Embed Size (px)
Citation preview

1
Demystifying CompressionCompression
Terry Treadwell, MD, FACSMedical DirectorInstitute for Advanced Wound CareMontgomery, Alabama
Compression Questions1. Are all compression bandages the same?2. Can compression therapy be used in the patient with edema
and an ABI < 0.8? 3. Can compression therapy be used in the patient with edema
and cellulitis? 4. Does compression therapy improve the skin of patients with
venous dermatitis? 5. Can compression therapy be used in the patient with edema
and congestive heart failure? 6. Can compression therapy be used in the patient with edema
and acute deep venous thrombophlebitis?7. Do patients care which compression bandage is used?
Looking for the Evidence??
Demystifying Compression

2
Are all compression bandages the same?bandages the same?
Compression Therapy• Short stretch or inelastic • Elastic• Single layer• Multiple layers• High pressure • Low pressure
D
Anterior
L
Compartments
Anterior Tibial
Greater Saphenous
Tibia
SuperficialPosterior
DeepPosterior
Lateral
Lesser Saphenous
Dr. HN Mayrovitz
Fibula
Skin
Posterior Tibial
Peroneal
Demystifying Compression

3
Pressures of Interest
Tibialis m.
Popliteus m
Pe
• Sub‐bandage• Surface• Contact
Tibia
Soleus m
Gastroc m.
Popliteus m.Tibialis m.
eroneus
•Tissue•Interstitial
Fibula
• Intramuscular
CompressionBandage or Device
Skin
Dr. HN Mayrovitz
Resting Pressure
R
Pressure (P) Due to Tension (T) of
LaPlace’sLaw
Superficial vessels affected the most
Tension (T) of Bandage and the Radius (R) of the Leg
Dr. HN Mayrovitz
P ~P ~ T T RR
Muscles Contract Bandage
Restricts Muscle
Contraction
Working (Dynamic) Pressure
High Pressure
Develops on Deeper Tissues
Pressure Is From WITHINDr. HN Mayrovitz
Demystifying Compression

4
Dynamic Pressure Depends onBandage Material Features
Form-fitted Steel Pipe(Cast)
res
su
re
Mayrovitz HN, et al. Clin Physiol. 1997;17(1):105‐117.
Bandage “Stretchability”
No External Compression
0
Inelastic(short stretch)
Elastic(long stretch)D
yna
mic
P
Working vs. Resting PressuresRole of Compression Material
Emptying
ure
(PT) Emptying
TimeDr. HN Mayrovitz
Tis
sue
Pres
s
Time
Pascal’s Law
Equal Distribution of
PPressure Throughout the
Leg with Muscle
Contraction
Demystifying Compression

5
Short Stretch Vs. Multi-stretch• Short stretch systems are effective at a lower resting
pressure than multi-stretch systems
• A lower resting pressure offers safer compression in the compromised limb
• Both systems can produce effective, dynamic working and resting pressures.
Can compression therapy be used in the
ti t ith d patient with edema and an ABI < 0.8?
Venous Ulcers and PVD1416 leg ulcers with venous reflux
14%2%
ABPI >1
0,85‐0,5
Humphreys ML et al. Br J Surg. 2007 Sep;94(9):1104‐7
84%
<0,5
Demystifying Compression

6
Venous Ulcer Healing
Marston W et al, J VascSurg 1999; 30:491
Control Leg
BeforeBandage
ml/min
Arterial Flow Pulses Below Knee Blood Flow via Nuclear Magnetic Resonance
Treated Leg
WithBandage
ml/min
Dr. HN Mayrovitz, Univ of Miami
Compression Therapy and Circulation
ABI Bandage Sub-bandage pressure (mm Hg)
> 0.8 4-layer 35-40
0.7 2-layer 17-25
0.6 2-layer 17-25
<0.5 Only with medical supervision
---
Moffatt C. www.worldwidewounds.com (12/5/09)
Demystifying Compression

7
Compression and Arterial Insufficiency
• 15 patients suffering from peripheral arterial occlusive disease with an ankle brachial pressure index (ABPI) of 0.5-0.8
1) 5 patients with ABPI of 0.5 and 0.6 2) 4 ti t ith ABPI f 0 6 d 0 7 2) 4 patients with ABPI of 0.6 and 0.7 3) 6 patients with ABPI of 0.7 and 0.8
• All patients treated with 3M Coban 2 Layer Lite Compression System
• Bandage remained on the leg 1 to 4 days• Study stopped after 14 days
Data on file – 3M
Results of 3M™Coban 2 Layer Lite Compression System Study
• An average supine subbandage pressure of ~ 28mmHg was measured just above the medial ankle after bandage application
• No pressure-related skin damage occurred in patients with reduced arterial perfusion
• No pain related to tissue hypoxia was detected
Data on file – 3M
Results of 3M™Coban 2 Layer Lite Compression System Study
• Laser doppler fluxmetry demonstrated positive effects on microcirculation including:– Increased overall tissue microperfusion – Reduced respiratory reflux in limbs with venous p y
insufficiency– Maintained stable capillary perfusion
• Limb volume reduction (reduced edema) compared to baseline
• High wearing comfort
Data on file – 3M
Demystifying Compression

8
Conclusions: 3M™Coban 2 Layer Lite Compression System Study
• Compression with Coban 2 Layer Lite Compression System is safe and well tolerated by patients with reduced peripheral arterial perfusionp p p
• Results of the laser doppler fluxmetry measurements indicate significant improvements of the dermal microcirculation under this compression therapy
Data on file – 3M
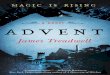
UNDER the Bandage: Increase of Flow
Toe pressure
40
60
80
100
+6% +9% +13%
mm
Hg
TcPO2
20
30
40
50
60
70
+7%
mm
Hg
DISTAL to the Bandage
0
20 n.s.
*** ***
0
10
20***
No impairment of arterial flow up to a pressure of 40 mmHg
Demystifying Compression

9
Ejection fraction
60
70
80
normal range
Inelastic Compression Improves Venous Pump
0
20-3
0
31-4
0
0
10
20
30
40
50
*** ***
+72% +103%
%
Venous Ulcer99 year old lady with ulcer for 8 months
ABI - 0.45
Informed that BK amputation was the
l thonly therapy
Treated with light compression and bi-layered tissue engineered skin
Wound healed after 47 weeks
Compression Bandage Too Tight Over Bony Prominences
Demystifying Compression

10
Sustained bandage pressure should never exceed the arterial perfusion pressure
(= ankle pressure)!
Warning!!!
Persisting or increasing pain:Remove the bandage!
Can compression therapy be used in
the patient with the patient with edema and cellulitis?
Treadwell TA, Fowler E, Bates-Jensen BB. Management of Edema in Wound Care: A Collaborative Practice Manual for Health Professionals, 4th Edition, Ed. BB Bates-Jensen, in press
Edema and Compression Therapy in Cellulitis
1. Normal anti-Streptococcal properties of skin are inactivated by edema fluid
2. Compression therapy:y• Removes protein-containing fluid from the
subcutaneous tissues• Increases blood flow to tissues • Increases antibiotic concentration in tissues
Demystifying Compression

11
Cellulitis of Leg
Healed after10 days of
antibiotics and 5 weeks of
compressioncompression therapy
Does compression therapy improve the skin of patients the skin of patients with venous dermatitis?
Properties of Edema Fluid
1. Edema fluid inhibits mitogenic activity and DNA synthesis.
2 Cytokine environment in edema fluid is more 2. Cytokine environment in edema fluid is more proinflammatory.
3. Protease activity is higher in edema fluid.4. Growth factors levels are decreased in edema
fluid.1. Ratliff, C. R. "Wound exudate: an influential factor in healing." Adv.Nurse Pract. 16.7 (2008):32-35.2. Trengove, N. J., H. Bielefeldt-Ohmann, and M. C. Stacey. "Mitogenic activity and cytokine levels in non-healing and healing chronic leg ulcers." Wound Repair Regen. 8.1 (2000):13-25.3. Trengove, N. J., S. R. Langton, and M. C. Stacey. "Biochemical analysis of wound fluid from nonhealing and healing chronic leg ulcers." Wound Repair Regen. 4.2 (1996): 234-39.
Demystifying Compression

12
Fibroblast Senescence and Venous Ulcers
17 60 66AS
4.00.33SK
12.61BB
14.91KM
Wound (%)Normal (%)Patient
Stanley A, et al. J Vasc Surg. 2001;33(6):1206‐1211.
26.32.33FF
210.33RG
14.31.33OB
17.60.66AS
Fibroblasts and Chronic Wound Fluid
60,000
50,000
40,000
(ce
lls
/da
y)
40
30
e C
ell
s(%
)
†
*P = .006; †P<.03.CM = complete media; VUWF = venous ulcer wound fluid; SA‐‐Gal = senescence‐associated ‐galactosidaseactivity.Mendez MV, et. al. J Vasc Surg. 1999;30:734‐743.
30,000
20,000
10,000
0
Gro
wth
Ra
te
*
CM VUWF
20
10
0
SA
--G
al
Po
sit
ive
CM VUWF
Proteases and Compression TherapyRelative MMP Levels in Healthy and Ulcer Tissue
Before and After Compression Therapy
400500
600 HealthyBefore TXAfter TX
otal p
rotei
n N=21
Marston WA, Beider S, Davies S, Berndt DF. Protease and Cytokine Levels in Non-Healing Venous Leg Ulcers Before and After Compression Therapy. Presented at Symposium on Advanced Wound Care/Wound
Healing Society Meeting, San Diego, CA. April 25, 2008
0100200
300
pg/µ
g to
Demystifying Compression

13
normal before after
Inflammatory Cytokines and Compression Therapy
00.002
0.0040.006
0.0080.01
0.012
0.0140.0160.018
0.02
Normal Before Afternormal before after0
0.05
0.1
0.15
0.2
0.25
0.3
normal before afternormal before after
Interleukins
0
2
4
6
8
10
12
14
16
normal tissue ulcer before Rx ulcer after Rx
Il-8
\normal tissue ulcer before RX ulcer after RX0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
0.18
normal before After
Il-1b
normal before after
normal before after
Marston WA, Beider S, Davies S, Berndt DF. Protease and Cytokine Levels in Non-Healing Venous Leg Ulcers Before and After Compression Therapy. Presented at Symposium on Advanced Wound Care/Wound Healing Society Meeting, San Diego, CA. April 25, 2008
TNF-alpha
normal before after
IFN-gamma
normal before after\normal tissue ulcer before RX ulcer after RX
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
norm al before after
IL12p40
normal before after
normal before after
Effect of Compression Therapy
1 Week of Compression
Stasis Dermatitis
Improvement after 22 weeks of
compression ptherapy
Demystifying Compression

14
Can compression therapy be used in the patient with
edema and congestive edema and congestive heart failure?
Massive Edema and CHF
Photo used with permission
Congestive Heart Failure and Compression Therapy
• No acute pulmonary edema• Once treatment started with
di ti l t di ti d cardiostimulatory medications and diuretics
Treadwell TA, Fowler E, Bates-Jensen BB. Management of Edema in Wound Care: A Collaborative Practice Manual for Health Professionals, 4th Edition, Ed. BB Bates-Jensen, in press
Demystifying Compression

15
Can compression therapy be used in the patient with edema and
acute deep venous thrombophlebitis?
Compression Therapy and Acute Deep Venous Thrombophlebitis
• Increases venous flow• Prevents further clotting
O l d fi i l i th t ld l t• Occludes superficial veins that could clot• Does not cause an increase in pulmonary
embolism
Dale AW. The Swollen Limb. Current Problems in Surgery, Year Book Medical Publishers, Inc., USA. 1973 (September), p 18
Treadwell TA, Fowler E, Bates-Jensen BB. Management of Edema in Wound Care: A Collaborative Practice Manual for Health Professionals, 4th Edition, Ed. BB Bates-Jensen, in press
Contraindication to Compression in Acute Deep Venous
Thrombophlebitis
Leg so painful that compression cannot be tolerated.
Dale AW. The Swollen Limb. Current Problems in Surgery, Year Book Medical Publishers, Inc., USA. 1973 (September), p 18
Demystifying Compression

16
Do patients care which compression bandage p g
is used?
Fact: Patients don’t like compression bandages!
• Only 48.8% of patients wore their compression bandages *
• May be as high as 80% *
• Determinants for NOT wearing compression bandages:Determinants for NOT wearing compression bandages:a. Ageb. Pain c. Wound sized. Wound depth
* Miller C, Kapp S, Newell N, et al. Predicting Concordance with Multilayer Compression Bandaging. Jour Wound Care 2011;20(3):101-112
Is this comfortable?
Demystifying Compression

17
10
actico k-two profore profore lite proguide short stretch long stretch rosidal sys coban 2 layer coban 2 lite
0
1
2
3
4
5
6
7
8
9
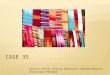
10Slippage in cm: after 24 and 48 hours
actico k-two profore profore lite proguide short stretch long stretch rosidal sys coban 2 layer coban 2 lite
After 48 hours of wear
Patient Preference for Compression Therapy
• 72% of patients preferred Coban 2 Layer Compression System over Profore when treated with both for venous ulcer
• Coban 2 Layer Compression System showed less slippage than Profore
• Quality of Life assessments were better with Coban 2 Layer Compression System than with Profore (p<0.05)
Moffatt CJ, Edwards L, Collier M, Treadwell T, Miller M, Shafer L, Sibbald G, Brassard A, McIntosh A, Ryzelman A, Price P, Kraus SM, Walters SA, Harding K. Randomized Controlled 8-Week Crossover Clinical Evaluation of the 3M Coban 2 Layer Compression System Versus Profore to Evaluate the Product performance in Patients with Venous Leg Ulcers. Int Wound Journal 2008; 5:267-279.
Compression Questions
1. Are all compression bandages the same? NO2. Can compression therapy be used in the patient with edema and
an ABI < 0.8? YES3. Can compression therapy be used in the patient with edema and
cellulitis? YES 4. Does compression therapy improve the skin of patients with venous
dermatitis? YES5. Can compression therapy be used in the patient with edema and
congestive heart failure? YES6. Can compression therapy be used in the patient with edema and
acute deep venous thrombophlebitis? YES7. Do patients care which compression bandage is used? YES
Demystifying Compression

18
“It is the individual patient who we treat, not the disease. It is the patient who recovers or dies, not the illness.”James Peck, MD, Am. Jour. Surg. 2004;187:569-574
Sponsored by an educational grant from 3M
For more information on 3M Compression Therapy visit 3M Compression Therapy visit
www.3m.com/coban2layer
3M is a provider approved by the California Board of Registered Nursing, Provider Number CEP 5770. Nurse participants may receive continuing education credit upon completion of education module.
Demystifying Compression