Embed Size (px)
DESCRIPTION
Credits to Owner
Citation preview

The following lecture has been approved for
University Undergraduate Students
This lecture may contain information, ideas, concepts and discursive anecdotes that may be thought provoking and challenging
It is not intended for the content or delivery to cause offence
Any issues raised in the lecture may require the viewer to engage in further thought, insight, reflection or critical evaluation

Depressive IllnessDepressive Illness
Dr. Craig JacksonDr. Craig JacksonSenior Lecturer in Health PsychologySenior Lecturer in Health Psychology
Faculty of Health Faculty of Health BCUBCU
health.bcu.ac.uk/craigjacksonhealth.bcu.ac.uk/craigjackson
[email protected]@bcu.ac.uk

““The good physician The good physician treats the disease, treats the disease, but the great physician but the great physician treats the person.”treats the person.”
William Osler William Osler

PathogenPathogen DiseaseDisease (pathology)(pathology)
ModifiersModifiersLifestyleLifestyleIndividual susceptibilityIndividual susceptibility
Traditional model of Disease DevelopmentTraditional model of Disease Development

Dominance of the biopsychosocial modelDominance of the biopsychosocial model
Mainstream in last 15 yearsMainstream in last 15 years
Hazard Hazard
Psychosocial FactorsPsychosocial FactorsAttitudesAttitudesBehaviourBehaviourQuality of LifeQuality of Life
Illness Illness (well-being)(well-being)
Rise of the person as Rise of the person as a “psychological a “psychological entity”entity”

Depressive IllnessDepressive Illness
Usually treatableUsually treatable
CommonCommon
Marked disabilityMarked disability
Reduced survivalReduced survival
Increased costsIncreased costs
Depression may beDepression may be
Coincidental associationCoincidental association
Complication of physical illness (i.e. “secondary depression”)Complication of physical illness (i.e. “secondary depression”)
Cause of / Exacerbation of somatic symptomsCause of / Exacerbation of somatic symptoms

Psychiatry in Pictures – Steve BlundellPsychiatry in Pictures – Steve Blundell
Digital CryDigital Cry
Stapled RedStapled Red

Depressive IllnessDepressive Illness
2% of population suffer from2% of population suffer from pure depressionpure depression(evenly distributed between mild, moderate,(evenly distributed between mild, moderate, and severe)and severe)
Further 8% suffer from a mixture of anxietyFurther 8% suffer from a mixture of anxiety and depressionand depression
Patients with symptoms not severe enoughPatients with symptoms not severe enough to qualify for diagnosis of either to qualify for diagnosis of either anxiety or depression..... ???anxiety or depression..... ???
Impaired working and social lives and many unexplainedImpaired working and social lives and many unexplained physical symptomsphysical symptoms
Greater use of medical servicesGreater use of medical services
““Walking Well”Walking Well”

Spectrum of mood disturbanceSpectrum of mood disturbance
Mild Mild thru to thru to SevereSevere
Transience Transience thru to thru to Persistence Persistence
Continuous distribution in populationContinuous distribution in population
Clinically significant when:Clinically significant when:(1) interferes with normal activities(1) interferes with normal activities(2) persists for min. 2 weeks(2) persists for min. 2 weeks
Diagnosis of depression / depressive disorderDiagnosis of depression / depressive disorder““Persistent & pervasive low mood”Persistent & pervasive low mood”““Loss of interest or pleasure in activities”Loss of interest or pleasure in activities”
““Ennui”Ennui”

EpidemiologyEpidemiology
2nd biggest cause of disability 2nd biggest cause of disability
worldwide by 2020 (WHO) worldwide by 2020 (WHO)
(IHD still the biggest)(IHD still the biggest)
Associated with increasedAssociated with increasedphysical illnessphysical illness
• 5% during lifetime have MDD5% during lifetime have MDD• 1 in 20 consultations1 in 20 consultations• 100 patients per GP100 patients per GP• MDD & Dysthmia > in femalesMDD & Dysthmia > in females• 20% develop chronic depression20% develop chronic depression• 30% of in-patients have depressive symptoms30% of in-patients have depressive symptoms

SuicideSuicide

SuicideSuicide
Final clinical pathwayFinal clinical pathway
1 million deaths per year, 10-12 million attempts1 million deaths per year, 10-12 million attempts
UKUK Males – most common in olderMales – most common in older
Female – most common in middle ageFemale – most common in middle age
Steady decline since 1990Steady decline since 1990
5,554 suicide deaths in UK 20065,554 suicide deaths in UK 2006
15 per 15 per 100,000 deaths males100,000 deaths males
6 per 6 per 100,000 deaths females100,000 deaths females

Almost 50% fail on first attemptAlmost 50% fail on first attempt
Previous attempters 23 times more likely to dies from suicide than those Previous attempters 23 times more likely to dies from suicide than those without previous attemptswithout previous attempts
Internal stressInternal stress
Pre-existing psychiatric morbidityPre-existing psychiatric morbidity Stack 2001Stack 2001
DemographicsDemographics
OpportunitiesOpportunities

Behavioural IndicatorsBehavioural Indicators
- recent bereavement or other life-altering loss - recent bereavement or other life-altering loss
-- recent break-up of a close relationship recent break-up of a close relationship
-- major disappointment (failed exams or missed job promotion) major disappointment (failed exams or missed job promotion) - change in circumstances (retire, redundant or children leaving home) - change in circumstances (retire, redundant or children leaving home) - physical illness- physical illness- mental illness - mental illness - substance misuse / addiction- substance misuse / addiction- deliberate self-harm, (particularly in women)- deliberate self-harm, (particularly in women)- previous suicide attempts - previous suicide attempts - loss of close friend / relative by suicidal means- loss of close friend / relative by suicidal means- loss of status- loss of status- feelings of hopelessness, powerlessness and worthlessness- feelings of hopelessness, powerlessness and worthlessness- declining performance in work / activities (sometimes this can be reversed)- declining performance in work / activities (sometimes this can be reversed)- declining interest in friends, sex, or previous activities- declining interest in friends, sex, or previous activities- neglect of personal welfare and hygiene- neglect of personal welfare and hygiene- alterations in sleeping habits (either direction) or eating habits- alterations in sleeping habits (either direction) or eating habits

Case Summary of a Depressed Patient #1Case Summary of a Depressed Patient #1
Date Symptoms Referral
1985 (16)1985 (16) AnorexiaAnorexia Secure unit teenagersSecure unit teenagers
1986 (17)1986 (17) Suicide attemptSuicide attempt Secure unit teenagersSecure unit teenagers
1986 (17)1986 (17) Self-harmSelf-harm Secure unitSecure unit CAMHS CAMHS (A levels)(A levels) Psychiatry - ECT unsubstantiatedPsychiatry - ECT unsubstantiated
1987-91987-9 Self-harm. AnorexiaSelf-harm. Anorexia UMCUMC (18-20)(18-20) (university)(university)
19901990 Working as au pairWorking as au pair GP monitoring & anti-depressantsGP monitoring & anti-depressants (21)(21) (left university)(left university)
19931993 Self-harmSelf-harm Secure unit admissionSecure unit admission(24)(24) (joined commune)(joined commune)
Female. Abused by father from 6 to 15. Moved to boarding school, then to grandparentsFemale. Abused by father from 6 to 15. Moved to boarding school, then to grandparents
Insomnia - Feeling worthless – Guilt - Recurrent morbid thought - Bleak views - Self harm – Suicide Ideation
Scholastically bright. University. Dropped out. Tried own business. Business failed.
Admin working.

EpidemiologyEpidemiology
Depression more common in those with:Depression more common in those with:
• Life threatened / limited / chronic physical illnessLife threatened / limited / chronic physical illness
• Unpleasant / demanding treatmentUnpleasant / demanding treatment
• Low social supportLow social support
• Adverse social circumstancesAdverse social circumstances
• Personal / family history of depression / psychological vulnerabilityPersonal / family history of depression / psychological vulnerability
• Substance misuseSubstance misuse
• Anti-hypertensive / Corticosteroid / Chemotherapy useAnti-hypertensive / Corticosteroid / Chemotherapy use
Q o LQ o L

AetiologyAetiology
Most depressions have triggering life events - Most depressions have triggering life events - Reactive depressionReactive depression
Especially inEspecially in a first episodea first episode
Many patients present initially with physicalMany patients present initially with physical symptoms (somatization)symptoms (somatization)
Some may show multiple symptoms ofSome may show multiple symptoms of depression in the apparent absencedepression in the apparent absence
of low mood - “Masked Depression”of low mood - “Masked Depression”
Some depression has no triggering cause - Some depression has no triggering cause - “Endogenous Depression”“Endogenous Depression”
More persistent and resistant to treatmentMore persistent and resistant to treatment

Clinical FeaturesClinical Features
• Adjustment DisordersAdjustment Disorders mildmild short-livedshort-lived reactive episodesreactive episodes
• Major Depressive Disorder (MDD)Major Depressive Disorder (MDD) 5 symptoms displayed in 14 days5 symptoms displayed in 14 days
• DysthymiaDysthymia depressed mood for 2+ yearsdepressed mood for 2+ years not severenot severe chronic depressionchronic depression unhealthy lifestyle associationsunhealthy lifestyle associations
• Bipolar Disorder / manic depressionBipolar Disorder / manic depression major depression & maniamajor depression & mania

Major depression (DSM IV)Major depression (DSM IV)
5 or more…..5 or more…..
• decreased interest / pleasure * decreased interest / pleasure * • depressed mood *depressed mood *• reduced energyreduced energy• weight gain / lossweight gain / loss• insomnia / hypersomniainsomnia / hypersomnia• feeling worthlessfeeling worthless• guiltguilt• recurrent morbid thoughtrecurrent morbid thought• psychomotor changespsychomotor changes• fatiguefatigue• poor concentrationpoor concentration• pessimism / bleak viewspessimism / bleak views• self harm ideas / actionsself harm ideas / actions• suicide ideationsuicide ideation

Classification of Depression (ICD-10)Classification of Depression (ICD-10)
PrimaryPrimaryUnipolarUnipolar
Mixed anxiety and depressive disorder (prominent anxiety) Mixed anxiety and depressive disorder (prominent anxiety) Depressive episode (single episode) Depressive episode (single episode) Recurrent depressive disorder (recurrent episodes) Recurrent depressive disorder (recurrent episodes) Dysthymia - Persistent and mild ("depressive personality") Dysthymia - Persistent and mild ("depressive personality")
BipolarBipolar Bipolar affective disorder - manic episodes ("manic depression") Bipolar affective disorder - manic episodes ("manic depression") Cyclothymia - Persistent instability of mood Cyclothymia - Persistent instability of mood
Other primaryOther primary Seasonal affective disorder Seasonal affective disorder Brief recurrent depression Brief recurrent depression
Depressive episode may beDepressive episode may beModerate or severe Moderate or severe With/Without somatic syndrome With/Without somatic syndrome With/Without psychotic symptomsWith/Without psychotic symptoms

Somatization Syndrome (DSM IV)Somatization Syndrome (DSM IV)
4 or more…..4 or more…..
AnhedoniaAnhedonia
Loss of emotional reactivity Loss of emotional reactivity
Early waking (>2 hours early) Early waking (>2 hours early)
Psychomotor retardation or agitation Psychomotor retardation or agitation
Marked loss of appetite Marked loss of appetite
Weight loss >5% of body mass in one month Weight loss >5% of body mass in one month
Loss of libidoLoss of libido

Linking Emotions with Physical SymptomsLinking Emotions with Physical Symptoms

Case Summary of a Depressed Patient #2Case Summary of a Depressed Patient #2
Date Symptoms Referral
1985 (17)1985 (17) Pervasive low moodPervasive low mood GP monitorsGP monitors
1986 (18)1986 (18) Suicide attemptSuicide attempt Child PsychiatryChild Psychiatry
1986 (18)1986 (18) Self-harmSelf-harm PsychiatryPsychiatry
1987 (19)1987 (19) Anorexia. Self-harm Anorexia. Self-harm Psychiatry – CPNPsychiatry – CPN
1988 (20)1988 (20) Suicide attemptSuicide attempt Psychiatry – CPNPsychiatry – CPN(failed romance)(failed romance)
1989 (21)1989 (21) Suicide attemptSuicide attempt Psychiatry – CPNPsychiatry – CPN(failed romance)(failed romance)
1990 (22)1990 (22) Fertility worriesFertility worries Psychiatry – CPN – fertility counsellingPsychiatry – CPN – fertility counselling
1990 (22) 1990 (22) Working in officeWorking in office GP monitoring & anti-depressantsGP monitoring & anti-depressants
1992 (24) 1992 (24) Self-harmSelf-harm MH unit (open door policy) CPNMH unit (open door policy) CPN
1996 (26) 1996 (26) Chronic FatigueChronic Fatigue MH unit (open door policy) CPNMH unit (open door policy) CPN
1998 (28) 1998 (28) FibromyalgiaFibromyalgia MH unit (open door policy) CPNMH unit (open door policy) CPN

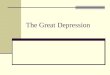
Risk Factors – Existing Health ConditionsRisk Factors – Existing Health Conditions

Depressed Patients and “Positive Symptoms”Depressed Patients and “Positive Symptoms”
Rosemary Carson Rosemary Carson
Sensations of maggots moving within her bodySensations of maggots moving within her body
Depressed, attemptedDepressed, attempted suicide at the age of 15suicide at the age of 15
Spent long periods of earlySpent long periods of early adult life in psychiatric hospitalsadult life in psychiatric hospitals
Treated with medication and electro convulsive therapyTreated with medication and electro convulsive therapy
17-year remission in affective symptoms and sensations of maggots17-year remission in affective symptoms and sensations of maggots
By 1996 became ill again - began to hear voicesBy 1996 became ill again - began to hear voices
Her art captures memories of fellow patientsHer art captures memories of fellow patients and situations from earlier admissionsand situations from earlier admissions

Depressed Patients and Positive SymptomsDepressed Patients and Positive Symptoms
Rosemary Carson - The Hospital Ward at NightRosemary Carson - The Hospital Ward at Night

ClassificationClassification
• Many patients do not fit neatly into categories of Many patients do not fit neatly into categories of either either anxietyanxiety or depressionor depression
• Mixed anxiety and depressionMixed anxiety and depression is now recognisedis now recognised
• Presence of physical symptoms indicatesPresence of physical symptoms indicates a a somatic syndromesomatic syndrome
• Value of somatic features in predicting response to treatmentValue of somatic features in predicting response to treatment is not clearis not clear
• Presence of Presence of psychotic featurespsychotic features has major implications has major implications for treatmentfor treatment
• Brief episodes of more severe depression areBrief episodes of more severe depression are also recognisedalso recognised ((brief recurrent depressionbrief recurrent depression))
• More prolongedMore prolonged recurrence is now termed recurrence is now termed recurrent depressive disorderrecurrent depressive disorder

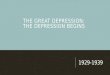
Return to WorkReturn to Work
Longer off work = Less likely to return to workLonger off work = Less likely to return to work%
retu
rnin
g to
wor
k
10 2
0 3
0 4
0 5
0 6
0 7
0 8
0 9
0 10
0
months not working
<1 2 4 6 8 10 12 14 16 18 20 22 24
Waddell, 1994Waddell, 1994

Risk FactorsRisk Factors
Anxiety + Sadness + Somatic discomfortAnxiety + Sadness + Somatic discomfort
Normal psychological response to life stressNormal psychological response to life stress
Clinical depression is a “final common pathway”Clinical depression is a “final common pathway”Resulting from interaction of Resulting from interaction of biologicalbiological, , psychologicalpsychological, and , and social factorssocial factors
Likelihood of this outcome depends on many factors:Likelihood of this outcome depends on many factors:• geneticgenetic and family predispositionand family predisposition• clinical course of concurrentclinical course of concurrent medical illnessmedical illness• nature of any treatmentnature of any treatment• functional disabilityfunctional disability• individual coping styleindividual coping style• social and other supportsocial and other support

Risk Factors - CausalityRisk Factors - Causality
CertainCertain illnesses such (stroke, Parkinson's disease, multiple sclerosis,illnesses such (stroke, Parkinson's disease, multiple sclerosis, and and pancreatic cancer) may cause depression via direct biopancreatic cancer) may cause depression via direct bio mechanisms. mechanisms.
Stroke received most attention, butStroke received most attention, but studies fail to show convincing direct studies fail to show convincing direct aetiologyaetiology

Psychological Consequences of Chronic IllnessPsychological Consequences of Chronic Illness
e.g. Cancere.g. Cancer
• DistressDistress
• Reduced QoLReduced QoL
• Delay seeking helpDelay seeking help FearFear DenialDenial
• Depressed / AnxiousDepressed / Anxious
• Increased somatic complaints (PainIncreased somatic complaints (Pain FatigueFatigue Breathlessness)Breathlessness)
Adjustment Disorder – commonest psychiatric diagnosisAdjustment Disorder – commonest psychiatric diagnosis
Neuropsychiatric complicationsNeuropsychiatric complications
Increased risk of suicide in early stagesIncreased risk of suicide in early stages

Depression in Cancer PatientsDepression in Cancer Patients
• Response to perceived lossResponse to perceived loss
• Awareness of losses to come = bereavementAwareness of losses to come = bereavement
• Loss of body, family, friends, role, lifeLoss of body, family, friends, role, life
• Severe depression X4 likely in cancer patientsSevere depression X4 likely in cancer patients
• 10-20% of cancer patients10-20% of cancer patients

Behavioural Responses to DiagnosesBehavioural Responses to Diagnoses
HedonismHedonism
Put life in orderPut life in order
Premature grieving Premature grieving
Sick RoleSick Role
Illness BehaviourIllness Behaviour
Over-sensitivity to symptomsOver-sensitivity to symptoms
Premature deathPremature death
ADAPTIVE COPINGADAPTIVE COPINGTalk about itTalk about itPlanningPlanningChangesChanges
MALADAPTIVE COPINGMALADAPTIVE COPINGDrinkDrinkEatEatSubstance useSubstance use

Neuropsychiatric ComplicationsNeuropsychiatric Complications
Brain metastases:Brain metastases:
DeliriumDeliriumDementiaDementiaDepressionDepression
Produce psych. symptoms before discoveryProduce psych. symptoms before discovery
• Paraneoplastic SyndromesParaneoplastic Syndromes
Neuropsychiatric problems in absence of metastasesNeuropsychiatric problems in absence of metastases
Orig. lung, ovary, breast, stomach, or Hodgkin’sOrig. lung, ovary, breast, stomach, or Hodgkin’s

Neuropsychiatric syndromesNeuropsychiatric syndromes
• 61 yr old female61 yr old female
• Frontal headaches for 3 months Frontal headaches for 3 months
• Lethargic and weakLethargic and weak
• Difficulty walkingDifficulty walking
• Diffuse areas of nodular destructive Diffuse areas of nodular destructive lesionslesions
• Consistent with multiple myeloma or Consistent with multiple myeloma or metastatic diseasemetastatic disease
• Skeleton is common site for mets from carcinomas and occasionally sarcomas Skeleton is common site for mets from carcinomas and occasionally sarcomas
• Lesions may be “silent” or symptomatic, such as pain, swelling, deformity,Lesions may be “silent” or symptomatic, such as pain, swelling, deformity, compression of the spinal cord, nerve roots, or pathologic fractures. compression of the spinal cord, nerve roots, or pathologic fractures.

Recognition & DiagnosisRecognition & Diagnosis
Often missed in diagnosesOften missed in diagnoses
1.1. Distinguish depressed behaviour (sadness and loss of interest), from Distinguish depressed behaviour (sadness and loss of interest), from realistic expected response to stress / physical illness realistic expected response to stress / physical illness
2.2. Confusion of whether physical symptoms of depression are due to Confusion of whether physical symptoms of depression are due to underlying medical condition underlying medical condition
3.3. Negative attitudes to diagnosis of depression Negative attitudes to diagnosis of depression
4.4. Unsuitability of clinical setting for discussing personal & emotional Unsuitability of clinical setting for discussing personal & emotional mattersmatters
5.5. Patients' unwilling to report symptoms of depressionPatients' unwilling to report symptoms of depression

Recognition & DiagnosisRecognition & Diagnosis
Depressive illness is often under-diagnosed and under-treatedDepressive illness is often under-diagnosed and under-treated
Especially if it coexists with physical illnessEspecially if it coexists with physical illness
This oftenThis often causes great distress for patients: mistakenly assumedcauses great distress for patients: mistakenly assumedthat symptoms (weakness or fatigue) are due to an underlyingthat symptoms (weakness or fatigue) are due to an underlying medicalmedicalcondition. condition.
Practitioners must be able to diagnose and manage depressive illness Practitioners must be able to diagnose and manage depressive illness • Alertness to clues in interviews Alertness to clues in interviews • Patients' manner Patients' manner
Use of screening questions can detect up to 95% of patients with major Use of screening questions can detect up to 95% of patients with major depression. depression.

Screening QuestionnairesScreening Questionnaires
“How have you been feeling recently?” “Have you been low in spirits?” “Have you been able to enjoy the things you usually enjoy?” “Have you had your usual level of energy, or have you been feeling tired?”“How has your sleep been?”“Have you been able to concentrate on your favourite tv shows?”
Self-report screening instrumentsSelf-report screening instrumentsBeck Depression Inventory (BDI) General Health Questionnaire (GHQ)Beck Depression Inventory (BDI) General Health Questionnaire (GHQ)
Hospital Anxiety Depression Scale (HAD)Hospital Anxiety Depression Scale (HAD)
Can’t replace systematic clinical assessment – Can’t replace systematic clinical assessment – LISTENINGLISTENING
Persistent low mood and lackPersistent low mood and lack of interest and pleasure in life cannot be of interest and pleasure in life cannot be accounted for by severeaccounted for by severe physical illness alonephysical illness alone

Non-Specific SymptomsNon-Specific Symptoms
Often missed in assessmentOften missed in assessment

Modern day complaintsModern day complaints
Multiple Chemical SensitivityMultiple Chemical SensitivityChronic Fatigue SyndromeChronic Fatigue SyndromeSick Building SyndromeSick Building SyndromeGulf War SyndromeGulf War SyndromeLow-level Chemical ExposureLow-level Chemical ExposureElectrical SensitivityElectrical SensitivityFibromyalgiaFibromyalgia
Historical complaintsHistorical complaints
Railway SpineRailway SpineNeurastheniaNeurastheniaCombat SyndromeCombat Syndrome
Prevalence of Non-Specific SymptomsPrevalence of Non-Specific Symptoms
SymptomSymptom Prevalence % Prevalence %
Stuffy noseStuffy nose 46.246.2HeadachesHeadaches 33.033.0TirednessTiredness 29.829.8CoughCough 25.925.9Itchy eyesItchy eyes 24.724.7Sore throatSore throat 22.422.4Skin rashSkin rash 12.012.0WheezingWheezing 10.110.1RespiratoryRespiratory 10.010.0NauseaNausea 9.09.0DiarrhoeaDiarrhoea 5.75.7VomitingVomiting 4.04.0
Heyworth & McCaul, 2001Heyworth & McCaul, 2001

Drug Treatment
TricyclicsTricyclicssince the 1950s effective and cheap
limit compliance variable degrees of sedation
fatal in overdose (except Lofepramine)
dose-related anticholinergic side effects postural hypotension
Monoamine Oxidise Inhibitors (MAOI’s)Monoamine Oxidise Inhibitors (MAOI’s)
rare fatalities tyramine-free diet
Selective Serotonin Re-uptake Inhibitors (SSRI’s)Selective Serotonin Re-uptake Inhibitors (SSRI’s)fluoxetine lack sedation no anticholinergic effects
improved compliance less immediate benefit for disturbed sleep
safe in overdose single or narrow range of doses works

Placebo & NoceboPlacebo & Nocebo
In approx. 30% of pop.In approx. 30% of pop.Subjected to more clinical trialsSubjected to more clinical trials than any other medicamentthan any other medicamentNearly always does better thanNearly always does better than anticipatedanticipatedThe range of susceptible conditions seems limitlessThe range of susceptible conditions seems limitlessDoes not always occurDoes not always occurPresent in subjective and objective outcomesPresent in subjective and objective outcomesNegative outcomes can occur (Nocebo effect)Negative outcomes can occur (Nocebo effect)
PlaceboPlaceboBig pills better than smaller pillsBig pills better than smaller pillsRed pills better than blueRed pills better than blue4 pills better than 24 pills better than 230% of pop.30% of pop.

Long Term PrognosisLong Term Prognosis

Identifying Unhelpful Patient BeliefsIdentifying Unhelpful Patient Beliefs
Discuss potential unhelpful beliefsDiscuss potential unhelpful beliefs
Counter any simple aetiological beliefsCounter any simple aetiological beliefs
Outline biopsychosocial perspectiveOutline biopsychosocial perspective
Can highlight potential perpetual factors that inhibit recoveryCan highlight potential perpetual factors that inhibit recovery
Agree on positive open minded approachAgree on positive open minded approach
Do not argue over best name for condition!Do not argue over best name for condition!

Treatment
Much depressive illness of all types is successfully treatedMuch depressive illness of all types is successfully treated in primary carein primary care
Four main reasons for referral to specialist psychiatric services:Four main reasons for referral to specialist psychiatric services:
1)1) Condition is severeCondition is severe
2) Failing2) Failing to respond to treatment (e.g. Psychomotor retardation)to respond to treatment (e.g. Psychomotor retardation)
3) Complicated by other factors (e.g. Personality disorder)3) Complicated by other factors (e.g. Personality disorder)
4) Presents particular risks (e.g. Agitation and psychotic behaviour)4) Presents particular risks (e.g. Agitation and psychotic behaviour)
• Principal decision is whether to treat with drugs or a talkingPrincipal decision is whether to treat with drugs or a talking therapytherapy
• Most patients in primary careMost patients in primary care settings would prefer a talking therapysettings would prefer a talking therapy
• EffectivenessEffectiveness is limited to particular forms of psychotherapyis limited to particular forms of psychotherapy
• Mild-Mod. Depression: CBTMild-Mod. Depression: CBT and antidepressants are equally effectiveand antidepressants are equally effective
• Severe Depression:Severe Depression: antidepressant drugs are more effectiveantidepressant drugs are more effective

Management
The main aims of treatment:The main aims of treatment:• improve mood and quality of lifeimprove mood and quality of life• reduce the risk of medical complicationsreduce the risk of medical complications• improve complianceimprove compliance with and outcome of physical treatmentwith and outcome of physical treatment• facilitate the "appropriate"facilitate the "appropriate" use of healthcare resourcesuse of healthcare resources
PrimaryPrimary care staff should be familiar with properties and use of:care staff should be familiar with properties and use of:1) common antidepressant drugs & brief psychological treatments1) common antidepressant drugs & brief psychological treatments
2) assessment of suicidal thinking and risk2) assessment of suicidal thinking and risk
Patients with more enduring or severe symptoms will usually require specific Patients with more enduring or severe symptoms will usually require specific treatment - usually drug therapytreatment - usually drug therapy
ForFor patients with suicidal ideation / whose depression haspatients with suicidal ideation / whose depression has not responded to not responded to initial management, specialist referral is theinitial management, specialist referral is the next stepnext step

Management
Low level risk Low level risk
Clinical pictureClinical picture ActionAction Suicidal ideation Suicidal ideation Consider referral to mental health Consider referral to mental health but no suicide attempts but no suicide attempts professional for routine appointment professional for routine appointment
(not always necessary)(not always necessary)
Supportive environmentSupportive environmentPhysically healthyPhysically healthyNo history of psychiatric illnessNo history of psychiatric illness

Management
Moderate level risk Moderate level risk
Clinical pictureClinical picture Action Action
Low lethality suicide attempt Low lethality suicide attempt Refer to mental health professionalRefer to mental health professional(patient's perception of lethality) (patient's perception of lethality) to be seen as soon as possibleto be seen as soon as possible
Frequent thoughts of suicideFrequent thoughts of suicidePrevious suicide attemptsPrevious suicide attemptsPersistent depressive symptomsPersistent depressive symptomsSerious medical illnessSerious medical illnessInadequate social supportInadequate social supportHistory of psychiatric illnessHistory of psychiatric illness

Management
High level risk High level risk
Clinical pictureClinical picture ActionAction Definite plan for suicide Definite plan for suicide Refer to mental health professional Refer to mental health professional (When? Where? How?) (When? Where? How?) for immediate assessmentfor immediate assessment
Major depressive disorderMajor depressive disorderHigh lethality suicide attempt or multiple attemptsHigh lethality suicide attempt or multiple attemptsAdvanced medical diseaseAdvanced medical diseaseSocial isolationSocial isolationHistory of psychiatric illnessHistory of psychiatric illness

SummarySummary
• Detection can be hard – symptom overlap and patient unawareDetection can be hard – symptom overlap and patient unaware
• Depression a natural occurrence in populationDepression a natural occurrence in population
• Whole range of depressive conditions with varying severityWhole range of depressive conditions with varying severity
• Depression can be present in acute or chronic statesDepression can be present in acute or chronic states
• Depression can have physiological, biological or social causesDepression can have physiological, biological or social causes
• Depression may have a mixture of causesDepression may have a mixture of causes
• Depression co-exists with many other symptomsDepression co-exists with many other symptoms
• Depression is a natural reaction to disease diagnosis and presenceDepression is a natural reaction to disease diagnosis and presence
• Depression and symptomotology are highly relatedDepression and symptomotology are highly related