Embed Size (px)
Citation preview

iences 269 (2008) 41–48www.elsevier.com/locate/jns
Journal of the Neurological Sc
Dengue encephalopathy in children in Northern India: Clinical featuresand comparison with non dengue
Rashmi Kumar a,⁎, Sanjeev Tripathi a, J.J. Tambe b, Vikas Arora a, Amit Srivastava a, V.L. Nag c
a Department of Pediatrics, Chhatrapati Shahuji Maharaj Medical University, Lucknow, (U.P.) 226003, Indiab Kalawati Saran Children's Hospital, New Delhi, India
c Department of Microbiology, Chhatrapati Shahuji Maharaj Medical University, Lucknow, India
Received 19 September 2007; received in revised form 11 December 2007; accepted 14 December 2007Available online 28 January 2008
Abstract
Background: Acute febrile encephalopathy (AFE) is a common cause of childhood hospital admissions in Lucknow. In recent years, manypatients have been hospitalized with AFE and hemorrhagic manifestations, some of whom were proven to have dengue viral infection.Objectives: To (i) define the role of dengue encephalopathy (DE) as a cause of AFE in children in Lucknow, (ii) document features of denguehemorrhagic fever (DHF) in them and (iii)compare clinical features of definite dengue and non dengue AFE.Study design: Prospective study at a teaching hospital in northern India. Children between 1–12 years of age hospitalized with fever andaltered consciousness of 2 weeks or less duration were enrolled after excluding bacterial and tuberculous meningitis and frank hepaticencephalopathy. Clinical and laboratory details were charted. Haemagglutination inhibition (HI) test for dengue and Japanese encephalitisviruses in paired sera and IgM antibody capture ELISA for dengue were done. Real time PCR was done in those samples testing positive fordengue IgM. Those with either positive HI test or positive dengue PCR in CSF or serum were considered definite dengue infection andfeatures of DHF were charted in them. Those negative for IgM antibodies after 5 days of illness or whenever done, HI test, were considereddefinite non dengue. Clinical and laboratory features were compared between definite dengue and non dengue groups.Results: A total of 265 patients of AFE were enrolled over a 2 year period. HI test was positive in 15/49 (30.6%) and IgM in 52/238 (21.8%)patients thus tested. A total of 62 patients were positive for dengue antibodies by either test. Real time PCR assay for dengue virus genomewas positive in 28/42 (69%) tested — 21/29 (72.4%) in CSF and 9/15 (60%) in serum. A total of 39 patients met the criteria for definitedengue infection of which only 2 fulfilled the WHO criteria for DHF. Comparing DE and non DE, rash, bleeding, swelling over body, andhepatomegaly were significantly more common and meningeal signs less frequent in DE. Mean platelet counts and serum albumen werelower and liver enzymes and INR were significantly higher in DE.Conclusions: Dengue viral infection is a cause of AFE in children in this region. Majority of DE here appears to be due to viral invasion ofbrain as suggested by high PCR positivity in CSF and lack of WHO criteria for DHF. Differentiating features of DE include swelling andhepatic dysfunction.© 2007 Elsevier B.V. All rights reserved.
Keywords: Acute febrile encephalopathy; Dengue encephalopathy; Dengue hemorrhagic fever; Viral encephalitis
1. Introduction
Dengue infections are a global public health problem,being the most important arbovirus infection of humans and
⁎ Corresponding author. Tel.: +91 522 2374777 (Home), 2257377 (Work).E-mail addresses: [email protected], [email protected]
(R. Kumar).
0022-510X/$ - see front matter © 2007 Elsevier B.V. All rights reserved.doi:10.1016/j.jns.2007.12.018
the most important tropical infectious disease after malaria[1]. Over the last 50 years more complicated forms of theinfection — dengue hemorrhagic fever (DHF) and dengueshock syndrome (DSS) have been recognized [1]. DHF isknown to have neurological manifestations includingencephalopathy [2–9].
Acute febrile encephalopathy (AFE), defined as fever andaltered sensorium of 14 days or less duration in a previously

42 R. Kumar et al. / Journal of the Neurological Sciences 269 (2008) 41–48
normal child [10], is a common problem presenting to us inLucknow, India. Causes include cerebral malaria, bacterialmeningitis, viral encephalitis etc. Over the last few years,manypatients have been admitted in our wards with AFE along withhemorrhagic manifestations, some of which were proven to bedengue viral infections. The present study was thereforeundertaken to define the role of dengue viral infection as acause of AFE in children in Lucknow and to delineate clinicaldifferentiating features of dengue encephalopathy (DE).
2. Subjects and methods
The study was conducted in the Childrens' wards ofChhatrapati Shahuji Maharaj (CSM) Medical University,Lucknow, which is the capital city of the state of Uttar Pradesh(or the northern state). This state is India'smost populous (witha population of a 160 million, about 1/6th of that of the wholecountry) and also one of its poorest with lowest humandevelopment indices. It is divided into 70 districts oradministrative units. This part of the country is the gangeticplain of northern India. The state's population density is 689people/km2 and children below 12 years account for roughly40% of the population [11]. About 79% of the people live inrural areas. There are 3 seasons — summer (March to June),rainy or monsoon season (July to October) and winter(November to February). Temperatures may soar up to45 °C in summer and fall as low as 3 °C in winter.
Lucknow, the state capital has a population of 4 million.The CSM Medical University Hospital is a tertiary careteaching hospital which caters mostly to the poor andseverely ill. The catchment area of the hospital includes theLucknow city and district and other eastern districts ex-tending up to Nepal. The pediatric services of this hospitalwhich cater to medical problems from birth to 12 years ofage, have been admitting about 150–200 cases of ‘encepha-litis’ annually — mostly in the monsoon and post monsoonseason. Since facilities for viral diagnosis are not regularlyavailable or are too expensive, most cases do not undergovirological investigations but are presumed to be Japaneseencephalitis which is known to be endemic in the easternregions of the state. Over the last decade, the region isrecognized as a high dengue transmission area and a severeepidemic of DF/DHF occurred in late 2003.
Children between 1–12 years of age hospitalized withAFE were screened for enrollment in the study. Those inwhom a firm diagnosis of bacterial or tubercular meningitiswas made on the basis of CSF examination or imaging orthose in whom consent was not obtained were excluded.Frank cases of hepatic encephalopathy with jaundice werealso excluded and the remaining cases were enrolled in thestudy. The enrolled children were worked up according to apre-designed protocol incorporating a detailed history andexamination including general, systemic and neurologicalexamination. Signs of raised intracranial tension were hyper-tension or bradycardia with hyperventilation or decerebra-tion. Investigations done at admission were complete blood
counts including packed cell volume (PCV) and plateletcount, liver function tests including s. bilirubin, s AST andALT, serum proteins, albumen and prothrombin time.Wherever possible and indicated, cerebrospinal fluid (CSF)was tapped at admission and examined for cells, protein andsugar. In addition, 5 ml blood was also collected on admis-sion in Eppendorf tubes and transported to the VirologyLaboratory of CSM Medical University, Lucknow forserological investigations. Convalescent sera were obtainedwhenever possible at least one week after acute serum or at thetime of discharge. Daily follow up was done till discharge.Haemagglutination inhibition (HI) test was done in 2003 onacute and convalescent phase sera by standard methods [12]for dengue and Japanese encephalitis (JE) viruses. The test wasconsidered positive for dengue if paired sera showed a 4 foldrise or fall in dengue HI antibodies without a similar responsein JE virus antibodies. IgM estimation for dengue viruswas also done in acute serum by IgM antibody captureELISA using commercial kits marketed by Focus Technolo-gies, USA.
2.1. Real time quantitative PCR
Serum and CSF samples from patients testing positive orborderline (equivocal) for dengue IgM were subjected toReal Time polymerase chain reaction (PCR) assays. TotalRNA was extracted by column based extraction kits ofQiagen (Viral RNA Mini kit). Real time PCR was performedon Rotor Gene 3000, (Corbett Research Australia) usingTaqMan probes, and primers designed to pick up all the fourtypes of dengue virus synthesized according to Drosten et al.by Tibmolbiol, Berlin, Germany [13] (provided by Profes-sional Biotech, New Delhi). Single tube RT-PCR was per-formed using Single tube RT/PCR premix obtained fromProfessional Biotech, Ltd. Standard curves were establishedwith plasmids whichwere cloned PCR products obtained fromclinical samples (Tibmolbiol) and contained complete cDNAsequence of the gene. Serial dilutions were prepared, starting at105 copies of the specific plasmid, to interpolate the unknowncopy number of specific RNA in each sample.
A case was considered to have ‘definite’ dengueinfection if either HI test in paired serum was positive orif Real Time PCR was positive in serum or CSF. A casewas considered as ‘non dengue’ if IgM test done on bloodsample collected after 5 days from onset of illness wasnegative and wherever done, HI test in paired sera showed norise or fall in HI antibodies and PCR for dengue genome wasnegative. A case of dengue viral infection was considered asdengue encephalitis if CSF Real Time PCR was positive. Acase testing IgM positive but equivocal or not tested by HI testand negative or not tested on PCR was considered ‘probabledengue’.
WHO criteria for DHF [14] were looked for in those withproven dengue viral infection.
Ethical Approval was obtained for the study by theInstitutional Review Board of Indian Clinical Epidemiology

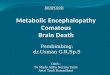
Fig. 1. Flow diagram showing flow of patients.
43R. Kumar et al. / Journal of the Neurological Sciences 269 (2008) 41–48
Network (IndiaCLEN) and from the Ethics Committee ofChhatrapati Shahuji Maharaj Medical University, Lucknow.
3. Results
A total of 265 cases of acute febrile encephalopathy(AFE) fulfilling criteria mentioned under Subjects andmethods were enrolled over the study period betweenAugust 2003 to July 2005.
3.1. HI tests
HI tests in paired sera for dengue and JE antibodies weredone in 2003 in 49 and 44 patients respectively. Fifteen of 49(30.6%) were positive for dengue and 9/44 (20.4%) werepositive for JE according to criteria given under Subjects andmethods.
3.2. IgM ELISA for dengue in serum
This was performed in a total of 238 patients, of which 52(21.8%) were positive and 5 were equivocal.
3.3. Dengue IgM versus HI result
Five patients had both IgM and HI test positive fordengue. Thus a total of 62 patients had one or both testspositive for dengue antibodies.
3.4. Dengue PCR
A total of 42 IgM positive or equivocal patients weretested by PCR. Fifteen patients had real time PCR in serum,of which 9 (60%) were positive. Number of RNA copies/mlranged from 35 to 256,688. Twenty nine CSF samples couldbe tested for dengue genome by Real time PCR, of which 21(72.4%) were positive, number of RNA copies ranging from138 to 68,718. Two patients were positive in both serum andCSF, so a total of 28 patients were positive in either or bothCSF or serum.
Four patients were positive by both PCR and HI test inpaired sera. So a total of 39 patients were positive by either orboth of these tests i.e. ‘definite dengue’. A total of 130patients fulfilled the criteria for ‘non dengue’ encephalo-pathy as described under Subjects and methods. Of the

44 R. Kumar et al. / Journal of the Neurological Sciences 269 (2008) 41–48
remaining 96 patients, 9 were JE and 26 were ‘probabledengue’ again according to criteria under Subjects andmethods. All the 96 patients were excluded from analysis.
Fig. 1 shows the test results on patients.Tables 1 and 2 compare clinical features at admission,
mortality and laboratory features at admission of DE and nonDE patients respectively. Mean age of DE patients washigher than non DE. The illness generally started withsudden onset of fever followed within 2–6 days by aconvulsion in the form of generalised tonic spasm, andaltered sensorium. Generalised increase in tone, rash,swelling all over the body, hepatomegaly, gastric bleedingand other bleeds were common manifestations in DE.Hyperventilation initially was observed in 13 DE patients.Meningeal signs were significantly more common in nonDE. Cranial nerve palsies were in the form of facial palsy in 3and facial palsy with ophthalmoplegia in one DE patient.Abnormal behaviour was observed in 2 DE patients andabnormal movements in one. Pain abdomen was complainedof in 3 patients. DE patients who died generally had severeincrease in tone, decerebration and peripheral vascular failureterminally. Those who survived usually made a completerecovery.
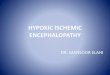
Fig. 2 shows characteristic facial swelling in a case of DE.
Table 1Demographic and clinical features at admission and mortality of DE and non DE
Variable Non dengue (130)
Age in months a 62.5 (41.2)Sex male b 91 (68.9)Weight for age a 80.9 (15.7)Duration since onset in days a 7.8 (3.9)Duration of prodrome in days a 4.7 (3.3)Convulsions b 112 (86.2)Convulsion type b
Generalised tonic 75/107 (70.1)Focal 13/107 (12.1)
Headache b 24 (18.5)Vomiting b 64 (49.6)Rash b 12 (9.2)Diarrhea b 13 (10.0)Gastric bleeding b 24 (18.5)Other bleed b 8 (6.1)Tourniquet test b 0 (0)Glasgow Coma Scale a 7.87 (2.47)Swelling b 11 (8.5)Hepatomegaly b 51 (39.2)Splenomegaly b 5 (3.8)Meningeal signs 46 (35.4)Fundus — papilledema b 15/118 (12.9)Increased tone b 83 (63.8)Cranial nerve palsies b 18 (13.8)Neurological deficits b 21 (16.1)Signs of ↑ intracranial tension b 30 (23.0)Died 42 (32.8)
a Number ( ) represent mean (SD) and 2 sample test was used.b Number ( ) represent number of patients (%) and χ2 test was used.c Significant.
Clinical and laboratory features of the 26 ‘probabledengue’ cases were similar to the definite dengue cases andthere were no significant differences between these 2 groupson univariate analysis.
Clinical features, mortality and laboratory data were alsocompared between 9 serum PCR +ve (viremic) patients andthe remaining 30 definite dengue patients and no significantdifferences were observed. All the same parameters werealso compared between 21 CSF PCR +ve (encephalitis)patients and the remaining 18 definite dengue patients andthe only significant difference was in mean age which waslower in encephalitis patients (64.6+/−40.4 versus 91.6+/−39.6 (p=0.042).
4. Discussion
The occurrence of neurological manifestations in dengueinfections has been recognized for long [2–9]. The cause ofencephalopathy in dengue was believed to be vasculitis withfluid exudation, cerebral edema, hypoperfusion and hypona-tremia [15]. Recently, however, direct neurotropic potential ofthe virus has been well recognized [15–20] primarily fromstudies in countries of southeast Asia [15,17,18,20]. Althoughencephalopathy with dengue infection was considered ‘not
patients
Dengue (39) OR (95% CI) P value
77.1 (41.8) – 0.05429 (74.3) 1.24 (0.52–3.03) 0.598
80.9 (12.5) – 0.9937.8 (4.7) – 0.9424.8 (4.6) – 0.30831 (79.5) 0. 62 (0.24–1.56) 0.311
25/30 (83.3) 2.13 (0.69–7.01) 0.1481/30 (3.3) 0.25 (0.01–1.97) 0.14010 (25.6) 1.52 (0.65–3.54) 0.32616 (41.0) 0.70 (0.34–1.45) 0.34611 (28.2) 3.86 (1.54–9.65) 0.002 c
5 (12.8) 1.32 (0.44–3.97) 0.40314 (35.9) 2.62 (1.18–5.80) 0.014 c
9 (23.1) 4.65(165–13.05) 0.001 c
2 (5.1) – 0.0528.79 (2.05) – 0.06313 (33.3) 5.40 (2.18–13.41) 0.000 c
24 (61.5) 2.47 (1.18–5.16) 0.013 c
4 (10.2) 2.86 (0.60–13.7) 0.2147 (17.9) 0.39 (0.16–0.96) 0.037 c
2/34 (5.9) 0.43 (0.06–2.13) 0.36323 (58.9) 0.81 (0.37–1.80) 0.5814 (10.3) 0.72 (0.22–2.26) 0.5694 (10.2) 0.62 (0.20–1.92) 0.4008 (20.5) 0.86 (0.35–1.81) 0.7369 (23.1) 0.61 (0.25–1.5) 0.247

Table 2Investigations at admission in DE and non DE
Variable Non dengue (130) No (%) Dengue (39) No (%) OR (95% CI) P value
Hb (g %) a 10.25 (1.73) 10.66 (2.27) – 0.194TLC/mm3 a 9151 (2550) 10,146 (5511) – 0.640
(Normal value 4000–11,000/mm3)Polymorphs in blood % a 67.45 (12.24) 69.18 (11.39) – 0.439Platelets/mm3 a 176,768 (80154) 163,936 (133482) 0.068Plateletsb.100,000 b/mm3 9 (7.4) 13/38 (34.2) 6.47 (2.49–16.80) 0.000 c
Normal value: 1.5–4.0×105/mm3
Packed cell volume a 31.53 (5.12) 32.0 (4.30) – 0.642PCVN36 b 14/122 (11.5) 2/32 (6.25) 0.51 (0.08–2.58) 0.526CSF cells (total) 45.2 (94.9) 64.0 (111.6) – 0.314N10/mm3 b 49/127 (38.6) 16/36 (44.4)
Normalb5 cells/mm3
CSF–polymorphs % a 35.3 (42.5) 44.0 (37.0) – 0.330CSF protein (mg %) a 47.7 (45.9) 61.9 (44.8) – 0.103
Normal value: 20–40 mg %CSF:blood sugar ratio a 0.64 (0.29) 0.62 (0.21) – 0.788
Normal value 66%Total S bilirubin mg % 0.97 (0.55) 0.95 (0.76) – 0.177
Normal valueb1 mg %S AST IU/l a 70.18 (84.71) 129.31 (111.23) – 0.046 c
b=40 b 22/32 (68.7) 4/16 (25.0) 0.15 (0.03–0.69) 0.004 c
41–200 b 7/32 (21.9) 9/16 (56.3) 15.34 (6.11–38.52) 0.000 c
N200 b 3/32 (9.4) 3/16 (18.8) 2.23 (0.39–12.6) 0.311Normal valueb15–40 U/l
S ALT IU/l a 42.83 (35.79) 116.12 (93.90) – 0.000 c
b=40 b 93/122 (76.2) 3/38 (7.9) 0.03 (0.01–0.10) 0.000 c
41–200 b 28/122 (23.0) 32/38 (84.2) 17.9 (6.3–53.5) 0.000 c
N200 b 1/122 (0.81) 3/38 (7.9) 10.37 (0.92–267.4) 0.041 c
Normal valueb15–40 U/lTotal s protein g % a 6.20 (0.90) 6.11 (0.98) – 0.620
b=5 g % 10 (8.1) 6/38 (15.8) 2.10 (0.62–6.93) 0.214b=6 g % 55 (49.1) 14/38 (36.8) 1.15 (0.52–2.56) 0.707Normal value 7–8 g %
S albumen g %a 3.45 (0.62) 3.17 (0.69) – 0.004 c
Normal value 4–5 g %Alb:globulin ratio a 1.30 (0.40) 1.11 (0.31) – 0.04 c
Normal value: N1.0International Normalised Ratio (INR) a 1.16 (0.18) 1.65 (1.00) – 0.000 c
S sodium (mEq/l) a 136.31 (14.37) 139.46 (10.50) – 0.288Normal value 130–145 mEq/l
S potasium (mEq/l) a 4.30 (0.78) 4.44 (0.84) – 0.355Normal value 3.5–4.5 mEq/l
Urea mg %a 35.54 (18.76) 44.19 (28.21) – 0.138Normal value: 20–40 mg %
Creatinine mg %a 0.84 (0.40) 0.97 (0.81) – 0.627Normal value 1 mg %
Pleural effusion 0/126 (0) 2/36 (5.5) – 0.048 c
a Number ( ) represent mean (SD) and 2 sample test was used.b Number ( ) represent number of patients (%) and χ2 test was used.c Significant.
45R. Kumar et al. / Journal of the Neurological Sciences 269 (2008) 41–48
uncommon’, encephalitis with viral invasion of brain was heldto be rare [7]. In India too, neurological complications ofdengue have been recognized [21]. However encephalopathywas noted in only 4% of cases in the 1996 epidemic of denguein Delhi [22]. This is at variance with our own observationsduring the 2003 epidemic of dengue in Lucknow. In thepresent study also, 39 (14.7%) of 265 AFE patients tested hadindicators of definite dengue infection while another 26 had
‘probable dengue’. At least in the Lucknow region, encephalo-pathy is an important presentation of dengue infection.
Our approach in this study was to enroll consecutivepatients presenting with AFE and systematically look forevidence of dengue infection. Those testing positive werethen compared in their clinical and laboratory profiles withthose without any evidence of this infection. To the best ofour knowledge this is the first such study from the Indian

Fig. 2. Characteristic facial swelling in DE.
46 R. Kumar et al. / Journal of the Neurological Sciences 269 (2008) 41–48
subcontinent. Strengths of the study are the prospectiveenrollment of consecutive cases and standardized work upover 2 calendar years. Since AFE is so common here, wecould enroll a sizeable number of cases. Standard WHOcriteria were used for diagnosis of dengue infection.Weaknesses included overlap with other causes of AFE.We excluded cases of bacterial or tuberculous meningitis, butstill some misclassification may have occurred. Hepaticencephalopathy with frank jaundice was excluded because itis a distinct clinical syndrome. We considered all IgMnegative patients tested after 5 days of illness as ‘definite nondengue’ and this may also have caused some misclassifica-tion but expect this to be minor. PCR assays were onlypossible in 42 patients. Convalescent sera were difficult toobtain because many patients died in the acute stage or weredischarged early. The HI tests were discontinued in ourinstitution in 2004. So we depended on acute phase IgMestimation by ELISA for the initial work up.
IgM however, has its limitations in the diagnosis ofdengue infection. Studies have shown 80% positivity in thefirst 5 days of illness, 93% positivity between 6 and 10 daysof illness onset and 99% positivity after the 10th day [1]. Anegative IgM in a patient sampled early in the illnesstherefore does not totally rule out dengue infection. On theother hand, a positive IgM does not always mean that thecurrent illness is dengue, but that dengue infection hasoccurred in the recent past i.e. 60–90 days. IgM positivitytherefore may merely mean that dengue transmission isgoing on. Further, although IgM type antibodies are held tobe specific between flaviviruses, some cross reactivity wasstill possible especially with Japanese encephalitis which isendemic here. Due to these limitations, WHO has putdiagnosis of dengue infection on basis of positive acutephase IgM ELISA test as ‘probable’ only.
We further went on to do Real Time PCR assays fordengue genome in 42 of our IgM positive patients and founda large proportion of CSF (21/29) and serum (9/15) positive.The high positivity in CSF suggests that actual dengueencephalitis with viral invasion of the brain is not such a rareentity as was hitherto believed, asmajority of DE appears to be
due to actual viral invasion. Dengue virus so far is considered aweakly neurotropic virus but our data suggest that a highlyneurotropic strain may be prevalent in this region.
Our ‘non dengue’ group comprised of other febrileencephalopathies seen here. Besides bacterial and tubercu-lous meningitis, Japanese encephalitis, other undefined viralencephalitides, Reye's encephalopathy, cerebral malaria,enteric and electrolyte encephalopathy are also causes offebrile encephalopathy seen here.
The only somewhat similar studies are those conductedby Solomon et al. who studied 378 cases of suspectedencephalitis in southern Vietnam and found evidence ofdengue infection by IgM and IgG antibodies, virus isolationor dengue PCR in 16 (4.2%) [17]; and Kankirawatana et al.who studied 44 children in Thailand of which 8 (18.1%) hadpositive dengue serology. Four of these had positive denguePCR and one had dengue virus isolation from CSF. Theseworkers concluded that patients with encephalitis likepresentation should be tested for dengue whether or notother features of the infection are present [20]. However,neither of these groups of investigators compared clinicalfeatures of dengue infected and non dengue groups. Cam etal. reported a case control study of 27 serologically provenDHF patients with neurological manifestations from among5400 patients admitted with DHF. Controls were 27 age andsex matched DHF patients without CNS symptoms.Hematocrit and platelets were deranged more severely inthe control group but all the liver function tests werederanged significantly more severely in the study group [18].Misra et al. studied 17 patients of dengue virus infection withneurological manifestations in Lucknow during 2003–2005.Eleven of these presented with encephalopathy and 6 withacute motor weakness. Diagnosis of dengue infection wasbased on IgM positivity alone [23].
Comparison of clinical features between DE and non DErevealed that rash and bleeding manifestations significantlymore common in DE. These are well known features of DF/DHF. A peculiar non pitting edema all over the body wasobserved significantly more commonly inDE patients (Fig. 1).This feature has not been sufficiently highlighted in literatureso far, and may be caused by capillary leak and/or low serumprotein or altered albumen: globulin ratio. Tourniquet test wasnegative almost uniformly. Of the neurological features,meningeal signs were significantly more common in the nondengue group. DE tends to have less focal deficits and lowermortality than other AFE seen here, although these differencesdid not reach significance.
Comparison of laboratory features shows that low plateletswere significantly more frequent in the dengue group. Nosignificant differences were found on CSF examination butliver function tests (LFT) were significantly more deranged inthe dengue group. Dengue virus is known to be hepatotropicand this property may be more pronounced with certainserotypes. The slight derangement observed in the non denguegroup may be because this group included illnesses likecerebral malaria, Reye's encephalopathy and enteric fever, all

47R. Kumar et al. / Journal of the Neurological Sciences 269 (2008) 41–48
of which could result in liver dysfunction. Low plateletsand elevated liver enzymes were observed in some of ourJapanese encephalitis patients seen during the epidemic of2005 also.
Differentiation between dengue and other encephalopa-thies prevalent here by clinical and simple laboratoryfeatures is important because sophisticated virologicalinvestigations are not generally available in regions wheredengue occurs. Our observations suggest that although mostneurological manifestations do not differ significantly be-tween dengue and non dengue AFE, the illness can usuallybe distinguished on the basis of other features of dengueinfection such as LFT, rash, swelling, thrombocytopenia andbleeding. Of these, LFT and swelling are not presently in theWHO criteria. However, since 3 of 39 patients did not showany feature of dengue, the illness should be kept in mind inendemic areas even when none of these characteristic featuresare present. Solomon et al. [17] found a much higher pro-portion (12/21 or 57%) of their DE patients without any typicalfeature of dengue. Our ‘probable dengue’ cases were probablyalso DE although they did not strictly fit the WHO criteria for‘confirmed’ dengue infection.
We also looked for WHO criteria for case definition ofDHF in our patients — both definite dengue infection andIgM positive groups. Only 2 of our 39 patients fulfilled allthe WHO criteria for diagnosis of DHF. This could bepossible if most of our patients had DF and dengue viralinvasion of brain without having DHF. The other explanationmay be that WHO criteria for DHF may not really hold truein our population. Many Indian workers have expresseddifficulty in applying the WHO criteria for DHF [22,24–26].Bleeding manifestations and low platelet count may not beseen in all patients and the tourniquet test has been rarelypositive [23,24]. In a country like India where prevalence ofanemia in varying grades of severity is high, the baselinepacked cell volume (PCV) is not known. Gomber et al. [26]tried to establish a cut off for PCV for our population and putthe figure at 36. Using this cut off, only 2 of our definitedengue patients had a high PCV suggestive of DHF.However, since the population hemoglobin is so variablehere, usefulness of any such cut off is debatable. No cut off forhypoproteinemia has been defined and again this finding waspresent in only a minority of our patients. Pleural effusion wasseen in only 2 cases, although a plain radiograph of the chestwas obtained in 212 patients. The other criterion for plasmacapillary leak— ascites may be detected on ultrasonographicexamination of the abdomen which is not easy in settingswhere dengue cases are seen especially in sick children whowould require a bedside ultrasound. This investigation was notdone in any of our cases. In a recent communication fromWHO, Bandyopadhyay et al. analysed 37 post 1975 papers ondengue classification [27]. Most studies reported difficulties inapplying the WHO criteria for DHF. A positive tourniquet testrepresenting the minimum requirement for a hemorrhagicmanifestation did not distinguish between DF and DHF. Incases of DHF, thrombocytopenia was observed in 8.6–96%,
plasma leak in 6–95% and hemorrhagic manifestations in 22–93%. These workers have concluded that a large multicentricstudy conducted over different dengue endemic areas isrequired to redefine criteria for diagnosis of DHF and modifythe current dengue classification.
Within our definite dengue group, we have a smallergroup of patients with PCR positive in CSF who can beclassified as ‘dengue encephalitis’. This subgroup of 21patients when compared with the remaining definite denguepatients was found to have a significantly younger mean age.This may mean that encephalitis may be seen even in primaryinfection whereas DHF being a manifestation of secondaryinfection occurs in a older age group. Similarly, the 9 patientswith PCR positive in serum can be regarded as having dengueviremia but lack of statistically significant differences betweenthese and the remaining dengue patients could be due to thesmall numbers.
Acknowledgements
This study was partly financially supported by a grant fromUSAID/INCLEN. We are grateful to M/s Professional Biotech PvtLtd, New Delhi for their help with the real time PCR studies.
References
[1] Gubler DJ. Dengue and dengue hemorrhagic fever. Division of VectorBorne Infectious Diseases, National Centre for Infectious Diseases,Centre for Disease Control and Prevention; 1999.
[2] Sumarno Wuler H, Jahja E, Gubler DJ, Suharyono W, Sorenson K.Clinical observations on virologically confirmed fatal dengue infec-tions in Jakarta, Indonesia. Bull WHO 1983;61(4):693–701.
[3] Hendarto SK, Hadinegoro SR. Dengue encephalopathy. Acta PaediatrJpn Overs Ed 1992;34(3):350–7.
[4] Patey O, Ollivaud L. Unusual neurologic manifestations occurringduring dengue fever infection. Am J Trop Med Hyg 1993;48:793–802.
[5] David R, Philip W. Dengue fever with encephalopathy in Australia.Am J Trop Med Hyg 1996;54:253–5.
[6] Thisyakorn U, Limpitikul W. Dengue infection with central nervoussystem manifestations. Southeast Asian J Trop Med Public Health1999;30(3):504–6.
[7] Panchareon C, Thisyakorn U. Neurological manifestations in denguepatients. Southeast Asian J TropMed Public Health 2001;32(2):341–5.
[8] Angibaud G, Luauti J, Laille M, Gaultier C. Brain involvement indengue fever. J Clin Neurosci 2001;8(1):63–5.
[9] Srey VH, Sadones H, Ong S, Masm M, Yin C, Sor S, et al. Etiology ofencephalitis syndromes among hospitalized children and adults in Takeo,Cambodia 1999–2000. Am J Trop Med Hyg 2002;66(2):2002–7.
[10] Kalra V. CNS infections in Practical Pediatric Neurology. New Delhi:Arya Publications; 2002. p. 100.
[11] Economic Profile of uttar pradesh available at http://www.economywatch.com/stateprofiles/uttarpradesh/profile.htm Accessed 20th September 2006.
[12] Clarke DH, Casals J. Technique for haemagglutination and haemag-glutination — inhibition with an arthropod borne virus. Am J TropMed Hyg 1958;7:561–73.
[13] Drosten C, Gottig S, Schilling S, Asper M, Panning M, Schmitz H, etal. Rapid detection and quantification of RNA of Ebola and Marburgviruses, Lassa virus, Crimean Congo hemorrhagic fever virus, RiftValley fever virus, Dengue and Yellow Fever virus by real time reversetranscriptase PCR. J Clin Microbiol 2002;40:2323–30.
[14] World Health Organisation. Dengue fever: diagnosis, treatment,prevention and control. 2nd Edition. Geneva; 1997.

48 R. Kumar et al. / Journal of the Neurological Sciences 269 (2008) 41–48
[15] Lum LC, Lam SK, Choy YS, George R, Harun F. Dengue encephalitis:a true entity? Am J Trop Med Hyg 1996;54(3):256–9.
[16] Guzman MG, Kouri G. Dengue: an update. Lancet 2002;3:33–42.[17] Solomon T, Dung MN, Vaughn DW, Kneen R, Thao LTT, Boonyos R,
et al. Neurological manifestations of dengue infection. Lancet2000;355:1053–9.
[18] Cam BV, Fonsmark L, Hue NB, Phuong NT, Poulsen A, Heegaard ED.Prospective case — control study of encephalopathy in children withdengue hemorrhagic fever. Am J Trop Med Hyg 2001;65(6):848–51.
[19] Hommel D, Talarmin A, Deubel V, Reynes JM, Drouet MT, Sarthou JL,et al. Dengue encephalitis in French Guiana. Res Virol 1998;149(4):235–8.
[20] Kankirawatana P, Chokephaibolkit K, Yoksan S, Pathavathana P.Dengue infection presenting with central nervous system manifesta-tions. J Child Neurol 2000;15(8):544–7.
[21] Rajajee S, Mukundan D. Neurological manifestations of denguehemorrhagic fever. Indian Pediatr 1994;31:688–9.
[22] Aggarwal A, Chandra J, Aneja S, Patwari AK, Dutta AK. An epidemicof dengue hemorrhagic fever and dengue shock syndrome in childrenin Delhi. Indian Pediatr 1998;35:727–32.
[23] Misra UK, Kalita J, Syam UK, Dhole TN. Neurological manifestationsof dengue viral infection. J Neurol Sci 2006;244(1–2):117–22.
[24] Narayanan M, Aravind MA, Thilothammal N, Prema R, SargunamCSR, Ramamurty N. Dengue fever epidemic in Chennai— a study ofclinical profile and outcome. Indian Pediatr 2002;39:1027–33.
[25] Srivastava VK, Suri S, Bhasin A, Srivastava L, Bhardwaj M. Anepidemic of dengue hemorrhagic fever and dengue shock syndrome inDelhi — a clinical study. Ann Trop Paediatr 1990;10:329–34.
[26] Gomber S, Ramachandran VG, Kumar S, Agarwal KN, Gupta P.Hematological observations as diagnostic markers in dengue hemor-rhagic fever — a reappraisal. Indian Pediatr 2001;38:477–81.
[27] Bandyopadhyay S, Lum LCS, Kroeger A. Classifying dengue: a reviewof the difficulties in using the WHO case classification of denguehemorrhagic fever. Trop Med International Health 2006;11:1238.