbar palsy and
unilateral facial nerve paresis. These deficits improved over
time, leaving residual mild facial nerve palsy. He also remains
dialysis-dependent.
In summary, patients 1, 2, and 3 presented in established
renal failure and remained dialysis-dependent long term. They
all developed significant neurologic sequelae 2 to 3 weeks
postingestion. Patient 1 died of neurological sequelae on day
19. Patients 4 and 5 presented with normal renal function, did
S. ALFRED ET AL.156
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
th C
arol
ina
Stat
e U
nive
rsity
on
11/0
7/13
For
pers
onal
use
onl
y.

TA
BL
E1
Su
mm
ary
of
the
clin
ical
and
bio
chem
ical
fin
din
gs
no
ted
atp
rese
nta
tio
nfo
rfi
ve
pat
ien
tsw
ith
die
thy
len
eg
lyco
lp
ois
on
ing
*
Pat
ien
tP
1P
2P
3P
4P
5
Tim
efr
om
ing
esti
on
top
rese
nta
tio
n(h
r)2
82
83
02
12
1
Vo
lum
ein
ges
ted
‘‘5
cup
s’’
‘‘2
–3
gla
sses
’’N
ot
reco
rded
No
tre
cord
ed‘‘
50
0m
l’’
Tre
atm
ent
Eth
ano
lin
fusi
on
&H
D
Eth
ano
lin
fusi
on
&H
D
Eth
ano
lin
fusi
on
&H
D
Eth
ano
lin
fusi
on
&
HD
(6h
ou
rso
nly
)
Eth
ano
lin
fusi
on
&
HD
(6h
ou
rso
nly
)
Uri
ne
mic
rosc
op
yN
oca
lciu
mo
xal
ate
cry
stal
sse
en
An
uri
cN
oca
lciu
mo
xal
ate
cry
stal
sse
en
No
calc
ium
ox
alat
e
cry
stal
sse
en
No
calc
ium
ox
alat
e
cry
stal
sse
en
pH
6.9
95
7.0
76
.78
97
.28
87
.20
2
PC
O2
11
.51
41
2.4
31
.72
4.9
PO
2(S
atu
rati
on
s%
)1
27
.4(9
9.1
)1
65
(99
)1
33
(97
.2)
11
0(9
8.3
)1
71
(99
.7)
Ba
seex
cess
�2
6.4
�2
4�
29
.5�
10
.6�
17
.1
HC
O3
2.7
4N
/A1
6.4
12
.1
An
ion
ga
p(m
mo
l/L
)3
7.1
38
.13
71
8.2
24
.5
Ser
um
osm
ola
lity
33
33
30
33
82
95
30
6
Osm
ola
rg
ap
(mm
ol/
kg
)4
6.9
19
.65
0.8
7.6
25
.5
Ser
um
crea
tin
ine
mg
/dl
(mm
ol/
L)
3.6
3(3
21
)2
.89
(25
6)
2.4
7(2
18
)1
.13
(10
0)
1.1
2(9
9)
Co
rrec
ted
seru
mca
lciu
mm
g/d
l(m
mo
l/L
)0
.66
(2.6
4)
0.5
2(2
.07
)0
.61
(2.4
5)
0.5
3(2
.12
)0
.58
(2.3
3)
Neu
rolo
gic
al
seq
uel
ae
.B
ulb
arP
alsy
.C
NII
.C
NV
III
.B
ulb
arP
alsy
.P
erip
her
aln
euro
pat
hy
.B
ulb
arP
alsy
.C
NV
II
No
No
Ou
tco
me
at
26
mo
nth
sD
ied
Day
19
.D
ialy
sis
dep
end
ent
.P
ersi
stin
gn
euro
log
ic
def
icit
.D
ialy
sis
dep
end
ent
.P
ersi
stin
gn
euro
log
ic
def
icit
Fu
llre
cov
ery
Fu
llre
cov
ery
HD
hem
od
ialy
sis.
*N
ote
:P
atie
nt
6an
d7
no
tin
clu
ded
asb
ioch
emic
ally
no
rmal
atp
rese
nta
tio
nan
dd
idn
ot
dev
elo
pcl
inic
alse
qu
elae
.
157
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
th C
arol
ina
Stat
e U
nive
rsity
on
11/0
7/13
For
pers
onal
use
onl
y.

not develop ongoing renal impairment, and were discharged
back to their correctional services facility where ongoing
medical review did not detect any evidence of evolving
neurological abnormalities over the ensuing weeks. Similarly,
patients 6 and 7 remained symptom free.
DISCUSSION
Diethylene glycol is a solvent with widespread industrial
usage; therefore its identification by GCMS within the
ingested fluid was consistent with the reported mode of
acquisition. Coupled with the lack of access to alternative
toxins within the prison system, a negative GCMS screen for
other toxins in the ingested fluid, and normal serological
parameters for alternative causes of elevated osmolar gaps
(glucose, lactate, ethanol, ethylene glycol, etc.) this presented
a strong case for DEG as a single agent exposure.
As evidenced in this case series DEG confers a significant
potential for the development of metabolic and renal toxicity if
ingested. Previous reports of epidemic DEG toxicity have
commonly occurred in third-world countries where access to
intensive care facilities and extracorporeal renal supportive
therapy is often nonexistent. Consequently patients com-
monly die rapidly as a result of metabolic acidemia and anuric
acute renal failure (3–11). There have been few long-term
survivors. However, delayed neurologic sequelae have been
observed in a small number of acute phase survivors with
ongoing renal impairment (12,13). We report significant and
delayed neurologic toxicity in three patients with established
renal failure at presentation following the ingestion of DEG
for recreational purposes.
Toxicological experience with DEG extends back to 1937
and the ‘‘Massengil Tragedy’’ in which 105 deaths resulted
following the release of a sulphanilamide elixir suspended in
DEG. Since then there have been mass casualties in South
Africa (1969), Spain (1985), India (1986 and 1998), Nigeria
(1990), Bangladesh (1990–1992), and Haiti (1996), with well
in excess of 500 documented deaths and many more un-
recorded. These epidemics can be attributed to the substitution
of DEG for more expensive, nontoxic glycols in medicinal
preparations. Typically acetaminophen elixirs have been
involved, explaining the preponderance of pediatric deaths.
Neurotoxicity following DEG poisoning was first reported
in South Africa, where three of seven DEG exposed children
with anuric acute renal failure developed optic neuritis (6).
Cerebrospinal fluid (CSF) from these three cases demonstrated
elevated protein levels which were thought to be indicative of
a demyelinating process (6). All seven children died despite
supportive therapy, which included peritoneal dialysis.
Autopsies demonstrated renal and hepatic changes consistent
with DEG poisoning without detectable CNS pathology (6).
Neurologic abnormalities were also reported in a number of
cases of pediatric DEG poisoning observed during the 1996
Haitian acetaminophen contamination episode. Facial nerve
paresis was seen in the acute acidemic phase of poisoning
(11). Unfortunately all children exhibiting this sign died of
renal failure, along with the vast majority of those exposed. Of
note, a 7-yr-old girl transferred to the United States for treat-
ment of established renal failure with hemodialysis devel-
oped optic neuritis, sixth cranial nerve and bulbar palsies on
day 10 postexposure (12), a delay similar to that observed in
our case series. Cerebrospinal fluid protein levels in this child
were found to be elevated, although myelin basic protein was
negative. An MRI demonstrated cerebral atrophy without evi-
dence of edema or demyelination. She was treated with high-
dose steroids and improved over time but was left with some
persisting neurologic abnormalities.
Rollins et al. reported similar delayed neurologic deterio-
ration in a 55-yr-old man who ingested DEG in a suicide
attempt (13). Diagnosis of and treatment for his DEG exposure
were delayed for several days. By the time hemodialysis was
initiated the patient was in established renal failure. On day 5
he developed bilateral lower limb weakness, which progressed
over the course of the next 5 days to hyporeflexive quad-
raparesis and was associated with progressive mental obtun-
dation and coma requiring endotracheal intubation and
ventilation. CSF protein levels were elevated with a positive
myelin basic protein, and electromyography/nerve conduction
studies confirmed a severe neuropathy with demyelinating
features. MRI scanning again failed to demonstrate evidence
of demyelination. He died 18 days postingestion. Autopsy
revealed patchy meningeal and perivascular lymphocytic
infiltrates around the brainstem and occasional chromatolytic
motor neurons within the spinal cord. The cerebral white
matter did not show any evidence of demyelination. Periph-
eral nervous system changes included widespread severe
myelin loss in all the sampled sections. Similarly, dorsal and
ventral nerve roots immediately adjacent to the cord at all
FIG. 1. Renal biopsy showing DEG induced diffuse cortical necrosis.
S. ALFRED ET AL.158
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
th C
arol
ina
Stat
e U
nive
rsity
on
11/0
7/13
For
pers
onal
use
onl
y.

spinal levels demonstrated similar myelin losses, as did cranial
nerves 6, 7, and 8 (13).
The mechanism of DEG neurotoxicity has not been fully
elucidated. Initially, it was theorized that production of oxalic
acid and calcium oxalate was involved in the neurotoxicity
seen with DEG poisoning. Early studies of DEG metabolism
suggested that it was first metabolized to ethylene glycol and
subsequently oxalic acid (15–17). This was subsequently dis-
proved by examining the metabolism of radiolabelled DEG,
demonstrating that ethylene glycol and ethylene glycol–re-
lated byproducts are not produced during DEG metabolism
(18–22). The main metabolite of DEG has been identified as
2-hydroxyethoxyacetic acid (HEAA) (22). The metabolism of
DEG to HEAA in rats has been prevented by inhibition of both
alcohol and aldehyde dehydrogenases (22). Consequently,
HEAA and other yet-to-be identified metabolites of DEG may
be the mediators of DEG toxicity in humans. Transcellular
fluid shifts, membrane destabilization through phospholipid or
ion channel effects, metabolic acid-base derangements, and
osmotic metabolite accumulation within cells all present as
possible mechanisms for this cellular toxicity.
From a clinical perspective, DEG toxicity is capable of
producing both acute phase neurologic impairment, with optic
neuritis, facial nerve palsies and cerebral edema (6,9,11), and
a delayed neurotoxicity in the form of optic neuritis, central
and peripheral neuropathies that may be demyelinating in
nature (12–14). As evidenced in this case series and the
previous cases of DEG poisoning with delayed neurological
features, the presence of metabolic acidemia with established
renal failure on presentation to hospital may be predictive of
subsequent delayed neurologic toxicity. None of the patients
with normal renal function in our case series developed any
neurological signs on subsequent evaluation.
Diethylene glycol poisoning has the potential to produce
significant morbidity and mortality, particularly in patients
who have delayed presentations. As with all toxic alcohol
exposures, the aim of therapy is to recognize the poisoning
early in its course and to prevent the development of acidemia
and renal failure. Specific therapies to block alcohol de-
hydrogenase conversion of DEG to its toxic metabolites, such
as intravenous ethanol infusion or fomepizole, should be
employed (23,24). Hemodialysis should be instituted as soon
as possible to remove DEG, its metabolites, and to treat any
metabolic acidemia that is present. Clinicians must be aware
that patients presenting with or developing renal failure fol-
lowing DEG poisoning may go on to exhibit significant
central and peripheral neurologic complications several days
to weeks following the exposure. Currently, there are no spe-
cific therapies available to treat DEG-induced neurotoxicity.
The natural course of this condition is unpredictable. Patients
may have resolution of some or all of their neurologic signs
over a matter of weeks or months, or die with fulminant cen-
tral nervous system failure.
REFERENCES
1. Von Oettingen WF, Jirouch EA. Pharmacology of ethylene glycol and
some of its derivatives. J Pharmacol Exp Ther 1931; 42:355.
2. Haag HB, Ambrose AM. Studies of the physiological effects of
diethylene glycol. J Pharmacol Exp Ther 1937; 59:93.
3. Leech PN. Elixir of sulphanilamide-massengill. JAMA 1937;
109(19):1531– 1539.
4. Calvery HO, Klumpp TG. The toxicity for human beings of diethyl-
ene glycol with sulphanilamide. South Med J 1939; 32(11):1105–
1109.
5. Lynch KM. Diethylene glycol poisoning in the human. South Med J
1938; 31(2):134–137.
6. Bowie MD. Diethlyene glycol poisoning in children. South Afr Med J
1972; 46:931– 934.
7. Cantarell MC, Fort J, Camps J, Sans M, Piera L. Acute intoxication due
to topical application of diethylene glycol (letter). Ann Intern Med 1987;
106(3):478 – 479.
8. Pandya SK. An unmitigated tragedy (letter). BMJ 1988; 297:117 –
119.
9. Okuonghae HO, Ighogboja IS, Lawson JO, Nwana JC. Diethylene gly-
col poisoning in Nigerian children. Ann Trop Paediatr 1992; 12:235–
238.
10. Hanif M, Mobarak MR, Ronan A, Rahman D, Donovan JJ, Bennish ML.
Fatal renal failure caused by diethlyene glycol in paracetamol elixir: the
bangladeshi epidemic. BMJ 1995; 311:88–91.
11. Junod SW. Diethylene glycol deaths in Haiti. Public Health Rep 2000;
115:78– 86.
12. Scalzo AJ. Diethylene glycol toxicity revisited: the 1996 Haitian
epidemic. Clin Toxicol 1996; 34(5):513–516.
13. Rollins YD, Filley CM, McNutt JT, Chahal S, Kleinschmidt-DeMasters
BK. Fulminant ascending paralysis as a delayed sequelae of diethlylene
glycol (sterno) ingestion. Neurology 2002; 59:1460–1463.
14. Drut R, Quijano G, Jones MC, Scanferla P. Hallazgos patologicos en la
intoxicacion por dietilenglicol. Medicina 1994; 54:1–5.
15. Durand A, Auzepy P, Herbet JL, Trien TC. A study of mortality and
urinary excretion of oxalate in male rats following acute experimental
intoxication with diethlyene glycol. Eur J Int Care Med 1976; 2:143–
146.
16. Herbet JL, Fabre M, Auzepy P, Paillas J, Durand A. Acute experimental
poisoning by diethylene glycol: acid base balance and histological data
in male rats. Toxicol Eur Res 1978; 1:289– 294.
17. Morris HJ, Nelson AA, Calvery AO. Observations on the chronic
toxicities of propylene glycol, ethylene glycol, diethlylene glycol,
ethylene glycol mono-ethly-ether, and diethlylene glycol mono-ethyl-
ether. J Pharmacol Exp Ther 1942; 74:266–273.
18. Brown CLM. Constitution and toxicities of the glycols. Pharm J 1938;
140:48.
19. Wiley FH, Hueper WC, Bergen DS, Blood FR. The formation of oxalic
acid from ethlylene glycol and related solvents. J Ind Hyg Toxicol 1938;
20:269– 277.
20. Balaz T, Jackson B, Hite M. Nephrotoxicities of ethlylene glycols,
cephalosporins and diuretics. Monogr Appl Toxicol 1982; 1:487– 497.
21. Wiener HL. Ethlylene and Diethlyene Glycol Metabolism, Toxicity and
Treatment. PhD dissertation. Columbu, OH: The Ohio State University,
1986.
22. Wiener HL, Richardson KE. Metabolism of diethlylene glycol in male
rats. Biochem Pharmacol 1989; 38(3):539–541.
23. Borron SW, Garnier MD. Intravenous 4-methylpyrazole as an antidote
for diethlylene glycol and triethylene glycol poisoning: a case report. Vet
Hum Toxicol 1997; 39(1):26– 28.
24. Vassiliadis J, Graudins A, Dowsett RP. Triethlylene glycol poisoning
treated with intravenous ethanol infusion. J Toxicol Clin Toxicol 1999;
37(6):773–776.
159DIETHYLENE GLYCOL POISONING AND DELAYED NEUROTOXICITY
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
th C
arol
ina
Stat
e U
nive
rsity
on
11/0
7/13
For
pers
onal
use
onl
y.