Embed Size (px)
Citation preview
Dengue and DHF
PPS Interim
GuidelinesGuidelines
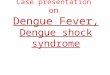
Epidemiology
• DF and DHF is the most important arthropod-borne
viral disease among humans
• In the last 50 years, cases have multiplied 30-fold
– Increasing geographic expansion to new countries causing – Increasing geographic expansion to new countries causing
high mortalities in early phase of outbreaks
– Shifted from urban to rural settings
– Public health emergency of international concern with
implications for health security due to disruption and rapid
epidemic spread beyond national borders
World Health Assembly 2005; Resolution 58.5
EpidemiologyEpidemiology
• ~ 2.5 billion people live in dengue endemic
countries
– WHO SEA region and Western Pacific: 1.8 B (>70%)
at risk population bear ~75% of current global at risk population bear ~75% of current global
disease burden
• WestPac: Cambodia, Philippines, Malaysia and
Vietnam reported >1 M cases (2001-2008)
– CFR highest in Cambodia and the Philippines
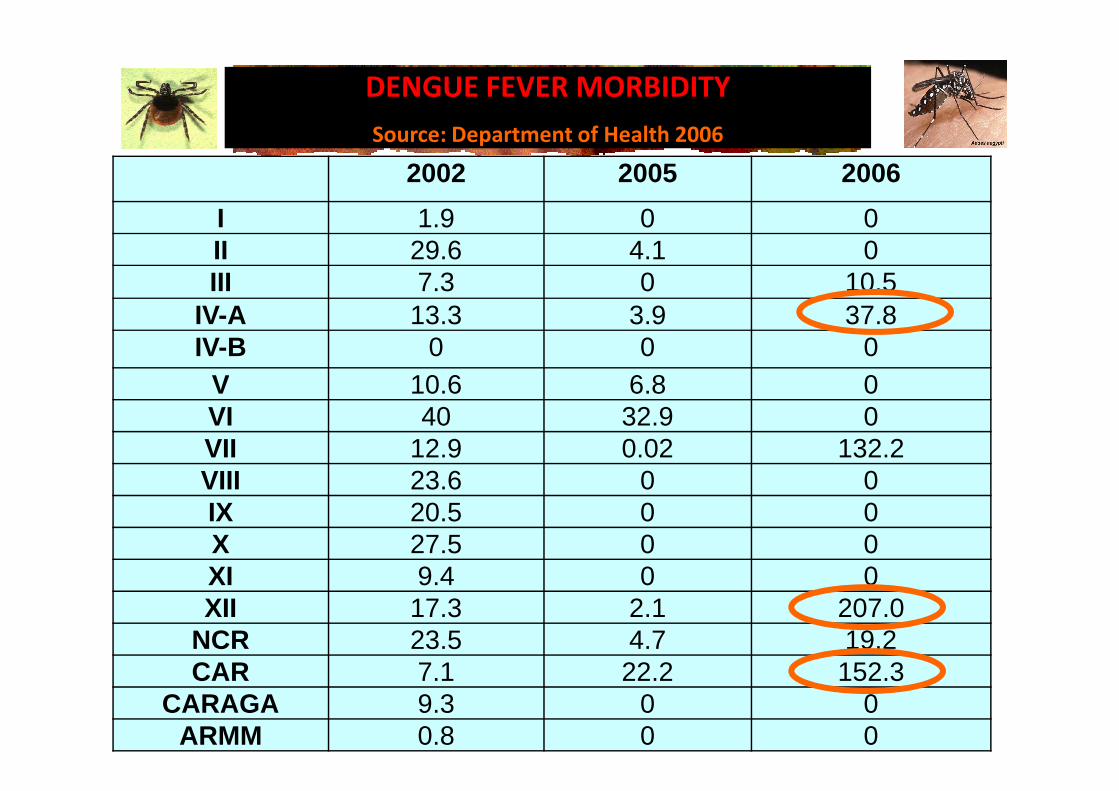
2002 2005 2006
I 1.9 0 0II 29.6 4.1 0III 7.3 0 10.5
IV-A 13.3 3.9 37.8IV-B 0 0 0
V 10.6 6.8 0
DENGUE FEVER MORBIDITY
Source: Department of Health 2006
V 10.6 6.8 0VI 40 32.9 0VII 12.9 0.02 132.2VIII 23.6 0 0IX 20.5 0 0X 27.5 0 0XI 9.4 0 0XII 17.3 2.1 207.0
NCR 23.5 4.7 19.2CAR 7.1 22.2 152.3
CARAGA 9.3 0 0ARMM 0.8 0 0
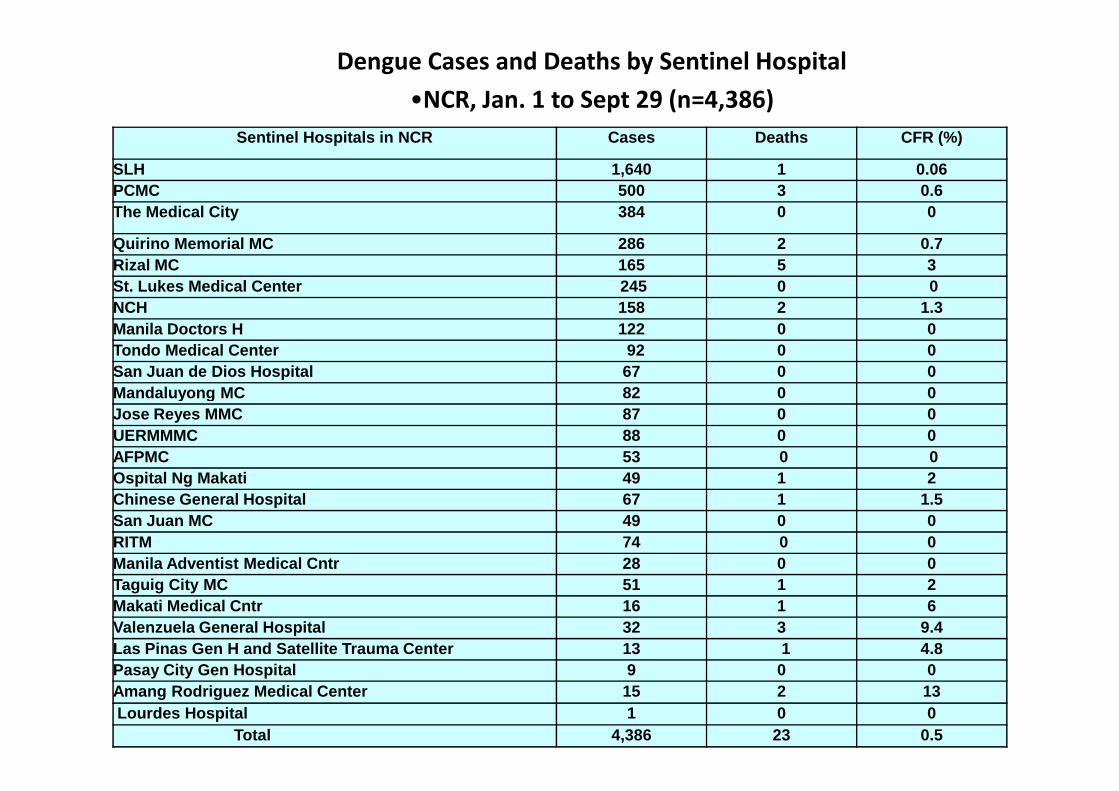
Dengue Cases and Deaths by Sentinel Hospital
•NCR, Jan. 1 to Sept 29 (n=4,386)
Sentinel Hospitals in NCR Cases Deaths CFR (%)
SLH 1,640 1 0.06PCMC 500 3 0.6The Medical City 384 0 0
Quirino Memorial MC 286 2 0.7Rizal MC 165 5 3St. Lukes Medical Center 245 0 0NCH 158 2 1.3 Manila Doctors H 122 0 0Tondo Medical Center 92 0 0 San Juan de Dios Hospital 67 0 0Mandaluyong MC 82 0 0Mandaluyong MC 82 0 0Jose Reyes MMC 87 0 0UERMMMC 88 0 0AFPMC 53 0 0Ospital Ng Makati 49 1 2Chinese General Hospital 67 1 1.5San Juan MC 49 0 0RITM 74 0 0Manila Adventist Medical Cntr 28 0 0Taguig City MC 51 1 2Makati Medical Cntr 16 1 6Valenzuela General Hospital 32 3 9.4Las Pinas Gen H and Satellite Trauma Center 13 1 4.8Pasay City Gen Hospital 9 0 0Amang Rodriguez Medical Center 15 2 13Lourdes Hospital 1 0 0
Total 4,386 23 0.5
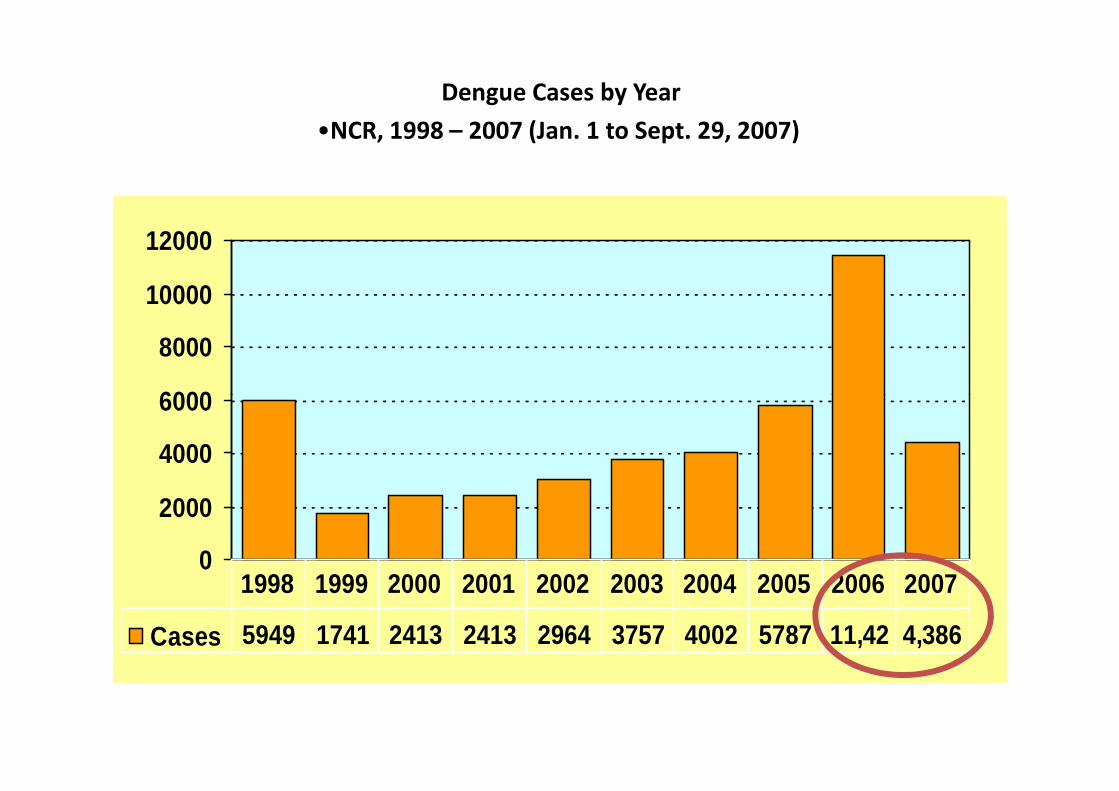
Dengue Cases by Year
•NCR, 1998 – 2007 (Jan. 1 to Sept. 29, 2007)
6000
8000
10000
12000
0
2000
4000
6000
Cases 5949 1741 2413 2413 2964 3757 4002 5787 11,42 4,386
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Dengue
• Caused by an arbovirus transmitted by Aedes mosquitoes.
• Highly seasonal in many countries in Asia and South AmericaSouth America
• Illness starts with acute onset of fever remaining continuously high for 2-7 days
• Most children recover but a small proportion develop severe disease
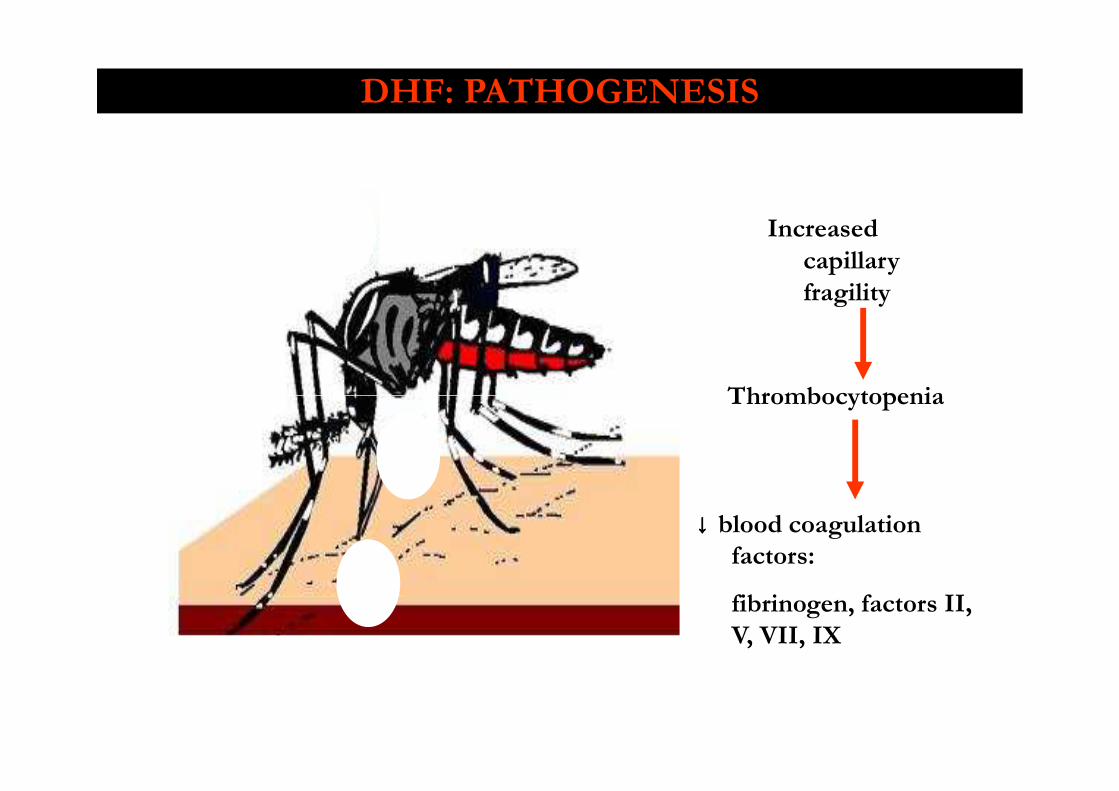
Increased
capillary
fragility
Thrombocytopenia
DHF: PATHOGENESIS
Thrombocytopenia
↓↓↓↓ blood coagulation factors:
fibrinogen, factors II,
V, VII, IX
Dengue Guidelines
2008 – PPS’ first evidence-based guidelines on Dengue Fever and Dengue Hemorrhagic Fever1
2009 - WHO “Dengue Guidelines for Diagnosis, 2009 - WHO “Dengue Guidelines for Diagnosis, Treatment, Prevention and Control- New edition 2009.”2
Dengue Guidelines
Two most important differences:
1. Dengue case classification
2. Clinical management
2010 INTERIM GUIDELINES ON FLUID MANAGEMENT OF DF/DHF
Objectives
1. To compare the Dengue Case Classification used in the 2008 PPS Dengue evidence-based guidelines and the proposed 2009 WHO Dengue Guidelines
2. To update the section on fluid management of the 2008 PPS Dengue evidence-based guidelines
3. To develop clinical algorithms on fluid resuscitation of patients with dengue based on presenting clinical features and based on the presence of compensated or uncompensated shock
2010 INTERIM GUIDELINES ON FLUID MANAGEMENT OF DF/DHF
Target Population
- pediatricians- family physicians- general practitioners- general practitioners- other healthcare professionals of various specialties
both in the private and government settings who are involved in the diagnosis and management of patients with dengue.
DENGUE CASE CLASSIFICATION
WHO Guidelines adopted by 2008 PPS guidelines:
DHF cases must fulfill all the following four criteria:1. fever or a history of acute fever lasting 2-7 days2. at least one of the ff hemorrhagic tendencies:
(+) TT, petechiae, purpura, ecchymoses;(+) TT, petechiae, purpura, ecchymoses;bleeding from mucosa, GIT, injection sites, orother location
3. thrombocytopenia with PC ≤ 100,000/µl4. hemoconcentration - ≥20% rise in hematocrit
relative to baseline or evidence of plasma leakage (i.e. pleural effusion, ascites, and/or hypoproteinemia)
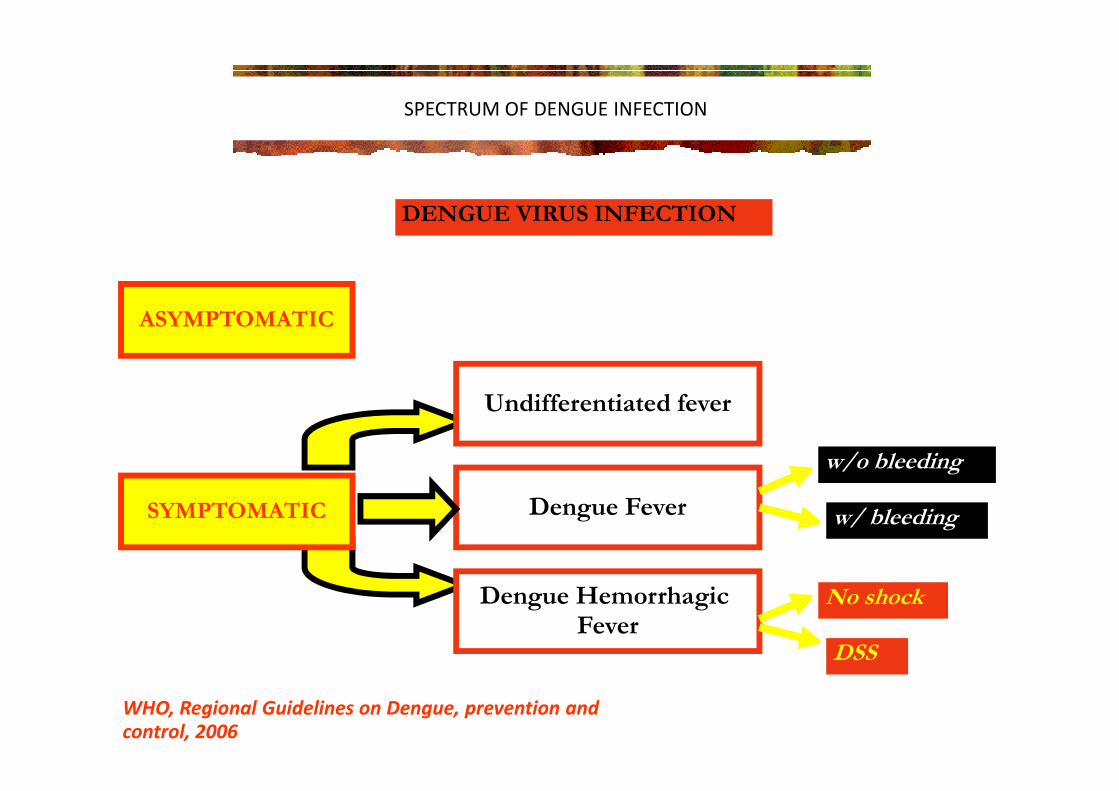
SPECTRUM OF DENGUE INFECTION
DENGUE VIRUS INFECTION
Undifferentiated fever
ASYMPTOMATIC
Undifferentiated fever
Dengue Fever
Dengue Hemorrhagic Fever
w/o bleeding
w/ bleeding
No shock
DSS
WHO, Regional Guidelines on Dengue, prevention and
control, 2006
SYMPTOMATIC
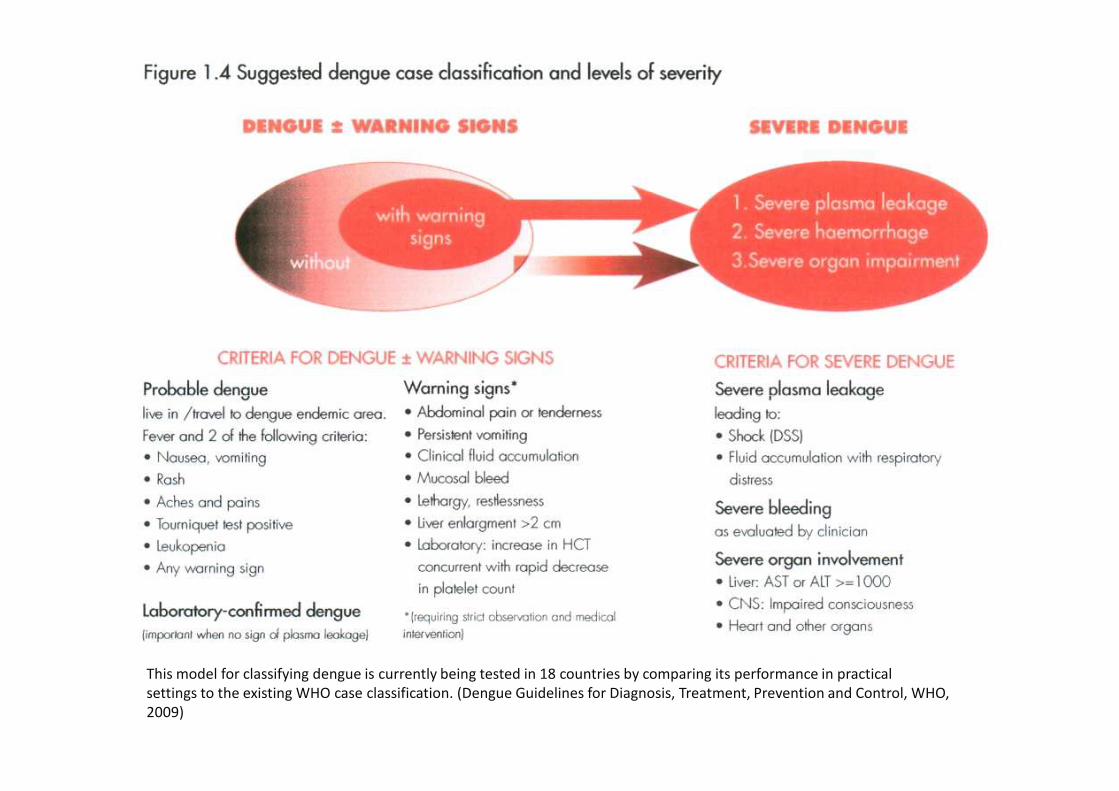
This model for classifying dengue is currently being tested in 18 countries by comparing its performance in practical
settings to the existing WHO case classification. (Dengue Guidelines for Diagnosis, Treatment, Prevention and Control, WHO,
2009)
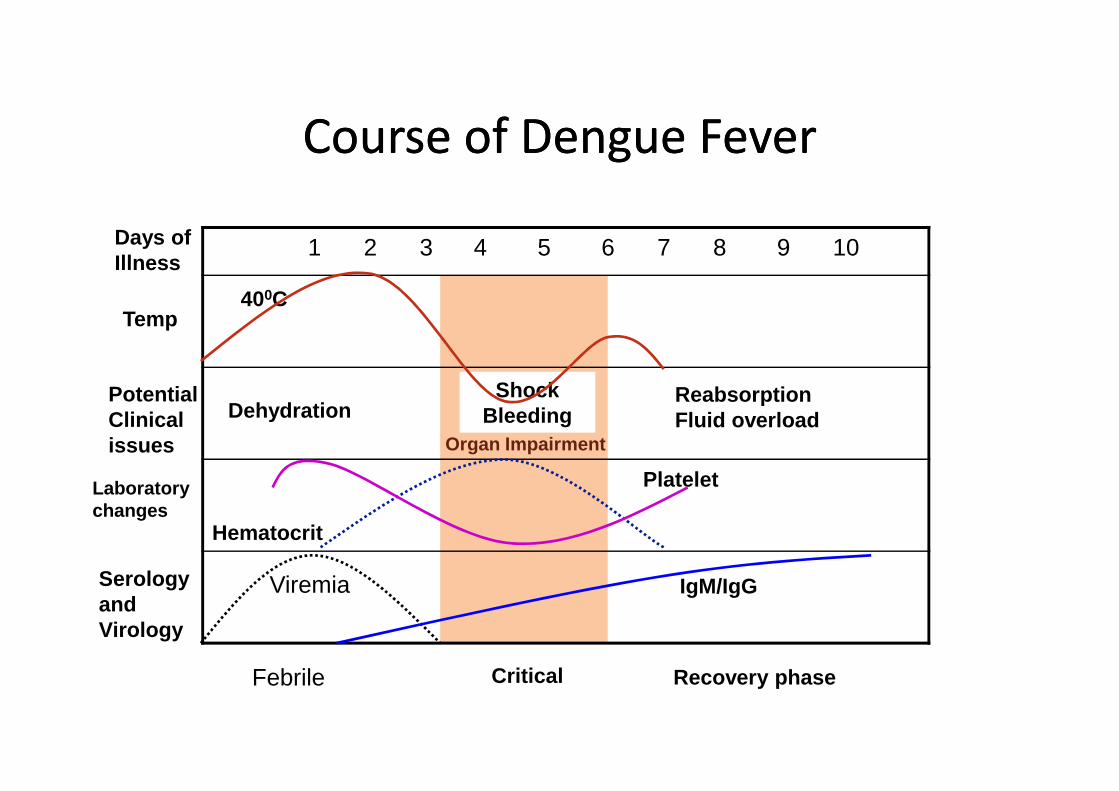
1 2 3 4 5 6 7 8 9 10Days ofIllness
Temp
Potential Shock Reabsorption
400C
Course of Dengue FeverCourse of Dengue Fever
PotentialClinicalissues
Laboratorychanges
SerologyandVirology
Febrile Critical Recovery phase
Dehydration
Hematocrit
Platelet
Viremia IgM/IgG
ShockBleeding
Organ Impairment
ReabsorptionFluid overload
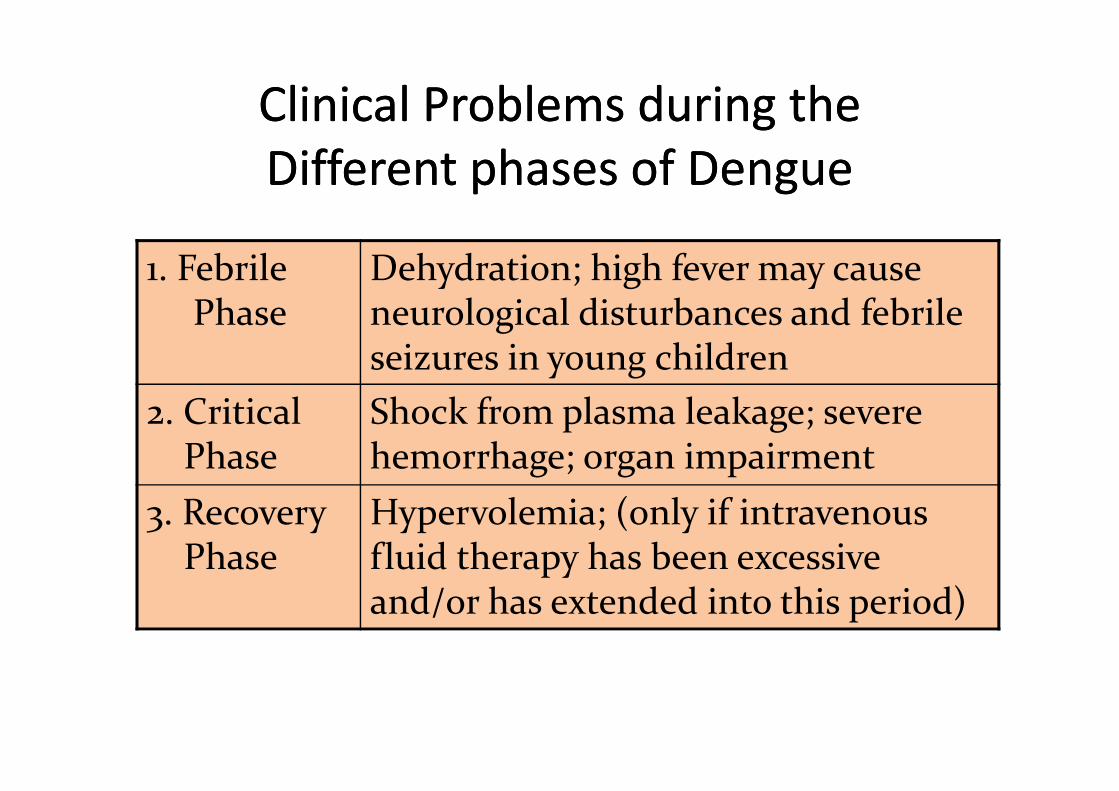
Clinical Problems during the
Different phases of Dengue
Clinical Problems during the
Different phases of Dengue
1. FebrilePhase
Dehydration; high fever may cause neurological disturbances and febrile seizures in young children
2. Critical Shock from plasma leakage; severe 2. CriticalPhase
Shock from plasma leakage; severe hemorrhage; organ impairment
3. RecoveryPhase
Hypervolemia; (only if intravenous fluid therapy has been excessive and/or has extended into this period)
DENGUE CASE CLASSIFICATION
2009 WHO case classification
- results of the validation study through a prospective multicenter study is expected to be prospective multicenter study is expected to be available before the end of 2010
- therefore, there is no recommendation yet to adapt this proposed 2009 case classification of dengue
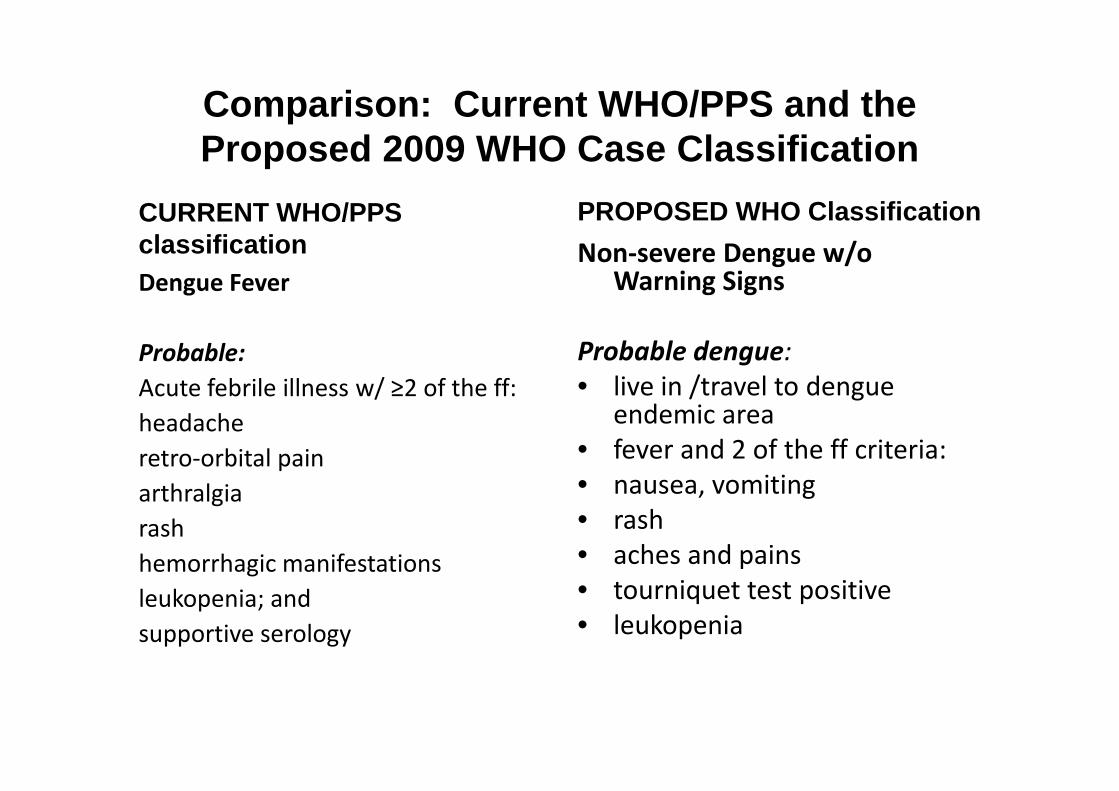
Comparison: Current WHO/PPS and the Proposed 2009 WHO Case Classification
CURRENT WHO/PPS classificationDengue Fever
Probable:
Acute febrile illness w/ ≥2 of the ff:
PROPOSED WHO Classification
Non-severe Dengue w/o Warning Signs
Probable dengue:
• live in /travel to dengue Acute febrile illness w/ ≥2 of the ff:
headache
retro-orbital pain
arthralgia
rash
hemorrhagic manifestations
leukopenia; and
supportive serology
• live in /travel to dengue endemic area
• fever and 2 of the ff criteria:
• nausea, vomiting
• rash
• aches and pains
• tourniquet test positive
• leukopenia
Comparison: Current WHO/PPS and the Proposed 2009 WHO Case Classification
CURRENT WHO/PPS classification
Dengue Fever
Confirmed:
PROPOSED WHO Classification
Non-severe Dengue w/o
Warning Signs
Laboratory-confirmed dengueConfirmed:
a case confirmed by
laboratory criteria
Laboratory-confirmed dengue
(important when no sign of
plasma leakage)
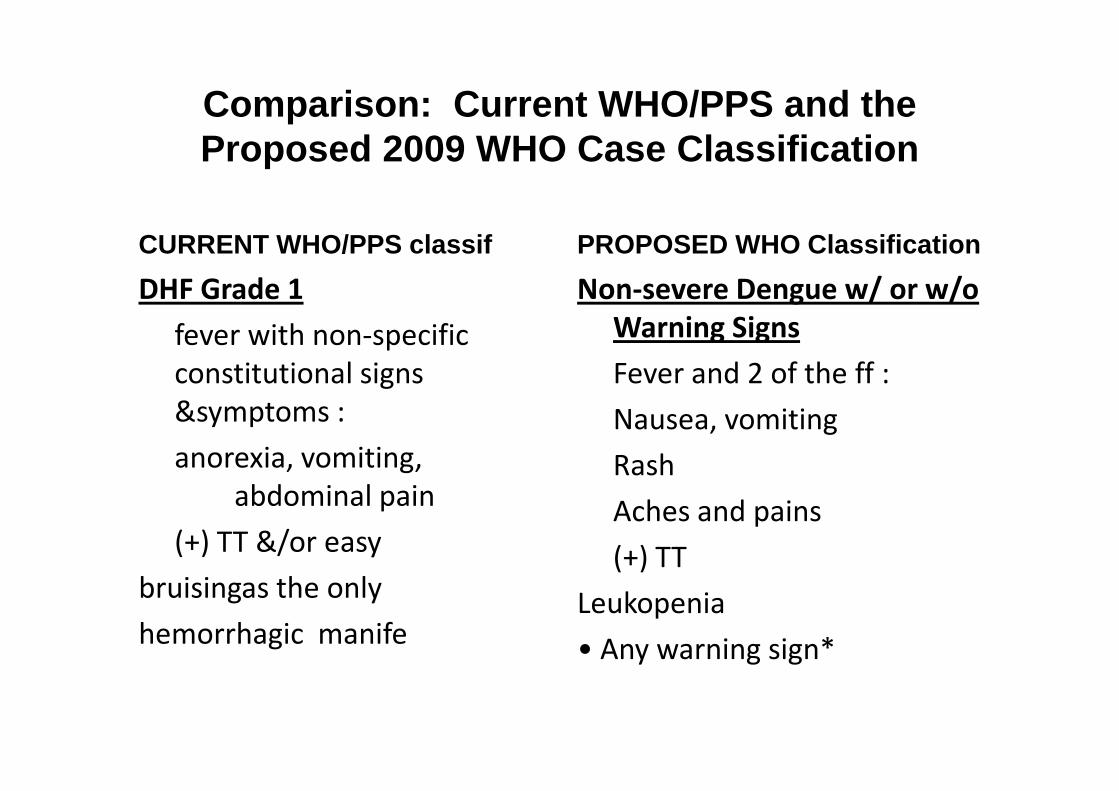
Comparison: Current WHO/PPS and the Proposed 2009 WHO Case Classification
CURRENT WHO/PPS classif
DHF Grade 1
fever with non-specific
constitutional signs
&symptoms :
PROPOSED WHO Classification
Non-severe Dengue w/ or w/o
Warning Signs
Fever and 2 of the ff :
&symptoms :
anorexia, vomiting,
abdominal pain
(+) TT &/or easy
bruisingas the only
hemorrhagic manife
Nausea, vomiting
Rash
Aches and pains
(+) TT
Leukopenia
• Any warning sign*
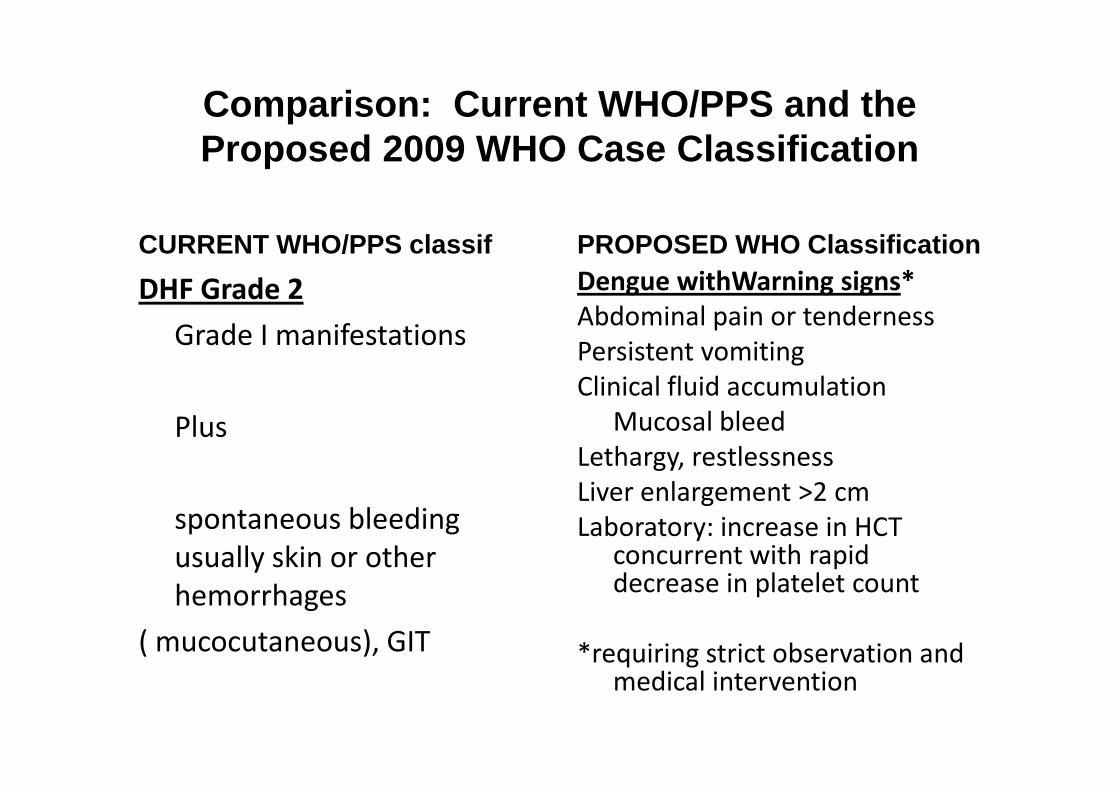
Comparison: Current WHO/PPS and the Proposed 2009 WHO Case Classification
CURRENT WHO/PPS classif
DHF Grade 2
Grade I manifestations
PROPOSED WHO ClassificationDengue withWarning signs*
Abdominal pain or tenderness
Persistent vomiting
Clinical fluid accumulation
Plus
spontaneous bleeding
usually skin or other
hemorrhages
( mucocutaneous), GIT
Clinical fluid accumulation
Mucosal bleed
Lethargy, restlessness
Liver enlargement >2 cm
Laboratory: increase in HCT concurrent with rapid decrease in platelet count
*requiring strict observation and medical intervention
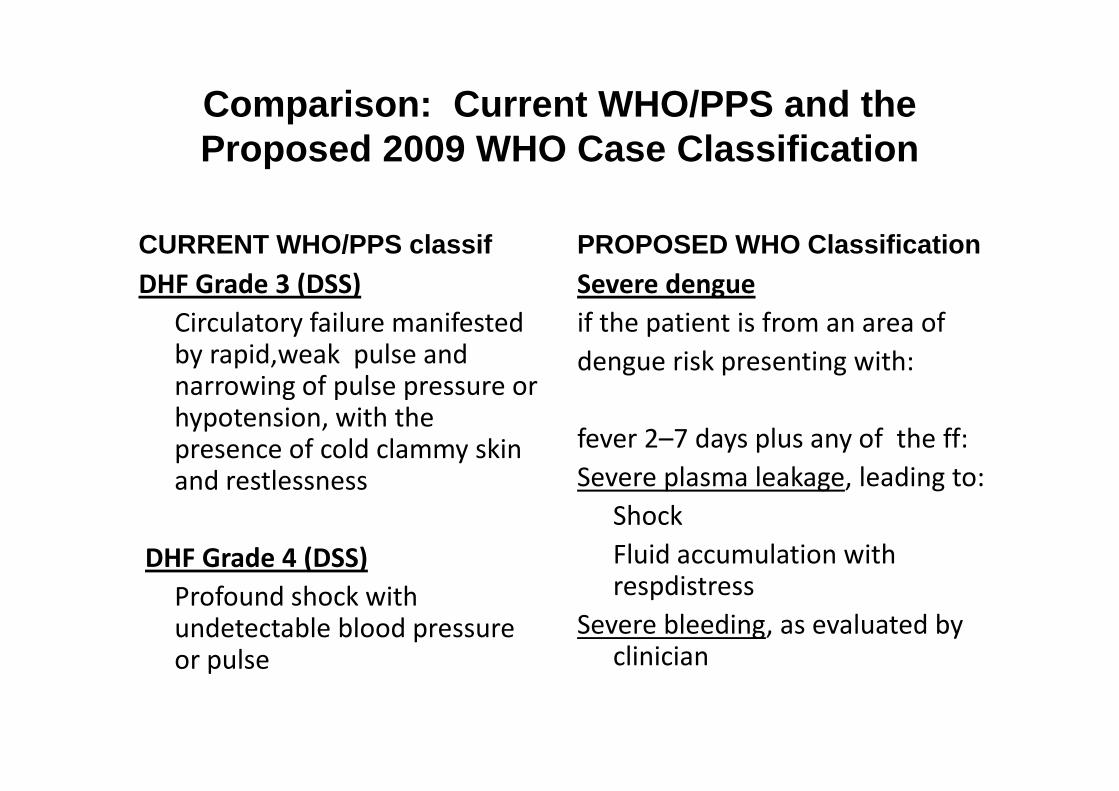
Comparison: Current WHO/PPS and the Proposed 2009 WHO Case Classification
CURRENT WHO/PPS classifDHF Grade 3 (DSS)
Circulatory failure manifested by rapid,weak pulse and narrowing of pulse pressure or
PROPOSED WHO ClassificationSevere dengue
if the patient is from an area of
dengue risk presenting with:narrowing of pulse pressure or hypotension, with the presence of cold clammy skin and restlessness
DHF Grade 4 (DSS)
Profound shock with undetectable blood pressure or pulse
fever 2–7 days plus any of the ff:
Severe plasma leakage, leading to:
Shock
Fluid accumulation with respdistress
Severe bleeding, as evaluated by clinician
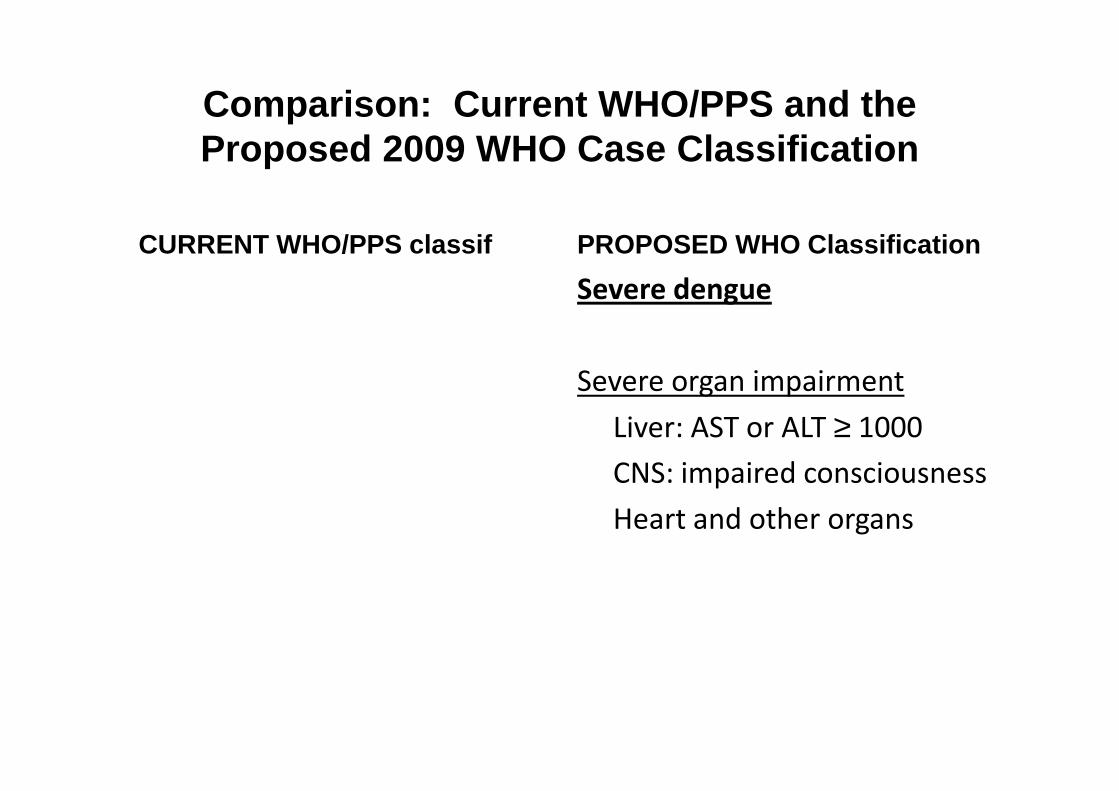
Comparison: Current WHO/PPS and the Proposed 2009 WHO Case Classification
CURRENT WHO/PPS classif PROPOSED WHO Classification
Severe dengue
Severe organ impairmentSevere organ impairment
Liver: AST or ALT ≥ 1000
CNS: impaired consciousness
Heart and other organs
Treatment
Proposed WHO Classification
• Most children managed at home provided parents
have reasonable access to hospital
– Counsel mother to bring child back for daily follow-up
but to return immediately if any of the ff. occurbut to return immediately if any of the ff. occur
• Severe abdominal pain
• Persistent vomiting
• Cold clammy extremities
• Lethargy or restlessness
• Bleeding e.g. black stools or coffee-ground vomit
Treatment
• Encourage oral fluid intake with clean H20 or ORS solution
• Paracetamol for high fever in an uncomfortable child. No aspirin or ibuprofenNo aspirin or ibuprofen
• Follow-up daily until temperature is normal. Check Hct daily where possible. Check for signs of severe disease
• Admit for signs of severe disease (mucosal or skin severe bleeding, shock, altered mental state, convulsions or jaundice) or with rapid or marked Hct rise
While new studies are being retrieved and evaluated, the updated CPG will have to await results of the validation studies being conducted by the WHO on their proposed dengue case classification and management guidelines. This will be crucial in order to come up with more comprehensive data on which to base comprehensive data on which to base recommendations for best practices on the management of dengue. The results of the validation studies are expected to be available before the end of
Thank You!!Thank You!!