Embed Size (px)
Citation preview
J O U R N A L OF ADOLESCENT H E A L T H CARE 1986;7:107-111
Depressive Symptoms and Life Ill Hospitalized Adolescents
Events in Physically
STUART L. KAPLANr M . D . r P A U L A GROSSMANI M . D . I BETH L A N D A r Ph. D. I
I. R O N A L D SHENKER~ M . D . r A N D C H A N T A L W E I N H O L D
To study life events and depressive symptoms in adoles- cents hospitalized for physical illness, we administered the Coddington Life Events Survey and the Beck Depres- sion Inventory (BDI) to 43 acutely ill adolescents, 42 chronically ill adolescents, and 140 adolescents from a general population. There were no differences between the three groups in total BDI, Psychological BDI, and Coddington Life Change Categories adjusted for hospi- talization. The Somatic BDI was significantly greater in the acutely ill and chronically ill than in the general popu- lation sample (p < 0.01). In the chronically ill, the Family Life Change score correlated with the psychological BDI (r = 0.44, p < 0.01) but the Undesirable Life Change score did not. In the acutely ill and the general population, the Undesirable Life Change Score correlated with the Psy- chological BDI (r = 0.44, p K 0.01), (r = 0.43, p K 0.01) but the Family Life Change Score did not.
KEY WORDS"
Depression Life events Physical illness
Cannon (1) observed that changes in emotions can lead to altered physiology and suggested the concept that emotions can precipitate physical illness. Based on Cannon's work, life event research has become an important area of study regarding the relationship between psychological variables and the onset of physical and psychiatric illness (1,2). Life events
From the Departments of Psychiatry and Pediatrics of the Long Island Jewish-Hillside Medical Center, Schneider Children's Hospital, New Hyde Park, New York.
Address reprint requests to: Stuart L. Kaplan, M.D., Rockland Chil- dren's Psychiatric Center, Convent Road, Orangeburg, NY 10962.
Manuscript accepted June 11, 1985.
such as marriage, divorce, births, job promotion, and moves necessitate change or reorganization of an individual's life, which may lead to stress. Stress may alter physiological states in such a way that the likelihood of becoming physically or psychiatrically ill is increased. According to Holmes and Rahe (3) and Dohrenwend (4), whether a life event is desir- able or undesirable is unrelated to whether that event may precipitate an illness because all life events require some interpersonal reorganization on the part of the individual. Most studies of life events in adults have found a minor (r = 0.12-0.3) rela- tionship between life events and physical illness (2).
Heisel et al. (5) and Coddington (6) used the Life Events Scale to study life events in general adoles- cent, general pediatric, and hospitalized pediatric samples, and in a mixed group of children and ado- lescents aggregated by diagnosis. They found more life change units in the hospitalized pediatric sam- ple, in hemophilliac children and adolescents with frequent bleeding episodes, in children and adoles- cents admitted for surgery, and in adolescent psychi- atric patients than in the general population sample.
Because of the lack of studies of life events and physical illness in hospitalized adolescents, we de- signed a study to compare the frequency and quality of life events in a hospitalized adolescent sample and in a general adolescent control group and to examine the relationship between life events and depressive symptoms in both groups. We hypothesized that hospitalized adolescents would have more life events than a nonhospitalized sample, and that hos- pitalized physically ill adolescents would have more depressive symptoms than nonhospitalized adoles- cents because physical illness and hospital confine- ment would be important undesirable life events.
© Society for Adolescent Medicine, 1986 107 Published by Elsevier Science Publishing Co., Inc., 52 Vanderbilt Ave., New York, NY 10017 0197-0070/86/$3.50

108 KAPLAN ET AL. JOURNAL OF ADOLESCENT HEALTH CARE Vol. 7, No. 2
Materials and Method
The Coddington Life Events Scale is a 50-item self- report life event instrument developed and stan- dardized for children and adolescents (7). The instru- ment provides three direct category scores: 1) Family Life Events, which inquire about the death, divorce, hospitalization, and change in job and income of family members; 2) Desirable Life Events, which in- clude items such as winning a prize, getting a sum- mer job, and graduating from high school; and 3) Undesirable Life Events, which include breaking up with a girlfriend or boyfriend, failing a grade in school, and hospitalization. We followed Cod- dington's instructions for the computation of these category scores. The frequency of individual life events was multiplied by weights established by Coddington to produce a life change unit raw score, which provides a measure of the social reorganiza- tion required by the life event. The raw scores are summed by Coddington's categories and then con- verted to standard scores based on norms developed by Coddington in a s tudy of 748 adolescents (7).
The Beck Depression Inventory (BDI) is a widely used and well-studied clinical and research self-ad- ministered measure of depression (8-11). The BDI consists of 21 questions with a 0 response if the de- pressive symptom is not present, a i if the symptom is present, and a 2 or 3 if the symptom is severe. The total BDI score is the sum of the individual items. The higher the score the greater the amount of depressive symptoms. Standard cut-off points are: 0-9, non- depressed; 10-15, mild depression; 16-23, moderate depression; 24+ severe depression. The BDI can be divided into two subscales: psychological (BDI items 1-13) and somatic (BDI items 14-21). Because the symptoms of physical illness can be identical with some of the physiological symptoms of depression, we employed these subscales to minimize confound- ing the symptoms of physical illness and depression.
One hundred forty-five adolescents who were consecutively admitted to an adolescent medicine in- patient unit were invited on admission to complete the BDI and the Coddington Life Events Scale. Twenty-one of the hospitalized adolescents refused to participate in the study because they felt too ill or regarded the inventories as "too personal." Thus we had 124 clinical subjects. The adolescents were in- structed to complete the Coddington based on their life events during the preceding six months.
A junior and a senior high school near the hospital were chosen to provide an adolescent control sample
that would provide an approximate match for age and social class with the hospitalized sample. On the basis of meetings with the principals and school counselors, classes were selected to meet our esti- mate of the age and subject number required for our study. Two classes from each of the three grades (seventh, eighth, and ninth) were chosen by the principal based on his estimate of the teachers' will- ingness to participate. One science class from each of the tenth, eleventh, and twelfth grades was chosen because it was thought that science students might have an interest in participating in the study.
Letters describing the study and consent forms were distributed to the students and had to be re- turned signed by the parent and child prior to the distribution of the questionnaires. Of the 272 consent forms distributed, 168 were signed and returned. Of 104 students who did not return the consent forms, two parents refused to allow their children to partici- pate. We have no data for the reasons the remaining students did not return the signed consent forms. During class time set aside for the research project, a research assistant distributed the questionnaires, the students filled them out, and the research assistant collected them. During the data analysis, 28 subjects of our 168 were excluded from the study because of missing data, leaving us with a total of 140 subjects in the control sample.
Because some forms of chronic illness may be as- sociated with a decreased number of life events as a result of a restricted life style (5), the hospitalized adolescents were divided into two illness groups, acute and chronic, to test for differences in the fre- quency of life events and depressive symptoms.
Chronic illness was defined as being ill for four months or longer (n = 42) based on chart review, and acute illness was defined as being ill for one month or less (n = 43) based on chart review. Those ill for one to four months were not considered further in the data analysis (n = 39).
Because of the wide variety of illnesses in the hos- pitalized sample, we were unable to categorize the illnesses easily. Illustrative of the diagnoses found in the acutely ill were 11 cases of infection, one new leukemia, seven trauma, two pregnancy complica- tions, and one new diabetic. Representative of the diagnoses of the chronically ill group were one cystic fibrosis, four oncology, one diabetic, one ulcerative colitis, and one sickle cell anemia.
Results In the analysis of the differences between the groups based on the demographic variables, there were no
MARCH 1986 DEPRESSIVE SYMPTOMS AND LIFE EVENTS 109
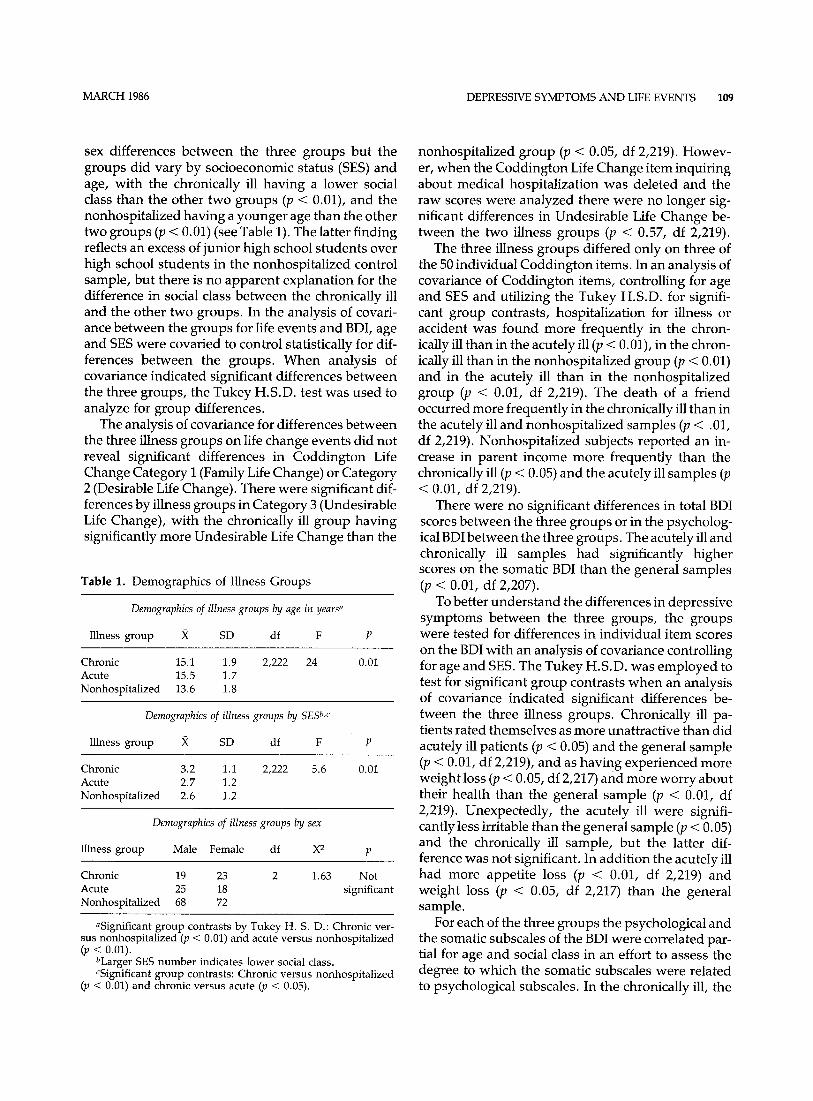
sex differences between the three groups but the groups did vary by socioeconomic status (SES) and age, with the chronically ill having a lower social class than the other two groups (p < 0.01), and the nonhospitalized having a younger age than the other two groups (p < 0.01) (see Table 1). The latter finding reflects an excess of junior high school students over high school students in the nonhospitalized control sample, but there is no apparent explanation for the difference in social class between the chronically ill and the other two groups. In the analysis of covari- ance between the groups for life events and BDI, age and SES were covaried to control statistically for dif- ferences between the groups. When analysis of covariance indicated significant differences between the three groups, the Tukey H.S.D. test was used to analyze for group differences.
The analysis of covariance for differences between the three illness groups on life change events did not reveal significant differences in Coddington Life Change Category I (Family Life Change) or Category 2 (Desirable Life Change). There were significant dif- ferences by illness groups in Category 3 (Undesirable Life Change), with the chronically ill group having significantly more Undesirable Life Change than the
Table 1. Demographics of Illness Groups
Demographics of illness groups by age in years ~
Illness group X SD df F P
Chronic 15.1 1.9 Acute 15.5 1.7 Nonhospitalized 13.6 1.8
2,222 24 0.01
Demographics of illness groups by SES b,c
Illness group X SD df F P
Chronic 3.2 1.1 Acute 2.7 1.2 Nonhospitalized 2.6 1.2
2,222 5.6 0.01
Demographics of illness groups by sex
Illness group Male Female df X 2 p
Chronic 19 23 2 1.63 Not Acute 25 18 significant Nonhospitalized 68 72
aSignificant group contrasts by Tukey H. S. D.: Chronic ver- sus nonhospitalized (p < 0.01) and acute versus nonhospital ized (p < O.Ol).
bLarger SES number indicates lower social class. cSignificant group contrasts: Chronic versus nonhospital ized
(p < 0.01) and chronic versus acute (p < 0.05).
nonhospitalized group (p < 0.05, df 2,219). Howev- er, when the Coddington Life Change item inquiring about medical hospitalization was deleted and the raw scores were analyzed there were no longer sig- nificant differences in Undesirable Life Change be- tween the two illness groups (p < 0.57, df 2,219).
The three illness groups differed only on three of the 50 individual Coddington items. In an analysis of covariance of Coddington items, controlling for age and SES and utilizing the Tukey H.S.D. for signifi- cant group contrasts, hospitalization for illness or accident was found more frequently in the chron- ically ill than in the acutely ill (p < 0.01), in the chron- ically ill than in the nonhospitalized group (p < 0.01) and in the acutely ill than in the nonhospitalized group (p < 0.01, df 2,219). The death of a friend occurred more frequently in the chronically ill than in the acutely ill and nonhospitalized samples (p < .01, df 2,219). Nonhospitalized subjects reported an in- crease in parent income more frequently than the chronically ill (p < 0.05) and the acutely ill samples (p < 0.01, df 2,219).
There were no significant differences in total BDI scores between the three groups or in the psycholog- ical BDI between the three groups. The acutely ill and chronically ill samples had significantly higher scores on the somatic BDI than the general samples (p < 0.01, df 2,207).
To better understand the differences in depressive symptoms between the three groups, the groups were tested for differences in individual item scores on the BDI with an analysis of covariance controlling for age and SES. The Tukey H.S.D. was employed to test for significant group contrasts when an analysis of covariance indicated significant differences be- tween the three illness groups. Chronically ill pa- tients rated themselves as more unattractive than did acutely ill patients (p < 0.05) and the general sample (p < 0.01, df 2,219), and as having experienced more weight loss (p < 0.05, df 2,217) and more worry about their health than the general sample (p < 0.01, df 2,219). Unexpectedly, the acutely ill were signifi- cantly less irritable than the general sample (p < 0.05) and the chronically ill sample, but the latter dif- ference was not significant. In addition the acutely ill had more appetite loss (p < 0.01, df 2,219) and weight loss (p < 0.05, df 2,217) than the general sample.
For each of the three groups the psychological and the somatic subscales of the BDI were correlated par- tial for age and social class in an effort to assess the degree to which the somatic subscales were related to psychological subscales. In the chronically ill, the
110 KAPLAN ET AL. JOURNAL OF ADOLESCENT HEALTH CARE Vol. 7, No. 2
somatic and psychological BDI subscales correlated r = 0.72, p ( 0.001; in the acutely ill the correlation was r = 0.68, p ( 0.001. Thus, somatic symptoms of de- pression and psychological symptoms of depression were highly related in all samples.
The Coddington Life Change categories Family Life Change, Desirable Life Change, and Undesir- able Life Change were correlated with the psycho- logical subscale of the BDI. In the chronically ill, Fam- ily Life Change correlated significantly with the psychological BDI (r = 0.44, p ( 0 . 0 1 ) but did not correlate in the acutely ill (r = 0.19, not significant) and nonhospitalized (r = 0.19, p ( 0 . 0 5 ) samples.
Undesirable Life Change correlated significantly with the psychological BDI in the acutely ill (r = 0.44, p (0 .01) and nonhospitalized samples (r = 0.43, p ( 0.01) but did not correlate significantly in the chron- ically ill. Desirable Life Change did not correlate sig- nificantly with the psychological BDI in the three samples.
Discussion The diagnosis of depression in physically ill adoles- cents is complicated by the similarity between the somatic symptoms of depression, such as sleep- lessness, irritability, and weight loss, with those symptoms in physical illness. The question of assess- ing whether these symptoms are expressions of de- pression or physical illness is often a vexing one for the physician attempting to establish a diagnosis of depression using the DSM III criteria (12).
Our data reflect this clinical difficulty. As ex- pected, the physically ill sample had more somatic symptoms than our general sample. Because there were no differences in total BDI between the three groups, the likely explanation for the increase in somatic symptoms of depression in the physically ill sample is that their somatic symptoms were related to their physical illness. On the other hand, there were strong correlations between somatic symptoms of depression and psychological symptoms of de- pression in both the physically ill and general sam- pies. This suggests that the somatic symptoms are strongly related to the psychological symptoms of depression in all three samples as well as to physical illness in the hospitalized samples. A longitudinal study of a hospitalized population to include the re- peated administration of the BDI during and after hospitalization along with the biological measures of physical illness as dependent variables might clarify the amount of variance in somatic symptoms of de- pression explained by physical illness versus that ex- plained by depressive symptoms in the physically ill.
Although early clinical studies of chronically ill children and adolescents suggested that they were burdened with a variety of psychological difficulties in excess of what would be expected in a general population, more recent and better controlled stud- ies do not support this clinical assumption (13-16). For example, Kellerman et al. (13) and Zeltzer et al. (14) in a study of 345 adolescents from a general pop- ulation and 168 mostly outpatient adolescents with a variety of serious chronic illnesses found no dif- ferences in self esteem and anxiety between the two groups. The general adolescent sample in the above study complained of as much disruption in their lives from minor illnesses such as colds as did the chron- ically ill with their serious illnesses. Our findings are consistent with these more empirical studies.
Furthermore, our data suggest that life changes are probably not more frequent in the six months preceding hospitalization of acute and chronically ill adolescents than in a general adolescent sample. Even categorizing life change items into Desirable, Undesirable, and Family Life Change Categories did not reveal significant differences between groups.
The lack of a correlation between Desirable Life Changes and depressive symptoms in our three sam- ples is consistent with the adult studies that report an absent or weak inverse relationship between positive life changes and depressive symptoms (17-21). These same studies report a strong correlation be- tween depressive symptoms and undesirable life changes. The significant correlations we found be- tween the Coddington Undesirable Life Event Cate- gory and the Psychological BDI in the acutely ill and general sample are supported by similar findings in adults. In our chronically ill subjects, the lack of a correlation between the Coddington Undesirable Life Change Category and psychological BDI was an unexpected negative finding, which is discussed below.
The interpretation of the correlations between the psychological BDI and the Family Life Change Cate- gory and the psychological BDI and the Undesirable Life Change Category in the chronically ill may re- quire a more detailed understanding of these two Coddington categories. The Family Life Change Cat- egory is composed of 17 items; 12 are aversive, or "undesirable," widely regarded as causing psycho- logical pain to adolescents. These items include: death of a grandparent, parent, or sibling; divorce or separation of a parent; and hospitalization of a par- ent or sibling. Because desirable life changes are un- related to depressive symptoms, the positive correla- tion between the Family Life Change Category and

MARCH 1986 DEPRESSIVE SYMPTOMS AND LIFE EVENTS 111
the psychological BDI in the chronically ill is proba- bly due to the correlation of aversive or "undesir- able" family life events in the Coddington Family Life Change Category with the psychological BDI.
The Coddington Undesirable Life Change Catego- ry refers to life changes that are aversive but are mostly not related to the family, such as failing a grade in school, drug abuse, and breaking up with a boyfriend or girlfriend.
The high correlation between the Family Life Change Category and the psychological BDI in the chronically ill and the lack of correlation between these two variables in the acutely ill and nonhospital- ized sample raise the question as to whether the chronically ill are more sensitive to events in their family than are the other two samples. Perhaps chronic illness makes adolescents closer to or more dependent on their families, and thus more vulnera- ble to the vicissitudes of family life.
We gratefully acknowledge the help of Cheryl Weston, R.N. and the many other nurses of Adolescent Medicine, Long Island Jew- ish-Hillside Medical Center, who assisted in our data collection.
References 1. DohrenwendBS, DohrenwendBP. Abriefhistoricalintroduc-
tion to research on stressful life events. In: Dohrenwend- Dohrenwend, eds. Stressful life events: Their nature and ef- fects. New York, John Wiley & Sons, 1974:1-5.
2. Rabkin JG, Struening EL. Life events, stress and illness. Sci- ence 1976;194:1013-20.
3. Holmes TH, Rahe RH. The social readjustment rating scale. Psychosom Res 1967;11:213-8.
4. Dohrenwend BS. Social class and stressful events. In Psychi- atric epidemiology: Proceedings of the international sym- posium held at Aberdeen University, July 22-25, 1969. New York, Oxford University Press, 1970:313-19.
5. Heisel JS, Ream S, Raitz R, Rappaport M, Coddington RD. The significance of life events as contributing factors in the diseases of children. III. A study of pediatric patients. J Pediatr 1973,83:119-23.
6. Coddington RD. The significance of life events as etiologic factors in the diseases of children. I. A survey of professional workers. J Psychosom Res 1972a;16:7-18.
7. Coddington RD. Life events scale adolescent scoring manual. 1979 (unpublished).
8: Beck AT. Depression: Clinical, experimental and theoretical aspects. New York, Harper & Row, 1967.
9. Bumberry W, Oliver JM, McClure JN. Validation of the Beck Depression Inventory in a university population using psychi- atric estimate as the criterion. J Consult Clin Psychol 1978; 46:150-5.
10. Strober M, Green J; Carlson G. Utility of the Beck Depression Inventory with psychiatrically hospitalized adolescents. J Consult Clin Psychol 1981;49:482-3.
11. Plumb MJ, Holland J. Comparative studies of psychological function in patients with advanced cancer. I. Self-reported depressive symptoms. Psychosom Med 1977;39:264-76.
12. Waller DA, Rush AJ. Differentiating primary affective disease, organic affective syndromes and situational depression on a pediatric service. J Am Acad Child Psychiatry 1983;22:52-8.
13. Kellerman J, Zeltzer L, Ellenberg L, Dash J, Rigler D. Psycho- logical effects of illness in adolescence: I. Anxiety, self-esteem and perception of control. J Pediatr 1980; 97:126-31.
14. Zeltzer L, Kellerman J, Ellenberg L, Dash J, Rigler D. Psychol- ogic effects of illness in adolescence. II. Impact of illness in adolescents--crucial issues and coping styles. J Pediatr 1980;97:132-38.
15. Bedell JR, Giordani B, Amour JL, Travormina J, Boll T. Life stress and the psychological and medical adjustment of chron- ically ill children. J Psychosom Res 1977;21:237-42.
16. Tavormina JB, Kastner LS, Slater PM, Watt SL. Chronically ill children. J Abnorm Child Psychol 1976; 4:99-110.
17. Finlay-Jones R, Brown GW. Types of stressful life events and the onset of anxiety and depressive disorders. Psychol Med 1981;11:803-15.
18. Lloyd C. Life events and depressive disorder reviewed. II. Events as precipitating factors. Arch Gen Psychiatry 1980;37:541-548.
19. Grant I, Sweetwood, HL, Yager J, Gerst M. Wuality of life events in relation to psychiatric symptoms. Arch Gen Psychia- try 1981;38:335-9.
20. Vinokur A, Seizer ML. Desirable versus undesirable life events: Their relationship to stress and mental distress. J Pers Soc Psychol 1975;32:329-37.
21. Paykel EJ, Myers JK, Dienelt MN, Klerman CL, Lindonthal JJ, Pepper MP. Life events and depression: a controlled study. Arch Gen Psychiatry 1969;21:753-60.