Embed Size (px)
Citation preview
Dr R Clarke www.askdoctorclarke.com 1
Dermatology Notes
Introduction Don’t forget the history Duration of lesion and change with time Where is affected Itching Topical treatment General health Effect on patient’s life FH- particularly atopic, psoriasis and “moles” and skin cancer Drugs- eg causing allergic reactions, including fixed drug eruptions Occupation Examination Skin is largest organ in body and ideally you’d like to check all of it. Essential to check nails Plus scalp, umbilicus, natal cleft, groin (common sites for psoriasis) Important definitions Flat Raised Less than 1cm Macule Papule or nodule More than 1cm Patch Plaque Try to describe skin lesions as accurately as possible This is just as important as knowing the correct diagnosis ?flat ?raised ?clearly defined margin (like psoriasis and unlike eczema) ie cut off between normal and abnormal ?how regular is margin: smooth in outline or irregular Size Site / distribution ?Scaling or ulceration (implies involvement of epidermis) Colour- eg red or purple
Dr R Clarke www.askdoctorclarke.com 2
Dermatology
Examples of Clinical Pictures Suitable for Examinations
1) Look at the pictures that follow and try to describe the lesions as accurately as you can.
2) If you can, attempt a diagnosis 3) If you know what the lesion is, write short notes on the condition 4) Once you’ve committed yourself to paper, have a look at the
answers and notes which follow.
Dr R Clarke www.askdoctorclarke.com 3
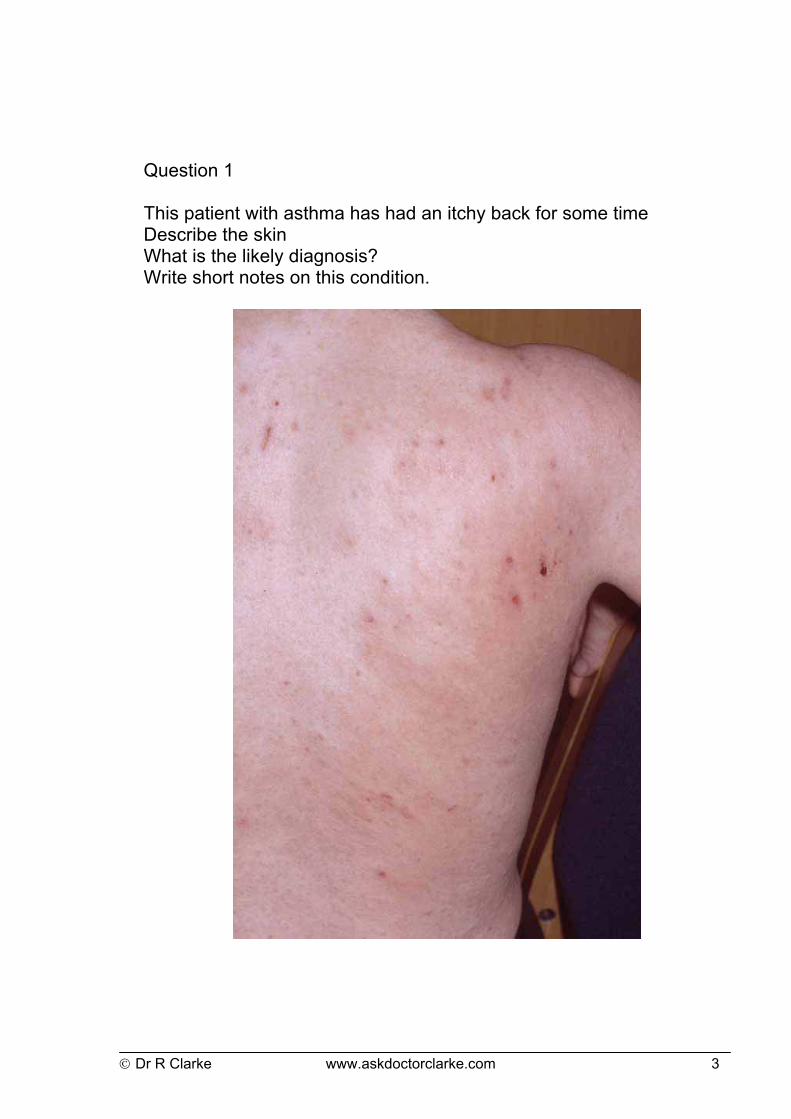
Question 1 This patient with asthma has had an itchy back for some time Describe the skin What is the likely diagnosis? Write short notes on this condition.
Dr R Clarke www.askdoctorclarke.com 4
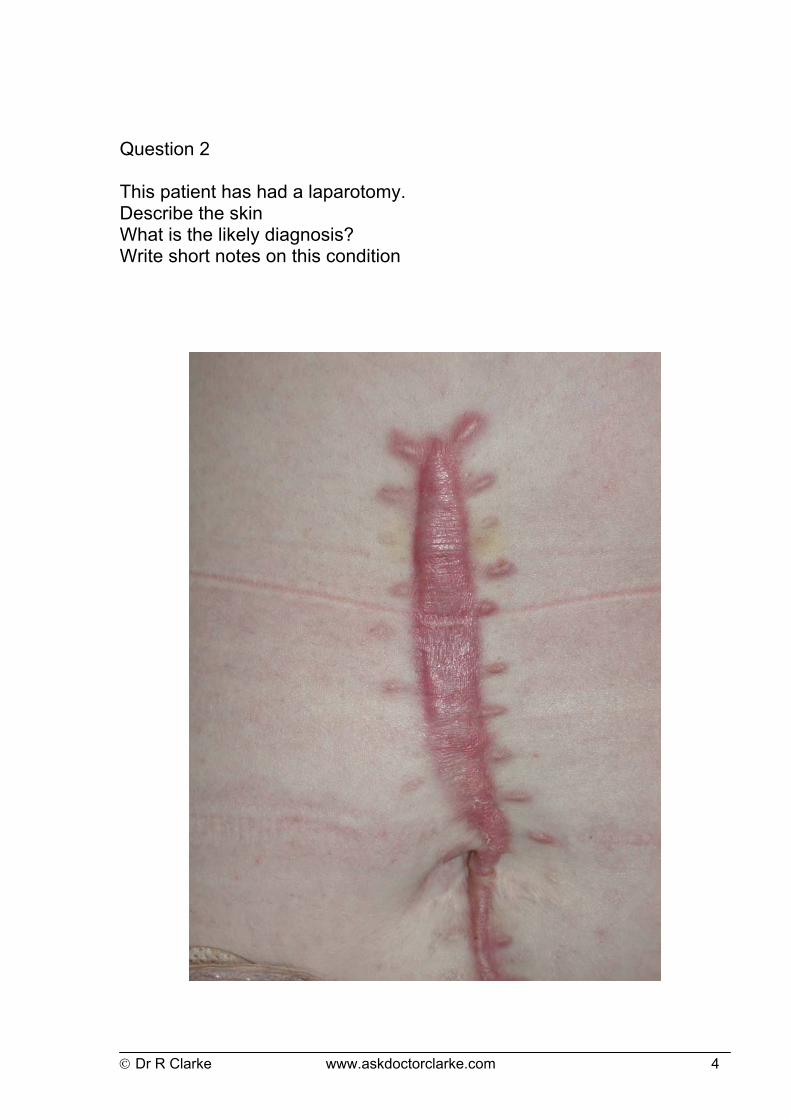
Question 2 This patient has had a laparotomy. Describe the skin What is the likely diagnosis? Write short notes on this condition

Dr R Clarke www.askdoctorclarke.com 5
Question 3 This patient has had type 1 diabetes for several years. He complains that the skin on his shins looks inflamed, though it is not itchy or painful. Describe the skin. What is the likely diagnosis? Write short notes on this condition
Dr R Clarke www.askdoctorclarke.com 6
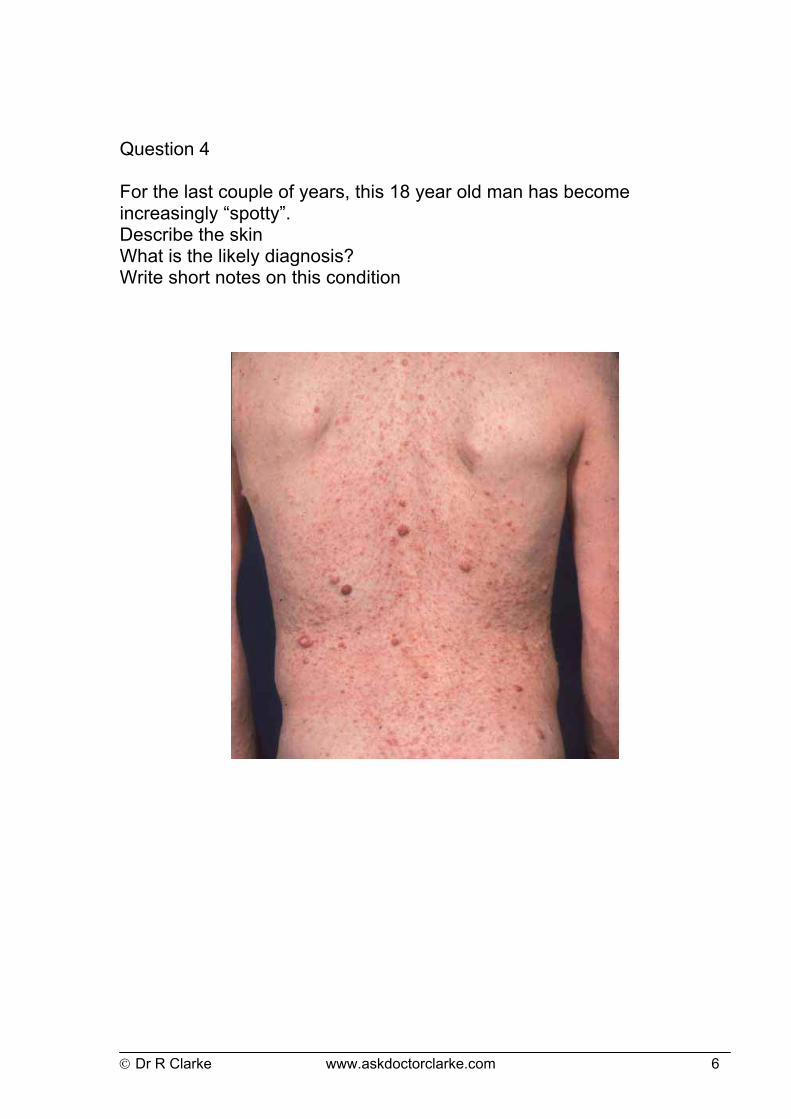
Question 4 For the last couple of years, this 18 year old man has become increasingly “spotty”. Describe the skin What is the likely diagnosis? Write short notes on this condition
Dr R Clarke www.askdoctorclarke.com 7
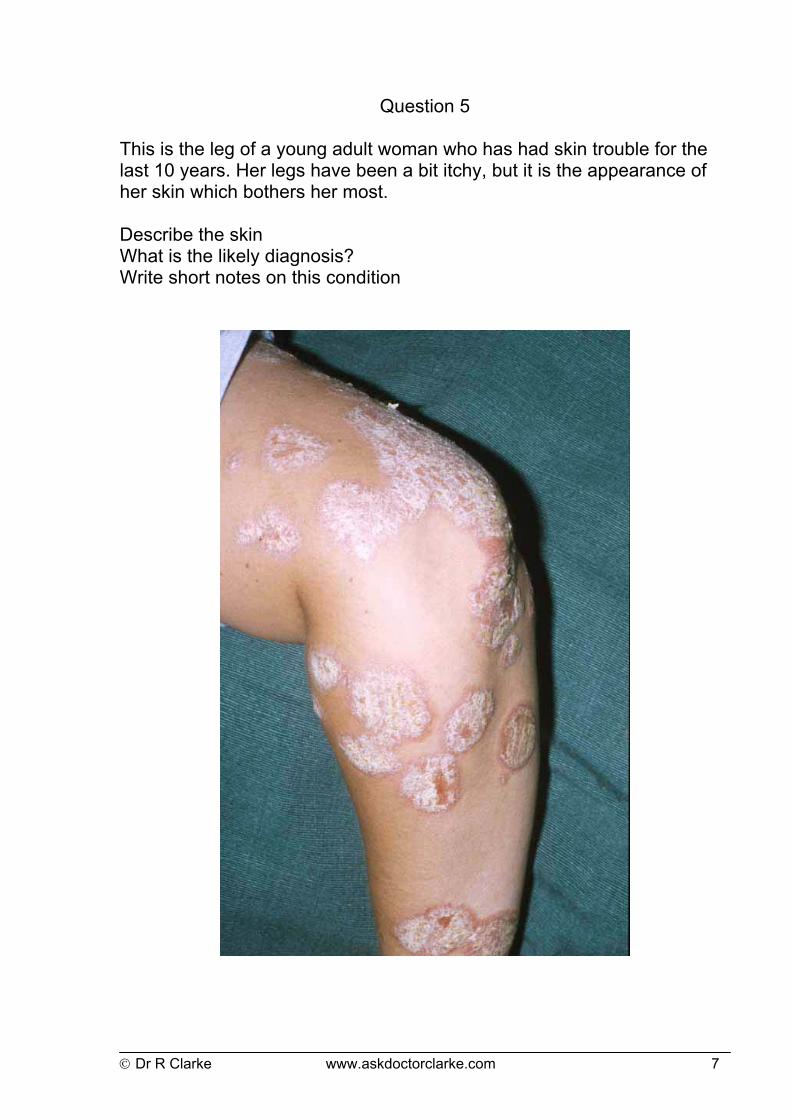
Question 5 This is the leg of a young adult woman who has had skin trouble for the last 10 years. Her legs have been a bit itchy, but it is the appearance of her skin which bothers her most. Describe the skin What is the likely diagnosis? Write short notes on this condition
Dr R Clarke www.askdoctorclarke.com 8
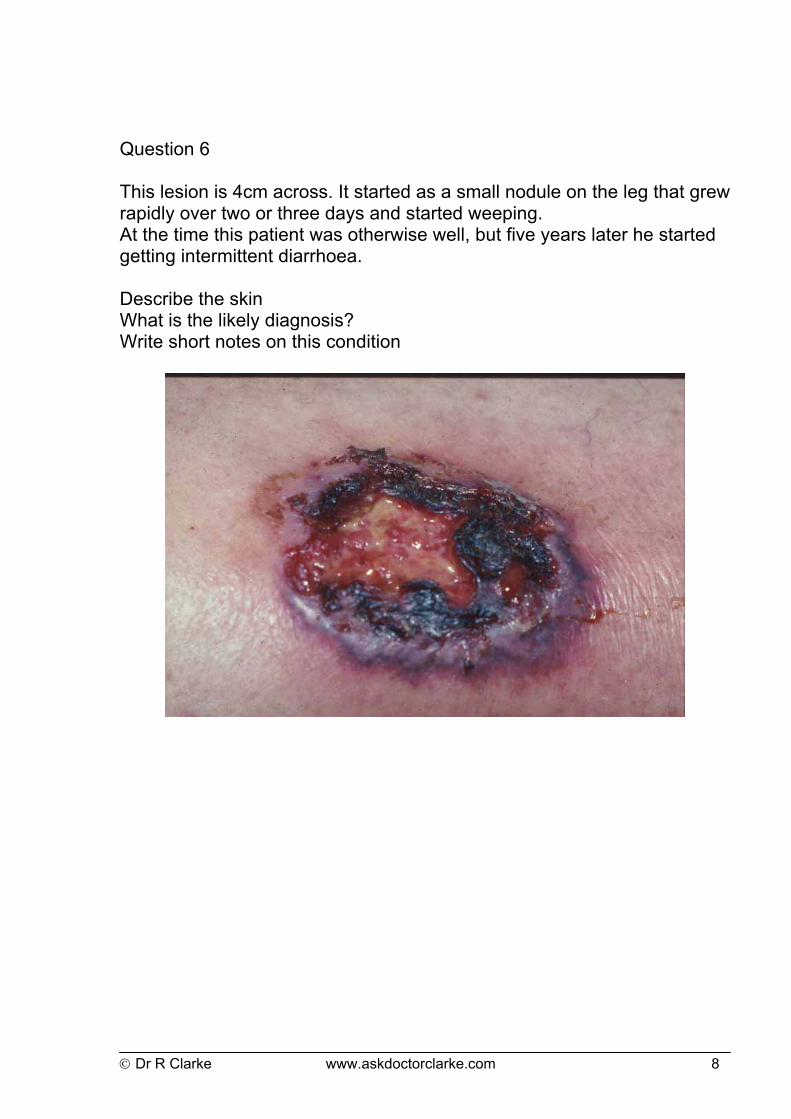
Question 6 This lesion is 4cm across. It started as a small nodule on the leg that grew rapidly over two or three days and started weeping. At the time this patient was otherwise well, but five years later he started getting intermittent diarrhoea. Describe the skin What is the likely diagnosis? Write short notes on this condition
Dr R Clarke www.askdoctorclarke.com 9
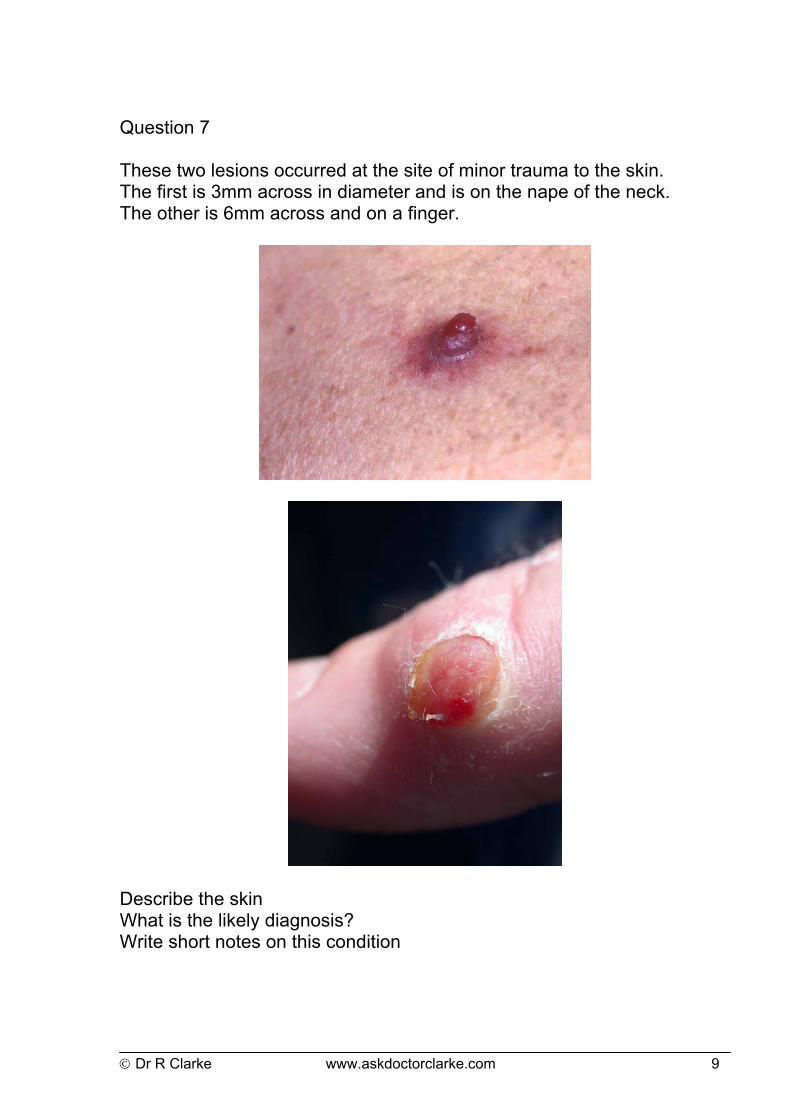
Question 7 These two lesions occurred at the site of minor trauma to the skin. The first is 3mm across in diameter and is on the nape of the neck. The other is 6mm across and on a finger.
Describe the skin What is the likely diagnosis? Write short notes on this condition
Dr R Clarke www.askdoctorclarke.com 10
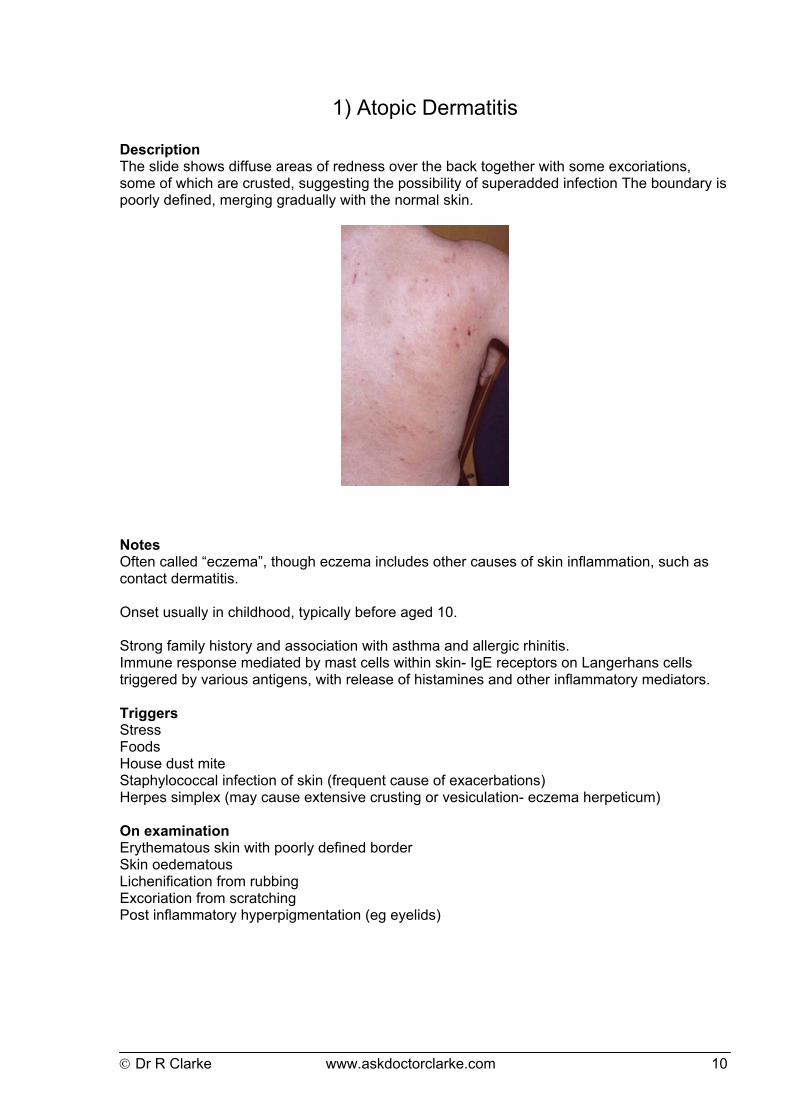
1) Atopic Dermatitis Description The slide shows diffuse areas of redness over the back together with some excoriations, some of which are crusted, suggesting the possibility of superadded infection The boundary is poorly defined, merging gradually with the normal skin.
Notes Often called “eczema”, though eczema includes other causes of skin inflammation, such as contact dermatitis. Onset usually in childhood, typically before aged 10. Strong family history and association with asthma and allergic rhinitis. Immune response mediated by mast cells within skin- IgE receptors on Langerhans cells triggered by various antigens, with release of histamines and other inflammatory mediators. Triggers Stress Foods House dust mite Staphylococcal infection of skin (frequent cause of exacerbations) Herpes simplex (may cause extensive crusting or vesiculation- eczema herpeticum) On examination Erythematous skin with poorly defined border Skin oedematous Lichenification from rubbing Excoriation from scratching Post inflammatory hyperpigmentation (eg eyelids)
Dr R Clarke www.askdoctorclarke.com 11
If infected: Crusts Exudation common Folliculitis (tiny spots related to infected hair follicles) Distribution Flexures: antecubital and popliteal fossa Dorsum of hands and wrists Neck Eyelids Differential Contact dermatitis (eg nickel allergy- jean studs, ear rings etc) Seborrhoeic dermatitis Psoriasis Scabies And others Treatment Hydrate skin with regular emollients ? careful use of sedative antihistamines at night to reduce the itch scratch cycle Topical steroids, using ointments wherever possible Nose swab if flare occurs as staph common- treat both nasal reservoir (eg topical neomycin) and may need systemic antibiotics (eg erythromycin or flucloxacillin).
Dr R Clarke www.askdoctorclarke.com 12
2) Keloid
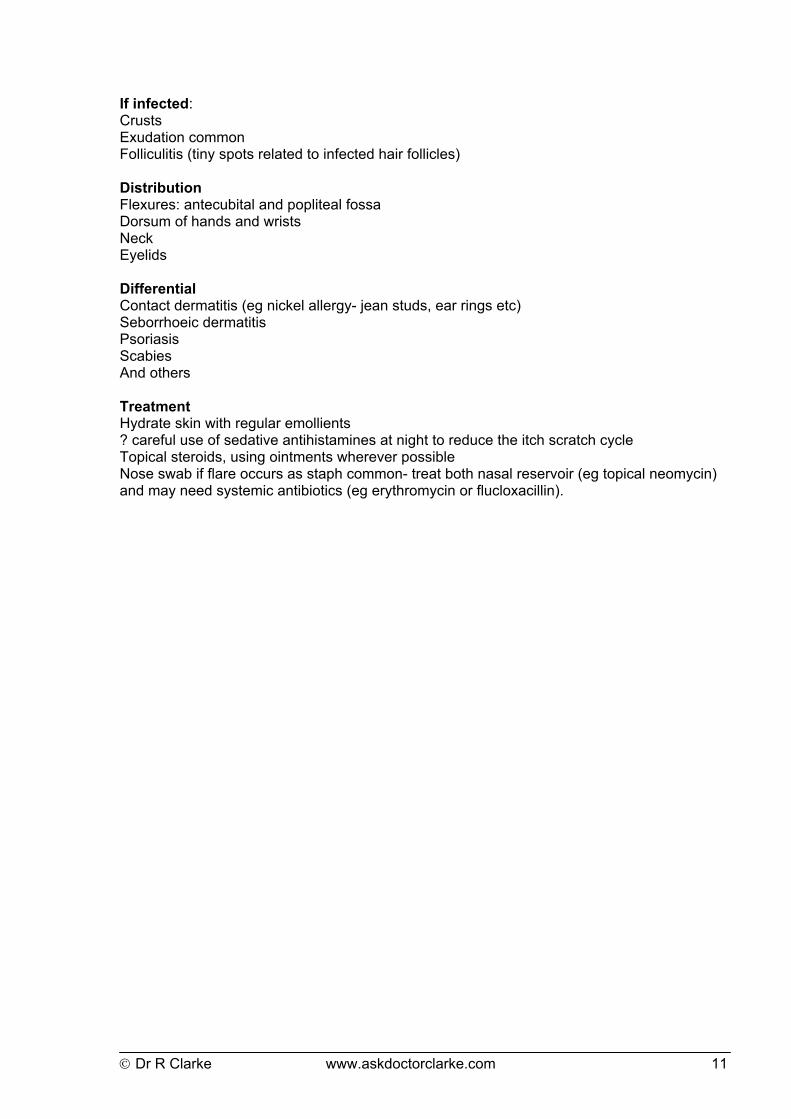
Description Hypertrophic laparotomy scar: raised purplish elongated plaque with smooth surface and very sharply defined border, together with smaller lesions at the site of stich insertion/
Notes Hypertrophic scar tissue extending beyond site of original injury Common in those with pigmented skin Typically occurs in 20’s and 30’s but may occur at any age. On examination Elevated scar tissue Linear or occasionally nodular (eg ear lobe) Firm Tender Smooth shiny surface Often with red or purplish tinge Distribution Chest Shoulders Upper arms Upper back Ear lobes Differential Usually typical appearance If nodular, ? dermatofibroma Avoid diagnostic biopsy as can induce further extension of keloid

Dr R Clarke www.askdoctorclarke.com 13
Treatment Prevention- avoid surgery if possible in risky areas in those who scar badly; always ask about previous scarring and warn of risks Observation and reassurance- sometimes keoids can get flatter with time, though very slow process Intralesionsal injection of steroid- often helps reduce size or degree of protruberance Surgical excision- high risk of recurrence; some success with post op radiotherapy to wound.
Dr R Clarke www.askdoctorclarke.com 14
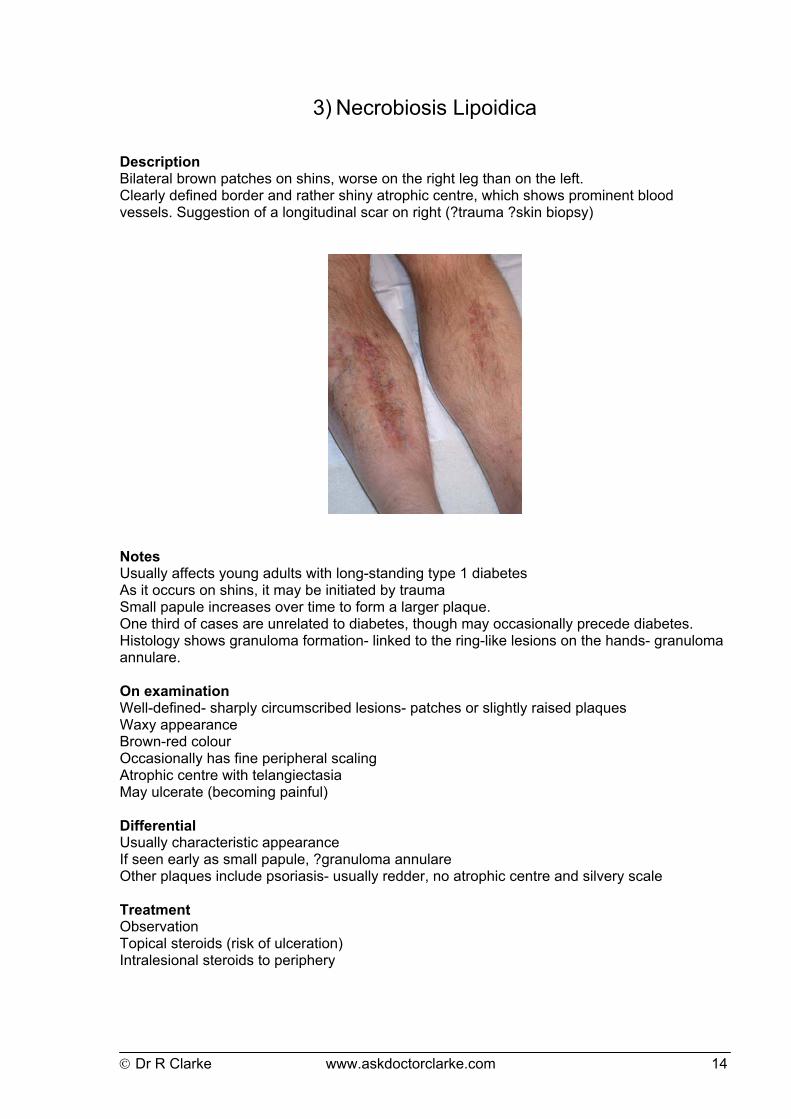
3) Necrobiosis Lipoidica Description Bilateral brown patches on shins, worse on the right leg than on the left. Clearly defined border and rather shiny atrophic centre, which shows prominent blood vessels. Suggestion of a longitudinal scar on right (?trauma ?skin biopsy)
Notes Usually affects young adults with long-standing type 1 diabetes As it occurs on shins, it may be initiated by trauma Small papule increases over time to form a larger plaque. One third of cases are unrelated to diabetes, though may occasionally precede diabetes. Histology shows granuloma formation- linked to the ring-like lesions on the hands- granuloma annulare. On examination Well-defined- sharply circumscribed lesions- patches or slightly raised plaques Waxy appearance Brown-red colour Occasionally has fine peripheral scaling Atrophic centre with telangiectasia May ulcerate (becoming painful) Differential Usually characteristic appearance If seen early as small papule, ?granuloma annulare Other plaques include psoriasis- usually redder, no atrophic centre and silvery scale Treatment Observation Topical steroids (risk of ulceration) Intralesional steroids to periphery
Dr R Clarke www.askdoctorclarke.com 15
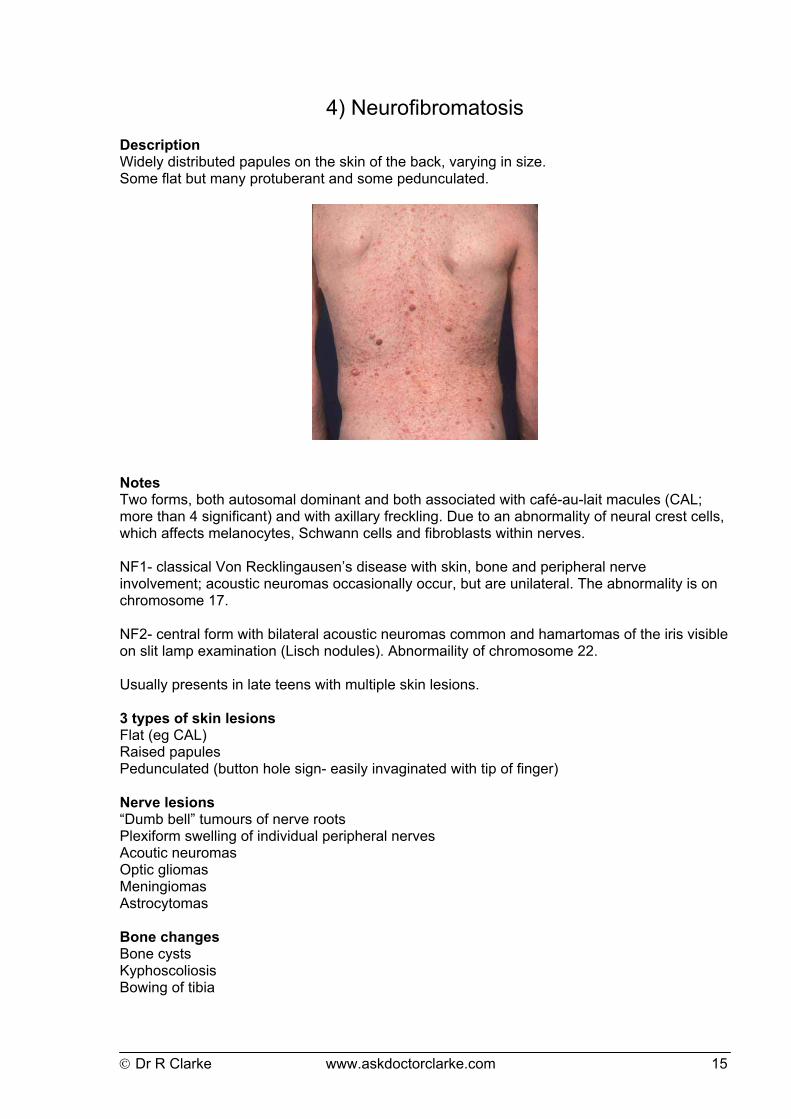
4) Neurofibromatosis Description Widely distributed papules on the skin of the back, varying in size. Some flat but many protuberant and some pedunculated.
Notes Two forms, both autosomal dominant and both associated with café-au-lait macules (CAL; more than 4 significant) and with axillary freckling. Due to an abnormality of neural crest cells, which affects melanocytes, Schwann cells and fibroblasts within nerves. NF1- classical Von Recklingausen’s disease with skin, bone and peripheral nerve involvement; acoustic neuromas occasionally occur, but are unilateral. The abnormality is on chromosome 17. NF2- central form with bilateral acoustic neuromas common and hamartomas of the iris visible on slit lamp examination (Lisch nodules). Abnormaility of chromosome 22. Usually presents in late teens with multiple skin lesions. 3 types of skin lesions Flat (eg CAL) Raised papules Pedunculated (button hole sign- easily invaginated with tip of finger) Nerve lesions “Dumb bell” tumours of nerve roots Plexiform swelling of individual peripheral nerves Acoutic neuromas Optic gliomas Meningiomas Astrocytomas Bone changes Bone cysts Kyphoscoliosis Bowing of tibia

Dr R Clarke www.askdoctorclarke.com 16
Malignant change Significant risk of development of neurosarcoma in later life Associated with phaeochromocytoma Careful review of blood pressure is essential Examination hint Though rare, this is a chronic condition and patients are often under regular review, so may occur in examinations. Main task is to describe the multiple macules, papules and pedunculated lesions, commenting on presence of CAL and axillary freckling. Emphasise the importance of checking blood pressure and the association with acoutic neuroma. The first clinical sign of an acoutic neuroma is usually loss of the corneal reflex due to involvement of trigeminal nerve, adjacent to acoustic nerve in cerebello-pontine angle.
Dr R Clarke www.askdoctorclarke.com 17
5) Psoriasis
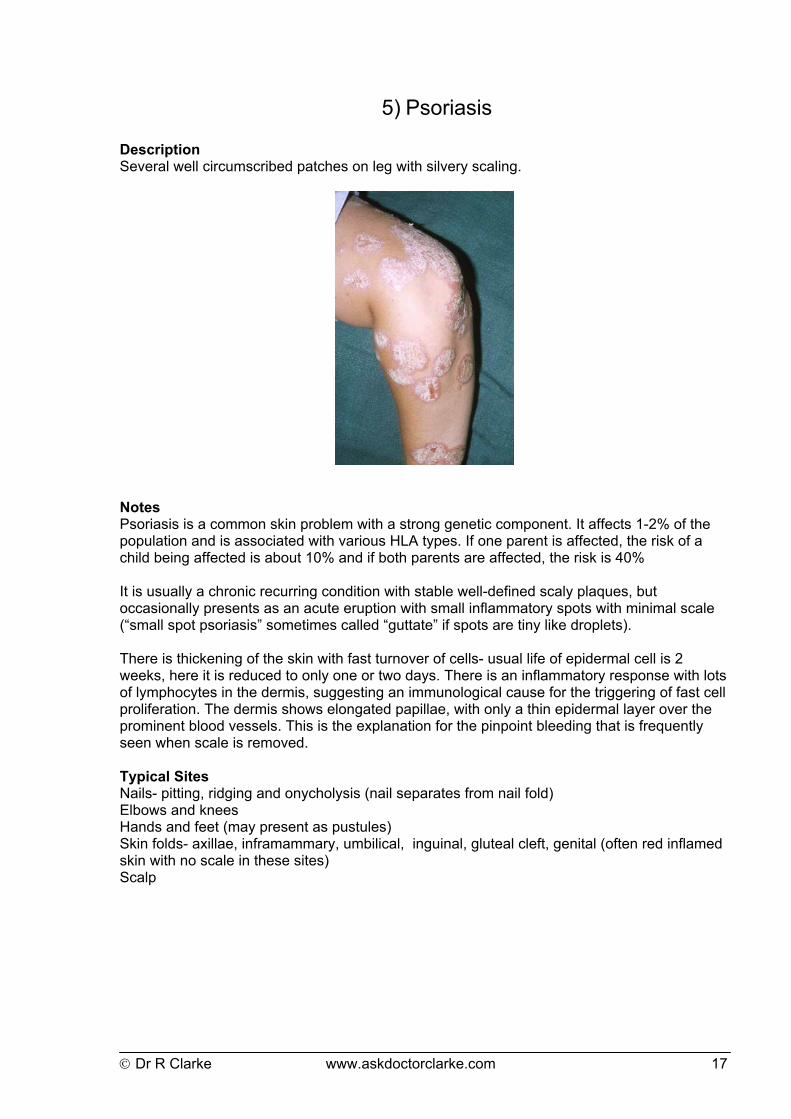
Description Several well circumscribed patches on leg with silvery scaling.
Notes Psoriasis is a common skin problem with a strong genetic component. It affects 1-2% of the population and is associated with various HLA types. If one parent is affected, the risk of a child being affected is about 10% and if both parents are affected, the risk is 40% It is usually a chronic recurring condition with stable well-defined scaly plaques, but occasionally presents as an acute eruption with small inflammatory spots with minimal scale (“small spot psoriasis” sometimes called “guttate” if spots are tiny like droplets). There is thickening of the skin with fast turnover of cells- usual life of epidermal cell is 2 weeks, here it is reduced to only one or two days. There is an inflammatory response with lots of lymphocytes in the dermis, suggesting an immunological cause for the triggering of fast cell proliferation. The dermis shows elongated papillae, with only a thin epidermal layer over the prominent blood vessels. This is the explanation for the pinpoint bleeding that is frequently seen when scale is removed. Typical Sites Nails- pitting, ridging and onycholysis (nail separates from nail fold) Elbows and knees Hands and feet (may present as pustules) Skin folds- axillae, inframammary, umbilical, inguinal, gluteal cleft, genital (often red inflamed skin with no scale in these sites) Scalp
Dr R Clarke www.askdoctorclarke.com 18
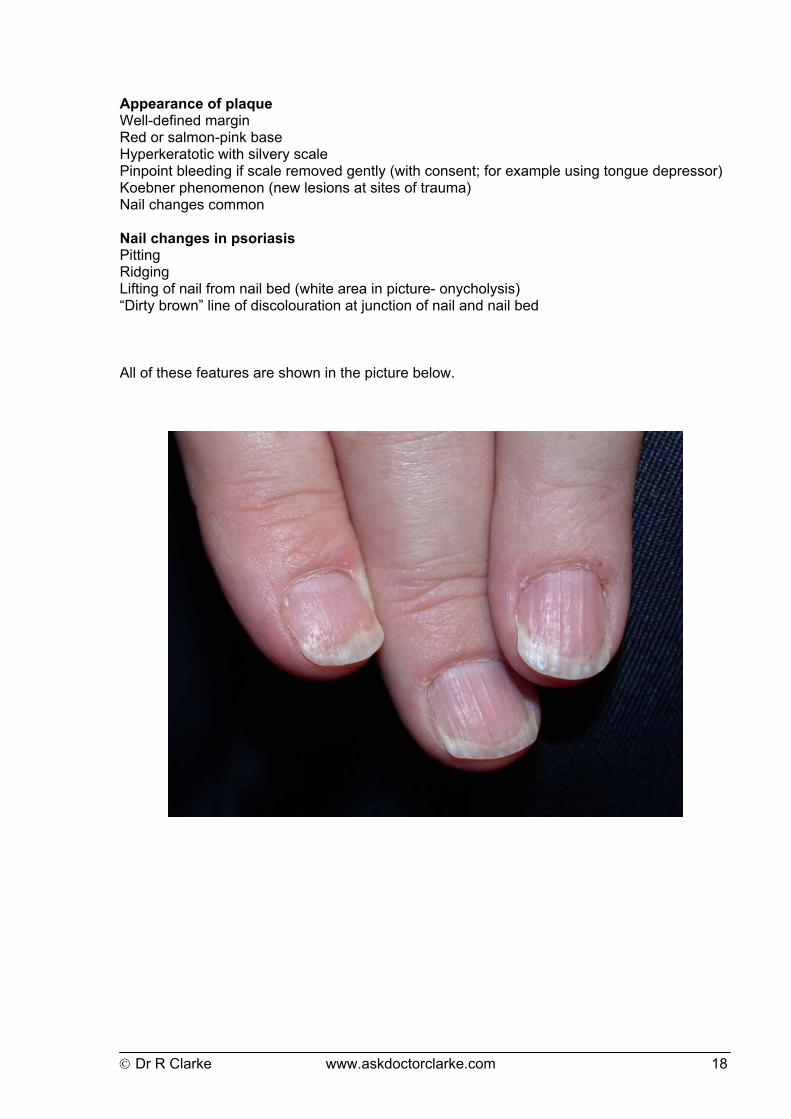
Appearance of plaque Well-defined margin Red or salmon-pink base Hyperkeratotic with silvery scale Pinpoint bleeding if scale removed gently (with consent; for example using tongue depressor) Koebner phenomenon (new lesions at sites of trauma) Nail changes common Nail changes in psoriasis Pitting Ridging Lifting of nail from nail bed (white area in picture- onycholysis) “Dirty brown” line of discolouration at junction of nail and nail bed All of these features are shown in the picture below.
Dr R Clarke www.askdoctorclarke.com 19
Atypical forms When it affects hands and feet, it appears as pustular psoriasis When triggered by infection (eg strep throat) it may appear as “small spot psorasis” or guttate psoriasis. Differential diagnosis of scaly lesions Seborhoeic dermatitis (scale less silvery- more yellow in colour) Fungal infection (tinea) Lichen simplex (itch scratch cycle causing thickening of skin) Psoriaform drug eruption- eg beta blockers, gold Mycosis fungoides (well defined plaques on trunk) Small spot psoriasis Sometimes it presents as an acute eruption with “small spot” psoriasis- these are sometimes distributed like tiny droplets (“guttate”) or larger coin lesions (“nummular”). Quite often this generalised eruption may follow a streptococcal throat infection, but sometimes idiopathic. May resolve spontaneously, but sometimes progresses to chronic plaque psoriasis. Differential diagnosis of small spot psoriasis Pityriasis rosea (often has peripheral scale) Secondary syphilis Drug eruptions (gold, beta blockers etc) Treatment options: for localised stable plaques Topical steroid ointments +/- salicylic acid (to remove scale) +/- occlusion Topical vitamin D analogues (eg calcipotriol) Tar based preparations (eg dithranol) For more extensive generalised psoriasis Phototherapy (UV B) Photochemotherapy (UV A plus oral psoralen) Methotrexate Cyclosporin
Dr R Clarke www.askdoctorclarke.com 20
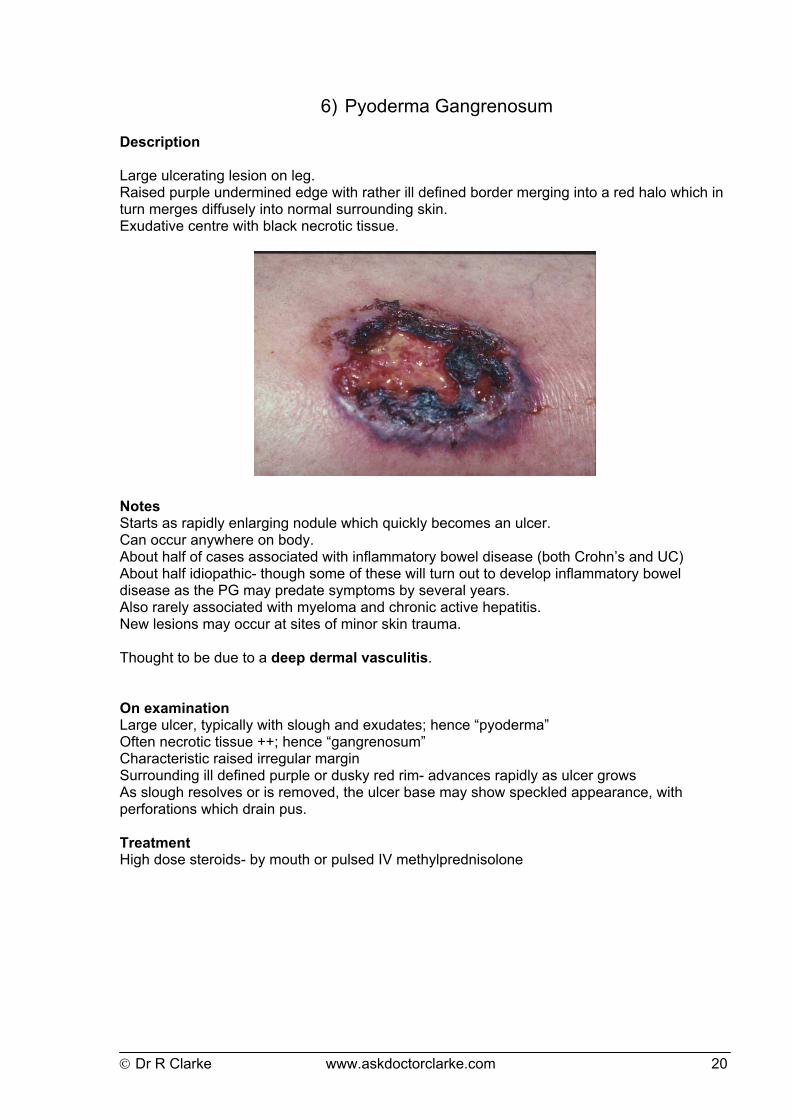
6) Pyoderma Gangrenosum Description Large ulcerating lesion on leg. Raised purple undermined edge with rather ill defined border merging into a red halo which in turn merges diffusely into normal surrounding skin. Exudative centre with black necrotic tissue.
Notes Starts as rapidly enlarging nodule which quickly becomes an ulcer. Can occur anywhere on body. About half of cases associated with inflammatory bowel disease (both Crohn’s and UC) About half idiopathic- though some of these will turn out to develop inflammatory bowel disease as the PG may predate symptoms by several years. Also rarely associated with myeloma and chronic active hepatitis. New lesions may occur at sites of minor skin trauma. Thought to be due to a deep dermal vasculitis. On examination Large ulcer, typically with slough and exudates; hence “pyoderma” Often necrotic tissue ++; hence “gangrenosum” Characteristic raised irregular margin Surrounding ill defined purple or dusky red rim- advances rapidly as ulcer grows As slough resolves or is removed, the ulcer base may show speckled appearance, with perforations which drain pus. Treatment High dose steroids- by mouth or pulsed IV methylprednisolone
Dr R Clarke www.askdoctorclarke.com 21
7) Pyogenic Granuloma
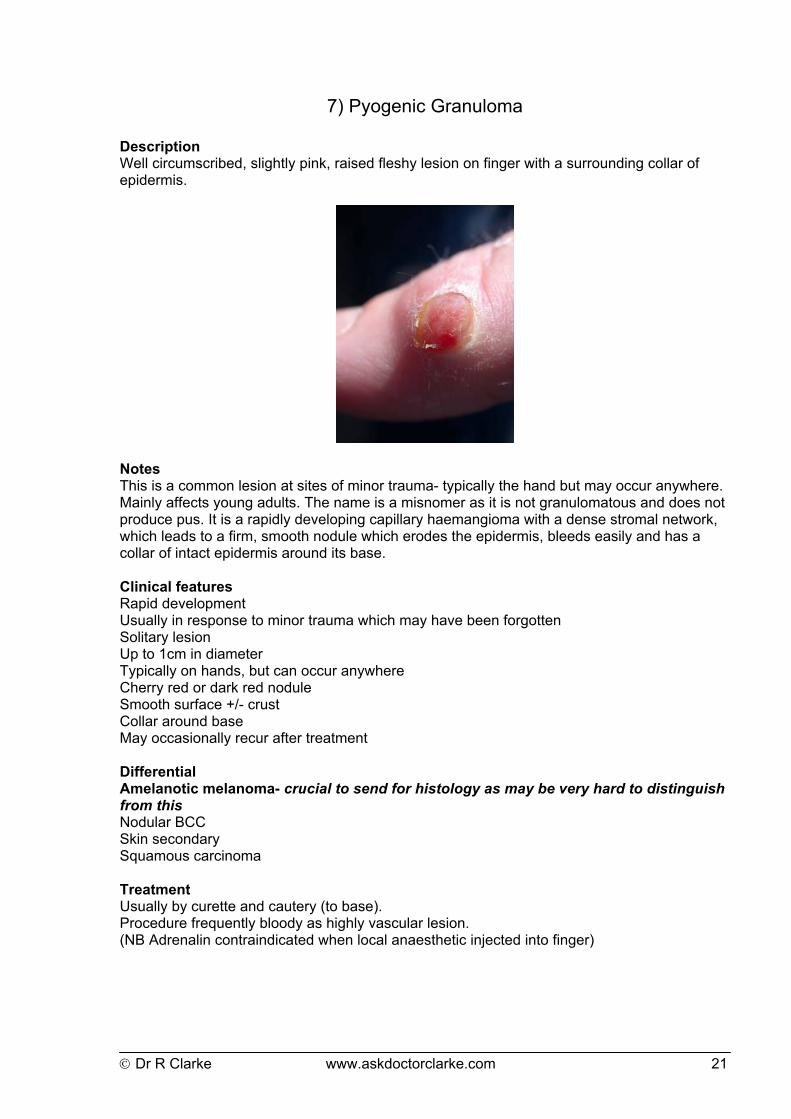
Description Well circumscribed, slightly pink, raised fleshy lesion on finger with a surrounding collar of epidermis.
Notes This is a common lesion at sites of minor trauma- typically the hand but may occur anywhere. Mainly affects young adults. The name is a misnomer as it is not granulomatous and does not produce pus. It is a rapidly developing capillary haemangioma with a dense stromal network, which leads to a firm, smooth nodule which erodes the epidermis, bleeds easily and has a collar of intact epidermis around its base. Clinical features Rapid development Usually in response to minor trauma which may have been forgotten Solitary lesion Up to 1cm in diameter Typically on hands, but can occur anywhere Cherry red or dark red nodule Smooth surface +/- crust Collar around base May occasionally recur after treatment Differential Amelanotic melanoma- crucial to send for histology as may be very hard to distinguish from this Nodular BCC Skin secondary Squamous carcinoma Treatment Usually by curette and cautery (to base). Procedure frequently bloody as highly vascular lesion. (NB Adrenalin contraindicated when local anaesthetic injected into finger)