Embed Size (px)
Citation preview

Dermal manifestations in VIRAL diseases in children
DR BINOD KUMAR SINGH Associate Professor, NMCH, Patna CIAP Executive Board Member 2015 NNF State President-2014 IAP State Secretary ,Bihar 2010-2011 NNF State Secretary , Bihar 2008-2009
Chief Consultant:- Shiv Shishu Hospital K- 208 P C Colony ,Hanuman Nagar, Patna 800020. Email- [email protected] web site :- www.shivshishuhospital.com

IN HISTORY TAKING :a) Exposures
- Viral diseases (home, day care…)- Travelling history-Pets, insects- Medications and drugs- Immunization
b) Features of rash- Temporal association (onset relative to fever)- Progression and evolution- Location and distribution- Pain or pruritus

• IN PHYSICAL EXAMINATION :a) Distribution pattern
- symmetrical- asymmetrical
b) Morphology- monomorphic- pleomorphic
c) Configuration- linear,
- annular, - grouped, -discrete

Macule PapuleFlat spots, not palpable
Elevated, palpable, small rounded lesions

Vesicles Pustules
Small, fluid-filled blistersSmall blisters containing purulent fluid

HERPES VIRUS GROUP
• Double stranded DNA virus• Latent but life long infection
HERPES SIMPLEX :HSV-1:-Orolabial herpes (most prevalent)HSV-2:-Genital herpes (after attaining sexual
activity)

OROLABIAL HERPES • C/F:- <1 % of patient develop HERPITIC
GINGIVOSTOMATITIS(mostly are children and young adults )• Asso with high fever, regional lymphadenopathy & malaise • Pain, foul breath, dysphagia & pharyngitis.• Diagnosis :- C/F –Typical vesicular lesons at the lips
virus isolation by cell culture PCR
• Treatment : Acyclovir 15mg/kg 5 times daily for 7 days.• Precaution:- Sunblock should be applied.
Dental & Surgical procedures should be done with utmost care

OROLABIAL HERPES ,TRIGGERED BY SUNBURN

•
HERPETIC GINGIVOSTOMATITIS Broken vesicles that appear as erosion or ulcers covered with white membrane spreads to oral mucosa, tongue and tonsils.

HSV-1,EYELID INFECTION CAUSED BY A KISS FROM INFECTED PERSON

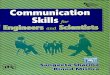
HERPETIC WHITLOW• Causative organism:-HSV-1• Age:-<10 years• Thumb sucking and nail biting by infected patients.• C/F:-lesions begin with tenderness &
erythema,usually of lateral nail fold or on the palm After 24-48 hrs- deep seated blisters develop
• Mimics cellulitis:- swelling of affected hand, lymphatic streaking & swelling of epitrochlear& axillary LN

Caused due to finger sucking.

NEONATAL HERPES • Causative organism:-HSV-2(70%)
HSV-1 (Contact with orolabial herpes)• Occurrence rate:- 85% -time of delivery
10-15%-non-maternal sources after delivery 5%- inutero with intact membrane
• Inutero infection:-foetal anamolies, limb hypoplasia, microcephaly,microphthalmus,encephalitis,chorioretinits,intracelebral calcification.
• Prenatally acquired neonatal herpes has 3 types :- A) localized infection of skin, eye or mouth(SEM)
B) CNS disease C) Disseminated disease-encephalitis,hepatitis,pneumonia, coagulopathy.

Limb hypoplasia with herpetic lesion

• FATAL OR PERMANENT NEUROLOGICAL SEQUELAE• Diagnosis:-Viral culture, DFA Staining of material from skin or ocular lesion.• Treatment:- IV Acyclovir-60 mg/kg/day
14 days (SEM)21days (CNS)
• PREFERRED CAESEREAN SECTION• Scalp electrodes and Vaccum delivery should be avoided .

NEONATAL HERPES ASSOCIATED WITH SCALP ELECTRODES

VARICELLA/CHICKENPOX•Caustative Organism: VaricellaZoster Virus•IP:-10-21 days•Mode of transmission:- aerosols•Infectivity period:-From 5days before to 5days after eruption•C/F:-Tear drop vesicles on erythematous base (dew drop on rose petal)Pleomorphic in nature.Initially macules, that develop into vesicles within 24hrs.•Site :- trunk, face & oral mucosa•Complications:-Sec. bacterial infection Cerebellar ataxia & encephalitis Reye syndrome:-hepatitis with acute encephalopathy caused by use of aspirin & other salicylates.

VARICELLA COMPLICATED WITH BULLOUS IMPETIGO

• Diagnosis :- Clinical manifestation Tzanck smear DFA test
• Treatment :-Acyclovir 20mg/kg 4 times a day (max. dose being 800mg)
• Prevention:- Live attenuated varicella vaccine » 1st dose -12-15 months 2nd dose -4-6 yrs.ZIG

CONGENITAL VARICELLA SYNDROME• Caused by Maternal infection –
in first 20 weeks of GA• Females are affected more• C/F:-Hypoplastic limb –usually
unilateral and lower extremity Cicatrical skin lesions Ocular disease-
microphthalmous, nystagmus, chorioretinitis, hypoplasia& atrophy of optic disc, congenital cataract &Horner syndrome
CNS- cortical atrophy ,
ventriculomegaly, MR, learning disabilities.

MODIFIED VARICELLA LIKE SYNDROME
• Occurs in previously immunized patients leading to reduced severity on exposure to natural varicella
• C/F:-mostly macules and papules ,with fewer
vesicles. average no.-35-50(unlike
300)

VARICELLA IN IMMUNOCOMPROMISED
• Severe and Fatal.• Lesions are ulcerative,
necrotic, hyperkeratotic .

HERPES ZOSTER/SHINGLES• Rare below 1yr.Caused by
intrauterine VZV or VZV exposure in 1st few yrs.
• Occurs due to reactivation of VZV in sensory dorsal root ganglion.
• Site:-Thoracic(55%), Cranial (20%) ,Lumbar(15%), Sacral (5%)
• C/F:- Pain in affected area precede or coincide with papule or plaque of erythema in a dermotome,
• within hours blisters develop

Ophthalmic zoster• Ophthalmic div. of 5th CN• Hutchison’s sign:-external div.
of nasocilliary branch involved leading to vesicles on side &tip of nose
• Ocular involvement:- uveitis(92%),keratitis(50%)
• Complications:- Ramsay hunt synd-7th &8th CN involvement
• S3 orS2 involvement:-acute urinary retention, heamaturia & pyuria
• Treatment-Bed rest,Hot fomentation,Acyclovir

INFECTIOUS MONONEUCLOSIS• Causative Organism:-Epstein Barr Virus • Mode of transmission:-oral secretions,
orogenital sex or hematogenous route also.
• IP:-3-7weeks
• C/F:-fever,headache,lymphadenopathy,splenomegaly,pharyngitis
• In mucous membrane-pinhead sized petechiae 5-20 in no.at the junc.of soft and hard palate=FORCHHEIMER’S SPOTS
• Treatment:-Acyclovir is ineffective. Prednisolone can be given in pharygeal
encroachment on the airway.

INFECTIOUS MONONUCLEOSIS

GIONOTTI-CROSTI SYNDROME/PAPULAR ACRODERMATITIS OF CHILDHOOD/PAPULOVESICULAR ACROLOCATED SYNDROME
• Causative organism:-EBV-MC (previously HBV) adenovirus,
CMV,enterovirus,rotavirus,Hep A &C,Parainfluenza virus,ParvovirusB19
Immunization against :-Poliovirus,diptheria,pertussis,JE,influenza,hepB,measels.
• Age:-6mo-14 yrs • Chuh proposed diagnostic criteria :-
i)monomorphous flat topped,pink brown,papules or papulovesciles of 1-10mm in diameter
ii)any 3 or 4 sites involved-face,buttocks,forearms,extensor legs
iii)symmetry iv)duration of atleast 10 days Negative Clinical features:- i)Extensive truncal lesions ii)Scaly lesionsMucous membrane spared.• Treatment :- NONE .self limiting.

CYTOMEGALIC INCLUSION DISEASE • Caustative organism:-Cytomegalo virus • 90% pts are asymptomatic• C/F:-cutaneous lesions are caused by
thrombocytopenia with resultant petechiae, purpura & ecchymoses
• Purpuric violaceous lesions(macular,papular or nodular)show extrameduallry hematopoeisis(dermal erythropoeisis)producing “BLUEBERRY MUFFIN BABY”
• Asso. with jaundice, hepatosplenomegaly, cerebral calcification,choriretinitis,
microcephaly , MR,deafness.• Treatment :-regresses in 1st 6 wks of
life so no treatment required.

ROSEOLA INFANTUM(EXANTHEM SUBITUM,6TH DISEASE)
• Causative organism:-HHV-6, HHV-7(Human herpes virus)
• Common cause of sudden,unexplained high fever in young children btw 6-36 months.
• C/F:-Prodromal-high fever,convulsions& lymphadenopathy.
On 4th day:-fever drops & morbilliform erythema consisting of rose coloured discrete macules on neck,trunk,buttocks.
Blanchable halo around the lesion. Mucous memb spared.• Treatment :- complete resolution
in 1-2 days so no treatment required.

MOLLUSCUM CONTAGIOSUM• Causative organism:-MCV 1-4,MCV-1-MC in
children,MCV-2-In HIV
• Mode of transmission:-direct skin to skin contact,spc if skin is wet
• .• C/F:-smooth surfaced, firm,dome
shaped,pearly papules,3-5mm in diam. “CENTRAL UMBILICATION” is characteristic. Giant lesion=1.5 cm in diam
• Site:-face,trunk & extremeties. If only genital involvement is there consider
sexual abuse.Spontaneous resolution,individual lesions lasts 2-
4mo,duration of infection is 2 yrs.
• Treatment:-Topical Tretinoin,5% Na nitrite+5% salicylic acid or Catharidin, nicking ,cryotherapy, TCA(Trichloroacetic acid)

HERPANGIA
• Causative Organism:-Coxsackievirus(A8,A10&A16),Echovirus,Enterovirus71
• C/F:-fever,headache,sore throat,dysphagia,anorexia.
->1 or more yellowish-white,slightly raised 2 mm vesicles in throat,usually surrounded by an intense areola,seen in ant.faucial pillars,tonsils,uvula,soft palate.
- they ulcerate,leaving a shallow punched out grayish-yellow crater2-4mm in diam
• Treatment:-it disappears in 5-10days.
Supportive treatment-Topical Anaesthetics.

HAND FOOT MOUTH DISEASE• Age:-2-10yrs• C/F:-Begins with Fever,sore mouth.
• Oral lesions- small 4-8mm,rapidly ulcerating vesicles surrounded by red areola on the buccal mucosa,tongue,soft palate & gingiva.
• Hand & Foot lesions-asymptomatic red papules that quickly become small,gray 3-7mm vesicles surrounded by red halo.
oval, linear or crescentric.
• Treatment:--Resolves in a week -Oral topical anaesthetics.

MEASELS/RUBEOLA• Causative organism:-Paramyxovirus• Age:-mostly <15 mon.• Mode of transmission:-aerosol• IP:-9-12days• C/F:-Prodrome-fever,malaise,conjunctivitis
&upp. Resp. sympt.(nasal congestion,sneezzing,coryza,cough)
After 1-7 days-exanthem appears usually macular,morbilliform lesion on ant. Scalp line &behind ears.
2nd day-trunk & extremeties3rd – 4th day-whole body involved6th-7th day-exanthem clearsKOPLIK’S SPOTS:-appear 1st on buccal mucosa
nearest to lower molar as 1mm white papules on erythematous base.
• Complication:-otitis media, pneumonia, encephalitis,thrombocytopenic purpura.
• Treatment:-Bed rest, analgesics, anti-pyretics. Vit A reduces morbidity & mortality.

MACULAR RASH
KOPLIK SPOTS
CONJUNCTIVITIS

RUBELLA/GERMAN MEASELS• Causative Organism:-Togavirus• Mode of transmission:-aerosols• IP:-12-23 days• C/F:-Prodrome-fever,malaise,sore
throat,eye pain,headache,red eyes,runny nose& adenopathy
Characteristic-pain on lateral & upward eye movement.
Cut. Lesions begin on face& progress caudal,covers the entire body in 24hrs,typically pale pink,morbilliform macules smaller than measles.
Resolves on 3rd day.Forchheimer’s sign:pinhead size red
macules or petechiae on soft palate & uvula
Post.cervical, suboccipital &postauricular lymphadenitis=>50% cases
• Diagnosis:-Rubella specific Ig M or PCR

CONGENITAL RUBELLA SYNDROME• Infants born to mothers
infected in 1st trimester.• C/F:-cong.catarct,cardiac
defect&deafnessCutaneous lesion :-
thrombocytopenic purpura, hyperpigmentation of navel, forhead & cheeks,infiltrated 2-8 mm lesions(BLUEBERRY MUFFIN TYPE) which represent dermal erythropoeisis,chronic urticaria&reticulated erythema of face & extremities.

ASSYMETRIC PERIFLEXURAL EXANTHEM OF CHILDHOOD/APEC
• Unilateral laterothoracic exanthem• Causative organism:-unkown,Parvovirus
B19 is speculated• Girls>boys• Age:-8mo-10yrs• Time:-late winter,early spring• C/F:-Prodrome-URTI,GIT infect.Cutaneous lesion:Discrete 1mm erythematous
papules, morbilliform plaque,mild pruritis. Starts unilaterally close to flexural area usually Axilla(75%). Normal skin may intervene
After 5-15days:Contralateral side may get involved(70%)
Lymphadenopathy-70%• Treatment:-Resolves in 2-6 wks.Oral antihistaminic for pruritis.

ERYTHEMA INFECTIOSUM/5TH DISEASE• Causative Organism:-Parvovirus• Time:-late winter,early spring• IP:-4-14days• C/F:-Prodrome-headache,runny
nose,low grade fever• 3 phases:- 1st:abrupt asympt. Erythema of
cheeks called slapped cheek(butterfly pattern)
2nd: prox. Extremities, trunk (After 1-4 days)
3rd:recurring,after exposure to heat,bathing,sunlight or crying & exercise
• Treatment:-Self limiting

PAPULAR PURPURIC GLOVES & SOCKS SYNDROME• Causative organism: Parvovirus• Age:-teenagers• C/F:-Pruritis,oedema,erythema
of hand and feet sharply cut off at wrist &feet.
Cheeks,elbows,knees &groin folds may also be involved.
Oral erosions-shallow ulceration,aphthous ulcers on labial mucosa,erythema of pharynx,Kopliks spot
Lips may be red &swollen.Vulvar oedema &dysuria may also
be seen.• Treatment :-Self limiting ,
resolves within 2 wks.

DENGUE• Causative organism:Arbovirus• Vector:-Aedes mosquitoes• IP:-2-15days• C/F:-sudden onset of high
fever,myalgia,retro-orbital pain,severe backache(BREAKBONE FEVER)
Cutaneous lesion-After 3 -5days of defervescence.
Morbilliform,confluent, characterestically small islands of normal skin-”islands of white in sea of red”
Facial flushing prominent.Cutaneous hemorrhage:DHF or DSS • Diagnosis:-Dengue specific IgM ELISA• Treatment:-Recovery in 7-10 days.

CHIKUNGUNYA• Causative organism:-Arbovirus• Vector:-Aedes mosquitoe• IP:-2-7 days• C/F:-morbilliform ,affects arms,upper
trunk &face. Confluent & island of sparing can be seen.
By 2nd day >1/2 of pts. are affected.In acute illness ecchymoses can be seen.In<1yr pt.-bullous eruption can be seen
which become hemorrhagic later. Nikolsky sign is +ve.
Resembles TEN, more than 80% of body surface becomes denuded.
• Diagnosis:-IgM,PCR• Treatment:-like burn pts.

VERRUCA VULGARIS/COMMON WART• Causative organism:-HPV-1,2,4,27,57
&63• Age:-5-20yrs• Risk factors:frequent immersion oh
hands in water• Site:-finger & palmsBy autoinoculation in nail biters to tongue
& lips• Lesion:-pinpoint to >1cm,avg about
5mm,rounded papules with rough grayish surface,grows in size for wks to mon.,tiny black dots may be visible representing thrombosed,dilated capillaries.
• Treatment :-Electrodissection, Ablative laser,Cryotherapy,keratolytic sol. (16.7%lactic acid or salicylic acid)

VERRUCA PLANA/FLAT WARTS• Causative organism:-HPV 3,10,28
& 41• Age:-children & young adults• Risk factors:-sun exposure &
swimmers• Lesion:-2-4mm flat topped
papules,slightly erythematous brown papule on pale skin & hyperpigmented on darker skin.Kobner’s pheno is seen.
• Site:-face,neck,dorsum of hands & wrists,elbows & knees.
• Treatment:-highest rate of spontaneous remission.
Chemical cautery or light electrodissection is successful.

VERRUCA PLANTARIS/PLANTAR WARTS• Causative organism:-HPV
1,2,4,27,57• Site:-Pressure points. on balls of
foot,esp. over the mid-metatarsal area
• Lesion:-painful,gray coloured,rounded,single or multiple,rough to feel,surrounded by collar of thick skin.
• Diagnosis:-Paring of the surface shows black dots unlike in corns
• Treatment:-Paring & 20-40% salicylic acid,16.7% of lactic acid or salicylic acid .

HIV/AIDS• Mode of transmission:-Intrauterine(25%), Intrapartum(70%),
Postpartum(5%)• Early mucocutaneous manifestation:-unresponsive or
relapsing candidiasis,molluscum contagiousum,warts,herpes,recurrent infection with pyogenic bacteria,dermatophytosis & scabies.
• Staging:-STAGE 1:asymptomatic,persistent generalised lymphadenopathySTAGE 2:hepatosplenomegaly,Papular pruritic
eruptions,seborrheic dermatitis,extensive wart virus infection,extensive molluscum contagiousum, fungal nail infections,recurrent oral ulceration,lineal gingival erythema,angular chelitis,hepes zoster,partotid enlargement,rec. chronic URTIs

STAGE 3:Unexplained unresponsive malnutrition,diarrhoea,fever. Oral candidiasis,oral hairy leukoplakia,acute necrotizing ulcerative gingivitis,periodontitis,pulm.TB, severe recur. Bacterial pneumonia
STAGE 4:severe wasting,pneumocystis pneumonia,severe bact. Infection-empyema,pyomyositis,bone or jt. Infection.
ch. Herpes simplex,extrapulm. TB,Kaposi’s sarcoma,oesophageal candidiasis,CNS toxoplasmosis,HIV encephalopathy
• Diagnosis:- <18 mo-PCR,viral load ELISA

Molluscum Contagiousum in AIDS Oral leukoplakia in AIDS

• Treatment:-STAGE 4- irrespective of CD4STAGE 3- irrespective of CD4,if >12mo with TB,LIP,OHL
or thrombocytopenia-ART may be delayedSTAGE 2- CD4 or TLC below thresholdSTAGE 1- CD4 at or below threshold