Embed Size (px)
Citation preview

Department of OUTCOMES RESEARCH

Perioperative Myocardial Infarction
www.or.org
Daniel I. Sessler, M.D.
Michael Cudahy Professor and ChairDepartment of OUTCOMES RESEARCH
Cleveland Clinic
No personal financial interestsrelated to this presentation

Perioperative Mortality
Intraoperative mortality rare
Thirty-day postoperative mortality•1% nationwide in United States•2% worldwide for inpatients ≥45 years old•80% during initial hospitalization
Mostly cardiovascular or consequent

Causes of Death
Bartels, et al., 2013, Anesthesiology

Postoperative MIs are Common≈230 million non-cardiac operations / year
MI incidence 8% among inpatients >45 years•≈10 million postoperative infarctions per year
Nearly all non-ST segment elevation•Plaque rupture?•Supply-demand mismatch?•Thrombus?
Postoperative MI poorly understood•Etiology?•Prediction?•Prevention? (today’s focus)•Treatment?

Silent and Deadly
Most MIs only detected by troponin•Only 15% report chest pain•65% entirely asymptomatic
Mortality identical after apparent & silent MIs•It’s not just “troponitis”
Mortality is 10% at 30 days•Twice as high as non-operative infarctions
–Different?–Unrecognized?–Untreated? VISION: Devereaux JAMA 2012
and Botto, Anesthesiology 2014

Troponin T Predicts Mortality
“Prognosis define diagnosis”
Even slight troponin elevations predict death•Population attributable risk = 34%
Peak Troponin (ng/ml)
30-day Mortality (%)
Time to death (days)
<0.01 1 —
0.02 4 13
0.03-0.29 9 9
≥0.3 17 6

MINS (Troponin Increase)
Outcome No MINS(n = 13,822), %
MINS(n = 1,194), %
OR (95% CI)
Nonfatal cardiac arrest
0.1 0.8 14.6 (5.7-37.0)
CCF 1.0 9.4 10.3 (8.0-13.4)
Stroke 0.4 1.9 4.7 (2.9-7.6)
Death 1.1 9.8 10.1 (7.8-13.0)
Composite 2.4 18.8 9.6 (8.0-11.5)

Universal Definition of MI*
“Most patients who have a perioperative MI will not experience ischemic symptoms. Nevertheless, asymptomatic perioperative MI is as strongly associated with 30-day mortality as symptomatic MI. Routine monitoring of cardiac biomarkers in high-risk patients … after major surgery is therefore recommended.”
*Thygeson, Circulation 2012

Elevated Troponin?
Cardiology consult•Some patients need catheterization ± angioplasty•Discussion of risk
Aspirin ± statins
Heart rate and hypertension control
Lifestyle•Smoking cessation•Reasonable diet•Exercise

ENIGMA-2
Background•N2O increases plasma homocysteine
•N2O impairs endothelial function
Hypothesis•N2O increases 30-day death or major CV events•MI required troponin elevation & clinical event
Randomized trial in 7,000 high-risk patients•70% nitrous oxide•70% nitrogen
Myles, Lancet, 2014


POISE-2 Background
Surgery•Inflammatory response activates platelets•Promotes tachycardia
Aspirin•Impairs platelet aggregation•Prevents non-operative primary & secondary MI
Clonidine•Moderates central sympathetic activation•Heart rate control•Less hypotension than beta blockers•Analgesic Devereaux, NEJM (2 papers) 2014

POISE-2 Design
Inpatients >45 years at cardiovascular risk
Blinded 2 X 2 factorial trial•Aspirin 100 mg/day vs. placebo for 7 or 30 days•Clonidine 75 µg/day vs. placebo for 72 hours
Primary outcome•Death or MI within 30 days•MI required troponin elevation and clinical events
Safety outcomes•Life-threatening bleeding (i.e., required reoperation) •Clinically important hypotension (syst < 90 mmHg & Rx)•Clinically important bradycardia (HR <55/min & Rx)

10,000 Randomized Patients
99.9% complete follow-up

Patient Characteristics, Aspirin
Aspirin(N=4998)
Placebo(N=5012)
Age – (years) 69 69
Male (%) 52 53
Known vascular disease (%)
33 33
History of PCI (%) 4.7 4.7
Similar for clonidine

Aspirin, Death & MI

POISE-2 Results, AspirinOutcome Aspirin
(4998)Placebo(5012)
HR (95% CI)
P
1O outcome:death or nonfatal MI
351 (7.0) 355 (7.1) 0.99 (0.86-1.15)
0.92
Major bleed 229 (4.6) 187 (3.7) 1.23 (1.01-1.49)
0.04
Stroke 16 (0.3) 19 (0.4) 0.84 (0.43-1.64)
0.62
No interaction with clonidine

POISE-2 Results, Clonidine
%

POISE-2, Clonidine Results
Outcome Clonidine(5009)
Placebo(5001)
HR (95% CI)
P
Clinically important hypotension
2385 (48) 1854 (37) 1.32 (1.24-1.40)
<0.001
Clinically important bradycardia
600 (12) 403 (8) 1.49 (1.32-1.69)
<0.001
Stroke 18 (0.4) 17 (0.3) 1.06 (0.54-2.05)
0.87
No interaction with aspirin

POISE-2 Conclusions
Aspirin•Does not prevent death or MI•Increases life-threatening bleeding•Should not be used for MI prophylaxis
Clonidine•Does not prevent death or MI•Causes clinically important hypotension•Should not be used for MI prophylaxis
A safe and effective way to prevent perioperative myocardial infarctions remains unknown

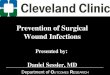
Association with MAP
Mascha, Anesthesiology, in press

Rare Outcomes: AKI and MI
Walsh, 2013
MAP < 55 mmHg

SIRS Background & DesignBackground•In-hospital mortality after cardiac surgery ≈5%•Inflammation believed to contribute•Small studies suggest that steroids help
Patients•7,500, high-risk cardiac surgery (Euroscore ≥6)•Surgery with bypass
Intervention•500 mg methylprednisilone vs. placebo, N=7,500
Major outcomes•30-day mortality•Myocardial infarction•Atrial fibrillation Whitlock, in review

SIRS ResultsOutcomes Steroid
N=3755PlaceboN=3752
RR (95% CI) p-value
First Co-Primary: Death
155 (4.1) 176 (4.7)0.88 (0.71-
1.09)0.23
Second Co-Primary: Composite death, MI, stroke, AKI, respiratory failure
908 (24) 869 (23)1.04 (0.96-
1.13)0.30
New atrial fib (%) 821 (21.9) 846 (22.5)0.97 (0.89-
1.06)0.53
MI 500 (13.3) 408 (10.9) 1.22 (1.08-
1.38) 0.001

SIRS Conclusions
Methylprednisolone in high-risk cardiac surgery•Does not reduce death•Does not reduce composite major morbidity
Does not reduce atrial fibrillation
Steroids increase perioperative MI by 20%
Do not use prophylactic methylprednisolone

Summary
MI after non-cardiac surgery•Common, mostly silent, and deadly
No known safe prophylaxis•Beta blockers work, but cause strokes•Nitrous oxide has no effect•Aspirin: no benefit and increased bleeding•Clonidine: no benefit and hypotension
Consider keeping MAP >55 mmHg

Department of OUTCOMES RESEARCH