Embed Size (px)
Citation preview

จัดทําโดย วรวฒุิ รุงประดับวงศ & คณา เกษมทรัพย
Dengue
Dengue
www.cueid
.org

Slide 2
Introduction
• Most important arbovirus (arthropod-borne virus)• Estimated 100 million cases per year• 2.5 billion people at risk• No antiviral treatment and vaccines• Best known for causing
- fever-arthralgia-rash syndrome (dengue fever)- hemorrhagic syndrome (DHF)
เช้ือไวรัสเด็งกี่เปนเช้ือ arbovirus หรือ arthropod-borne virus ซ่ึงก็คือเช้ือไวรัสที่อาศัยยุงเปนพาหะในการแพร
เช้ือที่มีความสําคัญมาก โดยพบประมาณ 100 ลาน case ตอป และมปีระมาณ 2,500 ลานคนที่เส่ียงตอการ
ติดเชื้อ เช้ือไวรัสชนิดน้ี ยังไมพบยาตานไวรัส และวัคซีนในการรักษา และเปนที่รูกนัวา เช้ือไวรัสเด็งกี่ เปนเชื้อท่ี
กอโรค fever-arthralgia-rash dyndrome หรือ dengue fever และ Hemorrhagic syndrome หรือ Dengue
Hemorrhagic Fever
www.cueid
.org
Slide 3
Dengue Virus
• Flavivirus genus, Flaviviridae family• Morphology
- small (50 nm)- spherical enveloped particles- 11 kb of ss positive sense RNA wrapped in a nucleocapsid core protein
• Dengue serocomplex- dengue-1, dengue-2, dengue-3, and dengue-4
Dengue virus อยูใน genus Flavivirus, Family Flaviviridae โดยมีลักษณะเหมือนเช้ือใน genus Flavivirus
อ่ืนๆคือ มีขนาดเล็กประมาณ 50 นาโนเมตร เปลือกหุมลักษณะเปนทรงกลม ภายในประกอบดวย single-
stranded positive sense RNA ซ่ึงถูกหุมอยูใน nucleocapsid core protein, dengue serocomplex หรือ
serotype ประกอบดวย 4 ชนิด คือ Dengue-1, -2, -3, และ -4
www.cueid
.org

Slide 4
Viral Attachment and Entry
• Envelope (E) protein- the largest structural protein- nearly 500 amino acids- 6 disulfide bridges- 2 potential glycosylation sitesvery similar for all flavivirusesMajor target of the humoral immune responseImportant in viral entry into host cells
การที่เช้ือไวรัสจะสามารถเขาสู host cell ได ตองอาศัย envelope protein ซ่ึงเปนสวนโครงสรางท่ีใหญที่สุด
ประกอบดวย amino acid ประมาณ 500 ตัว, 6 disulfide bridges และ 2 potential glycosylation sites โดย
โครงสรางเหลาน้ี จะคลายคลีงกันในกลุม flaviviruses และเปน major target ของ humoral immune
response ดวย
www.cueid
.org

Slide 5
Viral Attachment and Entry• Studies with monoclonal antibodies
- 3 antigenic domains domains II,III, and I- Domain III - putative receptor binding domain- Domain II - dimerization domain
- contains a putative fusion sequence- Domain I - central beta barrel
- hinge domain• Attachment Endocytosis Fusion of membrane
release of virion nucleocapsid into cytoplasm
จากการศึกษาโดยใช monoclonal antibodies พบวา Envelope มี 3 antigenic domains คือ domain I, II,
and III, ในสวน domain III เปน receptor binding domain ซ่ึงเช้ือไวรัสใชในการจับกับ host cell receptor,
domain II ประกอบดวย fusion sequence ชวยใหเช้ือสามารถ fuse กับ host cell membrane และ domain I
มีหนาที่เปน hinge domain ที่คอยเชื่อม 2 domains ไวดวยกนั สําหรับกระบวนการทีเ่ช้ือจะเขาสู host cell ก็
เร่ิมจาก Attachment Endocytosis � Fusion ของ virion & host membrane � ปลอย virion
nucleocapsid เขาไปยัง cytoplasm
www.cu
eid.or
g
Slide 6
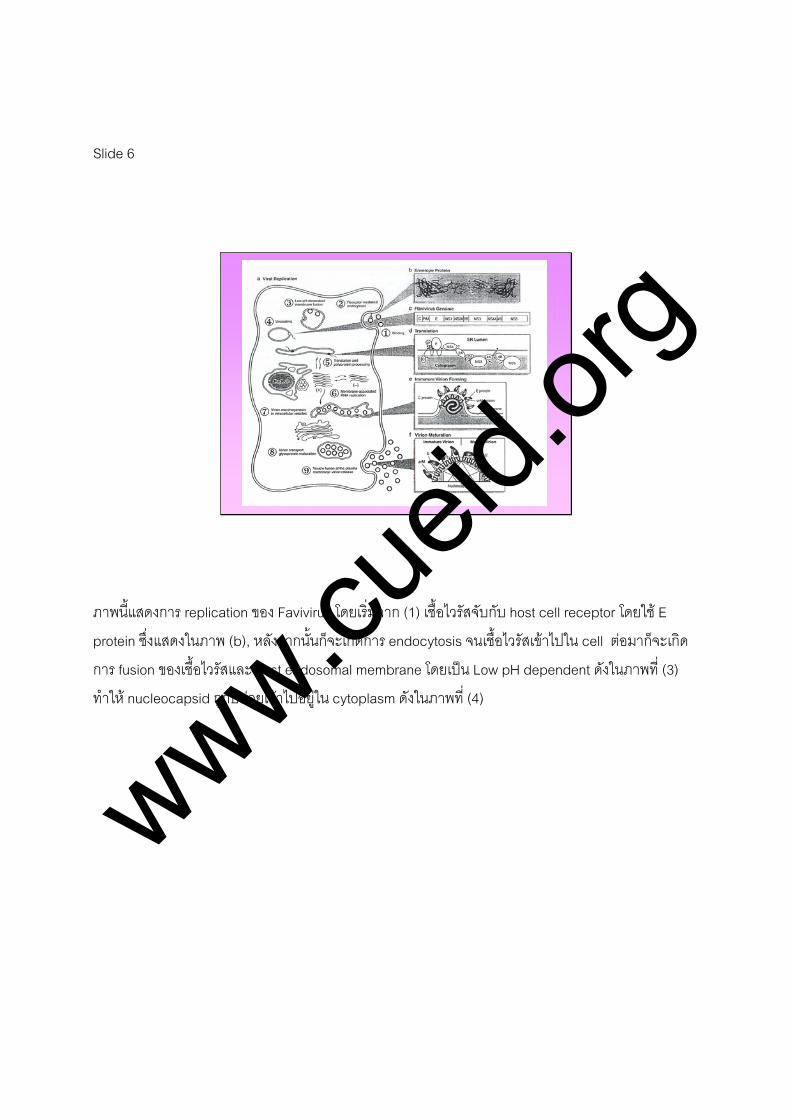
ภาพนี้แสดงการ replication ของ Favivirus โดยเร่ิมจาก (1) เชื้อไวรัสจับกับ host cell receptor โดยใช E
protein ซ่ึงแสดงในภาพ (b), หลังจากนั้นก็จะเกิดการ endocytosis จนเช้ือไวรัสเขาไปใน cell ตอมาก็จะเกิด
การ fusion ของเชื้อไวรัสและ host endosomal membrane โดยเปน Low pH dependent ดังในภาพที่ (3)
ทําให nucleocapsid ถูกปลอยเขาไปอยูใน cytoplasm ดังในภาพที่ (4)
www.cueid
.org

Slide 7
Viral Replication and Release
• Viral replication begins on surface of the endoplasmic reticulum
• Viral RNA is translated into a single 3,000 amino acid polyprotein
• Cleaved by host and viral proteases into the 3 structural (C, PrM, and E) and 7 nonstructural proteins (NS1, NS2A, 2B, NS3, NS4A, 4B, NS5)
• Positive-sense RNA is transcribed into negative-sense intermediate template
หลังจากที่ปลอย nucleocapsid เขาไปใน cytoplasm ไดแลว เชื้อไวรสัเด็งกี่ก็จะเพ่ิมจํานวนหรือ replicate
ตัวเอง ซึ่งเร่ิมที่ surface ของ endoplasmic reticulum โดยอันดับแรก Viral RNA จะถูก Translate ไปเปนสาย
amino acid polyprotein สายเด่ียว ซ่ึงประกอบดวย amino acid ประมาณ 3,000 ตัว แลวถูกตัดแบงโดย host
และ viral proteases เปน 10 สวน ไดแก structural protein 3 สวน คือ core, premembrane และ envelope
และ nonstructural protein อีก 7 สวน คือ NS1, NS2A, 2B, NS3, NS4A, 4B และ NS5 และตัวสาย
Positive-sense RNA ที่สามารถ Translate เปน protein ไดโดยตรงนี ้ก็จะ Transcribe ไปเปนสาย negative-
sense intermediate เพ่ือเปน Template สําหรับการสรางสาย Positive-sense RNA molecule ไปเปน
genome รุนลูกใหมีปริมาณมากๆดวย
www.cueid
.org

Slide 8
Viral Replication and Release
• Newly formed progeny viral RNA interacts with multiple copies of C protein to form nucleocapsid
• Nucleocapsid – bud through ER membrane immature virions exocytosis
หลังจากนั้น viral RNA ทีไ่ด ก็จะ interact กับ C protein เพ่ือ form เปน nucleocapsid แลวยืน่ออกมาจาก
endoplasmic reticulum กอนจะ exocytosis เปนไวรัสตัวใหมตอไป
www.cueid
.org

Slide 9
จากรูป ในภาพท่ี (5) single-stranded positive sense genome ตามรูป (c) ก็จะ translation ไดเปน สาย
amino acid polyprotein ท่ีมี amino acid ประมาณ 3,000 ตัว และถกู process ตอโดย protease ของ host
และ ไวรัสเปน structural protein 3 สวน คือ core, premembrane และ envelope และ nonstructural
protein อีก 7 สวน คือ NS1, NS2A, 2B, NS3, NS4A, 4B และ NS5 ตามในภาพ (d) ตอมา RNA replication
โดย Positive-sense RNA ที่สามารถ Translate เปน protein ไดโดยตรงน้ี ก็จะ Transcribe ไปเปนสาย
negative-sense intermediate เพ่ือเปน Template สําหรับการสรางสาย Positive-sense RNA molecule ไป
เปน genome และสาย Positive-sense RNA ก็จะรวมกยั C protein ดังในภาพ (e) และ form เปน immature
virion โดยการ budding เขาไปใน endoplasmic reticulum ดังในภาพท่ี (7) แลว Vesicle ที่บรรจุ immature
virion ก็จะถูกนําไปยัง surface ของ host cell ในภาพ (8) กอนที่ Premembrane protein จะถูกตัดเพ่ือ
เปล่ียนแปลงไปเปน mature virion ในภาพ (f) แลวก็ถกูปลอยออกไปภายนอก host cell โดย exocytosis ดัง
ในภาพที่ (9)
www.cueid
.org

www.cueid
.org

Slide 10
Dengue Serotypes
• 4 antigenically distinct dengue viruses (dengue-1, -2, -3, and -4)
• Identified by cross-neutralization tests using polyclonal antibodies
• Primary infection – individual’s first infection with any one of the four dengue viruses
• Secondary infection – second infection with a different dengue virus
อยางทีไ่ดกลาวไปแลววาเช้ือไวรัสเด็งก่ี มีท้ังหมด 4 serotype, identify โดย cross-neutralization tests โดย
การใช polyclonal antibodies, Primary infection หมายถึงการติดเชื้อคร้ังแรกโดย serotype ใดก็ได สวน
secondary infection หมายถึง การติดเช้ือคร้ังท่ี 2 โดย serotype ชนิดอ่ืน
www.cueid
.org

Slide 11
Dengue Serotypes
• Infection with one dengue virus lifelong immunity to that virus but does not protect against secondary infection with a different type
• E protein – main determinant of serological cross-reactivity
• Amino acid sequences of E protein from 4 dengue viruses show 62-78% homology
• Dengue-1 and -3 – most closely related, and dengue-4 is the most distant
โดยปกติแลว การติดเช้ือไวรัสเด็งก่ี serotype ใดก็แลวแต จะมีภูมิตานทานตลอดชวีิตตอไวรัสเด็งกี่ชนิดนั้น แต
จะไมสามารถปองกัน secondary infection จาก serotype อ่ืนได โดย E protein เปนตําแหนงทีจ่ะทําใหเกิด
serological cross reactivity ได เนื่องจากลําดับของ amino acid ของ E protein จากทั้ง 4 subtype
เหมือนกนั 62-78%, serotype dengue-1 และ dengue-3 มีความคลายคลึงกันมากที่สุด สวน dengue-4
แตกตางจากชนิดอ่ืนมากที่สุด
www.cueid
.org

Slide 12
Geographical distribution• The most widely mosquito-borne virus of
humans• Occurring in virtually every country between the
tropics of Capricorn and Cancer• DHF – largely confined in southeast Asia until
1980s• Since then – reemerged in Indian subcontinent
and occurred for the first time in China, Tahiti and Cuba, the Caribbean, the Pacific Islands, Venezuela, and Brazil
เช้ือไวรัสเด็งกี่ ปจจุบัน เปนเช้ือที่มีการแพรระบาดมากทีสุ่ดในมนษุย โดยจะพบมากในประเทศโซนรอนระหวาง
เสน Tropics of Cancer และ Tropics of Capricorn แตสําหรับ Dengue hemorrhagic fever จะพบมากใน
แถบเอเชียตะวันออกเฉียงใตจนกระทั่งถึงชวงทศวรรษที ่80 ก็เริ่มพบในแถบทวีปอินเดีย, จีน, ทาฮิติและคิวบา,
คาริบเบียน, หมูเกาะในมหาสมุทรแปซิฟค, เวเนซูเอลา และ ประเทศบราซิล
www.cueid
.org

Slide 13
ภาพนี้เปนภาพการแพรระบาดของเชื้อไวรสัเด็งกี่ทั่วโลก โดยพบมากในประเทศโซนรอน สีเทาแสดงประเทศที่มี
รายงานพบ Dengue fever สวนสีดําเปนประเทศที่มีรายงานพบ Dengue hemorrhagic fever ในชวง 25 ปที่
ผานมา
www.cueid
.org

Slide 14
Geographical distribution
• Estimated 250,000-500,000 cases of DHF globally each year
• The spread of dengue since World War II- worldwide resurgence of Aedes aegypti- poor vector control- overcrowding of refugee and urban populations- increasing human travel
มีการประมาณผูปวย Dengue hemoorhagic fever ทั่วโลกอยูท่ี 250,000-500,000 คนตอป การแพรระบาด
ของ dengue ต้ังแตสงครามโลกคร้ังที่ 2 มีความเกี่ยวของกับการแพรกระจายของยุงลาย Aedes aegypti ทั่ว
โลก เน่ืองจากการควบคุมที่ไมดี มีผูอพยพและประชากรเมืองจํานวนมาก และการทองเที่ยวที่เพ่ิมขึ้น
www.cueid
.org

Slide 15
Natural Cycle• Dengue is primarily a virus of humans.• Transmitted by Aedes mosquitoes, especially
Aedes aegypti• Also exists in a sylvatic (forest) cycle, where
non-human primates are the host (3 subgenus –Stegomyia, Finlaya, and Diceromyia of the genus Aedes)
• For human transmission – Aedes aegypti (subgenus Stegomyia, genus Aedes) is the most important
Natural cycle ของ Dengue virus จะไมเหมือน arbovirus ชนิดอ่ืนที่เปน zoonotic หรือ animal cycle และ
human infection เปน coincidental โดย dengue virus เปนเช้ือที่แพรกระจายในคน และtransmit ผานทาง
ยุง Aedes โดยเฉพาะ Aedes aegypti แตก็สามารถเปน sylvatic หรือ forest cycle โดยไมมีคนเปน host ก็ได
โดยพบรายงานใน 3 subgenera คือ Stegomyia, Finlaya, และ Diceromyia ใน genus Aedes อยางไรก็ตาม
สําหรับการแพรระบาดในคน Aedes aegypti subgenus Stegomyia, genus Aedes สําคัญที่สุด
www.cueid
.org
Slide 16
Dengue Vectors
• Aedes aegypti – “domestic” mosquito• Anthrophilic (i.e, feeds on humans)• Breeds in peridomestic collections of clean water
(storage jars, containers etc.)• Only female seek blood meals• Infected mosquito remains infectious for its
entire life• Transovarial transmission (mosquito its eggs)
has been documented
Aedes aegypti เปนยุงบานทีก่ินเลือดคนโดยเกิดเฉพาะในตัวเมีย และผสมพันธุในน้าํขังที่เปนน้าํสะอาด ยุงที่
ไดรับเช้ือเขาไป ก็จะเปนพาหะไดตลอดอายขุัยของมัน มีรายงานการแพรเช้ือผานทาง transovarial
transmission คือจากยุงไปยังไขไดเชนกนั
www.cueid
.org

Slide 17
Dengue Vectors
• Aedes aegypti eggs – survive for long periods in dry conditions spontaneous dengue outbreaks
• Aedes albopictus – better survival at cooler temperatures major European outbreak
• Other species- Aedes scutellaris hebrideus in New Guinea - Aedes polynesiensis in Tahiti- Aedes cooki in Niue
ไขของยุง Aedes aegypti สามารถมีชีวิตอยูไดนานในสถานที่ทีแ่หง จึงเปนเหตุผลของการเกิด spontaneous
dengue outbreaks สําหรับยุงชนิดอ่ืนที่สามารถเปนพาหะแพรเช้ือไดเชน Aedes albopictus ซึ่งทนตอสภาพ
ภูมิอากาศเย็นไดดีกวา จึงมักทําใหเกิด การแพรระบาดในยุโรป เช้ืออ่ืนๆ เชน Aedes scutellaris hebrideus,
Aedes polynesiensis, และ Aedes cooki
www.cueid
.org

Slide 18
History
• The name dengue – derive from a Swahili term to describe a dengue-like illness on the east coast of Africa in the mid-19th century
Ki-Dinga pepo, “a disease characterized by a sudden cramp-like seizure, caused by an evil spirit”
• Shortened to “denga” or “dyenga” and is thought to have become “dengue” as a Spanish derivative of the African term when the slave trade brought the disease to the West Indies
ประวัติความเปนมา ช่ือ dengue มาจาก Swahili term เพ่ือที่จะบรรยาย dengue-like illness บนชายฝง
ตะวันออกของทวีป Africa ในชวงกลางศตวรรษท่ี 19 โดยใชช่ือวา Ki-Dinga pepo มีความหมายวา โรคที่มี
อาการ sudden cramp-like seizure มีสาเหตุจากภูตผีวญิญาณ ตอมาคําก็ส้ันลงเปน denga หรือ dyenga
จนแผลงเปน dengue
www.cueid
.org

Slide 19
The Emergence of Dengue Hemorrhagic Fever
• In the1950s – outbreaks of an apparently new hemorrhagic fever occurred in Philippines and Thailand caused by dengue viruses
• Following further massive epidemics of DHF in Thailand
• WHO adopted clinical and laboratory criteria for diagnosing and treating dengue fever and DHF
ดานประวัติของการเกิด Dengue hemorrhagic fever เร่ิมจากในทศวรรษที่ 50 เกิดการระบาดของโรค
hemorrhagic fever ชนิดใหมขึน้ที่ประเทศฟลิปปนสและประเทศไทย ซ่ึงพบสาเหตุการเกิดโรคเปน dengue
virus หลังจากนัน้ก็เกิดการระบาดคร้ังใหญช้ึนท่ีประเทศไทย แลว องคการอนามัยโลกก็ไดต้ัง clinical และ lab
criteria สําหรับวินิจฉัยและรักษา dengue fever และ dengue hemorrhagic fever
www.cueid
.org

Slide 20
The Dengue Encephalopathy Controversy
• SEAMEO-TROPMED in Bangkok in 1976- 3 separate presentations from Thailand, Burma, and Indonesia attention to neurological manifestations of dengue
• It gradually became accepted that patients with severe DHF could develop encephalopathy secondary to the many complications of severe disease
Dengue encephalopathy เร่ิมมีการพูดถึง severe manifestation ของ dengue viral infection วานาจะ
เกี่ยวของกับโรคทางระบบประสาท โดยในการประชุม SEAMEO-TROPMED ที่กรุงเทพ ป 1976 ไดมีตัวแทน
จากประเทศไทย พมา และ อินโดนีเซีย กลาวถึง neurological manifestation ของ dengue หลังจากนั้นก็เร่ิม
มีการยอมรับวา ผูปวย severe dengue hemorrhagic fever สามารถเกิด encephalopathy ไดโดยเปนผล
จากหลายๆ complication ของตัวโรค
www.cueid
.org

Slide 21
The Dengue Encephalopathy Controversy
• These included- Hepatic dysfunction (sometimes as part of a Reye’s-like syndrome)
- Hyponatremia- Hypoxia- Cerebral edema or hemorrhage
• But whether dengue viruses could cross the BBB to cause a true viral encephalitis was not certain
Complication เหลานี้เชน Hepatic dysfunction, hyponatremia, hypoxia, cerebral edema หรือ cerebral
hemorrhage แต dengue virus นี้ จะสามารถผาน blood brain barrier ไปทาํใหเกดิ viral encephalitis ได
หรือไมนั้น กย็งัไมเปนทีแ่นชัด
www.cueid
.org

Slide 22
The Dengue Encephalopathy Controversy
• Controversy ?- Definition of encephalopathy and encephalitis were vague.
- capabilities for precisely diagnosing dengue infection and excluding other potential causes of CNS disease were variable.
สาเหตุสวนหนึ่งท่ียังเปนที่ถกเถียงกันอยูถงึแมจะมหีลายการศึกษา รวมทั้ง case reports หรือ retrospective
case series ออกมามากมาย อาจเปนเพราะ definition ของ encephalopathy และ encephalitis นั้นไม
ชัดเจน รวมทั้งความสามารถที่จะวินิจฉัย dengue infection ใหแมนยาํ และ exclude สาเหตุอ่ืนของ Central
nervous system นั้นยังไมเหมือนกันในแตละสถาบนั
www.cueid
.org

Slide 23
Epidemiology of Neurological Dengue
• Neurological manifestations of dengue infection have been described in almost all areas where dengue occurs.
• Many of the more recent epidemiological and clinical studies have come from Asia.
Epidemiology of neurological dengue – ไดมีรายงานเกี่ยวกับ neurological manifestation ของ dengue
infection เกือบทุก area ท่ีมกีารระบาดของเชื้อ dengue แตรายงานและ clinical studies สวนใหญมาจาก
ทวีปเอเชีย
www.cueid
.org

Slide 24
ตารางนี้สรุปรวมผลการวิจัยเกี่ยวกับระบาดวิทยาของ neurological dengue โดยมทีั้งการศึกษาโดยการหา
neurological manifestation ในผูปวยที่เปน dengue fever หรือ dengue hemorrhagic fever และ การศึกษา
หาผูปวย dengue infection ในผูปวยทีม่า present ดวย CNS disease ในแบบแรกมีหลายการวิจยัที่เกี่ยวของ
รวมทั้งของอ.จุล และอ.อุษา ทิสยากรทีทํ่าที่กรุงเทพ ในป 1987 และ ทําที่ กรุงเทพ และ สงขลา ในป 1987-
1994 โดยพบผูปวย neurological dengue 2.4% และ 1% ตามลําดับ
www.cueid
.org
Slide 25
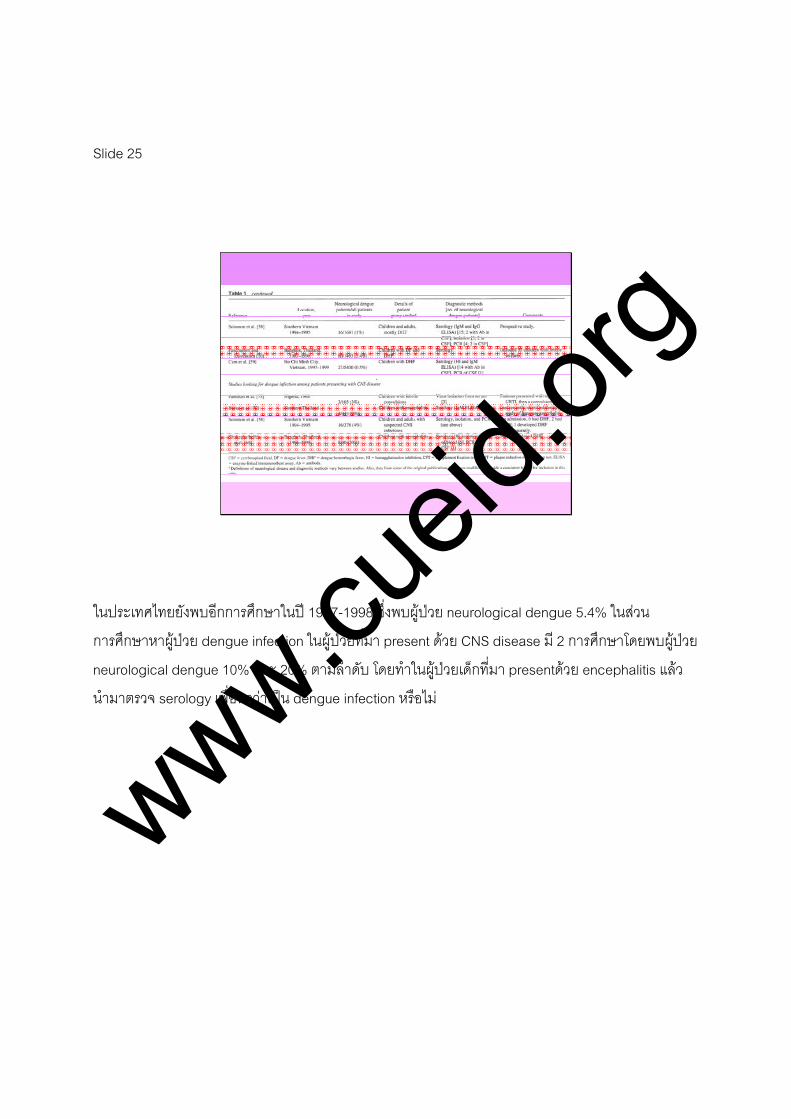
ในประเทศไทยยังพบอีกการศึกษาในป 1987-1998 ซ่ึงพบผูปวย neurological dengue 5.4% ในสวน
การศึกษาหาผูปวย dengue infection ในผูปวยที่มา present ดวย CNS disease มี 2 การศึกษาโดยพบผูปวย
neurological dengue 10% และ 20% ตามลําดับ โดยทาํในผูปวยเด็กที่มา presentดวย encephalitis แลว
นํามาตรวจ serology เพ่ือหาวาเปน dengue infection หรือไม
www.cueid
.org

Slide 26
Dengue Virus Types
• All 4 dengue viruses – associated with neurological dengue (dengue-2 and -3 most frequently)
• In Indian study – dengue-2 was most frequently isolated.
• In Thailand – dengue-1, -2, and -3 viruses were detected in equal numbers
• In Vietnam - dengue-3 in 5 patients- dengue-2 in 4 patients- dengue-1 in 1 patient
หากจะมาดู Type of dengue virus ที่ associate กับ Neurological dengue พบวา ท้ัง 4 type สามารถทาํให
เกิดไดท้ังหมด แตพบมากใน dengue-2 และ dengue-3 โดยในประเทศอินเดีย มีรายงานพบบอยใน dengue-
2 ในประเทศไทย พบใน dengue-1, dengue-2 และ dengue-3 เทาๆกนั สวนในประเทศเวียดนาม มีรายงาน
พบ dengue-3 5 คน dengue-2 4 คน และ dengue-1 1 คน
www.cueid
.org

Slide 27
Dengue Virus Types
• In Indonesia - high incidence of neurological dengue- dengue-3 was most frequently isolated
• No data that compare the frequency of dengue-3 virus isolation in neurological cases with the frequency in non-neurological cases
ในประเทศอินโดนีเซีย พบ high incidence ของ neurological dengue โดยพนเปน dengue-3 มากที่สุด แต
หากตองการจะดูความสัมพันธกับ neurological disease จําเปนตองเปรียบเทียบความถี่ของ dengue-3 ใน
ผูปวย neurological case เทียบกับความถ่ีในผูปวย non-neurological case ซ่ึงพบวา ไมมีการศึกษาลักษณะ
นี้ออกมา โดยมีเพียงการศึกษาบางการศึกษาท่ีแสดงใหเห็นวา dengue-3 อาจจะมคีวามสัมพันธกับปจจัยเส่ียง
ในการเกิด neurological disease
www.cueid
.org

Slide 28
Other Risk Factors for Neurological Dengue
• Young children and adults appear to be at greater risk of neurological disease than older children
• Severe DHF (gr III, IV – dengue shock syndrome)• Primary infection - associated with
- convulsions (especially in younger children)- peripheral neuropathies (especially in adults)
• Secondary infection – associated with- encephalopathic DHF
สวนปจจัยเส่ียงอ่ืนๆสําหรับ neurological dengue ไดแก 1.ผูปวยเด็กเล็ก และ ผูใหญ โดยพบวามีปจจัยเส่ียง
มากกวาเด็กโต 2. severe dengue hemorrhagic fever grade III, IV หรือ dengue shock syndrome 3.
primary infection โดยจะ associate กับ convulsion โดยเฉพาะในเด็กเล็ก และ associate กับ peripheral
neuropathies โดยเฉพาะในผูใหญ 4. secondary infection associate กับ encephalopathic dengue
hemorrhagic fever
www.cueid
.org

Slide 29
Pathophysiology of DHF
Pathophysiology of dengue hemorrhagic fever
www.cueid
.org

Slide 30
Antibody-Dependent Enhancement
• DHF is characterized by - increased permeability of blood vessels- hemorrhagic manifestations- thrombocytopenia
• Although DHF can occur in a primary infection, epidemiological evidence more likely in secondary infection with a different virus
Antibody-dependent enhancement
Dengue hemorrhagic fever มีลักษณะคือ increased permeability of blood vessels, hemorrhagic
manifestations และ thrombocytopenia แมวา dengue hemorrhagic fever สามารถเกิดไดใน primary
infection แตจากขอมูลทางระบาดวทิยาพบวามกัเกิดใน secondary infection จากเช้ือที่ตางชนิดกับคร้ังแรก
มากกวา
www.cueid
.org

Slide 31
จากสมมติฐานเกี่ยวกับ antibody-dependent enhancement ใน pathogenesis ของ dengue hemorrhagic
fever กราฟมุมซายบนแสดงใหเห็นถึง antibody level หลังจาก first dengue viral infection ถาเกิด early
infection โดยเช้ือท่ีมี serotype ตางจากชนิดแรก ระดับ IgG level ก็จะยังคงสูงเพียงพอที่จะเกิด cross-
reactive IgG antibody เพ่ือที่จะ neutralize second infection แตถา second infection เกิดขึ้นหางจากคร้ัง
แรกมาก neutralizing IgG antibodies ที่จะจับกับ critical epitopes ลดลง แต IgG antibodies ตอ
noncritical sites ทําใหเช้ือไวรัสไมตาย เกิดเปน viable virus-antibody complexes หลังจากนัน้ IgG ก็จะใช
สวน Fcγ portion เพ่ือจับกับ Fcγ receptors ทําใหเชื้อสามารถเขาสู monocyte ไดมากขึ้น ซ่ึงก็เปนการทําให
เกิด viral replication เพ่ิมขึ้น เรียก IgG ทีจั่บกับเช้ือไวรัสแลวทําใหเช้ือสามารถเขาสู cell ไดมากขึ้นนี้วา
enhancing antibody หลังจากเกิด viral replication เขาสูกระแสเลือดแลว ก็จะกระตุน T-cell immune
response เปนผลใหเกิด Cytokines, complement and platelet activation สงผลใหเพ่ิม vascular
permeability และ vascular leakage ในทีสุ่ด
www.cueid
.org

www.cueid
.org

Slide 32
Antibody-Dependent Enhancement
• Risk factor for DHF- circulating antibodies from previous dengue infection with a different virus type
- passively acquired maternal IgG
ดังนั้น ปจจัยเส่ียงสําหรับ dengue hemorrhagic fever ไดแก การมี circulating antibodies จากการติดเชื้อ
คร้ังกอนท่ีตางชนิดกัน และ การไดรับ IgG จากมารดา
www.cueid
.org

Slide 33
Strain Determinants
• Specific dengue virus types and the order of infection may also be important
• Data from Thailand and Cuba – most primary infections with dengue-2 and -4 asymptomatic
• In Rayong, Thailand, sequential infection with dengue-1 and then dengue-2 more likely to lead to dengue shock syndrome than other combinations
มีหลักฐานยืนยันถึงความสําคัญของ dengue virus type วาเปน strain ไหน รวมถึงลําดับของการติดเช้ือ วามี
ผลตอความรุนแรงของโรค โดยมีรายงานในประเทศไทยและคิวบาวา ถาติดเช้ือ primary infection ดวย
dengue-2 และ dengue-4 มักจะไมมีอาการ สวนรายงานจากจังหวัดระยอง พบวา หากติดเช้ือ dengue-1
ตามดวย dengue-2 มักจะทําใหเกิด dengue shock syndrome มากกวาการจับคูแบบอื่น
www.cueid
.org
Slide 34
Genetic Susceptibility
• DHF – more common in southeast Asia than in Africa and America
• This may because of - greater intensity with which the 4 serotypes of dengue viruses circulate in southeast Asia
- differences in genetic susceptibility• Recently HLA halotypes associated with
susceptibility to DHF were identified in Vietnamese and Thai children
Genetic susceptibility
การที่พบ dengue hemorrhagic fever มากในภูมิภาคเอเชียตะวันออกเฉียงใต มากกวาใน Africa และ
America อาจเปนเพราะ มีเชื้อทั้ง 4 serotype อยูในเอเชียตะวันออกเฉียงใต หรืออาจเกิดจากพันธุกรรมที่มี
สวนเกี่ยงของ โดยมีรายงานพบ HLA halotypes ที่ associate กับการเกิด dengue hemorrhagic fever ใน
ชาวเวียดนาม และเด็กไทย จึงเช่ือวา genetic นาจะมีสวนสําคัญในการเกิดโรค
www.cueid
.org

Slide 35
Pathophysiology of Neurological Complications
• Controversy• Range of complications of severe DHF reduced
consciousness in some patients- hepatic dysfunction (may be part of a Reye’s- like syndrome)
- hyponatremia - renal failure- metabolic acidosis - DIC- intracranial hemorrhage (frank or microvascular)- raised intracranial pressure - hypoxia
Pathophysiology of Neurological Complications
ยังคงเปนท่ีถกเถียงกันอยูเร่ือง neurological complication โดย range ของ complication ใน severe
dengue hemorrhagic fever อาจเปนผลมาจาก hepatic dysfunction, hyponatremia, renal failure,
metabolic acidosis, DIC, intracranial hemorrhage, increased intracranial pressure, และ hypoxia
www.cueid
.org

Slide 36
Pathophysiology of Neurological Complications
• However, if not appear to have any of these complications evidence on occasion dengue virus crosses BBB to enter the CNS and cause encephalitis
อยางไรก็ตาม ถาไมพบวามี complication เหลานี้ ก็มีรายงานวาอาจเกิดจาก dengue virus สามารถผาน
blood brain barrier เขา CNS ทําใหเกิด encephalitis ได
www.cueid
.org

Slide 37
Viral Invasion Across the Blood-Brain Barrier and Encephalitis
• Encephalitis – pathological Dx autopsy or brain Bx
• Recent histopathological evidence occasionally associated with inflammation and other changes at autopsy
• It was suggest that CD68+ macrophages might carry dengue viruses across BBB in a “Trojan horse” machanism and that neurons might be injured by contact with these dengue-infected macrophages
Encephalitis เปน pathological diagnosis โดย autopsy หรือ brain biopsy โดยมี evidence ของ
histopathological evidence วา dengue infection อาจ associate กับ inflammation และ การเปลี่ยนแปลง
อ่ืนๆที่พบใน autopsy มีรายงานวา CD68+ macrophage เปนตัวพา dengue viruses ผาน blood brain
barrier เขา CNS ได โดยลักษณะเดียวกับ Trojan horse หรือมาแหงกรุงทรอย คือ การเกิด second infection
มี enhance antibody ทําใหเช้ือไวรัสสามารถเขาสู macrophage มากขึ้น แลวเปนตัวพาเขาสู CNS
www.cueid
.org

Slide 38
Viral Invasion Across the Blood-Brain Barrier and Encephalitis
• Proof of a viral CNS infection- immunohistochemical proof- virus isolation from CSF- Ab detection in the CSF
in the context of an appropriate clinical picture, is a more appropriate gold standard than a histopathological description of an inflammatory response that can be seen only at autopsy or on brain Bx
การที่จะพิสูจน Viral CNS infection อาจทําไดโดย immunohistochemical proof, virus isolation จาก CSF,
และ Antibody detection ใน CSF โดยอาจถือเปน gold standard มากกวาที่จะใช histopathology จาก
autopsy หรือ brain biopsy
www.cueid
.org

Slide 39
Dengue Neuropathies and Myelopathy
• Nerve conduction studies – decreased motor conduction velocity demyelinating process
• Cause is uncertain, though deposition of immune complexes has also been suggested
Dengue virus สามารถทําใหเกิด Dengue Neuropathies และ Myelopathy ได จาก Nerve conduction
studies จะพบ decreased motor conduction velocity ซ่ึงเปน demyelinating process โดยสาเหตุยังไม
เปนที่แนชัด แมวามกีารอางวาอาจเกิดจาก deposition ของ immune complexes
www.cueid
.org

Slide 40
Raised ICP & Herniation• Fluid management: difficult• Conflict: shock resuscitation & cerebral edema• Restore BP and perfusion : 1st priority• Prefer isotonic crystalloid or hypertonic colloid• If no shock: fluid maintainance = 2/3 of normal• ↑ ICP ↓ level of consciousness, s/s of herniat
20% mannitol (0.5-1.0g/kg) is givenRole of steroids : not been assessed
www.cueid
.org

Slide 41
Other measures• Suspected bacterial meningitis broad
spectrum ABO should be given• Hypoglycemia common in many tropical
pediatric conditions• Adequate nutrition• Avoid complications of severe encephalopathy:
pneumonia, UTI, bedsores and contractures
www.cueid
.org
Slide 42
Prevention of Dengue• No commercial available vaccine • Surveillance for dengue, mosquito activity &
control vectors• Personal protection with insect repellents
containing N,N-diethyl-m-toluamide (DEET)efficacy is variable
www.cueid
.org

Slide 43
Dengue Vaccines• Development of vaccine against dengue has
been hampered• Tetravalent dengue vaccine• Life-attenuated vaccine: phase I & II in Thailand
and US.• Recombinant dengue vaccine: being developed• Fully incorporated into expanded program• Vector control remain our only defense against
dengue commitment, education & community participation
www.cueid
.org

Slide 44
Clinical features
www.cueid
.org

Slide 45
Outlines• Dengue Fever• Dengue Hemorrhagic Fever• Classification of Neurological Dengue• Cerebral Dengue• Neurological manifestation of Dengue Infection• Diagnosis and Management
โดยหวัขอที่จะบรรยายจะแบงเปนเร่ืองหลักไดทั้งหมด 6 เร่ือง ดังนี้ คือ ไขเดงกี ไขเลือดออกเดงกี การจําแนก
ประเภทโรคทางระบบประสาทที่เกี่ยวของกับการติดเชื้อเดงกี ภาวะเซเรบรอล เดงกี
อาการและอาการแสดงทางระบบประสาทท่ีเกิดจากการติดเช้ือเดงกี รวมทั้งการวินจิฉัยและการรักษา
www.cueid
.org

Slide 46
Dengue fever• Incubation period 4-7 days• Undifferentiated febrile illness in young children• 30% of diagnosed URI in BKK virus isolation
or serology have acute dengue infection• Older child fever-arthralgia-rash syndrome• Tourniquet test : traditionally recommended• Lymphadenop, leukopenia & thrombocytop =
common
สําหรับ DF จะมีอาการภายหลังจากระยะฟกตัวประมาณ 4-7 วัน โดยในเด็กเล็กมักจะมาพบแพทยดวย
อาการไขไมทราบสาเหตุ จากการสํารวจพบวาเด็กในกรุงเทพมหานครที่มาพบแพทยที่คลินกิผูปวยนอกดวย
อาการติดเชื้อทางเดินหายใจสวนบนมีจํานวนกวารอยละ 30 ที่พบวามีการติดเช้ือไวรัสเดงกีชนิดเฉียบพลัน
สวนในเด็กโตมักจะมีอาการไข ปวดขอและมีผ่ืน ซ่ึงจะกลาวตอไปในรายละเอียด นอกจากนี้มักจะตรวจพบวา
มีเม็ดเลือดขาวและเกล็ดเลือดตํ่า รวมทั้งพบวามีตอมน้าํเหลืองโตได การทํา Tourniquet test ควรทําเพ่ือชวย
confirm clinical diagnosis ในกรณีที่ผลตรวจเปนบวก
www.cu
eid.or
g

Slide 47
Dengue fever• Clinical findings not very helpful in distingushing
DF from other febrile illnessDDx: Measles
MalariaChikungunyaTyphoidLeptospirosis
laboratory confirmation is needed
เน่ืองจากลักษณะทางคลินกิเพียงอยางเดียวไมเพียงพอที่จะแยก dengue fever ออกจากไขเฉียบพลันที่มี
สาเหตุมาจากโรคอ่ืน จึงจําเปนตองใชการตรวจปฏิบัติการเพ่ือชวยยินยันและวางแผนการรักษา
www.cueid
.org

Slide 48
Fever-arthralgia-rash syndrome
• Fever: high grade with anorexia, nausea vomiting and abdominal pain
Arthralgia: muscle and joint ache retro-orbital pain
Skin eruption: occur in 50% of pt.mottling flushing and MP rashbleeding diathesis
อาการไขมักเปนไขสูง ตัวรอน รวมกับอาการที่เดน คือ คล่ืนไสอาเจียนและปวดทอง มีอาการปวดขอ ปวด
ตามกลามเนื้อ ปวดเบาตาและปวดกระดูก และพบรวมกับอาการแสดงทางผิวหนงัไดประมาณรอยละ 50
www.cueid
.org

Slide 49
Tourniquet test• Measure of capillary fragility• Inflated BP cuff half between SBP & DBP
duration 5 min• Positive test: ≥ 20 in a 2.5 cm square• Recent study in Vietnam & Thailand =
Highly specific but low sensitivity
การทาํ Tourniquet test เปนการทดสอบความเปราะบางของเสนเลือดแดงฝอย โดยมีวิธกีารดังนี ้คือ วัดความ
ดันโลหิตดวย manual sphygmomanometer ตามปกติ เมื่อไดคา systolic blood pressure
และ diastolic blood pressure แลว นํามาบวกกันแลวหารดวยสอง ผลลัพธท่ีไดจะใชเปน pressure ท่ีจะรัด
แขนของผูปวย โดยระยะเวลาที่ใชวัดประมาณ 5 นาที การอานคาจะดูที่ทองแขนในระดับที่ตํ่ากวาขอบลาง
ของ cuff ที่ใชวัด โดยนับจุดเลือดออกพีทีเคียใน 1 ตารางนิ้ว ถานับไดมากกวาหรือเทากับ 20 จุดใน 1
ตารางนิ้ว ถือวาการทดสอบใหผลบวก แตการแปลผลตองทําดวยความระมัดระวัง เพราะจากการศึกษา
ผูปวยไขเลือดออกท้ังในประเทศไทยและเวยีดนามเมื่อไมนานมานี้พบวาการทํา tourniquet test มี
ความจําเพาะตอไขเดงกีสูงแตความไวตํ่าถาจะใชตรวจหาการติดเช้ือไขเดงกี
www.cueid
.org

Slide 50
DHF• Major pathophysiological process in DHF
↑ vascular permeabilityPlasma leakage from blood vessels
Clinical manifestationsThrombocytopeniaHemorrhagic manifestationLeukopenia, atypical lymphocyteMild DIC with prolong PTT, TTFibrinogen & complement depletion
ในสวนของไขเลือดออกเดงกี พบวาพยาธสิรีรวิทยาของการเกิดโรคคือ มีการเพ่ิมขึ้นของความสามารถในการ
ซึมผานของหลอดเลือด ทําใหมีการร่ัวของ plasma ออกมานอกหลอดเลือด เปนผลทําใหเกิดอาการและ
อาการแสดงเหลานี้ตามมา เกล็ดเลือดตํ่า มีเลือดออกผิดปกติ เม็ดเลือดขาวลมิโฟซัยตํ่า พบเม็ดเลือดขาว
ชนิด atypical lymphocyte เพ่ิมสูงมากขึ้น และมีแนวโนมที่จะเกิด อาจตรวจพบคา PT, PTT จะนานมากขึน้
และมีการลดลงของ fibrinogen และ complement
www.cueid
.org

Slide 51
Classification of neurological Dengue
• Gubler et al: described 3 forms of disorder
• Acute Phase of Illness:HeadacheDizzinessDeliriumSleeplessness RestlessnessMental irritability
กั๊บเลอรและคณะไดจําแนกอาการและอาการแสดงทางระบประสาทในผูปวยไขเดงกีไว สามประเภทดังนี้ คือ
ระยะแรก
www.cueid
.org

Slide 52
Classification of neurological Dengue
Severe neurological manifestations:Depressed sensoriumLethargyConfusion SeizureMeningismParesis Coma
www.cueid
.org

Slide 53
Classification of neurological Dengue
• Post infectious or parainfectious disorderDelayed symptoms includingsParalysis of upper/lower extremities + larynxEpilepsy DementiaTremor Guillain-Barre’ syndrome AmnesiaLoss of sensationManic psychosisDepression
www.cueid
.org
Slide 54
Controversy• Headache, dizziness and lethargy can not be
considered evidence of neurological disease• Many of the terms such as delirium, confusion
and depressed sensorium are ill-defined• Classification without any supporting evidence
ซ่ึงการจําแนกดังกลาวอาจทาํใหเกิดความสับสนไดในหลายประเด็น เชน
www.cueid
.org

Slide 55
Prospective clinical studies in Vietnam
• Clear definitionEncephalopathy = ↓Glasglow or Blantyre
pediatric coma scoreEncephalitis = Encephalopathy which on
metabolic or other cause could be found plus at least 1 feature suggestive of focal brain inflammation
CSF pleocytosis Focal neurological signsConvulsions
จากการทาํการศึกษาแบบ prospective ในประเทศเวียดนาม ไดใหคําจํากัดความของ term ตางตาง ดังนี้
เอนเซฟาโลพาที นยิาม คือ การลดลงของกลาสโกลว หรือ บลองไทร พีดีเอทริก โคมา สกอร
เอนเซฟาไลทิส นิยาม คือ ภาวะเอนเซฟาโลพาที ลักษณะที่บงบอกวามีการอักเสบเฉพาะท่ีของเนื้อสมองอยาง
ใดอยางหนึ่งตอไปน้ี คือ
การที่มีเซลในนํ้าไขสันหลังเพ่ิมสูงขึ้น
มีอาการหรืออาการแสดงของอาการทางระบบประสาทเฉพสะท่ี
มีอาการชัก
www.cueid
.org

Slide 56
Cerebral Dengue• New Classification of neurological dengue• Not presume encephalitis until pathology prove• First classified by neurological features• Including DF DHF and systemic complication of Dengue
infection• Cerebral Dengue
acute dengue infection + comano other obvious explanation for the coma
Dengue encephalitisPathologically proven encephalitis
www.cueid
.org

Slide 57
Classification of Neurological Dengue
ASSESSA. Laboratory evidence of acute dengue infection in the serum
or CSF, by Detection of virus by isolation or PCR, orDetection of Ab by IgM ELISA or 4 fold rising in HI or other serological test
1.If virus or Ab is detected in the CSF (in the absence of traumatic LP ) this is defined as a CNS dengue infection, as is immuno histochemical or nucleic acid hybridization evidence of Dengue virus in brain tissue obtained from biopsy or autopsy
2.Other microbiological, toxic, or metabolic causes of neurological disease must be excluded
www.cueid
.org

Slide 58
• B. Level of consciousness1.Encephalopathy ( a reduced level of consciousness )
a. Encephalopathy is defined as coma score that is at least1 less than normal
Glasglow coma scale or Adelaide pediatric coma of < 15 orb. As a quick assessment, any patient who is disoriented in time,
space and person (or for children under 5, fail to recognize a parent) is encephalopathic
c. Patients with a reduced level of consciousness following a convulsion, except for those with a single simple febrile convulsion, defines as followsSimple febrile convulsion: Children between 6mo-5yr of age
with a single convulsion lasting less than 15 min who recover consciousness within 60 min2.Coma a. Glasgow coma score < 11
b. Blantyre coma score < 4c. As a quick assessment, any patient who fails to
localized a painful stimmulus
www.cueid
.org

Slide 59
• C. Systemic consequences of dengue infection
DHFHemorrhagic diseaseVascular leakAcute hepatic dysfunctionHyponatremia < 120 ml/LHypoglycemia Blood sugar level <2.2mmol/L
www.cueid
.org

Slide 60
Other Neurological manifestations
• Dengue meningism/meningitis• Neuropathy
อาการแสดงทางระบบประสาทอ่ืนอ่ืนของไขเดงกี ซ่ึงเปนรายงาน case
www.cueid
.org

Slide 61
Neurological manifestation of Dengue infection
• Reduced Level of consciousness• Peripheral neuropathies & Myelopathies• Psychiatric illness• Outcome of Neurological complications• Radiological & Neurophysiological findings• Cerebrospinal fluid
อาการและอาการแสดงทางระบบประสาทในผูปวยที่ติดเช้ือเดงกี สามารถแบงประเภทไดเปน
การลดลงของระดับความรูสึกตัว
พยาธิสภาพของระบบประสาทสวนปลายและกลามเนื้อ
การเจ็บปวยทางระบบจิตประสาท
ผลกระทบจากภาวะแทรกซอนทางระบบประสาท
ลักษณะทางรังสีและประสาทสรีรวทิยา
การตรวจวิเคราะหน้ําในโพรงไขสันหลัง
www.cueid
.org

Slide 62
Reduced level of consciousness
• Most common neurological manifestation• 55-100% of patient series• Range from lethargy, drowsiness and irritability
to deep coma• Convulsion common in young children
Simple febrile convulsion orAssociated with prolonged coma
Pyramidal or long tract signs also occur
การลดลงของระดับความรูสึกตัว
เปนภาวะที่พบไดบอยที่สุด โดยพบตั้งแตทําอะไรเชื่องชา เพลีบเพลียไปจนถึง โคมา
อาจพบอาการชักซ่ึงอาจเกิดจากไขสูงในเด็กหรือการที่มีโคมาอยูนาน รวมทั้งอาจพบ pyramidal หรือ long
tract signs อ่ืนอ่ืน
www.cueid
.org

Slide 63
Reduced level of consciousness
• Extrapyramidal tremors & tone abnormalitycharacterize other arboviral encephalitides but less common in dengue
• Acute disseminated encephalomyelitis• Meningism is up to 30% of patients• Simple viral meningitis due to dengue = rare
การพบ Extrapyramidal tremors & tone abnormality เปนส่ิงท่ีพบไดไมบอยนัก
www.cueid
.org

Slide 64
Reduced level of consciousness
Classified in 2 group• 1.Occur after DHF• 2.Present with neurological disease and no
obvious signs of dengueIndistinguishable from other viral enceph.Most importance DDx = JE2-3 days of non-specific febrile illnessFollow by confusion and coma
JE : rural area DHF: urban area
การลดลงของระดับความรูสึกตัว แบงเปน สองกลุม คือ
www.cueid
.org

Slide 65
Peripheral neuropathty and myopathies
• Mono and polyneuropathies ( involve cranial nerve and & peripheral nerves )
• Describe in adult rather children• Asso.with DF, rather than DHF
1919 – 2 pts.in Honolulu1940 – 13 service personnel in Central Pacific2 pts.develop acute polyneuropathy 1 week after onset of dengue
อาการพยาธิสภาพที่ปลายประสาทและอาการกลามเนื้อ
อาการพยาธิสภาพที่ปลายประสาทเกิดไดทั้งแบบเดี่ยวและหลายหลายปลายประสาท มักพบในผูใหญ
สัมพันธกับไขเดงกีมากกวาไขเลือดออกเดงกี มีรายงานผูปวยในฮาวายและประเทศในแถบ central pacific
www.cueid
.org

Slide 66
Peripheral neuropathty and myopathies
• Nerve conduction studies : ↓ motor velocities• Acute infectious polyneuritisSpinal cord dysfunction
Primary vs SecondarySpecific damage of anterior horn cellsOccurs in many other arboviral CNS infection
พยาธิสภาพของปลายประสาทและกลามเนื้ออักเสบ
การทดสอบการนํากระแสไฟฟาของเสนประสาท พบวามกีารลดลงของมอเตอรเวโลซิต้ี
อาจใหอาการและอาการแสดงในลักษณะของการอักเสบของปลายประสาทหลายหลายเสนที่เกิดจากการติด
เช้ือเฉียบพลัน
อาจพบการทํางานของไขสันหลังที่ผิดปรกติไป โดยอาจเกิดจากตัวเช้ือโรคเองหรือภาวะแทรกซอนที่ตามมา
โดยมักจะเลือกทําลายที่ anterior horn cell ซึ่งพบไดในการติดเช้ืออาโบไวรัสในระบบประสาทสวนกลาง
www.cu
eid.or
g

Slide 67
Psychiatric ill ness
• Depression & Lethargy common feature in recovered from DF
• Manic psychosis & amnesia, dementia Occasional case reports
อาการทางจิตประสาท
อาการเซ่ืองซึมเปนอาการที่พบไดบอยในระยะหลังจากทีห่ายปวย
อาการจิตเภท หลงลืมหรือความจาํเส่ือมพบเปนรายงานผูปวย
www.cueid
.org
Slide 68
Outcome of Neurological Complications
• Range of fatality rate 0-56%, median 10%• Most on severe DHF ( severe shock &
hemorrhage )• Reports of MR directly related to neurological
disease relatively rare• Direct comparison between studies is difficult
ผลตามมาจากภาวะแทรกซอนทางระบบประสาท
อัตราตายในผูปวยที่มีภาวะแทรกซอนทางระบบประสาทมีรายงานไวคอนขางท่ีจะหลากหลาย ต้ังแต ศูนยถึง
หาสิบหกเปอรเซนต โดยมีคากลางอยูที่ สิบเปอรเซนต
โดยผูปวยท่ีเสียชีวิตสวนใหญมักจะมีภาวะชอคหรือเสียเลือดที่รุนแรง รายงานอัตราตายที่สัมพันธกับ
ภาวะแทรกซอนทางระบบประสาทโดยตรงมีนอยมาก และ
การที่จะนาํเอาผลของแตละการศึกษามาเปรียบเทียบกนัเปนเร่ืองที่ทําไดยาก
www.cu
eid.or
g
Slide 69
Report cases
• Sequellae of patients with dengue encephalopathy
HemiparesisSpastic hemiparesisTetraparesisAlteration in personalityEpilepsy
รายงานผูปวย แสดงถึงผลกระทบท่ีเกิดตามหลังจาก dengue encephalopathy มีดังน้ี คือ
มีอาการออนแรงของรางกายครึ่งซีก
มีอาการเกร็งแขนขาคร่ึงซีก
มีอาการออนแรงของแขนและขาท้ังสองขาง
มีพฤติกรรมท่ีเปล่ียนแปลงไป
มีอาการกลายเปนโรคลมชัก
www.cu
eid.or
g

Slide 70
Investigations• Radiological Findings
CT scan of encephalopathic dengueTypical: Diffuse brain swellingReport:
Frank ICHAbnormality of thalamus, basal ganglia, brain stem and cerebellum
เคร่ืองมือที่ใชในการตรวจวินจิฉัย
การตรวจทางรังสีวิทยา
จากภาพถาย CT scan ส่ิงที่พบไดบอยคือ การที่มีเนื้อสมองบวมทั่วทั่ว
สวนในรายงานผูปวย อาจพบวามี ภาวะเลือดออกในเนื้อสมอง ความผิดปกติของ
thalamus, basal
ganglia, brain stem และ cerebellum ไดใน CT scan
www.cu
eid.or
g
Slide 71
Investigations• Radiological findings• MRI
Cam et al. perform MRI scan 18 in 27 patients with dengue & neurological symptoms
4 pts – Normal2 pts – Encephalitic-like changes
12 pts – Cerebral edema1 pts – Intracranial hemorrhage
การตรวจทางรังสีวิทยา
การถายภาพสมองดวยคลื่นแมเหล็กไฟฟา ซ่ึง Cam และคณะศึกษาในผูปวยที่ติดเช้ือไขเดงกีที่มีอาการ
และอาการแสดงทางระบบประสาท โดยพบวา
มีผูปวย 4 คน ผล MRI brain ปกติ
ผูปวย 2 คน พบวามีการเปล่ียนแปลงของเนื้อสมองท่ีมีลักษณะคลายกับการอักเสบของเนื้อสมอง
ผูปวยจํานวนถึง 12 คน ที่พบลักษณะของเน้ือสมองที่บวมทั่วทั่วไป และมีผูปวย 1 รายทีพ่บเลือดออก
ในโพรงกระโหลกศีรษะ
www.cueid
.org

Slide 72
Investigations
Neurophysiological findings• Electroencephalograms ( EEGs )
Typically show generalized slow wavesGomes et al: reported change 44% of DHF
การตรวจทางประสาทวิทยา
การตรวจคล่ืนไฟฟาสมองจะพบลักษณะที่เรียกวา เจเนอรอลไลซ สโลว เวฟ โดยโกมสและคณะรายงานวา
พบลักษณะคล่ืนไฟฟาสมองแบบนีไ้ดถึง 44 เปอรเซนต ในผูปวยไขเลือดออกเดงกี
www.cueid
.org
Slide 73
Investigations• Cerebrospinal fluid
15-30% of encephalithic dengue have a moderater pleocytosis usually lymphocytic
Most patients have normal CSFCSF opening pressures were moderately
elevated ( 21-30 cm )
การตรวจวิเคราะหน้าํไขสันหลัง
พบวาประมาณ 15-30 เปอรเซนต ในผูปวยที่มีภาวะสมองอักเสบจากการติดเชื้อเดงกี ถานําน้าํไขสันหลัง
มาตรวจจะพบวามีเซลลออกมาปานกลาง และมักจะเปนเซลลเม็ดเลือดขาวชนิดลิมโฟซัยท แต
ผูปวยสวนใหญมักจะมีผลการวิเคราะหน้าํไขสันหลังที่ผิดปกติ และพบวาความในในชองไขสันหลังกอนระบาย
น้ําไขสันหลังจะสูงขึ้นเล็กนอย คือ 21-30 มิลลิเมตร ปรอท
www.cueid
.org
Slide 74
Diagnosis
• Traditional• Virus isolation• Antibody tests
การวนิิจฉัยการติดเช้ือไวรัสเดงกี แบงแนวทางการวินิจฉัย ออกเปน 3 ประเภท ใหญใหญ คือ
วิธีการโดยทัว่ไป
วิธีการจําแนกไวรัส
วิธีการทดสอบดวยแอนติบอด้ี
www.cueid
.org
Slide 75
Virus isolation• Isolated from serum : 1st few day of illness• Using continuous mosquito cell lines after 7-14
days• Formation of large syncytia in Aedes albopictus
C6/36 cells• Confirmed by indirect immunofluorescence with
serotype-specific monoclonal Ab
การวนิิจฉัยโดยการจาํแนกชนิดของไวรัส
โดยแยกจากซีร่ัม ในชวงวันแรกแรกที่ผูปวยมีอาการเจ็บปวย โดยทําในเซลลไลนของยุงอยางตอเนื่อง 7-14
วัน โดยถามีเช้ือไวรัสอยูจริงจะมีการจับกลุมกันเปนรางแห โดยเฉพาะใน aedes albopictus
แมจะสามารถทําการจําแนกไวรัสไดแลว ก็ตองมีการยืนยันผล ดวยวิธีการ indirect immunofluorescence
และ serotype-specific monoclonal Ab
www.cu
eid.or
g
Slide 76
Antibody testings• After defavescence: viral culture & PCR become
negative• IgM & IgG capture ELISA• Serological cross-reactivity: especially JE• Area with >1 Flavivirus cocirculate need to test
against both viruses in parallel• Endemic area: IgM Ab persisted > 3 mo
การทดสอบดวยแอนติบอดี
หลังจากระยะที่รางกายมกีารกําจัดเช้ือไวรัสแลว การตรวจหาไวรัสดวยการเพาะเช้ือหรือวิธีพีซอีารมักจะ
ใหผลลบ จึงมีการใชการตรวจหารองรอยของการติดเช้ือไวรัส โดยตรวจหาแอนติบอดีที่รางกายสรางขึ้นเพ่ือ
ตอตานเชื้อไวรัส โดยใชวิธีที่เรียกวา อิมมูโนกลอบูลินเอ็มและจี แคพเจอรอีไลซา แตอยาลืมวาการตรวจทางซี
โรโลจี มีโอกาสท่ีจะเกิดการทําปฏิกิริยาขามกลุมหรือที่เรียกวา ครอส รีแอคติวิตี
โดยเฉพาะกับเช้ือเจแปนิส เอนเซฟาไลทิส ไวรัส เพราะฉะน้ันในพ้ืนทีท่ี่มีการติดเช้ือในกลุมฟลาวิไวรัสมากกวา
1 ชนิด การทดสอบเพ่ือตรวจหาแอนติบอดีตอไวรัส ควรทําตอไวรัสทัง้สองชนิดเสมอ
สวนการแปลผลซีโรโลจีในพ้ืนที่ท่ีมีความชุกของโรคสูงก็ตองทําดวยความระมัดระวัง ยกตัวอยางเชน เดงกี ไอจี
เอ็ม แอนติบอดี จะคงอยูไดนานมากกวา 3 เดือน
www.cueid
.org

www.cueid
.org

Slide 77
Strong evidence
• Demonstrated during the neurological illness• IgM Ab in CSF• Dengue virus is detected in CSF
หลักฐานที่หนกัแนนพอทีจ่ะบอกวามีการติดเช้ือไวรัสเดงกีในระบบประสาท คือ
สามารถแสดงใหเห็นวามกีารติดเช้ิอจริงระหวางท่ีผูปวยยังมีอาการและอาการแสดงทางระบบประสาท
ตรวจพบเดงกีไอจีเอ็ม แอนติบอดีในน้าํไขสันหลัง
ตรวจพบเดงกีไวรัสในน้าํไขสันหลัง
www.cueid
.org

Slide 78
ELISAs
• Now commercially available• Test for more than one Flavivirus in parallel• Simple kit for rapid testing withut sophisticated
equipment• False negative may occur
อีไลซา หรือทีย่อมาจาก เอนไซม ลิงค อิมมูโนซอรเบนท แอสเซ
ซ่ึงปจจุบันพัฒนามาเปนชดุคิทที่วางขายตามทองตลาดแลว โดยพบวาสามารถทดสอบฟลาวิไวรัสได
มากกวา 1 ชนดิไดในการตรวจเพียงคร้ังเดียว โดยวิธีการใชคิทในการตรวจก็งายไมซับซอน และสามารถทําได
อยางรวดเร็ว แตการแปลผลก็ตองระมัดระวังเชนเดียวกัน ตัวอยาง เชน ใชคิทไปตรวจในชวงเออรลี ไวรีเมีย
ซ่ึงรางกายยังไมทันสรางแอนติบอดีตอเชื้อไวรัส ทําใหการทดสอบทีต่รวจหาแอนติบอดีตอเช้ือใหผลเปนลบ
แตที่จริงแลวมกีารติดเช้ืออยู
www.cu
eid.or
g

Slide 79
Viral causes of Encephalopathy
• Encephalitis due to arboviruses by geographical region
• Asia: JE,West Nile, dengue, Murray valleyChikungunya, Metri
มีไวรัสหลายตอหลายชนิดทีส่ามารถทําใหเกิดภาวะเอนเซฟาโลพาทไีด ยกตัวอยางเชน การเกิดสมองอักเสบ
มักจะเกิดจาก อารโบไวรัส ซ่ึงก็ขึ้นอยูกับพ้ืนทีแ่ละภูมิประเทศ ซ่ึงถาเปนแถบเอเชียไวรัสที่เปนสาเหตุของสมอง
อักเสบท่ีพบบอย คือ เจแปนิส เอนเซฟาไลทิส. เวส ไนล . เดงกี. มัวเร วัลเล. ชิกุงกุนยาและเมท ี
www.cueid
.org

Slide 80
Management• Neurological Dengue
Encephalopathic dengueSimilar to other encephalopathies
Level of consciousnessSeizureRaised intracranial pressureBrainstem herniation syndromes
การดูแลรักษาผูปวย ในผูปวยทีม่ีอาการและอาการแสดงทางระบบประสาทที่เกิดจากการติดเช้ือเดงกี
เดงกี เอนเซฟาโลพาที การดูแลก็เชนเดียวกับภาวะเอนเซฟาโลพาทีจากสาเหตุอ่ืน โดยจะพิจารณาดูที ่
ระดับความรูสึกตัว
ชัก
การเพ่ิมขึ้นของความดันในโพรงกระโหลกศีรษะ
และกลุมอาการท่ีเกิดจากสมองเล่ือนมากดทับกานสมอง
www.cueid
.org

Slide 81
Level of Consciousness• Scoring system : GCS for adult & modified
version for children• AVPU scale
A: AwakeV: Responds to VoiceP: Responds to PainU: Unresponsive
โดยที่ระดับความรูสึกตัว อาจประเมินโดยใชระบบการใหคะแนแ โดยอาจใชกลาสโกลว โคมา สเกลในผูปวยที่
เปนผูใหญ และอาจใชแบบประยุกตเพ่ือใหเหมาะสมกบัผูปวยที่เปนเด็ก
หรืออาจใชวธิกีารงายงายที่เรียกวา AVPU สเกล ก็ได
www.cueid
.org

Slide 82
Level of Consciousness• Coma
Sedated & ventilated in ICUAirway protectionMaximum medication to control seizuresHyperventilation to reduced ICPOxygen administrationCareful fluid management & drug doses
โดยผูปวยท่ีอยูในชวงโคมา หลักการดูแลรักษา คือ
ใหผูปวยไดหลับพักผอนอยางเต็มที่และชวยหายใจในหออภิบาลผูปวยหนัก
ดูแลปองกันเร่ืองทางเดินหายใจใหเปดโลงอยูเสมอ
ใชยาจนสามารถควบคุมอาการชักได
ชวยหายใจแบบเร็วเพ่ือลดการเกิดสมองบวมและลดความดันในโพรงกระโหลกศรีษะ
การใหออกซิเจนเสริม
และที่สําคัญ คือ การควบคุมดูแลปริมาณสารนํ้าและยาที่จะใหเขาไปในตัวผูปวยอยางใกลชิด
www.cueid
.org

Slide 83
Seizures
• Subtle motor seizure: malaria, JE, other cause of non-traumatic coma
• Twitching of a digit, or lip, nystagmoid eye movement, or tonic eye deviation EEG revealed = status epilepticus
• Need careful examination: lifting the eyelids is recommended
อาการชัก สามารถพบได เชนเดียวกับ มาลาเรีย ไขเจแปนิส เอนเซฟาไลทิส และสาเหตุอ่ืนทีท่ําใหเกิดโคมา
โดยไมไดมาจากอุบัติเหตุ
โดยอาการชักอาจมแีคการบิดของนิ้ว ริมฝปาก ตากลอกแบบกระตุกไปมาหรือคาง ซ่ึงในผูปวยกลุมนีถ้าทํา
การตรวจดวยการตรวจคล่ืนไฟฟาสมองจะพบวามีอาการชักคาง
ดังนั้นเวลาตรวจรางกายเพ่ือติดตามเปนระยะในผูปวยประเภทนี้ จึงแนะนาํใหเปดเปลือกตาดูทุกคร้ัง
www.cueid
.org

Slide 84
Raised ICP & Herniation• Fluid management: difficult• Conflict: shock resuscitation & cerebral edema• Restore BP and perfusion : 1st priority• Prefer isotonic crystalloid or hypertonic colloid• If no shock: fluid maintainance = 2/3 of normal• ↑ ICP ↓ level of consciousness, s/s of herniat
20% mannitol (0.5-1.0g/kg) is givenRole of steroids : not been assessed
การเพ่ิมขึ้นของความดันในโพรงศีรษะและการเล่ือนตัวของสมอง
การบริหารการใหสารน้าํเปนส่ิงท่ีสําคัญและมักจะทําไดคอนขางยาก
เน่ืองจากตองคํานึงถึงภาวะ shock แตในขณะเดียวกนัก็ตองคํานึงถึงภาวะสมองบวม
แตอยางไรก็ตามส่ิงแรกท่ีควรคํานึงถึงคือ ความดันโลหติและการไหลเวียนเลือด
นิยมใช สารน้าํชนิดที่เปน isotonic crystalloid โดยถาผูปวยไมอยูในภาวะ shock จะพิจารณาใหสารน้ําเพียง
สองในสามของความตองการตอวันของผูปวย
www.cu
eid.or
g
Slide 85
Other measures
• Suspected bacterial meningitis broad spectrum ABO should be given
• Hypoglycemia common in many tropical pediatric conditions
• Adequate nutrition• Avoid complications of severe encephalopathy:
pneumonia, UTI, bedsores and contractures
ภาวะที่อาจเกดิรวมที่ตองเฝาระวัง ไดแก
ถาสงสัยวาจะเกิดเยื่อหุมสมองอักเสบจากเชื้อแบคทีเรีย ก็สามารถพิจารณาใหยาปฏิชีวนะที่คลอบคลุมเช้ือ
ไดทนัท ี
ในผูปวยเด็ก โดยเฉพาะเด็กเล็กตองระวังวาอาจเกิดภาวะน้ําตาลในเลือดตํ่าได
อยาละเลยเร่ืองการดูแลดานโภชนาการใหผูปวยเสมอ
พยายามดูแลผูปวยเพ่ือหลีกเล่ียงภาวะแทรกซอนที่เกิดจากพยาธิสภาพของสมองที่รุนแรง ยกตัวอยาง เชน
ภาวะปอดติดเช้ือ ติดเชื้อในทางเดินปสสาวะ แผลกดทบั รวมถึงการยึดติดของขอที่ไมไดใชงาน
www.cueid
.org

Slide 86
Prevention of Dengue• No commercial available vaccine • Surveillance for dengue, mosquito activity &
control vectors
ในปจจุบันยังไมมีวัคซนีที่ใชในการปองกนั
การเฝาระวังและควบคุมพาหะของโรค ซ่ึงก็คือยุงจึงเปนส่ิงสําคัญ
www.cueid
.org

Slide 87
Dengue Vaccines• Development of vaccine against dengue has
been hampered• Tetravalent dengue vaccine• Life-attenuated vaccine: phase I & II in Thailand
and US.• Recombinant dengue vaccine: being developed• Fully incorporated into expanded program• Vector control remain our only defense against
dengue commitment, education & community participation
เกี่ยวกับเดงกีวัคซีน
ปจจุบันเดงกีวัคซีน อยูระหวางการพัฒนาเพ่ือใหสามารถปองกันการติดเช้ือไวรัสเดงกีไดอยางมี
ประสิทธิภาพ โดยมีรูปแบบเปนเตตราวาเลนท วัคซีน โดยวัคซีนในรูปแบบที่ยังเปนเช้ือมีชีวิตท่ีถกูทําใหออน
กําลังนัน้ กําลังทําการศึกษาอยูที่ระยะที่ 1 และ 2 ในประเทศไทยและสหรัฐอเมริกา สวนวัคซีนที่อยูในรูปแบบ
รีคอมบิแนนทกําลังถูกคิดคนและพัฒนา ดังนั้นในปจจุบันจึงยังไมมวีคัซีนปองกันไขเลือดออกใชในโปรแกรม
การฉีดวัคซีน การควบคุมพาหะของโรคซ่ึงก็คือ ยุงลาย จึงเปนส่ิงที่ยังจําเปน ซึ่งทุกหนวยงานรวมท้ัง
ประชาชนเองตองตระหนักถึงความสําคัญของเร่ืองนี้และรวมมือกนัเพ่ือแกไข
จัดทําโดย
วรวฒุิ รุงประดับวงศ & คณา เกษมทรัพย
www.cueid
.org





























