Embed Size (px)
Citation preview
This Speaker Series is a summary of a workshop on psoriasis from a nurse’s perspective, touching on its diagnosis and management, patient care and ways of optimising treatment options. The Workshop was held in Richmond, Victoria in March 2017 and was sponsored by Novartis.
ImpactofpsoriasisonqualityoflifeReduction in quality of life (QoL) in psoriasis is comparable with other chronic diseases e.g. cancer, diabetes1
In a survey of approximately 5,600 psoriasis patients, QoL was significantly impaired in the majority of patients2
1
6%
94%
12%
88%18%
82%
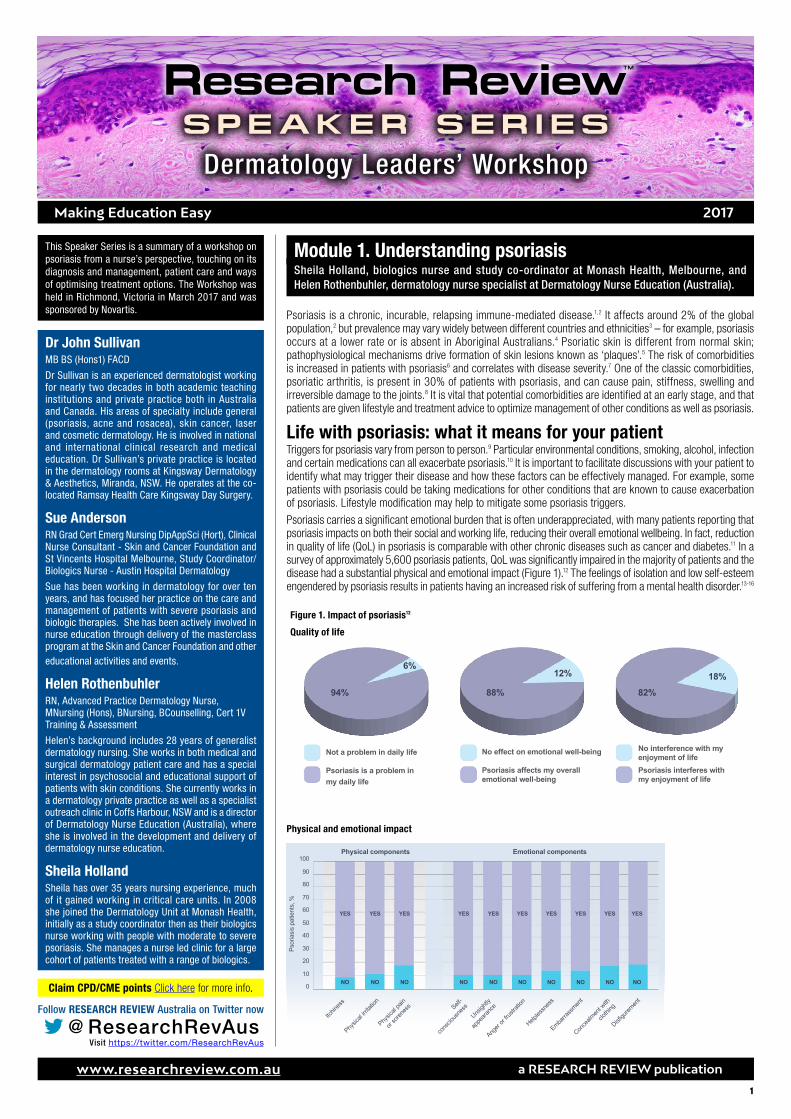
No effect on emotional well-being No interference with my enjoyment of lifeNot a problem in daily life
Psoriasis affects my overall emotional well-being
Psoriasis interferes with my enjoyment of life
Psoriasis is a problem in my daily life
Dr John Sullivan MB BS (Hons1) FACD
Dr Sullivan is an experienced dermatologist working for nearly two decades in both academic teaching institutions and private practice both in Australia and Canada. His areas of specialty include general (psoriasis, acne and rosacea), skin cancer, laser and cosmetic dermatology. He is involved in national and international clinical research and medical education. Dr Sullivan’s private practice is located in the dermatology rooms at Kingsway Dermatology & Aesthetics, Miranda, NSW. He operates at the co-located Ramsay Health Care Kingsway Day Surgery.
Sue Anderson RN Grad Cert Emerg Nursing DipAppSci (Hort), Clinical Nurse Consultant - Skin and Cancer Foundation and St Vincents Hospital Melbourne, Study Coordinator/Biologics Nurse - Austin Hospital Dermatology
Sue has been working in dermatology for over ten years, and has focused her practice on the care and management of patients with severe psoriasis and biologic therapies. She has been actively involved in nurse education through delivery of the masterclass program at the Skin and Cancer Foundation and other educational activities and events.
Helen RothenbuhlerRN, Advanced Practice Dermatology Nurse, MNursing (Hons), BNursing, BCounselling, Cert 1V Training & Assessment
Helen’s background includes 28 years of generalist dermatology nursing. She works in both medical and surgical dermatology patient care and has a special interest in psychosocial and educational support of patients with skin conditions. She currently works in a dermatology private practice as well as a specialist outreach clinic in Coffs Harbour, NSW and is a director of Dermatology Nurse Education (Australia), where she is involved in the development and delivery of dermatology nurse education.
Sheila HollandSheila has over 35 years nursing experience, much of it gained working in critical care units. In 2008 she joined the Dermatology Unit at Monash Health, initially as a study coordinator then as their biologics nurse working with people with moderate to severe psoriasis. She manages a nurse led clinic for a large cohort of patients treated with a range of biologics.
11
2017 Making Education Easy
www.researchreview.com.au a RESEARCH REVIEW publication
Dermatology Leaders’ WorkshopSPEAKER SER IESResearch Review
TM
Claim CPD/CME points Click here for more info.
Module 1. Understanding psoriasis Sheila Holland, biologics nurse and study co-ordinator at Monash Health, Melbourne, and Helen Rothenbuhler, dermatology nurse specialist at Dermatology Nurse Education (Australia).
Psoriasis is a chronic, incurable, relapsing immune-mediated disease.1,2 It affects around 2% of the global population,2 but prevalence may vary widely between different countries and ethnicities3 – for example, psoriasis occurs at a lower rate or is absent in Aboriginal Australians.4 Psoriatic skin is different from normal skin; pathophysiological mechanisms drive formation of skin lesions known as ‘plaques’.5 The risk of comorbidities is increased in patients with psoriasis6 and correlates with disease severity.7 One of the classic comorbidities, psoriatic arthritis, is present in 30% of patients with psoriasis, and can cause pain, stiffness, swelling and irreversible damage to the joints.8 It is vital that potential comorbidities are identified at an early stage, and that patients are given lifestyle and treatment advice to optimize management of other conditions as well as psoriasis.
Life with psoriasis: what it means for your patientTriggers for psoriasis vary from person to person.9 Particular environmental conditions, smoking, alcohol, infection and certain medications can all exacerbate psoriasis.10 It is important to facilitate discussions with your patient to identify what may trigger their disease and how these factors can be effectively managed. For example, some patients with psoriasis could be taking medications for other conditions that are known to cause exacerbation of psoriasis. Lifestyle modification may help to mitigate some psoriasis triggers.
Psoriasis carries a significant emotional burden that is often underappreciated, with many patients reporting that psoriasis impacts on both their social and working life, reducing their overall emotional wellbeing. In fact, reduction in quality of life (QoL) in psoriasis is comparable with other chronic diseases such as cancer and diabetes.11 In a survey of approximately 5,600 psoriasis patients, QoL was significantly impaired in the majority of patients and the disease had a substantial physical and emotional impact (Figure 1).12 The feelings of isolation and low self-esteem engendered by psoriasis results in patients having an increased risk of suffering from a mental health disorder.13-16
Figure 1. Impact of psoriasis12
Quality of life
In depth: Physical and emotional impact of psoriasisThis chart shows an evaluation of the physical and emotional impact of psoriasis on patients1
2
Emotional components100
90
80
70
60
50
40
30
20
10
0
Psor
iasi
s pa
tient
s, %
YESYESYES YES YES YES YESYES YES YES
Physical components
NONONO NO NO NO NONO NO NO
Physical and emotional impact
@ ResearchRevAusVisit https://twitter.com/ResearchRevAus
Follow RESEARCH REVIEW Australia on Twitter now
22
www.researchreview.com.au a RESEARCH REVIEW publication
Research Review TM
SPEAKER SERIESDermatology Leaders’ Workshop
Managing psychosocial needs: In practiceMany patients will feel uncomfortable discussing the emotional burden of psoriasis and this may compound their feelings of isolation and helplessness.Ask the patient how psoriasis affects their quality of life. Specific questions about different aspects of their life will encourage more honest and detailed answers; for example:
• Has your condition caused any work-related problems?
• How does psoriasis impact on your relationships and social life?
• Does it prevent you from participating in activities that you would otherwise enjoy?
Know what help and support is available for your patients, and offer practical advice; for example:
• Details of psoriasis charities/support groups – online forums or face-to-face groups can help patients feel less alone, provide an outlet to voice their feelings, as well offering practical advice.
• Guidance on lifestyle modifications, such as increasing exercise or taking up meditation, to help relieve stress.
• Information on how to discuss their condition with their employer and ask for additional support.
Discuss all the options available with the patient, working with them to develop a strategy that will effectively address their psychosocial needs.
Diagnosing psoriasisPsoriasis varies widely in both severity and appearance.8 There are a number of different types of psoriasis, which are classified by the skin’s appearance. These include plaque psoriasis, inverse (flexural) psoriasis, erythrodermic psoriasis, pustular psoriasis, guttate psoriasis, and psoriatic nail changes. Accurately diagnosing the type of psoriasis that is present will allow optimal management via delivery of the most appropriate treatment. The mean time between the onset of symptoms and diagnosis is 2 years.17
Plaque psoriasis is the most common form of psoriasis.8 Lesions seen in patients with plaque psoriasis are red, raised and well-defined with a silvery-white scale.8,18 Most commonly seen on elbows, knees, scalp, legs and lower back, they can be very itchy and painful.2,8 A full body examination and use of appropriate diagnostic methodology will help to distinguish plaque psoriasis from alternative forms of psoriasis and from other skin conditions.
Diagnosing plaque psoriasis: In practiceWhat does my patient look like?Ask your patient if they would mind you touching their skin, as part of the initial evaluation.
Explain that examining the skin thoroughly will allow you to gain important clinical information about the way the skin looks and feels.
Consider factors such as the sex of the patient, religion and culture before performing a physical examination. The patient must feel comfortable – a warm and private location is essential.
Discuss with your patient their past medical history, their occupation and hobbies, family history of skin disease, if they are taking any medications, if they smoke or consume alcohol, and if they have any allergies, as part of the initial work-up.
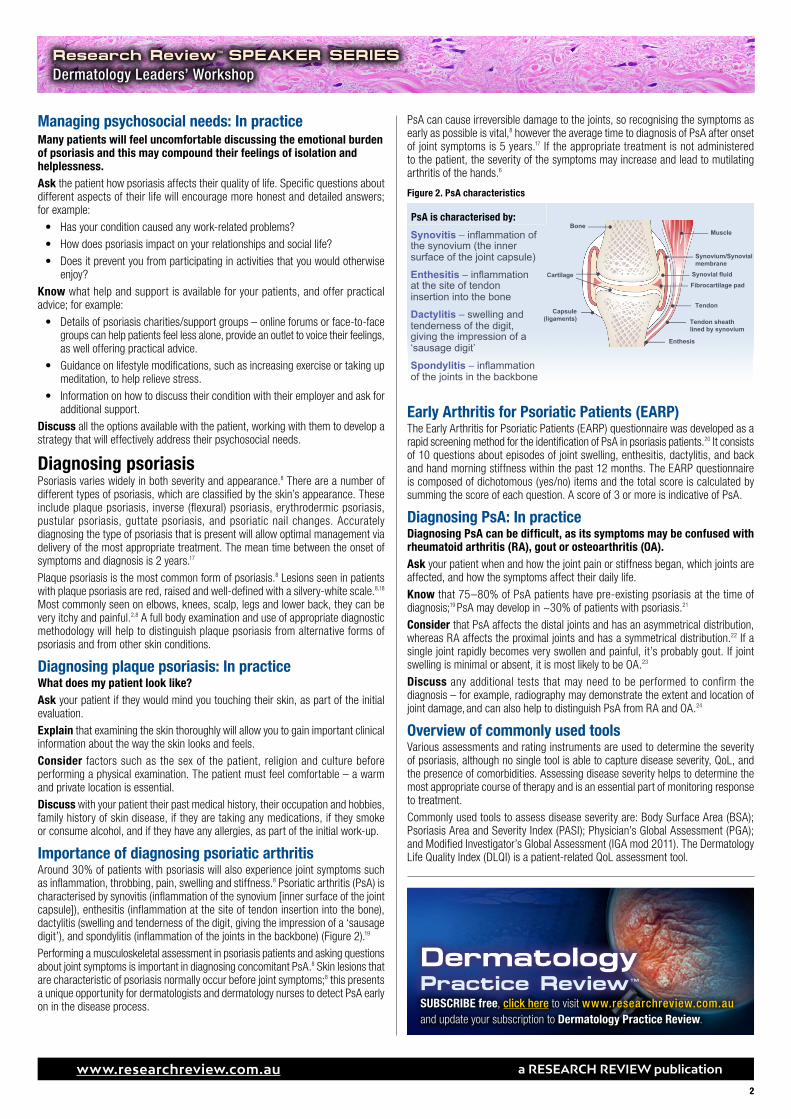
Importance of diagnosing psoriatic arthritisAround 30% of patients with psoriasis will also experience joint symptoms such as inflammation, throbbing, pain, swelling and stiffness.8 Psoriatic arthritis (PsA) is characterised by synovitis (inflammation of the synovium [inner surface of the joint capsule]), enthesitis (inflammation at the site of tendon insertion into the bone), dactylitis (swelling and tenderness of the digit, giving the impression of a ‘sausage digit’), and spondylitis (inflammation of the joints in the backbone) (Figure 2).19
Performing a musculoskeletal assessment in psoriasis patients and asking questions about joint symptoms is important in diagnosing concomitant PsA.8 Skin lesions that are characteristic of psoriasis normally occur before joint symptoms;8 this presents a unique opportunity for dermatologists and dermatology nurses to detect PsA early on in the disease process.
PsA can cause irreversible damage to the joints, so recognising the symptoms as early as possible is vital,8 however the average time to diagnosis of PsA after onset of joint symptoms is 5 years.17 If the appropriate treatment is not administered to the patient, the severity of the symptoms may increase and lead to mutilating arthritis of the hands.6
Early Arthritis for Psoriatic Patients (EARP) The Early Arthritis for Psoriatic Patients (EARP) questionnaire was developed as a rapid screening method for the identification of PsA in psoriasis patients.20 It consists of 10 questions about episodes of joint swelling, enthesitis, dactylitis, and back and hand morning stiffness within the past 12 months. The EARP questionnaire is composed of dichotomous (yes/no) items and the total score is calculated by summing the score of each question. A score of 3 or more is indicative of PsA.
Diagnosing PsA: In practiceDiagnosing PsA can be difficult, as its symptoms may be confused with rheumatoid arthritis (RA), gout or osteoarthritis (OA).Ask your patient when and how the joint pain or stiffness began, which joints are affected, and how the symptoms affect their daily life.
Know that 75–80% of PsA patients have pre-existing psoriasis at the time of diagnosis;19 PsA may develop in ~30% of patients with psoriasis.21
Consider that PsA affects the distal joints and has an asymmetrical distribution, whereas RA affects the proximal joints and has a symmetrical distribution.22 If a single joint rapidly becomes very swollen and painful, it’s probably gout. If joint swelling is minimal or absent, it is most likely to be OA.23
Discuss any additional tests that may need to be performed to confirm the diagnosis – for example, radiography may demonstrate the extent and location of joint damage, and can also help to distinguish PsA from RA and OA.24
Overview of commonly used toolsVarious assessments and rating instruments are used to determine the severity of psoriasis, although no single tool is able to capture disease severity, QoL, and the presence of comorbidities. Assessing disease severity helps to determine the most appropriate course of therapy and is an essential part of monitoring response to treatment.
Commonly used tools to assess disease severity are: Body Surface Area (BSA); Psoriasis Area and Severity Index (PASI); Physician’s Global Assessment (PGA); and Modified Investigator’s Global Assessment (IGA mod 2011). The Dermatology Life Quality Index (DLQI) is a patient-related QoL assessment tool.
PsA is characterised by:Synovitis – inflammation of the synovium (the inner surface of the joint capsule)
Enthesitis – inflammation at the site of tendon insertion into the bone
Dactylitis – swelling and tenderness of the digit, giving the impression of a ‘sausage digit’
Spondylitis – inflammation of the joints in the backbone
1
Cartilage
BoneMuscle
Capsule(ligaments)
Synovium/Synovial membrane
Synovial fluidFibrocartilage pad
Tendon
Tendon sheath lined by synovium
Enthesis
Figure 2. PsA characteristicsPsA is characterised by:Synovitis – inflammation of the synovium (the inner surface of the joint capsule)
Enthesitis – inflammation at the site of tendon insertion into the bone
Dactylitis – swelling and tenderness of the digit, giving the impression of a ‘sausage digit’
Spondylitis – inflammation of the joints in the backbone
1
Cartilage
BoneMuscle
Capsule(ligaments)
Synovium/Synovial membrane
Synovial fluidFibrocartilage pad
Tendon
Tendon sheath lined by synovium
Enthesis
PsA is characterised by:Synovitis – inflammation of the synovium (the inner surface of the joint capsule)
Enthesitis – inflammation at the site of tendon insertion into the bone
Dactylitis – swelling and tenderness of the digit, giving the impression of a ‘sausage digit’
Spondylitis – inflammation of the joints in the backbone
1
Cartilage
BoneMuscle
Capsule(ligaments)
Synovium/Synovial membrane
Synovial fluidFibrocartilage pad
Tendon
Tendon sheath lined by synovium
Enthesis
DermatologyPractice ReviewTM
SUBSCRIBE free, click here to visit www.researchreview.com.au and update your subscription to Dermatology Practice Review.
PsA is characterised by:
33
www.researchreview.com.au a RESEARCH REVIEW publication
Research Review TM
SPEAKER SERIESDermatology Leaders’ Workshop
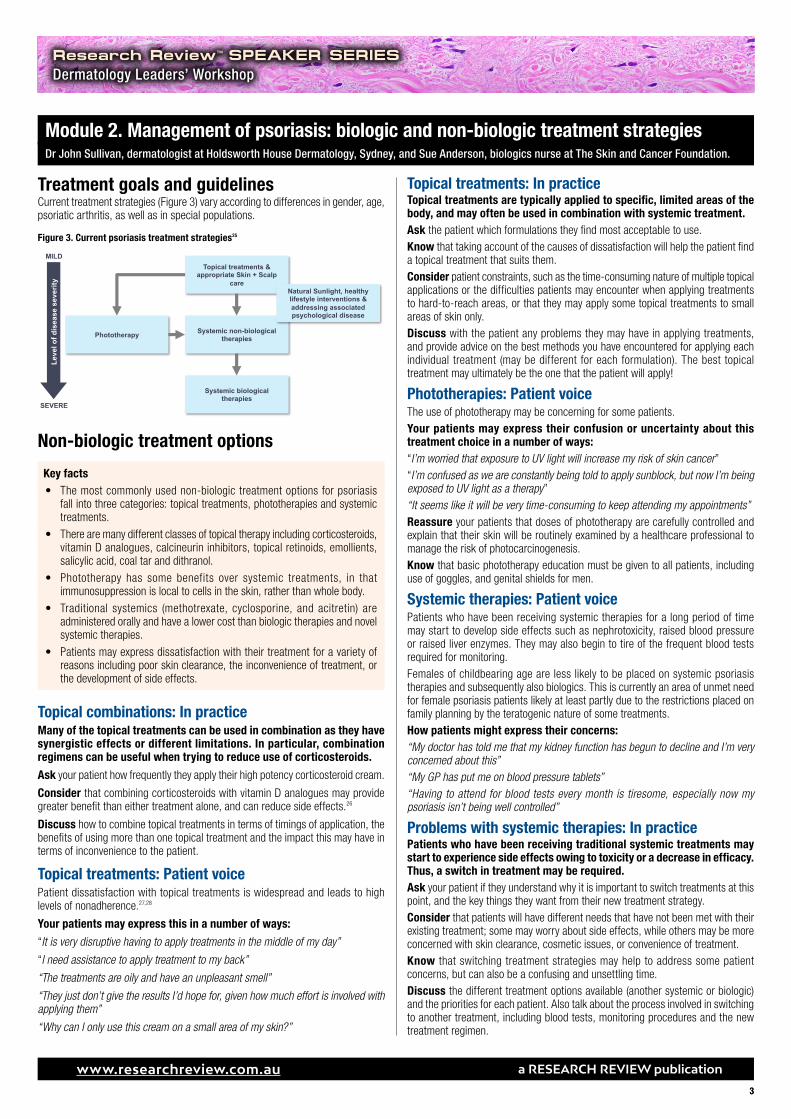
Treatment goals and guidelines Current treatment strategies (Figure 3) vary according to differences in gender, age, psoriatic arthritis, as well as in special populations.
Non-biologic treatment options
Key facts• The most commonly used non-biologic treatment options for psoriasis
fall into three categories: topical treatments, phototherapies and systemic treatments.
• There are many different classes of topical therapy including corticosteroids, vitamin D analogues, calcineurin inhibitors, topical retinoids, emollients, salicylic acid, coal tar and dithranol.
• Phototherapy has some benefits over systemic treatments, in that immunosuppression is local to cells in the skin, rather than whole body.
• Traditional systemics (methotrexate, cyclosporine, and acitretin) are administered orally and have a lower cost than biologic therapies and novel systemic therapies.
• Patients may express dissatisfaction with their treatment for a variety of reasons including poor skin clearance, the inconvenience of treatment, or the development of side effects.
Topical combinations: In practiceMany of the topical treatments can be used in combination as they have synergistic effects or different limitations. In particular, combination regimens can be useful when trying to reduce use of corticosteroids.
Ask your patient how frequently they apply their high potency corticosteroid cream.
Consider that combining corticosteroids with vitamin D analogues may provide greater benefit than either treatment alone, and can reduce side effects.26
Discuss how to combine topical treatments in terms of timings of application, the benefits of using more than one topical treatment and the impact this may have in terms of inconvenience to the patient.
Topical treatments: Patient voicePatient dissatisfaction with topical treatments is widespread and leads to high levels of nonadherence.27,28
Your patients may express this in a number of ways:
“It is very disruptive having to apply treatments in the middle of my day”
“I need assistance to apply treatment to my back”
“The treatments are oily and have an unpleasant smell”
“They just don’t give the results I’d hope for, given how much effort is involved with applying them”
“Why can I only use this cream on a small area of my skin?”
Topical treatments: In practiceTopical treatments are typically applied to specific, limited areas of the body, and may often be used in combination with systemic treatment.Ask the patient which formulations they find most acceptable to use.Know that taking account of the causes of dissatisfaction will help the patient find a topical treatment that suits them.Consider patient constraints, such as the time-consuming nature of multiple topical applications or the difficulties patients may encounter when applying treatments to hard-to-reach areas, or that they may apply some topical treatments to small areas of skin only.Discuss with the patient any problems they may have in applying treatments, and provide advice on the best methods you have encountered for applying each individual treatment (may be different for each formulation). The best topical treatment may ultimately be the one that the patient will apply!
Phototherapies: Patient voiceThe use of phototherapy may be concerning for some patients. Your patients may express their confusion or uncertainty about this treatment choice in a number of ways:“I’m worried that exposure to UV light will increase my risk of skin cancer”“I’m confused as we are constantly being told to apply sunblock, but now I’m being exposed to UV light as a therapy”“It seems like it will be very time-consuming to keep attending my appointments”Reassure your patients that doses of phototherapy are carefully controlled and explain that their skin will be routinely examined by a healthcare professional to manage the risk of photocarcinogenesis.Know that basic phototherapy education must be given to all patients, including use of goggles, and genital shields for men.
Systemic therapies: Patient voicePatients who have been receiving systemic therapies for a long period of time may start to develop side effects such as nephrotoxicity, raised blood pressure or raised liver enzymes. They may also begin to tire of the frequent blood tests required for monitoring.Females of childbearing age are less likely to be placed on systemic psoriasis therapies and subsequently also biologics. This is currently an area of unmet need for female psoriasis patients likely at least partly due to the restrictions placed on family planning by the teratogenic nature of some treatments.How patients might express their concerns:“My doctor has told me that my kidney function has begun to decline and I’m very concerned about this”“My GP has put me on blood pressure tablets”“Having to attend for blood tests every month is tiresome, especially now my psoriasis isn’t being well controlled”
Problems with systemic therapies: In practicePatients who have been receiving traditional systemic treatments may start to experience side effects owing to toxicity or a decrease in efficacy. Thus, a switch in treatment may be required.Ask your patient if they understand why it is important to switch treatments at this point, and the key things they want from their new treatment strategy.Consider that patients will have different needs that have not been met with their existing treatment; some may worry about side effects, while others may be more concerned with skin clearance, cosmetic issues, or convenience of treatment.Know that switching treatment strategies may help to address some patient concerns, but can also be a confusing and unsettling time.Discuss the different treatment options available (another systemic or biologic) and the priorities for each patient. Also talk about the process involved in switching to another treatment, including blood tests, monitoring procedures and the new treatment regimen.
Current treatment strategies1
Phototherapy Systemic non-biological therapies
Topical treatments & appropriate Skin + Scalp
care
Systemic biologicaltherapies
SEVERE
MILD
Leve
l of d
isea
se s
ever
ity
1
Natural Sunlight, healthy lifestyle interventions & addressing associated psychological disease
Figure 3. Current psoriasis treatment strategies25
Module 2. Management of psoriasis: biologic and non-biologic treatment strategiesDr John Sullivan, dermatologist at Holdsworth House Dermatology, Sydney, and Sue Anderson, biologics nurse at The Skin and Cancer Foundation.
44
www.researchreview.com.au a RESEARCH REVIEW publication
Research Review TM
SPEAKER SERIESDermatology Leaders’ Workshop
Summary of unmet needs with existing treatmentsTopical therapies29
• Administration can be labourious and messy.• Adherence to treatment can be poor.• Risks associated with frequent and long-term use of topical steroids.
Phototherapies29
• Inconvenient as requires frequent visits to phototherapy unit.• Potential side effects associated with photodamage and photo-carcinogen.• High cumulative exposure to oral PUVA associated with a dose-related increase
in the risk of non-melanoma and melanoma skin cancer.
Traditional systemic therapies29 • Adverse effects including nephrotoxicity, hypertension, hepatotoxicity, bone
marrow suppression and teratogenicity limit their use.• Complex monitoring may be required.
Biologics in psoriasis treatmentKey facts• Biologics are protein-based drugs derived from living cells cultured in a
laboratory.• Patients may switch to biologics due to the potential for improved efficacy,
reduction in side effects and overcoming existing treatment failure.• Needle phobia may limit the willingness of some patients to switch to
biologics.• Current biologics used in psoriasis treatment are inhibitors of TNF-α,
IL-12/23 and IL-17A and include adalimumab, etanercept, infliximab, ixekizumab, secukinumab and ustekinumab.
• Biologics can provide very high levels of skin clearance, even in severe cases.• Neutralising anti-drug antibody development may be a challenge with
biologics.• In general, patients on biologics may be more vulnerable to infection.• Close monitoring of patients on biologics for side effects is important.
Biologics can offer an alternative to systemic therapies Improved scientific understanding of immunogenesis in psoriasis has enabled the development of biologics,30 which are protein-based drugs derived from living cells cultured in a laboratory.31 Biologics have been designed to alter the activity of T-lymphocytes and cytokines involved in the pathogenesis of psoriasis32 and target specific parts of the immune system, rather than the whole system.33
Moderate-to-severe psoriasis has historically been treated using traditional systemic agents, topical agents and phototherapy.8 Biologics act through targeted inhibition; this specificity leads to reduced side effects relative to toxicities found with broad-spectrum therapies.34 Biologics may be prescribed as either first-line or second-line therapy, dependent on individual patient needs.2
Switching to biologics can bring benefits to patients Switching to biologics can bring benefits to patients such as:
• Improved efficacy and skin clearance. Newer biologic agents may provide substantially higher rates of clearance for patients with moderate-to-severe psoriasis.34
• Less intensive administration schedules than some therapies. Applying topical treatments or using phototherapy can be time consuming; most biologic therapies can be self-administered at home, without the need to travel to a hospital or clinic.34
• Potential reduction in side effects. Common side effects with biologics are generally mild; serious side effects have been reported, but these are rare.34
Switching treatments: Patient voicePatients can express dissatisfaction with their existing treatment and its outcomes in a variety of ways. How patients might express their concerns:“I’m not very happy with the unpleasant side effects I’ve had with my current treatment”“I’ve read about these new treatments called biologics, and wonder if they would help me get clearer skin”
“I don’t think my current treatment is very effective”“I still have a lot of itching and pain”“The treatment I’m currently taking is inconvenient – is there an easier way of taking this treatment, such as a pill or an injection?”
Switching from non-biologics to biologics: In practiceIf a patient has experienced initial success with a traditional systemic therapy, but is now experiencing loss of efficacy, they may be eligible for treatment with biologics.Ask if your patient would be willing to try a different treatment approach, in order to potentially manage their condition more effectively.Know that the loss of treatment response can be a significant setback for patients with psoriasis, but switching to a new treatment approach could improve adherence and patient outcomes.35
Consider whether another systemic or topical therapy could deliver efficacy, or whether the patient might see better results from transitioning to a biologic therapy. Does the patient have any comorbidities that might affect treatment choice?Discuss the alternative treatment approaches available that offer new hope for effective treatment; ensure that the patient is well-informed and engaged in the discussions about switching to a biologic.If a patient appears from their body language to be uncomfortable with the appearance of their skin, this may suggest that their symptoms are not optimally controlled.Ask if your patient is happy with the level of skin clearance that their current treatment provides.Know that newer biologic agents may provide substantially higher rates of clearance for patients with moderate-to-severe psoriasis.34
Consider that psoriasis symptoms can also have a detrimental impact on the patient’s quality of life.Discuss realistic expectations regarding the potential efficacy of treatment with a biologic and how it could impact their physical and emotional symptoms.
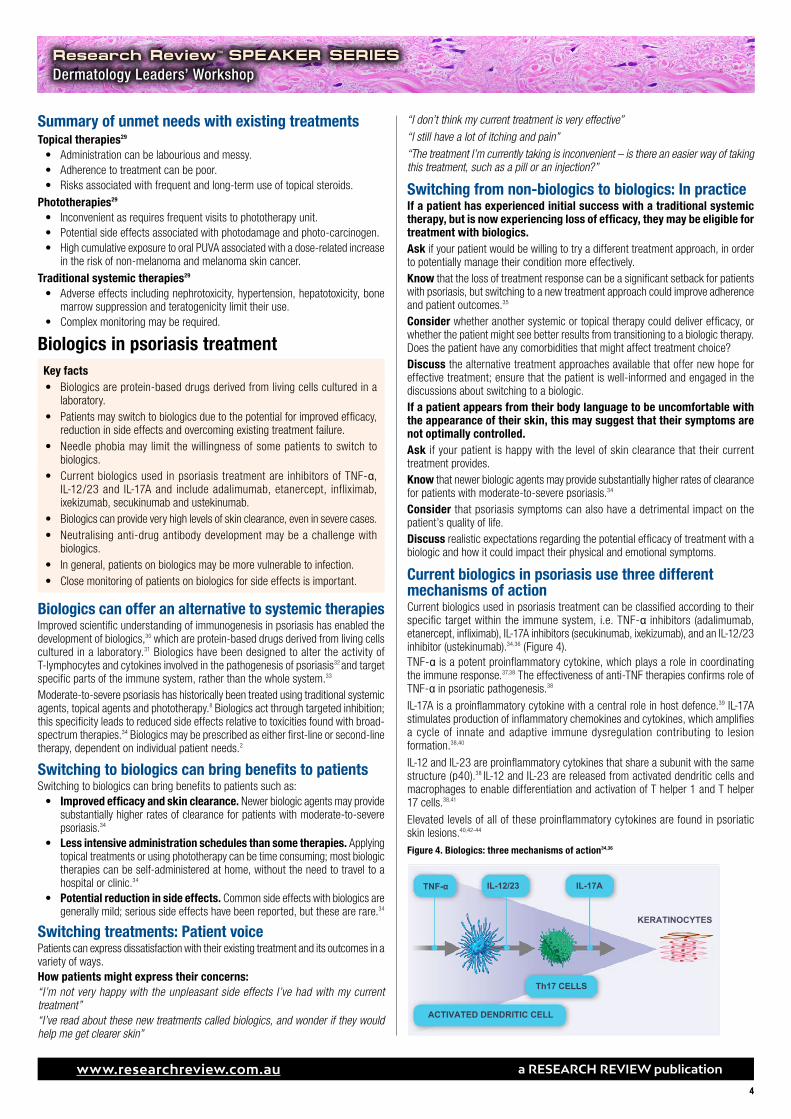
Current biologics in psoriasis use three different mechanisms of actionCurrent biologics used in psoriasis treatment can be classified according to their specific target within the immune system, i.e. TNF-α inhibitors (adalimumab, etanercept, infliximab), IL-17A inhibitors (secukinumab, ixekizumab), and an IL-12/23 inhibitor (ustekinumab).34,36 (Figure 4).TNF-α is a potent proinflammatory cytokine, which plays a role in coordinating the immune response.37,38 The effectiveness of anti-TNF therapies confirms role of TNF-α in psoriatic pathogenesis.38
IL-17A is a proinflammatory cytokine with a central role in host defence.39 IL-17A stimulates production of inflammatory chemokines and cytokines, which amplifies a cycle of innate and adaptive immune dysregulation contributing to lesion formation.38,40
IL-12 and IL-23 are proinflammatory cytokines that share a subunit with the same structure (p40).38 IL-12 and IL-23 are released from activated dendritic cells and macrophages to enable differentiation and activation of T helper 1 and T helper 17 cells.38,41
Elevated levels of all of these proinflammatory cytokines are found in psoriatic skin lesions.40,42-44
Figure 4. Biologics: three mechanisms of action34,36
IL-17A
ACTIVATED DENDRITIC CELL
Th17 CELLS
KERATINOCYTES
IL-12/23TNF-α
1
55
www.researchreview.com.au a RESEARCH REVIEW publication
Research Review TM
SPEAKER SERIESDermatology Leaders’ Workshop
Biologics have proven their effectiveness in the treatment of autoimmune disease.45 However, their immunomodulatory action can increase the likelihood of certain adverse reactions, for example systemic infections, malignancy, anaphylaxis and hypersensitivity.45 Immunogenicity can occur due to the nature of biologics, which are proteins, and may in specific cases potentially be linked to loss of efficacy.
InfectionTuberculosis infection can be atypical and severe and reactivation of latent TB also a risk for patients on TNF-α.
MalignancyIt can be difficult to differentiate drug-induced malignancy from the nature of underlying disease and chronic inflammatory state.45 Non-melanoma skin cancer and lymphoma occur more commonly in moderate to severe psoriasis patients. Malignancies associated with immunosuppression have not been observed with immunomodulatory biologics used to treat psoriasis. Similarly, an increase in the risk of solid tumours has not been observed.
Immune reactionsAnaphylaxis has been reported following administration of adalimumab, etanercept, infliximab, ixekizumab, secukinumab and ustekinumab.46-51 If an anaphylactic or other serious allergic reaction occurs with any biologic therapy, the treatment should be immediately discontinued and appropriate therapy initiated.
Immune dysregulation resulting in autoimmune and immune inflammatory syndromes has been observed. (e.g. TNF-α inhibitors and multiple sclerosis and/or drug induced lupus and/or immune reconstitution inflammatory syndromes such as hepatitis on stopping infliximab in patients with chronic active hepatitis B).
ImmunogenicityDevelopment of anti-drug antibodies (ADAs) against biologics may be associated with decreased treatment efficacy and may increase risk of adverse events.52 ADA development can occur in patients with psoriasis receiving TNF-α, IL-12/23 and IL-17A inhibitors.53 Even fully human monoclonal antibodies can be immunogenic.54 Mechanisms behind ADA development and potential neutralising consequences of ADAs are not clearly understood, but their effects on decreasing treatment efficacy may be clinically significant.53 However, tests for specific ADAs are not yet readily available for some biologics, and are rarely used in dermatology, so monitoring development in clinical practice may be challenging.55
Biologics: In practiceWhen switching patients to a biologic, it is important to help them understand why a change in treatment is appropriate and what they can expect in terms of efficacy, side effects and monitoring.Ask if they fully understand why a switch in their treatment has been suggested and what they can expect from the new treatment.Consider that empowering patients to self-inject increases the patient convenience of these treatments but may require significant support from healthcare professionals from the start.Know that some patients will find switching treatments challenging, both mentally and in practice. Be prepared for this and aim to reassure and educate to reduce fear.Discuss the side effect profile of the new treatment and how to manage and report common side effects. Reassure and counsel patients who have concerns regarding administration methods e.g. needle phobia.
Monitoring loss of efficacy for biologics: In practiceWhen a patient presents with a loss of treatment efficacy with biologics, it may be due to different reasons, including ADA development.52
Know that secondary failure of one drug may correspond to a higher risk of a similar response for subsequent biologic therapies in the same class, although this has not yet been confirmed.55,56
Consider potential causes for loss of treatment efficacy – e.g. changes in adherence or emergence of further comorbidities.Discuss with the treating physician whether switching therapies may be advisable to improve patient outcomes.
Monitoring biologics: In practiceMonitoring patients on biologic treatments can be quite intensive, especially during the initial stages. It is recommended that patients are monitored every six months with clinic contact available to the patient in between monitoring.
Ask if the patient understands why it is important that he/she attend the clinic for their monitoring appointments.
Consider that many patients will have questions and concerns when starting a new treatment so try to allow time at each monitoring appointment to address these.
Know that monitoring for infection and particularly for tuberculosis is a key requirement for patients receiving biologics.
Discuss how to make the monitoring schedule convenient for the patient and stress the importance of attending the appointments.
How to use biologicsKey facts• Pre-biologic checklists can identify key questions to ask your patient or
any additional tests that may be required, before treatment with a biologic therapy commences.
• Biologics may be delivered by IV infusion, or self-administered by patients via an autoinjector pen or prefilled syringe – familiarise yourself with the different steps involved for each approach.
• Biologics should be stored at around 4°C to maintain their integrity, and all needles disposed of in an appropriate sharps disposal bin.
• If a biologic is not achieving the best outcomes for a patient, due to waning efficacy or side effects, it may be switched to another treatment, potentially with a different mechanism of action.
Before starting treatment with a biologicThere are specific questions that you will need to ask a patient prior to commencing biologic treatment. Performing a full risk analysis of each patient using a pre-biologic clinical checklist before treatment is administered will help to ensure that the right patients receive biologic therapies.57
You should also record: the patient’s weight and height; any allergies (e.g. latex); if they are using contraception or are planning to become pregnant; if they have any surgery planned; any pre-existing medical condition. These factors may influence the choice of treatment.58
With the exception of infliximab, which is given via IV infusion, most biologics prescribed for psoriasis can be given through self-injection. In some cases, the treatment is delivered via an auto-injector pen where the needle is not visible to the patient (adalimumab, etanercept, ixekizumab, secukinumab). Pre-filled syringes may also be available (adalimumab, etanercept).
Administration of biologics: Patient voicePatient preference for and confidence with administering a specific biologic treatment option may vary.56
How patients might express their concerns:“I really don’t like needles”“What if I forget to inject myself?”“I’m afraid my hands will tremble as I’m doing the injection”“Will it hurt a lot?”
Administration of biologics: In practiceEven if it initially appears daunting, self-injection can be a very convenient approach for a patient with psoriasis to receive their treatment.Ask the patient if they have any concerns with needles or self-injection
• Are they willing to administer their own injections?
• Do they have the ability to self-administer injections?57
Discuss the options for overcoming their doubts
• Reassure the patient that with time, self-injecting should become quicker and easier.
• They may ask a partner or carer for support in administering treatment.57
Consider the number of supervised practice sessions that an individual patient will need to assess their competence in the technique.57
Explain that you will continue to support the patient throughout their treatment with biologic therapies, regardless of whether they are self-injecting.
If you have any concerns over the patient’s emotional or functional condition, you should refer them to the prescribing consultant dermatologist.
66
www.researchreview.com.au a RESEARCH REVIEW publication
Research Review TM
SPEAKER SERIESDermatology Leaders’ Workshop
Storage of biologicsStoring a biologic in suboptimal conditions may alter its efficacy.59 Biologics should be stored in a refrigerator and kept at around 4°C to maintain their integrity.60 Biologics should never be frozen as this can inactivate the drug.60 Removing the biologic from the refrigerator 15–30 minutes before administration can help to eliminate the discomfort commonly associated with injecting a cold medication.60
Monitoring biologic response: In practiceIdentifying whether the patient is achieving the best possible outcomes is essential.Discuss with the patient how the benefits of their treatment will be assessed, and the possible reasons treatment might be stopped.57
Ensure that the patient knows when they will have follow-up appointments to fully assess and review their treatment (at least once every 3 months).34
Explain to patients that they should contact their local dermatology department if they have concerns about their health, or experience any signs of infection; provide the patient with the relevant contact numbers, including out-of-hours and on-call dermatologist.
Switching between biologicsSwitching between biologic therapies is a common and effective strategy to optimise patient outcomes, and may be instigated by:34
• Loss of efficacy or treatment failure.• Safety concerns (side effects).• Changing to a more convenient therapy (e.g. IV infusion to self-injecting).• Availability of a better treatment.
Although treatment failure with one anti-TNF agent does not always predict failure with another anti-TNF agent, studies have reported that switching from a TNF-α inhibitor to a biologic with a different mechanism of action (e.g. secukinumab or ixekizumab, which are IL-17A inhibitors, or ustekinumab, an IL-12/IL-23 inhibitor) can result in significant improvements in PASI response rates in patients who failed to respond to previous anti-TNF therapy.56
Switching between biologics: Patient voiceAsk your patient if they have any questions about switching treatment to another biologic. Examples of questions that your patient may ask:“How is this new treatment different to the one I was on before?”“Do I have to administer this treatment in a different way? ““What will happen when I start the new treatment? Will there be any side effects?“How quickly will I see the results?
Switching between biologics: In practiceIf it is necessary to switch to another biologic, spending some time with the patient discussing the rationale will help them to understand and prepare for the change.Ask if the patient fully understands why it is important to switch to another biologic treatment at this point.Consider that your patient may require reassurance that the switch is for a valid reason.Know that the patient should feel engaged with the new approach; empower them by providing sufficient information about the new drug.Discuss the dosing, treatment schedule and method of administration. Emphasise the importance of reporting any side effects that they may experience following the switch. Explain any new monitoring procedures associated with this treatment.
Assess treatment responseImprovement in PASI/disease severity score
Improvement in DLQI score
Patient satisfaction
Monitoring biologicsBaseline & yearly TB skin tests
Complete blood counts
Hepatic function (anti-TNF only)
Reasons for stopping treatmentWaning efficacy
Side effects
Module 3. Patient care: understand your patient Sue Anderson, biologics nurse at The Skin and Cancer Foundation.
Key facts• It is important to build a strong, trusting relationship with your patient that
will allow you to identify their priorities and preferences for treatment.
• By facilitating the patient-physician dialogue, you can help to maximise health outcomes.
• Patients may have unrealistic expectations with regards to their treatment, which should be managed appropriately via the provision of additional information and guidance.
• Creating tailored treatment plans for individual patients can help to improve patient management and ensure that the appropriate follow-up procedures are in place.
Building relationships with patients: In practiceA therapeutic nurse-patient relationship is based on mutual trust and respect, and effectively supporting the patient’s physical and emotional needs.
Ask your patient open-ended questions, and actively listen to their responses, which may contain essential information that will increase your understanding of their condition and priorities.
Know that non-verbal cues (e.g. facial expressions, tone of voice, body language) may be as important as verbal responses.
Consider that your patient may need further encouragement from you if they are struggling to communicate.
Discuss and clarify what your patient is thinking and feeling; offer empathy, and make the patient feel you have their best interests at heart. Try to convey the message: “I care”.
Understanding patient priorities: In practicePatients should be able to influence the treatment they receive for their psoriasis, and you can support them in doing so.Ask about and consider their expectations and preferences.Consider that their physician’s priorities may differ, as they may focus on diagnosis, treatment, and ensuring that the patient knows why and how they should carry out their treatment.Discuss with the patient that although it’s important for them to voice their opinions, they should also listen to the advice of their physician.Know that nurses can help to facilitate any patient-physician conversations. Make sure that patients are kept fully informed when it comes to any decisions about their care.
Managing patient expectations – biologics Patients may expect to see much higher efficacy rates with biologics than those previously achieved with traditional systemic agents; however, patients should realise that biologics are not a cure for psoriasis, and it is important to not ‘over promise’ the concept of clear skin via this therapy.Clinical studies have shown that over 50% of all patients treated with biologics can achieve at least a 75% improvement in PASI score, if the recommended dosing schedule is adhered to34 (with certain biologics, around 80% of patients can achieve this level of improvement).50,61
Thus, there are some patients who will benefit from biologic therapy, and others who will not, and a 100% improvement in PASI may not be possible.
PsoriasisResearch ReviewTM
This publication is supported by Novartis Pharmaceuticals Australia Pty Ltd. The content is entirely independent and based on published studies and the authors’ opinions. It may not reflect the views of Novartis.
www.researchreview.com.au a RESEARCH REVIEW publication
77© 2017 RESEARCH REVIEW
Speaker Series are prepared with an independent commentary from relevant specialists. To become a reviewer please email [email protected] Review Australia Pty Ltd is an independent Australian publisher. Research Review receives funding from a variety of sources including Government depts., health product companies, insurers and other organisations with an interest in health. Journal content is created independently of sponsor companies with assistance from leading local specialists. Privacy Policy: Research Review will record your email details on a secure database and will not release them to anyone without your prior approval. Research Review and you have the right to inspect, update or delete your details at any time. Disclaimer: This publication is not intended as a replacement for regular medical education but to assist in the process. The reviews are a summarised interpretation of the published study and reflect the opinion of the writer rather than those of the research group or scientific journal. It is suggested readers review the full trial data before forming a final conclusion on its merits. Research Review publications are intended for Australian health professionals.
Australian Research Review subscribers can claim CPD/CME points for time spent reading our reviews from a wide range of local medical and nursing colleges. Find out more on our CPD page.
Research Review TM
SPEAKER SERIESDermatology Leaders’ Workshop
Managing patient expectations: In practiceSetting expectations and establishing short-term treatment goals for disease improvement.Ask your patient to communicate their expectations and treatment goals openly and honestly.
Know that showing sensitivity and empathy towards the patient may help them to feel less frustrated.
Consider that your patient may have had unrealistic expectations about the level of benefit they are likely to achieve from their current treatment strategy.
Discuss their current treatment approach and identify if further explanation or clarification is needed; avoid the use of medical jargon where possible, and focus instead on simple, everyday language that the patient is more likely to understand. Agree on what may realistically be achieved in the short term by continuing with this treatment.
Treatment plans and follow-upTreatment plans help to guide psoriasis patients on their journey through treatment. They can begin from the initial assessment and flow into discharge planning.
Follow-up appointments may be used to check that the patient is taking their treatment correctly, assess the efficacy of the treatment and note any side effects, perform any required tests, and determine the patient’s overall satisfaction with their treatment.
References1. Kuek A, et al. Postgrad Med. J 2007;83:251–260.
2. Menter A, et al. J Am Acad Dermatol. 2008;58:826–850.
3. Parisi R, et al. J Invest Dermatol. 2013;133:377–385.
4. Langley GB, et al. Ann Rheum Dis. 2005;64(suppl II):ii18–ii23.
5. Krueger JG, et al. Ann Rheum Dis. 2005;64(Suppl II): ii30–ii36.
6. Mef fer t J. Psoriasis. Medscape. Mar 25, 2016. ht tp: //emedicine.medscape.com/article/1943419-overview
7. Yeung H, et al. JAMA Dermatol. 2013;149:1173–1179.
8. National Psoriasis Foundation. The psoriasis and psoriatic arthritis pocket guide, 3rd Edition. 2009.
9. National Institutes of Health (NIH) – Senior Health. Psoriasis: causes and risk factors. www.nihsenior health.gov/psoriasis/causesandriskfactors/01.html.
10. UpToDate. Patient education: Psoriasis (Beyond the Basics). https://www.uptodate.com/contents/psoriasis-beyond-the-basics
11. Rapp SR, et al. J Am Acad Dermatol. 1999; 1(3 Pt 1): 01–407.
12. Armstrong AW, et al. PLoS One. 2012;7:e52935.
13. Hrehorow E, et al. Acta Derm Venereol. 2012;92:67–72.
14. Gupta MA, Gupta AK. Am J Clin Dermatol. 2003;4:833–842.
15. Connor CJ, et al. Dermatology Research and Practice. 2015;2015:409637.
16. Singh SM, et al. Cutis. 2016;97(2):107–12.
17. Lebwohl MG, et al. J Am Acad Dermatol. 2014;70:871–881.
18. Patient.info. Chronic plaque psoriasis, 2015. http://patient.info/doctor/chronic-plaque-psoriasis.
19. Mease PJ, et al. Drugs. 2014;74:423–441.
20. Tinazzi I, et al. Rheumatology (Oxford). 2012;51:2058–2063.
21. Mease PJ, et al. J Am Acad Dermatol. 2013.69:729–735.
22. Gladman D. Ann Rheum Dis. 2006;65(Suppl III): iii22–iii24.
23. Arthritis Foundation. Psoriatic Arthritis Diagnosis. http://www.arthritis.org/about-arthritis/types/psoriatic-arthritis/diagnosing.php
24. Gottlieb A, et al. J Am Acad Dermatol. 2008;58:851–864.
25. NICE. Psoriasis: assessment and management. 2012.
26. AAD Psoriasis: Combinations of topical therapies. https://www.aad.org/practice-tools/quality-care/clinical-guidelines/psoriasis/topical-therapy/combinations-of-topical-therapies.
27. Brown KK, et al. J Am Acad Dermatol. 2006;55:607–613.
28. van de Kerkhof PC, et al. Dermatology. 2000;200:292–298.
29. Gottlieb AB. Nat Rev Drug Discov. 2005;4:19–34.
30. Villasenor-Park J, et al. Cleve Clin J Med. 2012;79:413–423.
31. Shear NH. Drug Saf. 2006;29:49–66.
32. Ferrandiz C, et al. Clin Dermatol. 2010;28:81–87.
33. de Felice C, et al. Biologics. 2007;1:11–18.
34. Aldredge LM, Young MS. J Dermatol Nurses Assoc. 2016;8:14–26.
35. Hsu L, et al. Expert Rev Clin Immunol. 2013;9:949–958.
36. Eli Lilly Ltd. Summary of Product Characteristics. Taltz (ixekizumab). Updated 25 April 2016.
37. Shear NH. Drug Saf. 2006;29:49–66.
38. Nestle FO, et al. N Engl J Med. 2009;361:496–509.
39. Ivanov S, Linden A. Trends Pharmacol Sci. 2009;30:95–103.
40. Martin DA, et al. J Invest Dermatol. 2013;133:17–26.
41. Iwakura Y. J Clin Invest. 2006;116:1218–1222.
42. Ettehadi P, et al. Clin Exp Immunol. 1994;96:146–51.
43. Piskin G, et al. J Immunol. 2006;176:1908–1915.
44. Yawalkar N. J Invest Dermatol. 1998;111:1053–1057.
45. Sathish JG, et al. Nat Rev Drug Discov. 2013;12:306–324.
46. AbbVie Pty Limited. PI. Humira (adalimumab). Oct 2016.
47. Pfizer AU Pty Limited. PI. Enbrel (etanercept). Nov 2016.
48. Janssen-Cilag Pty Ltd. PI Remicade (infliximab). April 2016.
49. Janssen-Cilag Pty Ltd. PI. Stelara (ustekinumab). Aug 2016.
50. Novartis Pharmaceuticals Australia Pty Ltd. PI. Cosentyx (secukinumab). Oct 2016.
51. Eli Lilly Australia Pty Ltd. PI. Taltz (ixekizumab). Jan 2017.
52. Levin EC, et al. J Derm Treat. 2014;25:78–82.
53. Hsu L, et al. Br J Dermatol. 2014;170:261–73.
54. Blair HA, Dhillon S. Drugs. 2016;76:1023–30.
55. Strober B. Practical Dermatology. 2016. http://practicaldermatology.com/2016/07/monitoring-biologic -therapy-in-psoriasis-a-primer/
56. Kerdel F, et al. Dermatologic Therapy. 2015;28:390–403.
57. Royal College of Nursing. Assessing, managing and monitoring biologic therapies for inflammatory arthritis. April 2003.
58. British Association of Dermatologists. UK Biologics Checklist. 2014.
59. Pearce DJ, et al. Dermatology Nursing. 2005;17:265-270, 295.
60. Abrouk M, et al. Dermatol Ther (Heidelb). 2016;6:325–331.
61. Merck Sharp & Dohme Limited. Summary of Product Characteristics. Remicade (infliximab). Jul 2016.
DermatologyResearch ReviewTM
SUBSCRIBE free, click here to visit www.researchreview.com.au and update your subscription to Dermatology Research Review.





























