Embed Size (px)
Citation preview

Department of Rheumatology RPAH Grand Rounds
4 May 2012 Jan Vaile Jane Bleasel

osteoporotic fracture is an increasing problem with the ageing population
50% of women and 33% of men over the age of 50 will have an osteoporotic fracture
16% of women will have a hip fracture, of whom a quarter will die within a year half will be at least partially disabled and will not regain their
previous level of function a third will be totally disabled
every 6 minutes (heading for 4) someone is admitted to an Australian hospital with a fragility fracture
prediction that by 2020, 1 in 3 hospital beds will contain a hip fracture patient

Having a low trauma fracture at least doubles the risk of a subsequent fracture (3 or more fractures has 11-fold risk of further fracture)
NSW data 2002-2008 : around 35% of patients with fracture will be re-admitted to same hospital with new fracture
About half of hip fracture patients will have sustained a previous fracture (ie. will have provided warning that they could fracture the hip)
Drugs are available which about halve the risk of subsequent fracture, in a patient with a low trauma fracture
Medicare funds treatment (bisphosphonates and others) for patients with low trauma fracture (and now for a few other groups)

only about 20% of patients with low trauma fracture are investigated and treated for osteoporosis

Ambulance staff Local doctor (time of fracture) Emergency nurses Emergency doctors Inpatient nurses Inpatient doctors Fracture clinic nurses Fracture clinic doctor Fracture clinic physios Rehab staff Geriatric nurse Geriatric doctorsPharmacist Local doctor (after eventual discharge from “the system”)
Yet often no-one does (too busy, not my job, too many other health priorities, some one else will have done it, “normal ageing”, will get to that later…….)
Enter ……. Fracture liaison services

Osteoporosis nurse (ON) loiters around fracture clinic and identifies patients aged 50+ with low trauma fracture
ON interviews appropriate patients re fracture, medical history, risk factors and previous therapy
ON organises blood tests + BMD Osteoporosis doctor sees the patient and begins
therapy if needed Phone call at one month Review at one year Funded by initial pharma grant, then trust funds

399 eligible fracture clinic patients 77% (306) were captured by the ON 87% (268/306) of osteopenic/osteoporotic 68% (209/306) patients seen by OP doctor 46% of osteopenic/ osteporotic had low vit D 97% of patients seen by OD were commenced
on a bisphosphonate. 95% reviewed at 12 months continued to take
the prescribed medication.

62 year old Greek lady Tripped at home (FOOSH) 8/1/2010 RPAH Emergency - right distal radius fracture Closed reduction 9/1/2010 (No osteoporosis discussion documented
during the admission)

18/1/2010 : Fracture clinic review 25/1/2010: Fracture clinic review
Osteoporosis nurse assessment during fracture clinic assessment: Legally blind, no previous fracture, menopause 45 no
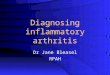
HRT, no medics, calcium intake low, nil alcohol / tobacco, otherwise well, dental extraction pending, no maternal hip # BMD spine T score -2.0, total hip 0.1, femoral neck-0.9 Vitamin D 58: TSH / Ca / PTH/ LFT normal, Cr 118

20 30 40 !-<! 00 70 80 90 100
Age (years)
11ct r or d .aunosis
Roferonce: Left Femur Total BMO (glcm') YA.T-Sccre
I
Age (years)
0.891 0.940 1.000 0.933 0.917 0.9"8 0.9"3 0.972 0.957 0.965
·2.0 ·2.2 ·1.7 ·2.2 ·2.1 ·1.9 ·2.0 · 1.9 · 2.0 ·2.0
-o.s -o.9 .0.4 ·1.0 -o.s -o.6 .0.7 -o.7 -o.s -Q.7
Milrchcd for Age, Vlci~ht (l'em;:lcs 25 100 kg), Etl1n>: .Aus:ralia (Lunu ) (ages 20-10) IJ> Spine Reference Population (v105)
Staostrcally 68% of f'l'P23t scans fall wrtllrn 150 (: 0.0' 0 Olen> for AP Spine ..2·L4)
BMO Young-Adult Age-Matchecl
Region (g/cm•) T·!iclore z-score Neck 0.875 ·0.9 0.3 wards 0.718 ·1.5 0.2 Troch 0.838 0.4 1.0 Totill 1.017 0.1 1.0
~~ttlled for ~e. Weight (females 25·100 kg), Ethnic .Ar.,;-ralla (I 11nar) (ag•.s "HO) f t'fllur R~f~"''nce Population :v 105)
Stat!Sti<:ally 6S'!'o 01 repaat scans Ia' I wttl>ln 1~0 (± 0.012 glen• tor Lett Femur Total)

March 2010 Osteoporosis Clinic • further history: 2 sisters on alendronate, 3 falls last
year • dental review planned • alendronate, vitamin D, calcium supplementation following dental work recommended
Fracture Risk Assessment Tools FRAX: 10 year risk of major fracture 3.9%, 10 year
risk of hip fracture 0.5% Garvan: major fracture 22% , hip fracture 4%

FRAX http://www.shef.ac.uk/FRAX
age (40+), height, weight, gender, previous fracture, smoking, alcohol>3 units, parental hip fracture, steroids >7.5, RA, secondary OP (eg early menopause, hyperPTH+ others)
uses femoral neck BMD 10 year risk hip fracture,
major fracture
Garvan http://garvan.org.au/promotions/bone-fracture-risk/calculator/index.php
gender, age (60+), number of fractures since 50, falls in the last year, BMD (hip not specified)
can use weight if BMD not available
5 and 10 year risk of hip or any fracture

Mar 2011: Osteoporosis Clinic - Review one year • alendronate not commenced: “dentist would not
give blessing” • spine stable, hip -3% • risk of jaw problems vs fracture discussed:
alendronate commenced

April 2012: Osteoporosis Clinic no problems with alendronate BMD spine improvement 6% ( T score -1.6), hip + 5% no further fractures eye surgery: much improved sight vitamin D 100 plan to continue 2 more years then review ? stop

First fracture: doubles risk of further fractures Fracture prediction: previous fracture, age,
BMD – models may help Individualise patient assessment Don’t forget calcium + vitamin D Don’t forget falls risk Risk of drugs are low (but not zero –
osteonecrosis of jaw overly well publicised)

82 year old Jehovah’s Witness living alone Fall at home: going to the toilet at night, no
lights on 2 Feb 11 ED Elsewhere: left
subtrochanteric fracture 2 Feb 11 Femoral pin 21 Feb11 Revision surgery for malrotation Complications: anaemia (transfused with
consent), hypotension 10 Mar 11 Rehab transfer

Medical history during admission “Osteoporosis”, urinary incontinence, short term
memory loss, gastrectomy for peptic ulcer disease, osteoarthritis, TIA’s, anxiety/ panic attacks
No Vitamin D measurement Discharged to Balmain on 16 medications
including vitamin D, Caltrate (but on omeprazole) oxycodone temazepam

19 Apr 2011 RPAH fracture clinic (with difficulty) Osteoporosis Nurse assessment #ribs age 80: tripped up a step # scapula - fall in the street #elbow – simple fall Menopause 54, no HRT Non-smoker, no alcohol Poor calcium intake, vitamin D 100 (after 2 months treatment
- great) BMD spine T score -5.3, total hip -5.2 FRAX: not needed – no help needed with decision zoledronic acid infusion administered

Balmain rehab Transitional care unit Mobilising with frame Further Balmain admission with abdominal
pain Permanent nursing home placement Never returned to home

Osteoporosis Clinic April 2012 BMD: spine T score -4.9, hip T score -4.9
Further IV zoledronic acid Continue calcium, D
Continuing high risk for fracture

First fracture predicts future fracture High falls risk increases fracture risk Hip fracture is a very serious event in an
elderly person mortality > 25% at one year 50% never regain normal function nursing home admission common and expensive
IV bisphosphonates are a good option for patients with tolerance, comorbidity or compliance issues

Fracture Prevention Service database 2008 Designed to track all patients attending
Emergency Department with low trauma fracture
Reviewed to see where the problems are Still funded by trust funds generated by staff
specialists, not by general hospital funds: database analysis funded by pharma grant

768 patients attending ED with low trauma fracture, in one year 2008-2009 Identification very problematic Review of daily lists to identify possibles, review of
shortlisted charts a thousand ED attendances a week 50-70 shortlisted 15 likely low trauma fracture

You have been referred to the RPAH Fracture Clinic. It is a Public Clinic. There are no apoolntment times. The time given is YOUR ARRIVAL TIME. The clinics are generally very busy and people require several services while at the clinic e.g. X Ray, Osteoporosis Assessment, Physiotherapy as well as the review by the Orthopaedic surgeon. This can take some time. A broad guideline on clinic is around 3- 4 hours.
Morning clinic arrival times range between 0800 and 1030 Afternoon clinic arrival times is between 1300 and 1430
Please ensure you have booked into the clinic. Phone 95159812
Ensure you bring with you any medications that you might need for the time you are in the clinic.
OSTEOPOROSIS
If you are over 50 and broke your bone in a simple slip, trip or fall you will be offered an osteoporosis assessment while you are attending the fracture clinic. You might be referred to the Osteoporosis Clinic or you can see your own GP. There are very simple and effective treatments for Osteoporosis and it might help in the prevention of further fractures.

540 of the 768 (70%) attended fracture clinic and therefore available for OP nurse review
(non-attenders time-consumingly chased by nurses)
62% (336) had BMD (No BMD: already on treatment or assessed elsewhere, patient too ill or frail esp hip #, patient declined, patient just missed (8%) )
Of those, 60% (207) osteoporotic or osteopenic 90% of these accepted OP doctor review 70 % calcium inadequate 53 % vitamin D inadequate 89 % bisphosphonate commenced

Emergency
Problems with identifying patients –incorrect inclusion and exclusion issues Potential solutions: coding, protocols, database
links (radiology / ED) Almost a third don’t get to fracture clinic Older – likely NESB, frail, comorbidities Potential solutions: “selling it”, protocols, non-
English handouts / invitations, GP

Fracture clinic -only 8% missed Logistics, manpower Potential solutions - nursing time! Funding! Funding! Funding! Telehealth for frail elderly? More nursing time should be for this, and less for admin
and chasing-up ED misses Osteoporosis clinic
Doctor time – 4 sessions a week still not enough Follow up - mushrooming population problematic (how long
to treat? How to hand over care? ) Solutions - dissemination to family doctors for investigation,
and treatment, protocols, Teleheath, letters, GP training…

The problem is not lack of available treatment, but sporadic opportunity to be prescribed it
Solutions may be in the systems Fracture liaison services: need to be available &
funded Tracking and identification systems – databases +
people to run them Follow-up systems Increased awareness of the size and urgency of the
issue may improve funding and therefore coverage