Embed Size (px)
Citation preview
Demonstration of Varicellazoster Virus Antigens in the Vitreous Aspirates of Patients with Acute Retinal Necrosis Syndrome SUMI SOUSHI, MD,l HIROKO OZAWA, MD,2 MASAKAZU MATSUHASHI, MD,2
JUN SHIMAZAKI, MD,2 UTAKO SAGA, MD,2 TAKESHI KURATA, MD, PhD3
Abstract: Four cases of acute retinal necrosis (ARN) syndrome were studied virologically. Varicella-zoster virus (VZV) antigen was demonstrated by immunofluorescence in cells from vitreous aspirates of two cases. No herpes simplex virus (HSV) or cytomegalovirus (CMV) antigens were detected by the same technique. Antibody to VZV in vitreous fluid was present in two cases; however, it was not detected in sera. Although virus isolation was unsuccessful, these findings strongly suggest that VZV may play an important role in the etiology of ARN syndrome. [Key words: acute retinal necrosis syndrome, acyclovir, immunofluorescence, necrotizing retinitis, varicella-zoster virus, vitreous aspirate.] Ophthalmology 95: 1394-1398, 1988
Acute retinal necrosis (ARN) syndrome, which has been known as "Kirisawa-type uveitis"l in Japan, is a form of uveitis of unknown etiology. The disease begins with severe unilateral or bilateral obstructive retinal arteritis and retinal necrosis in the periphery, resulting in serious rhegmatogenous retinal detachment (RD). As a rule, no signs of systemic involvement are present. 2-5
Recently, an etiologic role for herpes-group viruses has been strongly suggested based on virologic studies of
Originally received: January 25, 1988. Revision accepted: June 27, 1988.
1 Department of Ophthalmology, Tokai University School of Medicine, Tokyo.
2 Department of Ophthalmology, Keio University School of Medicine, Tokyo. 3 Department of Pathology, National Institute of Health, Tokyo.
Presented at the Twenty-fifth Intemational Congress of Ophthalmology.
Reprint requests to Sumi Soushi, MD, Department of Ophthalmology, Tokai University School of Medicine, Tokyo Hospital, 1-2-5 Yoyogi Shibuya-ku Tokyo, 151 Japan.
1394
aqueous and vitreous fluid and retina of ARN syndrome patients.6- 9
In the current study, we attempt to detect viral antigens of herpes-group viruses by immunofluorescence, to ascertain the presence of herpesvirus antibody, and to isolate virus using the vitreous aspirates of four patients with typical ARN syndrome.
CASE REPORTS
Case 1. In a 42-year-old man, decreased vision developed in his right eye at the beginning of September 1984. On September 10, he visited an ophthalmologist and was treated with oral and topical steroids for suspected panuveitis. Because of rapid decrease in visual acuity in the right eye, he was admitted to Keio University Hospital on September 18. He did not have flu-like signs during this episode, On admission, his visual acuity was 20/200 in the right eye and 20/20 in the left. The right eye showed granulomatous keratic precipitates, 3+ cells and 3+ flare in the anterior chamber, and marked cellular infiltration and opacity in the vitreous. Results of funduscopic examination
SOUSHI et al • VZV ANTIGENS IN ARN SYNDROME
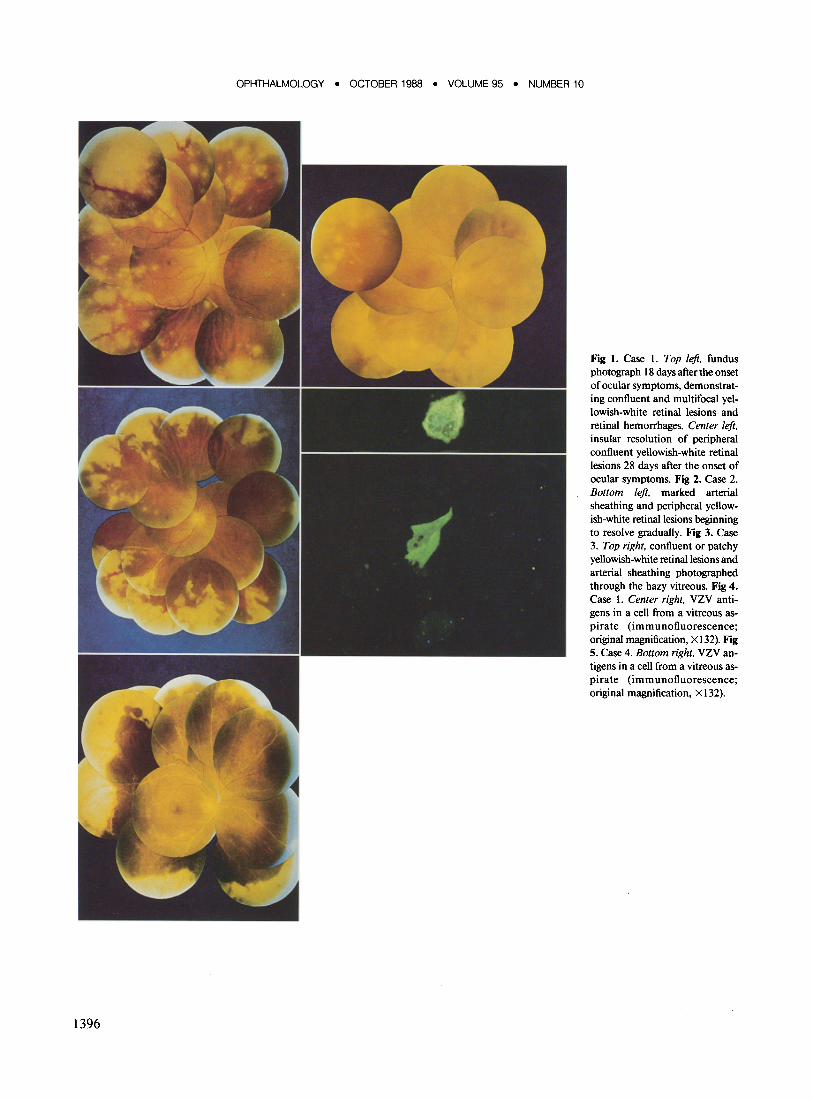
showed patchy and confluent yellowish-white lesions with hemorrhages all around the peripheral retina, partly advancing to the vascular arcade. There was marked arterial narrowing and sheathing, and scattered hemorrhages along with the vessels (Fig 1, top left). His left eye was normal. Thus, the diagnosis of ARN syndrome was made. His significant past history included a mild diabetes mellitus 4 years before admission which had been controlled well by diet therapy.
Laboratory studies showed that leukocyte count, differential, sedimentation rate, and coagulation time were all normal. Blood chemistries, serum immunoglobulin levels, and chest x-ray were normal. Numbers ofB and T lymphocytes were normal. Results of purified protein derivative test were negative. Antibody titers to herpes simplex virus (HSV), varicella-zoster virus (VZV), and cytomegalovirus (CMV) determined by the complement fixation test were less than 1:4 in the serum and less than 1: 1 in the cerebrospinal fluid, respectively.
Acyclovir (250 mg/every 8 hours) was given to the patient intravenously for 10 days beginning September 19. One week later, the yellowish-white retinal lesions began to regress gradually (Fig 1, center left). On September 28, photocoagulation was done at posterior sites adjacent to the same lesions. Because of increasing vitreous haze, a simple vitrectomy was performed on October 5 to prevent tractional RD. At the same time, the vitreous fluid was aspirated and examined for the presence of virus antigens and specific virus antibodies. Virus isolation was also attempted from the same fluid. As posterior vitreous detachment occurred with tight traction to vitreous base and superior area offundus, another vitrectomy was done on October 25. On November 30, the patient was discharged with visual acuity of 20/ 60. Three days after discharge, rhegmatogenous RD developed, which was successfully reattached by a scleral encircling procedure, cryotherapy, subretinal fluid drainage, and air tamponade. Three months later, however, rhegmatogenous RD recurred and reattachment was unsuccessful.
Summaries of cases 2 and 3 are described in Tables 1 and 2 with the funduscopic illustrations (Figs 2, 3).
Case 4. In a healthy 65-year-old man, a painless decrease in vision and redness in his left eye developed during a flu-like illness in February 1986. He was found by his referring ophthalmologist to have visual acuity of20/600 in his left eye on March 25. He had marked granulomatous keratic precipitates, 3+ cells and 3+ flare. Despite the heavy vitreous opacity, arterial sheathing and extensive confluent yellowish-white lesions in the periphery were noted. He was treated with oral beta-methazone (3 mg daily). His visual acuity improved gradually toward the end of April. One month later, however, rhegmatogenous RD developed suddenly and the patient was admitted to Keio University Hospital on June 5, 1986. His visual acuity was 20/20 in his right eye and hand motions in the left eye. Ocular tension was 12 mmHg in the right eye and 2 mmHg in the left. There were eight tears leading to total RD in the equator zone of the retina. The next day, the number of tears increased to about 20, probably due to retinal thinning. The right eye was normal. Hematologic studies showed a leukocyte count of 14,700 ~l with a normal differential and normal coagulation time. Blood chemistries were all normal. Results of purified protein derivative test were positive, 25 X 20 mm. Serum complement fixation antibody titers to HSV, VZV, and CMV were less than 1:4, 1: 4, and 1: 16, respectively. Cryopexy, vitrectomy, and subretinal fluid drainage was done, but a scleral encircling procedure could not be attempted because of high ocular tension due to choroidal and vitreous bleeding. The retina did not reattach. To prevent involvement of the right eye, the patient was treated expectantly with acyclovir (750 mg daily) intravenously for 7 days. On July
2, he was discharged without light perception in his left eye, and normal vision in his right eye.
VIROLOGIC STUDIES
IMMUNOFLUORESCENCE
Vitreous aspirates from all patients were examined by immunofluorescence for the presence of viral antigens. Direct or indirect immunofluorescence methods were used respectively in case I or cases 2, 3, and 4. The vitreous aspirates which were collected at vitrectomy were centrifuged, the precipitates were coated on spot slides, and they were fixed with acetone for 10 minutes at room temperature. The IgG-fraction from the convalescent serum of a zoster patient, without antibody to other herpes-group viruses, was conjugated with fluorescein isothiocyanate for use in direct immunofluorescence.
For indirect staining of VZV antigens, specific monoclonal antibodies lO to glycoprotein and nucleoprotein were applied. After washing, anti-mouse IgG conjugated with fluorescein isothiocyanate (MILES-YEDA, LTD, Israel) was added. For HSV studies, anti-HSV-I or -2 mouse monoclonal antibodies conjugated with fluorescein isothiocyanate (MicroTrak Herpes, DaiSyva Co Ltd, Japan) were used. CMV antigen was identified by fluorescein isothiocyanate-conjugated anti-CMV convalescent human IgG.
These antibodies were applied to the spot slides and incubated for I hour at 37°C. After washing in phosphatebuffered saline for 15 minutes, the specimens were observed under the fluorescence microscope.
ANTIBODY TITERS
Antibody titers to HSV, VZV, and CMV of the vitreous aspirates without dilution were determined by complement fixation.
VIRUS ISOLATION
The vitreous aspirates were co-cultured with human embryonic lung fibroblasts, and were observed during 4 weeks for cytopathic effects.
RESULTS
IMMUNOFLUORESCENCE
Varicella-zoster virus antigens were detected in cells from the vitreous aspirates of cases I and 4 by immunofluorescence (Figs 4, 5), but not in cases 2 and 3. The cells exhibiting positive immunofluorescence were larger (approximately 20 X 25 J.Lm) than lymphocytes or plasma cells, and appeared to have microscopic characteristics of a retinal cell. No HSV-l and -2 or CMV antigens were demonstrated in any case.
1395
OPHTHALMOLOGY • OCTOBER 1988 • VOLUME 95 • NUMBER 10
1396
Fig 1. Case 1. Top left, fundus photograph 18 days after the onset of ocular symptoms, demonstrating confluent and multifocal yellowish-white retinal lesions and retinal hemorrhages. Center left, insular resolution of peripheral confluent yellowish-white retinal lesions 28 days after the onset of ocular symptoms. Fig 2. Case 2. Bottom left, marked arterial sheathing and peripheral yellowish-white retinal lesions beginning to resolve gradually. Fig 3. Case 3. Top right, confluent or patchy yellowish-white retinal lesions and arterial sheathing photographed through the hazy vitreous. Fig 4. Case I. Center right, VZV antigens in a cell from a vitreous aspirate (immunofluorescence; original magnification, X 132). Fig S. Case 4. Bottom right, VZVantigens in a cell from a vitreous aspirate (immunofluorescence; original magnification, X 132).
SOUSHI et al • VZV ANTIGENS IN ARN SYNDROME
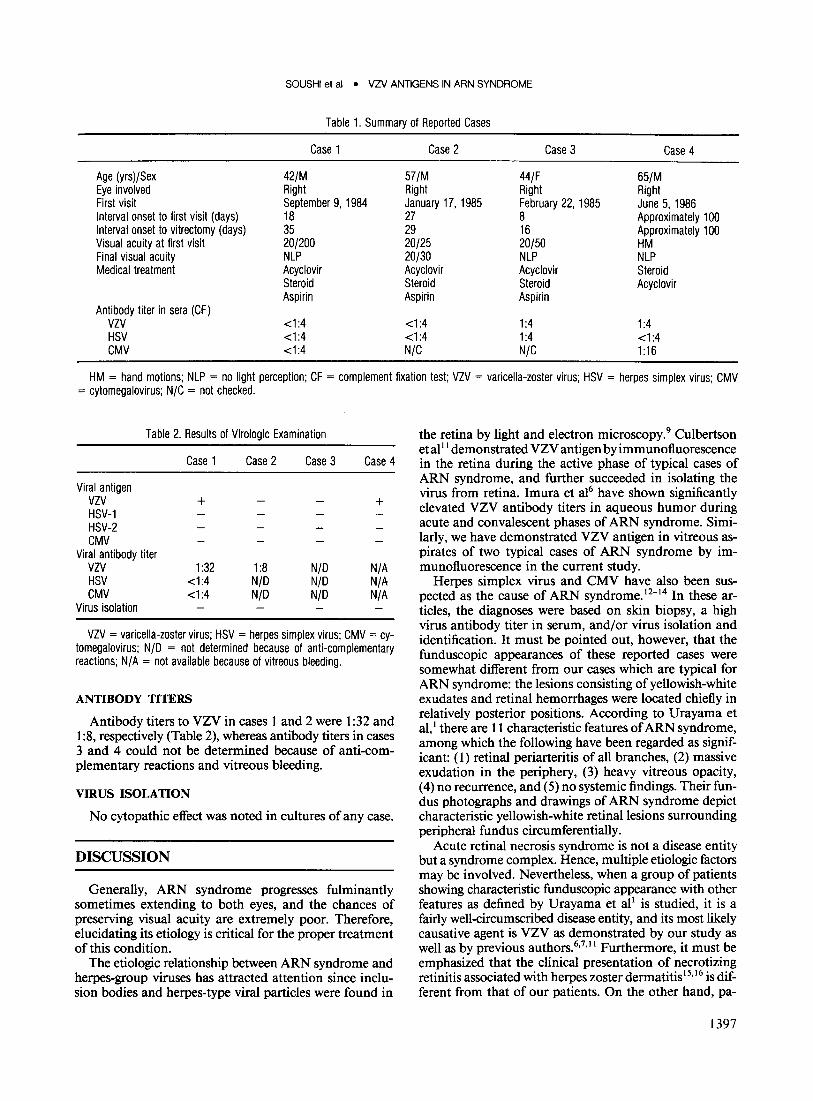
Table 1. Summary of Reported Cases
Case 1 Case 2 Case 3 Case 4
Age (yrsl/Sex 42/M 57/M 44/F 65/M Eye involved Right Right Right Right First visit September 9, 1984 January 17, 1985 February 22, 1985 June 5, 1986 Interval onset to first visit (days) 18 27 8 Approximately 100 Interval onset to vitrectomy (days) 35 29 16 Approximately 100 Visual acuity at first visit 20/200 20/25 20/50 HM Final visual acuity NLP 20/30 NLP NLP Medical treatment Acyclovir Acyclovir Acyclovir Steroid
Steroid Steroid Steroid Acyclovir Aspirin Aspirin Aspirin
Antibody titer in sera (CF) VZV <1:4 <1:4 1:4 1:4 HSV <1:4 <1:4 1:4 <1:4 CMV <1:4 N/C N/C 1:16
HM = hand motions; NLP = no light perception; CF = complement fixation test; VZV = varicella-loster virus; HSV = herpes simplex virus; CMV = cytomegalovirus; N/C = not checked.
Table 2. Results of Virologic Examination
Case 1 Case 2 Case 3 Case 4
Viral antigen VZV + + HSV-1 HSV-2 CMV
Viral antibody titer VZV 1:32 1:8 N/D N/A HSV <1:4 N/D N/D N/A CMV <1:4 N/D N/D N/A
Virus isolation
VZV = varicella-loster virus; HSV = herpes simplex virus; CMV = cytomegalovirus; N/D = not determined because of anti-complementary reactions; N/ A = not available because of vitreous bleeding.
ANTIBODY TITERS
Antibody titers to VZV in cases 1 and 2 were 1 :32 and 1 :8, respectively (Table 2), whereas antibody titers in cases 3 and 4 could not be determined because of anti-complementary reactions and vitreous bleeding.
VIRUS ISOLATION
No cytopathic effect was noted in cultures of any case.
DISCUSSION
Generally, ARN syndrome progresses fulminantly sometimes extending to both eyes, and the chances of preserving visual acuity are extremely poor. Therefore, elucidating its etiology is critical for the proper treatment ofthis condition.
The etiologic relationship between ARN syndrome and herpes-group viruses has attracted attention since inclusion bodies and herpes-type viral particles were found in
the retina by light and electron microscopy.9 Culbertson et alII demonstrated VZV antigen by immunofluorescence in the retina during the active phase of typical cases of ARN syndrome, and further succeeded in isolating the virus from retina. Imura et al6 have shown significantly elevated VZV antibody titers in aqueous humor during acute and convalescent phases of ARN syndrome. Similarly, we have demonstrated VZV antigen in vitreous aspirates of two typical cases of ARN syndrome by immunofluorescence in the current study.
Herpes simplex virus and CMV have also been suspected as the cause of ARN syndrome. 12
-14 In these ar
ticles, the diagnoses were based on skin biopsy, a high virus antibody titer in serum, and/or virus isolation and identification. It must be pointed out, however, that the funduscopic appearances of these reported cases were somewhat different from our cases which are typical for ARN syndrome: the lesions consisting of yellowish-white exudates and retinal hemorrhages were located chiefly in relatively posterior positions. According to Urayama et al, I there are 11 characteristic features of ARN syndrome, among which the following have been regarded as significant: (1) retinal periarteritis of all branches, (2) massive exudation in the periphery, (3) heavy vitreous opacity, (4) no recurrence, and (5) no systemic findings. Their fundus photographs and drawings of ARN syndrome depict characteristic yellowish-white retinal lesions surrounding peripheral fundus circumferentially.
Acute retinal necrosis syndrome is not a disease entity but a syndrome complex. Hence, multiple etiologic factors may be involved. Nevertheless, when a group of patients showing characteristic funduscopic appearance with other features as defined by Urayama et all is studied, it is a fairly well-circumscribed disease entity, and its most likely causative agent is VZV as demonstrated by our study as well as by previous authors.6,7,11 Furthermore, it must be emphasized that the clinical presentation of necrotizing retinitis associated with herpes zoster dermatitis I 5,16 is different from that of our patients. On the other hand, pa-
1397

OPHTHALMOLOGY • OCTOBER 1988 • VOLUME 95 • NUMBER 10
tients with ARN syndrome in which HSV or CMV has been shown to be responsible have exhibited somewhat different clinical presentation and funduscopic findings including various systemic disorders. 12-14
It has generally been accepted that the diagnosis of viral diseases should be determined by at least one of the following laboratory tests: (1) significant elevation of viral antibody titers in paired samples, (2). demonstration of viral antigen in infected cells by immunohistochemistry, or (3) virus isolation and identification from infected organs. Since identification of viral antigen in vitreous fluid by immunofluorescence requires only 1 or 2 hours, this procedure is recommended for the rapid diagnosis of uveitis of unknown etiology. On the other hand, several days to weeks may be needed to isolate some viruses in cell culture. Furthermore, virus isolation may be difficult when anti-herpesvirus therapy has already been initiated. To maximize favorable prognosis for the patients, treatment with anti-herpesvirus drugs should begin at an early phase of the disease, because the etiologic agent is very likely to be VZV. Anti-herpesvirus drug therapy may also be beneficial to patients with a later stage of the disease in order to prevent infection in the other eye. Intravitreal infusion of anti-herpesvirus drug may be even more effective for ARN syndrome. I?
REFERENCES
1. Urayama A, Yamada N, Sasaki T, et al. Unilateral acute uveitis with retinal periarteritis and detachment. Jpn J Clin Ophthalmol 1971; 25: 607-19.
2. Willerson 0 Jr, Aaberg TM, Reeser FH. Necrotizing vaso-occlusive retinitis. Am J OphthalmoI1977; 84:209-19.
3. Young NJA, Bird AC. Bilateral acute retinal necrosis. Br J Ophthalmol 1978; 62:581-90.
1398
4. Bando K, Kinoshita A, Mimura Y. Six cases of so-called "Kirisawa Type" uveitis. Jpn J Clin Ophthalmol1979; 33:1515-21.
5. Okinami S, Tsukahara I. Acute severe uveitis with retinal vasculitis and retinal detachment. Ophthalmologica 1979; 179:276-85.
6. Imura N, Imura R, Oku H, et al. Rise of antibody titer for varicellazoster virus in the aqueous and vitreous in 2 cases with Kirisawa uveitis. Jpn J Clin Ophthalmol1985; 39:101-6.
7. Usui M, Hasemi M, Onishi Y, et al. Electron microscopic study and biochemical analysis on the vitreous of uveitis: two cases of Kirisawa's uveitis. Jpn J Clin Ophthalmol1984; 38:381-7.
8. Nakayama T, Matsuo N, Koyama T, et al. Clinical investigation of acute retinal necrosis. 3. Ultrastructure of biopsy specimens and possibility of herpes virus infection. Folia Ophthalmol Jpn 1984; 35: 1 029-36.
9. Culbertson WW, Blumenkranz MS, Haines H, et al. The acute retinal necrosis syndrome. Part 2: Histopathology and etiology. Ophthalmology 1982; 89:1317-25.
10. Okuno T, Yamanishi K, Shiraki K, Takahashi M. Synthesis and processing of glycoproteins of varicella-zoster virus (VlV) as studied with monoclonal antibodies to VlV antigens. Virology 1983; 129:357-68.
11. Culbertson WW, Blumenkranz MS, Pepose JS, et al. Varicella zoster virus is a cause of acute retinal necrosis syndrome. Ophthalmology 1986; 93:559-69.
12. Ludwig IH, legarra H, lakov IN. The acute retinal necrosis syndrome: possible herpes simplex retinitis. Ophthalmology 1984; 91:1659-64.
13. Matsuzono T, Hirayama Y, Takano J. A case of Kirisawa's uveitis associated with neovascular glaucoma and elevation of serum HSV-1 antibody. Folia Ophthalmol Jpn 1984; 35:2585-8.
14. Rungger-Brandle E, Roux L, Leuenberger PM. Bilateral acute retinal necrosis (BARN): identification of the presumed infectious agent. Ophthalmology 1984; 91: 1648-58.
15. Schwartz IN, Cashwell F, Hawkins HK, Klintworth GK. Necrotizing retinopathy with herpes zoster ophthalmicus: a light and electron microscopical study. Arch Pathol Lab Med 1976; 100:386-91.
16. Tsukimoto N, Kohzuka T, Yamaguchi H. Necrotizing retinitis caused by opportunistic virus infection in a non-Hodgkin lymphoma: a case report. Folia Ophthalmol Jpn 1983; 34:561-6.
17. Peyman GA, Goldberg MF, Uninsky E, et al. Vitrectomy and intravitreal antiviral drug therapy in acute retinal necrosis syndrome: report of two cases. Arch OphthalmoI1984; 102:1618-21.