Embed Size (px)
Citation preview

Abridged from the
Dermatology Foundation
Progress in Dermatology
Editor: Alan N. Moshell , MD.
Atopic Dermatitis: Recent Trends in Pathogenesis and Therapy
Kevin D. Cooper Immunodermatology Unit, Department of Dermatology, Universiry of Michigan Medical School; and Ann Arbor Veterans Administration Medical Center, Ann Arbor, Michigan, U .S.A.
Emerging concepts in the areas related to the pathogenesis and treatment of atopic dermatitis are reviewed. In particular, recent findings have revealed several key steps in the maintenance of a vicious circle of spongiotic dermatitis associated with elevated T -lymphocyte activation, hyperstimulatory Langerhans cells, defective cell-mediated immunity, and B-cell IgE overproduction. The discovery of specific IgEbinding structures on Langerhans cells provides a mechanism for Langerhans cells to capture and present IgE-targeted allergens to allergen-specific T cells. Furthermore, certain microbial allergens that tend to preferentially elicit IgE-type responses also elicit a T-cell response dominated by the IgEinducing lymphokine interleukin 4. Repeated stimulation by activated Langerhans cells appears to induce just such a response. Abnormal biochemical responsiveness and mediator release by AD monocytes, mast cells, and eosinophils also participate in the sustainment or initiation of such a vicious circle, and contribute directly to the dermatitis as well. Developments in the areas of neuropeptides, genetics, microbial superantigens, and cytokine networks in the skin also appear to have promise in providing a rational link between immune defects and the inflammatory events in AD.
Recent a~vances in the pathog,eneSiS of atopic dermatitis are leadmg to novel forms of therapies for this disease, which can have enormous impact, not only on the life of the patient, but also on his or her family. An understanding of these developments and the underlying
biology is critical to successful physician utilization of our cllrrently available agents and newer agents that are currently under develop-
Reprint requests to: Dr. Kevin D. Cooper, Immunodermatology Unit, Universiry of Michigan, R5548 Kresge IjCampus Box 0530, Ann Arbor, MI48109.
Conventional therapy remains the mainstay of atopic dermatitis management; however, new therapies based upon the above concepts are being tested in clinical trials. Although the difficulty of objectively grading AD lesional activity and the high placebo response of AD patients hampers the interpretation of many reports, several types of approaches are coming into focus. The effectiveness of cyclosporinA, which targets T-cell activation and antigen presentation, indicates that additional agents with such activity should be effective, and verifies the criticality of these cells in AD pathogenesis. Therapy with biologic response modifiers, such as interferon gamma or thymopentin, is oriented toward normalization of imbalanced immune responsiveness, rather than direct suppression of the immune system. The mechanism of action of and toxicities of Chinese herbal mixtures require further investigation, but may reveal hitherto unconsidered avenues. Other recent therapeutic trials have focused on reduction of trigger factors, such as house dust mite exposure, foods, and the abnormal epidermal lipid barrier to irritation. Key words: IgE/immunology/T lymphocytes/antigens. ] Invest Dermatol 102:128-137, 1994
ment. Many concepts of pathogenesis are currently being explored, as evidenced by the activity in the field of atopic dermatitis; among approximately 4000 publications that are currently available on atopic dermatitis, over 1000 have been published just since 1989. For a treatment of this previolls literature, the reader is referred to several wide-ranging articles that review materials prior to 1989 in greater depth than the current manuscript [1-4].
Abbreviations: ELAM, endothelial leukocyte adhesion molecule; MFCTCL, mycosis fungoides - rype cutaneous T -cell lymphoma; VIP, vasoac_ tive intestinal peptide; PDE, phosphodiesterase.
Copyright © 1994 Dermatology Foundation, 1560 Sherman Avenue, Evanston, Illinois 60201
128

VOL. 102, NO. 1 JANUARY 1994
GENETICS
Atopic dermatitis is clearly a genetic disorder. The inherited abnormality appears to be carried in the immune system; atopic dermatitis and antigen-specific IgE reactivity has been transferred into a nonatopic bone-marrow transplantation recipient from an atopic dermatitis donor [6,7). The promise of gene therapy as a future approach for atopic dermatitis is evidenced by the observation that the eczema ofWiskott-Aldrich syndrome cleared following successful engraftment of a nonatopic bone marrow (8). However, progress on identifyi ng the gene for atopic dermatitis is limited [9,10].
CLINICAL IMMUNOLOGY
Abnormalities in the immune system known to be associated with atopic dermatitis include an increased susceptibility to viral and fungal infections, microbes normally handled by T cel ls generated by the delayed-type hypersensitivity (DTH) arm of the immune system. Consonant with such susceptibility, patients are frequently anergic upon intradermal DTH testing. Because atopic dermatitis patients exhibit generally normal ill lIitro proliferative blood T -cell responses to the same antigens to which they exhibit cutaneous anergy (11), the immune defect appears skin limited, and the patients are not considered to be systemically immunosuppressed . Atopic dermatitis patients are, however, deficient in their ability to engage the mechanisms leading to allergic contact dermatitis, w hich also depends upon the generation of antigen-specific T cells. Thus, in a careful quantitative study, atopic dermatitis patients were definitely shown to exhibit an impaired ability to become contact sensitized to dinitrochlorobenzene (DNCB) (12). Impaired sensitization appears to be proportional to the disease severity at the time of immunization [13] . These findings explain the clinical observations that patients with atopic dermatitis develop contact allergic dermatitis less frequently than nonatopic subjects (14). However, because of their heavy exposure to topical medications, atopic dermatitis patients often do exhibit reactivity to contact allergens. The most common allergens for atopic dermatitis patients include fragrance-mix, balsam of Peru, and neomycin, which can be components of these topical agents, as well as nickel [15), so patch testing can be a useful clinical maneuver in discovering trigger factors that can be removed .
In addition to cell-mediated immune defects of the T cell arm, defects in monocyte and neutrophil chemotaxis and phagocytosis are present [2], and may be implicated in susceptibility to bacterial infection, in particular, Staphylococcus aurellS.
IMMUNOPATHOLOGY
Infiltrating Leukocytes Increased numbers of lymphocytes, monocyte/macrophages, and fully granulated mast cells (16) are present in atopic dermatitis lesions. The lymphocytes within atopic dermatitis lesions are predominantly of the CD4 + helper cell phenotype, with a mean CD4: CD8 ratio of7: 1 [17]. A subset ofT cells appears to undergo intralesional activation, as evidenced by their expression of IL-2 receptors (CD25) [18,19)' and the majority express HLA-DR (a class II major histocompatibility complex molecule), which is another, less labile, marker ofT-cell activation. The CD4 + T lymphocytes are of the memory subset (indicating previous encounter with antigen) [20] and express high levels of the skin-homing Sialyllewisx/ c lectin ligand for the endothelialleukocyte adhesion molecule 1 (ELAM-l) [21,22].
EndotheliulIl In addition to histologically evident hypertrophy, endothelial cells in lesional atopic dermatitis skin abnormally express ELAM-l (22) as well as upregulated levels of intercellular adhesion molecule (ICAM-l) [22,23]. Because T cells that express the highest levels of ligands for these endothelial adhesion molecules are those that have recently undergone activation, it is possible that T cells in atopic dermatitis may activate in lymphoid organs (i.e., nodes) prior to landing in the skin. A number of mechanisms may be responsible for the enhanced adhesiveness of atopic dermatitis vasculature for leukocytes: mast cell release of tumor necrosis factor (TNF) can induce ELAM- l [24,25), monocyte or keratino-
ATOPIC DERMATITIS 129
cyte IL-l can induce ELAM-l and ICAM-l [26), and T-cell interleukin 4 (IL-4) can potentiate ELAM-l (27). Thus T-cell activation can lead to enhanced adhesiveness of the microvasculature, either directly through lymphokine release, or indirectly through the release of mast cell-degranulating factors [28], which in turn leads to enhanced binding and extravasation of leukocytes into the lesional milieu, and further increasing the likelihood of addi tional T-cell activation.
Keratinocytes Keratinocytes in lesional atopic dermatitis exhibit evidence of cytokine or lymphokine modulation. In some cases ICAM-l can be visualized on epidermal keratinocytes [23,29], although not universally [18]' and almost always in the absence of HLA-DR (17), indicating that interferon gamma (IFN-y) is not likely to be the inducing lymphokine. CD36 and CDla, and even IgE, have been observed on atopic dermatitis epidermal keratinocytes, f~~the~ testimony to tl~e abnormal cytokine milieu of atopic dermatitis sklJ1 [30,31]. Studies on epidermal cytokine production are limited in atopic dermatitis but abnormalities in IL-l (3 2) and IL-8 [33] have been noted.
Shared Features of Atopic DerlIlatitis and Cutaneous T-Cell LYlIlpholIla (CTCL) The high CD4: CD8 ratios in lesional atopic dermatitis can be as high as that in the mycosis fungoides form of CTCL (MF-CTCL) [34,35]. Combined with exocytosis of activated lymphocytes into the epidermis, the distinction of MFCTCL from active, chronic atopic dermatitis is difficult. The degree of spongiosis in relation to the pattern of infiltration and other features is usually sufficient to make the distinction, but spongiosis and epidermotropism can be altered by the presence of topical corticosteroids, so biopsy of patients withdrawn from steroids is preferred . CTCL can arise in patients with severe atopic dermatitis l36] (unpublished observations), and CTCL can appear as a spongiotic dermatitis in its early stages, so the differential diagnosis can be highly relevant.
Langerhans Cells Lesional skin of atopic dermatitis shares additional abnormal features with CTCL; both exhibit increased numbers of dermal Langerhans cells [37]' as well as epidermal Langerhans cells of abnormal phenotype, and hyperstimulatory antigen-pres~nting.a.ctivity. Such Langerhans cells abnormally express CDlb (111 addltlon to CDla) and CD36, and are able to induce activation of resting T cells from the same individual in the absence of any added antigen [38,3~] . Thus, the normal compartmentalization of LC phenotype that 1S maintained in normal skin (epidermal LC-high CDla, absent CDlb, absent CD36; dermal LC-Iow CDla, positive CDlb, absent CD36) [40] is replaced by a single milieu characteristic of atopic dermatitis in which both epidermal and dermal LC express the same phenotype: CDla and CDlb are both expressed simultaneously at high levels, and in concert with positive CD36 expression [38]. Additional evidence for a markedly modulated LC population in lesional atopic dermatitis skin is the abnormal expression of the interpenetrating reticulum cell marker RFD-l, a molecule normally reserved for dendritic antigenpresenting cells of the T-cell area of lymph nodes [19], and the binding of easily detectable levels of 19E on the Langerhans cells surface.
The abnormal status of atopic dermatitis Langerhans cells may be of significance in both the maintenance of the dermatitis and the tilt of the immune system response in atopic dermatitis toward IgE and eosinophil production with concomitant depression of DTH responses (recently reviewed in [41 D. Whereas normal Langerhans cells are unable to activate resting blood CD4+ T cells from the same individual (autologous T cells and LC) in the absence of added antigens [42], atopic dermatitis lesional Langerhans cells are potent activators of autologous resting CD4+ T lymphocytes under such conditions [38]. In part, the reactivity is due to presentation of self peptides, indicating a component of true autoreactivity [43]. The remaining signal could be due to presentation of processed foreign antigen or binding of microbial superantigen, both of which could result in T-cell activation in the lesion by LC themselves. The signal

130 COOPER
C.N.S. Inflammation
\. I Neuropeptldes
\ o
THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
;;GE~ t Leukocyte
Monocyte ... Recruitment
Other Mediators
lPD~/ J
HOM? /
-:I~------'. su:'~gV IL-S?
Spongiotic Dermatitis
with 1 Cell
Mediated Immunity
=='L. P.ovale? ~
IL-4
IgE ~ ® .~-----.-"" " Eosinophilia
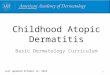
Figure 1. Overview of interacting inflammatory mechanisms in atopic dermatitis. APCs, in particular hyperstimulatory Langerhans cells, present antigens to T cells and induce intralesional T cell activation, lymphokine production, and spongiotic dermatitis. The antigens may be focused on those targeted by IgE (i.e., house dust mite (HOM) or P. Ova/e), because of Fe binding ofIgE on Langerhans ce ll s, or the antigens may be self peptides, or staph super-antigens (Staph Super Ag) . An abnormal balance of neuropeptides in atopic dermatitis skin would appear to favorT -cell activation. Although uncommon in many skin diseases, TH2 cells are present in lesional atopic dermatitis skin. Their production of IL-4 may help promote the hyper IgE of atopic dermatitis, and their putative production of IL-5 may be responsible for eosinophilia in atopic dermatitis. THl cells are also present, but their relative role may be diminished by the overproduction of PGE (selectively inhibitory for THl cells) by abnormal monocytes with elevated cAMP phosphodiesterase. THl cells may also be selectively inhibited by TNF released from mast cells which are easily triggered in atopic dermatitis, possibly in response to T-cell-derived histamine-releasing factor (a putative lymphokine). The diminished role ofTHl in AD is theorized to result in less gamma interferon (IFN) inhibition ofTH2 cells, which, in turn, act to inhibit THl expansion and cell-mediated immunity. Lymphokines and cytokines induce endothelial adhesion molecules and leukocyte recruitment, further propagating the cycle.
for autoreactive T-cell stimulation by lesional epidermis does not arise from keratinocytes themselves presenting antigen or superantigen, because depletion ofleukocytes (leaving all the keratinocytes behind) totally removes the stimulus for T-cell activation [38]. An important concept has recently emerged that CD4 + T cells repeatedly stimulated with activated (cultured) LC differentiate into T lymphocytes that produce high amounts of IL-4 and negligible IFNy [44,45] . Such Tcells are termed "TH2" and exist in a dynamic opposition with "TH 1" type T cells, which produce IFNy, but little IL-4, IL-5 , or IL-I0 [46] .
Because IL-4 induces IgE synthesis and the expression of receptors for IgE on cells, a positive feedback loop might be operative in atopic dermatitis, which is linked to allergic responses. In this concept, IgE directed toward certain allergens is passively bound to Langerhans cells, the IgE captures selected allergens (e.g., dust mite or pollens), which are then internalized and processed by the LC for presentation to T lymphocytes, which in turn are influenced to be of the IL-4 (Th2) type, further boosting IgE production. The evidence for this hypothesis is as follows. Langerhans cells and dendritic dermal cells in atopic dermatitis (and other high-IgE states) [47] have detectable levels ofIgE on their surface [48 - 50], particularly in eczematous skin [51]. This appears to occur by absorption of circulating IgE onto a specific receptor for the Fc portion of the IgE molecule (Fc epSilon R I) [52- 541 and via lectin-like IgE-binding molecules [48]. That the surface IgE might skew the type of antigens presented by Langerhans cells is evidenced by findings that atopic dermatitis Langerhans cell s could only present house dust mite antigen if the Langerhans cells was surface IgE positive [55], and that Langerhans cells pre-incubated with antigen-specific IgE could present that antigen if it were then available to the Langerhans cel ls [48] .
lMMUNOREGULATION
T-Cell Subsets: Thl and Th2 In mice, CD4+ T lymphocytes have been classified according to their profile of lymphokines that they release upon activation. Certain strains of mice tend to generate
immune responses dominated by the Thl subset, which produces large amounts of IFNy, along with IL-2, TNF, and other, less specific lymphokines, but Thl cells produce very little IL-4, IL-5, and IL-lO [46,56] . Thl cells mediate DTH responses, and mice who develop strong Th 1 responses handle microbes requiring DTH responses, like Leishmania, quite effectively [57,58] . This feature may be related to the ability ofThl responses to recruit monocytes and activate macrophages at sites of intracellular infections, and to induce cytolytic T lymphocytes [59] .
Other strains of mice tend to develop a Th2-dominated response; these mice do not handle Leishmania well, but are very effective at handling intestinal parasites, such as NiJ?postrongyloides, which the Thl-generating mice handle poorly l58,60,61]. Th2 cells, in contrast to Th 1 cells , make large amounts ofIL-4, IL-5, and IL-I0, and very little IFNy [46,62]. IL-4 is a potent inducer of B-cell IgE production, IL-5 induces eosinophilia, and IL-I0 depresses DTH responses, possibly at the antigen-presenting cell level [63,64] . All of these features are manifested in the atopic dermatitis state, but may be useful in dealing with helminths (alternatively, helminths may have evolved to elicit an immune response that allows their survival [59,60]). Both the Th 1 and the Th2 responses tend to be self-amplifying and inhibitory to the recipropical subset, such that IL-4 inhibits THl-type responses and IFNy inhibits Th2-type responses [65 ,66]. In humans, Th2 responses appear to dominate over Thl responses in diseases such as lepromatous leprosy (which explains the poor handling of organisms in these patients) [67], in allergic (lgE-associated) disorders [59]. and in the Sezary syndrome variant of cutaneous T-cell lymphoma [68] . Conversely, diseases with IFNy-producing T cells (Thl-type response) include allergic contact dermatitis [69] , tuberculoid leprosy [67], and psoriasis [70 -72].
Atopic dermatitis patients exhibit reduced abil ity to generate IFNy l73 - 75], a situation that could be improved by blocking the activity oflL-4 in the culture [73] , or by removing monocytes [75] . Atopic dermatitis T cel ls appear particularly responsive to IL-4 [76], possibly related to their elevated levels ofIL-4 receptor mRNA [77] .

VOL. 102. NO.1 JANUARY 1994
Lesional skin of patients with allergic conjunctivitis and atopic dermatitis clearly contain T cells of the Th2 type [55.78-84J. Of particular interest was that a high percentage (10-47%) ofTh2 cell clones grown from lesional atopic dermatitis skin appeared to be specific for a house dust mite antigen [80] or for grass pollens [82]. This phenomenon was also quite pronounced in epicutaneous patch tests to aeroallergens [80 - 83J. In one study the frequency of Dermatophagoides pteronyssimls- reactive T-cell clones was estimated to be 0.4 - 2.7%. and 42% of the clones were found to be of the Th2 type [85]; in another study. all of the clones were reactive to the inciting aeroallergen. and 70% were of the Th2 type [86]. Why such high percentages of T cells are reactive to these aeroallergens is unclear: antigen-induced enrichment of antigen-specific T cells is the favored hypothesis, but self-antigen cross-reactivity (autoimmune molecular mimicry), or superantigen-like stimulatory properties of the extracts, or a selection due to the cloning procedure must also be held as possibilities.
Despite the clear presence ofTh2-type T cells, the lesional skin of patients with atopic dermatitis also contains IFNy-producing (Th 1-like) T-cell clones [59,79]; their antigen specificity remains unknown. The actual frequency of Th 1 and Th2 cells in lesions, and their relative roles in initiating or maintaining the dermatitis, will be the focus of much work in coming years. However, the identification ofTh2 cells in atopic dermatitis blood and skin has formed a rational basis for therapeutic intervention with recombinant human IFNy, which should be inhibitory to such cells, in patients with atopic dermatitis [87].
Other T-Cell Abnormalities Depressed DTH and cell-mediated immunity (CMI) in atopic dermatitis may be related to more than the Th 1 /Th2 imbalance concept, and there may be many more ramifications of Th 1/Th2 imbalance than are currently appreciated. Alternatively, a Th 1/Th2 imbalance may be the result of a serious underlying immunoregulatory abnormality. For instance, transforming growth factor beta (TGF/f), a potent immunosuppressive cytokine and tissue regulator, favors the activation ofTh2 over Th 1 cells [60]. Depressed CMI could also be related to a shift of the primary site of T-cell activation from the regional lymph node to the skin; dendritic antigen-presenting cells in atopic dermatitis lymph nodes demonstrate abnormal morphology and reduced interdigitation with T lymphocytes [88]. However, the sera of atopic dermatitis patients clearly displays evidence of ongoing and significant T-cell activation in some location by the elevated levels of soluble IL-2 receptors [89,90] and CD8 molecules [91]. The demonstration of IL-2 receptor bearing T cells in lesional atopic dermatitis skin [19] strongly suggests that the skin is a major source of the shed IL-2 receptors in the serum of these patients.
Activated lymphocytes spill out of their tissue sites and are detectable in the blood of patients with atopic dermatitis. In addition to release of activated CD4 + cells [92J, enlarged (activated) B cells and enlarged CD8+ Cllb+ T cells (putative suppressors) are found increased in the blood of patients with AD [93] , indicating selective circulation of these activated lymphocyte subsets. Indeed, some patients have CD8 + T suppressor cells that, upon removal, can be shown to have been restraining the atopic dermatitis patient's CD4 + proliferative response to herpes simplex virus [94].
Despite the evidence of in llivo activated T cells in atopic dermatitis, blood mononuclear cells of atopic dermatitis patients often exhibit slight reductions in their ability to be stimulated in vitro. In addition to the above-mentioned reductions in IFNy production, atopic dermatitis patients release less IL-l [32,95]' TNF [96], and IL-2 [97] , and proliferate less briskly, possibly due to the selective inhibitory effect on CD4+ T cells of prostaglandin E overproduction by atopic dermatitis monocytes [98]. Decreased proliferation by atopic dermatitis T cells may also reflect the tendency of patients with atopic dermatitis to demonstrate reduced lymphocyte counts in general [93]; in at least one case, erythrodermic flares are associated with CD4+ lymphocytopenia [99] .
Subtle alterations in the proportions of immunoregulatory subsets are present in the blood of atopic dermatitis patients that are not
ATOPIC DERMATITIS 131
currently understood. Reduced numbers of lymphocytes bearing the LFA-3 receptor, CD2, have been documented for years, with the most consistent reduction being found within a subset that expresses CD8 and Fc receptors for IgG (reviewed in [3] and [1 J) , and that may represent a reduction in a CD2 + natural killer-type cell subset [93,100]. Whether this reduction is due to the extreme sensitivity of natural killer cells to topical steroid applications is not yet clear [101].
Alterations in CD4/CD8 ratios are also detectable in atopic dermatitis (reviewed in [1,3,84]), but the ratio can be found to be either elevated or reduced, which I believe relates to how the "small lymphocytes" are electronically separated from the "large monocytes"; in atopic dermatitis this separation is not distinct as it is in normals, likely because of the above-described selective shifts of normally small lymphocytes into the "monocyte-sized" cell cluster following enlargement upon activation. Thus, the lymphocyte ratios can be altered by how the cells are chosen for analysis. In a recent study that reported both small and large cell data, the CD4/CD8 ratio was minimally changed among the small lymphocytes and markedly reduced among the large cells, due primarily to an increase in CD8 + CDl1b+ cells and a decrease of CD4+ cells [93J.
Modulation of the Immune Response by Abnormal Monocytes in Atopic Dermatitis The T-cell activation that occurs as a result of hyper stimulatory Langerhans cells in patients with atopic dermatitis appears to be influenced by several factors. A current hypothesis is that the profile of lymphokines produced by the activated T cells is "tilted," resulting in the unique constellation of atopic dermatitis features that eventuate in spongiotic dermatitis, hyperimmunoglobulinemia of IgE, depressed cell-mediated immunity, tendency to respiratory allergy, and eosinophilia. Recent work by Hanifin el ai, described below, has begun to shed light on how abnormally functioning monocytes with an impaired ability to recognize immunoregulatory signals can affect the nature of T-cell differentiation.
Peripheral blood mononuclear cells, and particularly monocytes, from patients with atopic dermatitis produce elevated levels of prostaglandin E2 (PGE2) [75 ,102]. Although normal CD4+ cells do not adjust to external PGE2 by raising their cyclic adenosine monophosphate (cAMP) phosphodiesterase, atopic dermatitis CD4 + T cells do, resulting in a marked reduction in atopic dermatitis T-cell cAMP levels [103]. Thus, atopic dermatitis monocyte restriction of atopic dermatitis T-cell IFNy lymphokine secretion appears due to both a disordered level of PGE2 production by atopic dermatitis monocytes and an abnormal response on the part of atopic dermatitis T cells to the PGE2 [75J .
Because PGE2 can inhibit THl IFNy, but not TH2 IL-4, PGE oversecretion can tip the balance of the immune response in favor of a TH2 response [104] . The ability of a cAMP phosphodiesterase inhibitor with beneficial clinical activity in atopic dermatitis [105] to reduce atopic dermatitis ill I,ilro IgE secretion by blood mononuclear cells [106] could now be interpreted such that the inhibitor may make atopic dermatitis T-cell IFNy less susceptible to inhibition by atopic dermatitis monocyte PGE2. PGE2 can also act directly on B cells to enhance IgE production [104J. Thus , monocytic series PGE2 overproduction may represent an important factor in the tilt of the atopic dermatitis immune response toward a "TH2-like" immune lymphokine pattern.
Monocytes Monocytes are present in increased numbers in th e lesional skin of atopic dermatitis patients [19,1 07J, and may thereby account for the elevated levels ofPGE series prostaglandins detectable in atopic dermatitis skin [108J . Besides elevated PGE production, atopic dermatitis monocytes are abnormally primed for superoxide production [109], additional evidence of ;n ";"0 activation. The abnormal state of atopic dermatitis mOllocytes may be due to the elevated level of activation ofT lymphocytes [19,38,89] and the monocyte response to stimulation by T-cell lymphokines [110]. However, atopic dermatitis monocytes may exist in an abnormal functional state as a consequence of th eir profound elevation of cAMP phosphodiesterase levels [111] and elevated adenyl ate cyclase

132 COOPER
levels [112]. This abnormality is independent of lesional activity and is present even in the cord blood of infants of atopic parents [113], leading to the speculation that this defect in atopic dermatitis monocyte membrane proteins may be linked to the genetic defect(s) responsible for atopic dermatitis susceptibility, and that cAMP phosphodiesterase levels may be useful as a diagnostic test for atopic dermatitis [114] .
Mast Cells/Basophils Evidence has existed for many years that atopic dermatitis patients experience intermittent mast degranulation (see previous reviews). cAMP agonists (PGE, adrenergic agents, histamine) in normals exert a down-modulatory tone on mast cell or basophil degranulation; an alteration in responsiveness to such agents due to an elevated level of cAMP phosphodiesterase in atopic cells may playa role in the excessive releasibiliry ofbasophils in atopic dermatitis patients [115] and mast cells in atopic dogs l116]. The ability of substance P, a neuropeptide released by cutaneous nerves, to degranulate cutaneous mast cells [117] provides another mechanism for mast cell histamine release that may be highly relevant in explaining the close relationship of psychic stress to cutaneous inflammation in atopic dermatitis.
In addition to the well-appreciated effects of mast cell products on inflammation and itching, the products of mast cells have also been implicated in the epidermal hyperplasia of atopic skin [118]. Furthermore, mast cell release may be a contributing factor in the "tilt" of the atopic dermatitis T-cell response toward Th2 because of their ability to release TNF [24]. TNFa inhibits the growth of Thl IFNy-producing T-cell clones, but not atopic dermatitis skin infiltrating Th2 (IL-4-producing) T-cell clones [81]. Indeed, plasma TNF levels are elevated in the serum of patients with atopic dermatitis, and the levels are tightly correlated with plasma histamine [119] .
Eosinophils High eosinophil counts are common in atopic dermatitis [120] . Whether this is due to the concomitant production of IL-5 by Th2 cells .in atopic dermatitis remains to be established. However, the eosinophils are acutely regulated and undergo activation in correlation with disease activity. Eosinophils degenerate in atopic dermatitis skin [121], presumably releasing the polypeptide crystalloid core of the eosinophil granule, termed major basic protein. This/rotein is distributed extensively in atopic dermatitis dermis, an is also capable of degranulating mast cells (reviewed in [1] and [3]). The eosinophil cationic protein is also useful as a marker of eosinophil activity in vivo; eosinophil cationic protein levels are elevated in atopic dermatitis serum [89,122,123], providing further evidence for eosinophil involvement in atopic dermatitis. Interestingly, eosinophilia was the most sensitive blood element to treatment with IFNy [87,93] and cyc1osporin A [124].
TRIGGER FACTORS
Early recognition of the presence of trigger factors can allow earlier appropriate intervention and less severe exacerbations, and thus are an important part of clinical management. Patients usually learn early in life that wool (lanolin) and harsh detergents are irritating to their skin. A recent study has documented that the skin of atopic dermatitis patients demonstrates a statistically significantly higher increase in skin thickness (by ultrasound) in response to exposure to sodium !auryl sulfate, as compared to controls [125]. Whether this is due to the abnormalities in epidermal lipid metabolism, in particular elevated free arachidonic acid, of patients with atopic dermatitis [126] or abnormally low levels of ceramides in the stratum corneum of atopic dermatitis patients [127] or to defective conversion of linoleic acid [128] remains to be determined. Other contributory factors include various microbes and psychic stress. Under rare circumstance, triggers can include dietary foods, aeroallergens [129], and ultraviolet [130]. Contact urticaria to raw foods [131], or contact allergens, i.e., dermatitis, but mainly extrinsic contact irritant dermatitis is responsible for the high incidence of hand dermatitis. Several studies have documented that 80-85% of patients with occupational hand epidermis had coexisting atopy [132,133], a
THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
finding likely related to the high prevalence of atopy in the general population.
House Dust Mites There seems to be no question that patients with atopic dermatitis have a high frequency of IgE antibodies that detect house dust mite antigens and that the skin and blood of at least some patients also harbor T cells that can recognize house dust mite antigens when presented by appropriate antigen-presenting cells (recently reviewed in [84]). These findings generally occur in patients who demonstrate a positive epicutaneous "patch" test to dust mite antigens. Because dust Inites are ubiquitous, it is attractive to postulate that either aeroallergens or epicutaneous exposure can initiate immunologic events that exacerbate the dermatitis. In fact, there is a positive correlation between the magnitude of exposure to dust mites and the frequency of disease [134]. However, although dust mites are known to have a more favorable growth rate under damp conditions than dry conditions, the association was independent of the presence of domestic humidity. Thus, these authors hypothesize that the association between high densities of mites and atopic dermatitis may be related to differences in lipid composition of the shed squames on which the mites feed, or perhaps on the amount of squame available [134] .
A cornerstone of the work implicating dust mite antigens as a trigger in atopic dermatitis has been the development of an epicutaneous patch test to detect a subset of patients with atopic dermatitis that have such reactivity. In many instances investigators use tape stripped or somewhat abraded skin to obtain positive reactions. The lack of standardized preparations and methods of application is the likely cause of variations in the literature with regard to the frequency of atopic dermatitis patients with positive tests. In one recent study, the authors varied both the type of allergen and the state of the skin being patch tested; they found positive patch tests in 40 - 50% of atopic dermatitis patients and favored a simple application on healthy appearing skin [135]. In another comparative study, non-specific reactions due to tape stripping, fixation tape, or patchtest occlusion were observed in up to 80%, with specific reactions occurring in only 30% of atopic dermatitis patients. Almost all of these reactions occurred in patients with extremely high serum IgEs [136]. Careful use of this test is therefore required. However, the immunoreactivity that occurs after initiation of such a test has revealed significant useful information. Presentation of house dust antigen via specific IgE bound to Langerhans cells has been demonstrated, as described above [55], and an antibody to house dust mite antigen has even been used to visualize the antigen in positive patch tests by immunoelectron microscopy in epidermal and dermal Langerhans cells [137].
In addition to dust mites, other airborne allergens, such as tree and grass pollens, have been used in occlusive chamber-scarification patch tests to elicit contact sensitivity -like delayed-in-time responses in patients with atopic dermatitis. Although such special testing may be able to elicit atopic dermatitis -like cutaneous inflammation under these controlled circumstances, it still is extremely unusual for allergen desensitization to provide any benefit for the dermatitis of atopic dermatitis. Another ubiquitous antigen, which has been found to elicit reactions in patients with atopic dermatitis under chamber-scarification patch tests is PityrosponlPl/ ova Ie. Large molecular weight antigenic substances from P. ollale (greater than 60 kD) have been found to induce lymphocyte proliferation in atopic dermatitis patients with positive patch test to P. ovale extracts [138]. IgE antibodies against P . ol/ale were found in two of three atopic dermatitis patients, particularly in those with lesions predominantly in the seborrheic areas, the area of highest prevalence of P. ol/ale [139] in young adults . Whether this commOn lipophilic yeast is truly pathogenic, or whether these findings merely reflect the propensity of atopic dermatitis patients to develop IgE-dominated responses to microbial and aeroallergens is currently unclear.
The mechanism by which Staphylococcus aureus can trigger atopic dermatitis flares might be one of several things. Staphylococcal cell

VOL. 102, NO.1 JANUARY 1994
wall products (teichoic acid and peptidoglycan), as well as a staphylococcal secreted superantigen, entero-toxin B, can stimulate peripheral blood lymphocytes , and, particularly in combination with IL-4, can lead to a pronounced increase in IgE synthesis and FeIgE receptor expression [140]. Staphylococcal superantigens also have the capacity to activate large classes of T cells, regardless of their antigen specificity, because they are able to bridge the linkage between the class II major histocompatibility complex molecule on the antigen-presenting cell and the T-cell receptor without having to be processed and presented by the antigen-presenting cell. In this scenario, staphylococcal superantigens released into the epidermis would find a way onto class II major histocompatibility complexpositive Langerhans cells or dermal DR + cells, and could thereby cause a marked stimulation of several classes of T cells that have been non-specifically recruited into the lesion. This hypothesis is consistent with our findings that Langerhans cells exclusively carry the autostimulatory signal for autologous T lymphocytes in atopic dermatitis [38]. However, this cannot be the entire source of stimulation, because a significant component of the T-cell response to self antigen-presenting cells can be removed by removing autoreactive T cells that respond to blood antigen-presenting ' cells [43] .
Foods In a highly selected group of patients, patients with food allergies and atopic dermatitis who follow an appropriate avoidance diet can have substantial clinical improvement [141] and lose their food hypersensitivities [142]. In certain patients in whom a careful history clearly implicates certain foods, ingestion of a food allergen during challenge can lead to a pruritic, morbilliform rash, which can become eczematous after a series of positive challenges over the course of several days [143]. How large food proteins in the diet could induce reactivity in the skin is not clear, but it has been postulated that increased intestinal permeability allows penetration of certain of these antigens such that the food antigens could be processed by antigen-presenting cells similarly to the in vitro model in which food antigens can stimulate atopic dermatitis peripheral blood mononuclear cells to produce high levels ofIL-2 [144]. Exposure of carefully identified patients to the offending foods causes their peripheral blood basophils to spontaneously release histamine, which in turn appears dependent upon elevated production of a histamine-releasing factor from mononuclear cells [28]. Interestingly, avoidance of the specific food can result in decreased levels of blood histamine-releasing factor and actual histamine release from atopic dermatitis basophils [28]. More generalized food-avoidance diets do not have a good response/risk ratio; an elemental diet has been tried in children with widespread atopic dermatitis and, although some clinical benefit was obtainable, the patients required prolonged hospitalization and experienced a fall in body weight and serum albumin, and, in addition, experienced a significant risk of anaphylactic shock in over 10% of the cases [145]. Highly restricted (few foods) diets are extremely arduous, although beneficial for some children, but the long-term outcome does not appear to be affected by compliance or non-compliance for such a diet [146] . A large follow-up cohort of 736 patients was recently evaluated at 7, 11 , and 14 years of age to determine the effect of cow's milk. Children with an atopic family history ran the same risk of subsequent atopic disease whether they were fed formula or breast milk alone, as compared to cow's milk [147].
Neurocutaneous Alterations As reagents for detecting and measuring neuropeptides have become available, it is becoming possible to visualize and quantitate these neuropeptides and the nerves that carry them. A number of abnormalities in atopic dermatitis are already becoming apparent. For instance, somatostatin-immunoreactive nerves, easily visualized in normal skin, were not found in the skin of patients with atopic dermatitis [148]. By contrast, neuropeptide Y - positive dendritic cells in the epidermis are present in lesional atopic dermatitis skin, but not in controls [148]. Also in atopic dermatitis there was an increase in nerve fibers revealed by anti-neura l filament antibody and anti-neuron specific protein 9.5 antibody, but a reduction in adrenergic-innervated fibers
ATOPIC DERMATITIS 133
(neuropeptide Y and tyrosine hydroxylase). Markers of sensory nerve fibers (calcitonin gene-related peptide and substance P) also showed a somewhat increased density of fibers [149].
The total skin content of neuropeptides is beginning to be explored. Two groups have found elevated vasoactive intestinal polypeptide (VIP) in lesional skin of atopic dermatitis [150,151], and in one study this was associated also with a reduction in the level of substance P [152]' Because VIP and substance P are somewhat in dynamic opposition with regard to their immunomodulatory effects, an imbalance of VIP over substance P may participate in the impaired immunologic responses of atopic dermatitis skin. In contrast to substance P, which is stimulatory for lymphocyte proliferation and monocyte cytokine production, VIP is inhibitory to lymphocyte proliferation and natural killer cell activity [152] . It is tempting to speculate that the observed imbalances in the neurocutaneous innervation in atopic dermatitis are related to abnormal vasoactive cutaneous responses in atopic dermatitis [153,154] and the increased itch responses that patients with atopic dermatitis exhibit for agents such as wool fibers [155] , and even a TH1/TH2 imbalance [156].
THERAPY
Objective Assessment of Atopic Dermatitis A critical advance in the study of atopic dermatitis occurred upon the adoption of standardized diagnostic criteria. A similar effort is now needed to standardize the quantitative clinical assessment tools avai lable for assessing whether atopic dermatitis patients improve with a specific therapy. Many clinical trials a.re riddled with subjectivity, because quantitative assessments of severity and pruritis almost invariably allow subjective patient perceptions to influence the physician's assessments, whether intended or unintended. In addition, the margins of atopic dermatitis lesions are not distinct, like those of psoriasis, so that an accurate quantitation possibly of total body surface involvement is very difficult , because patients have spongiosis even in apparently uninvolved skin and exhibit variable degrees of xerosis blending into frank scaling, which is also modified by the number of hours since bathing or moisturizing. The problem is further compounded by the extremely high placebo response in studies of patients with atopic dermatitis, which can mask the detection of a partially effective therapy, or falsely give the impression that an ineffective approach has a response rate. There is also a problem of "subsets," that is, there appear to be therapies in which a percentage of atopic dermatitis patients receive a great deal of benefit, whereas others experience little benefit.
A workshop on the subject outlined quantifiable signs and symptoms, issues regarding target site selection, and recommendations for systemic and topical steroid washout periods [157J. Other authors have recommended weighting the extent of disease by the distribution of severe and mild changes, either as a modification of the psoriasis a.rea and severity index [158], or using a simplified and rapid point-counting technique [159] . Methods involving portable data loggers for the continuous recording of itch [155] have been developed, and actigraphic watches are avai lable to monitor scratching. Ultrasound has been used to quantitate the degree of skin edema. Others have argued that simple, rapid assessments are as accurate as elaborate grading methods [160]. For the purpose of determining whether equally severe patients are entered into both the placebo and active therapy arm of a trial, a system for estimating the lifelong severity of a patient's AD has been proposed [161 J.
Recent Advances in Therapy
UV: Although PUVA [162] and UVB alone provide a response rate, studies have revealed that addition of UV A to the UVB (UV AB) provided a detectably improved therapeutic response [163,164]. Interestingly, UVB is also effective at reducing Staph aureus colonization. Subsequent studies have demonstrated the superiority of short-wave UVA (UVAII) [165J and, in particular, long-wave UV A (UVAI) [1 66] over UVB. The ability oflong-wave UVA (UVAI) to selectively reduce and transiently inactivate Lan-

134 COOPER
gerhans cells without inducing infiltration of inflammatory macrophages into the skin [167,168] may be a factor in the improved performance of UVAI over UVB in AD.
Cyclosporil1 A: Systemic immunosuppression with corticosteroids is clearly effective in atopic dermatitis, but oral or parenteral corticosteroids should be limited to brief courses of therapy in extremely severe situations, due to the significant long-term toxicity and dependency associated with steroid use in atopic dermatitis. However, other forms of systemic immunosuppression are being developed for atopic dermatitis. Oral cyclosporin A, at a dose of 5 mg/kg/d, was highly effective in reducing disease extent and severity scores, and in improving itch and sleep scores in a double-blind crossover study of atopic dermatitis [158] . Although patients experienced nausea, abdominal discomfort, and paresthesias, and elevations of bilirubin and worsening of renal function were reported, the adverse effects were considered more tolerable than placebo [158], indicating high patient acceptance, despite the use of a maximal dose level. This study validates earlier open trials and case reports of the effectiveness of oral cyclosporin A for atopic dermatitis [169-171]. By contrast, topical cyclosporin A application does not appear to be particularly effective for atopic dermatitis [172,173]. Despite the efficacy of cyclosporin A in atopic dermatitis, such therapy does not appear to reduce either intracutaneous skin tests or patch tests to dust mite antigens [170), reducing the likelihood that cyclosporin A is acting primarily to stabilize mast cells, and consistent with the potent ability of cyclosporin A to block Langerhans cell antigenpresenting activity and T-cell activation in the skin [174]. Indeed, cyclosporin A therapy of atopic dermatitis patients results in a potent inhibition of the hyperstimulatory Langerhans cells present in lesional atopic dermatitis skin [175], and in a reduction of activated T cells, Langerhans cells bearing IgE, and macrophages [18].
1I1te1eroll Gamma: In addition to the application of immunosuppressant agents to atopic dermatitis, several agents have been recently utilized that·have an immunomodulatory effect, rather than strictly suppressive capacity. Recombinant interferon gamma has been administered to patients with atopic dermatitis in a doubleblind, placebo-controlled trial of atopic dermatitis, and found to be statistically significantly superior to placebo [87] . We found clinical benefit to be accompanied by a reduction in eosinophil count, although no reduction in serum IgE was noted [87]. Eosinophils were not the only blood element to be reduced, however; reductions in the overall white blood cell count, in particular those with clinical benefit, were also observed [93]. These findings confirm a phase I open erial, which also suggested that atopic dermatitis patients benefitted from IFNy therapy [176] . Although it was originally hypothesized that IFNy would be of benefit for atopic dermatitis via its ability to down regulate Th2 responses, there was no reduction in spontaneous IgE production [176].
Thymoperltil1 : In a similar recently reported double-blind clinical trial, thymopentin, the active pentapeptide of a thymic hormone with immunostimulatory potential, gave significantly better clinical improvement than placebo in severity and pruritus at 6 weeks of treatment [177]. A smaller trial of thymopentin had also demonstrated a beneficial effect of the agent, in contrast to placebo [178]. Like IFNy, the agent was well tolerated, despite that subcutaneous injections are required (because both these agents are proteins and therefore cannot be administered orally). In the IFNy trial, patients self-administered the medication, and the concept was well accepted by the patients, including children.
Mixtures of Chi"ese Herbal Extracts: Two recent controlled trials of traditional Chinese herbal mixtures were performed, one in children and one in adults. Highly significant reductions in erythema and surface changes were found in the experimental group in the adult study [179]. Children also seemed to benefit, but the unpalatability of the concoction limited its applicability [180]. However, over 1 00 active compounds are present in these mixtures, and administration, which is often via enema, can be associated with hepatoxicity. Whether potent immunosuppressive, anti-inflammatory,
THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
antibiotic, or sedative activities of these plants are responsible is currently under active investigation.
Dieta ry Lipids: Dietary modifications involving supplementation with n-3 fatty acids (including eicosapentanoic acid) slightly favored the experimental group over the control group [179]. However, ingestion of oil of evening primrose extract (which contains the deficient linoleic and gamma-linoleic acids), demonstrated no difference from a control group taking olive oil, or from a group ingesting a combination of primrose oil and fish oil (eicosapentanoic acid) (181,182]' Although studies have been performed that exhibited a beneficial effect of primrose oil on atopic dermatitis [183], a lack of effect of primrose oil was also found by others [181,182] .
House Dust Mites: Hyposensitization with dust mite allergen was unsuccessful in improving atopic dermatitis [184]. Attempts to reduce mite levels in the home and to obtain clinical benefit with this approach have been elusive [185 ,186]' including the use of natamycin, which kills the aspergillus on which mites feed. Vacuum cleaning, neither alone or in combination with natamyacin, were able to reduce mite numbers sufficiently to provide clinical benefit [186]' Patients were able to obtain benefit from mite reduction only in a hospital setting in which a room was specially treated to reduce mite density to less than three mites per meter squared. In this study, night-time admission to the mite free room gave 11 of 13 atopic dermatitis patients relief from itching and dermatitis within 2 - 3 weeks.
Mast Cells/Phosphodiesterase: From a mast-cell- stabilizing point of view, reports of activity of ketotifin in atopic dermatitis continue to appear, and even topical cromolyn applied to lesions of young children improved the dermatitis [188]. Phosphodiesterase inhibition would also be expected to provide some mast cell stabilization, but papaverine (which has limited phosphodiesterase activity) was found to be ineffective [189,190]. However, the development of phosphodiesterase inhibitors specific for the cAMP phosphodiesterase elevated in atopic dermatitis monocytes continues to be a valid option, and candidates with promising in vitro activity have been identified (105].
CONCLUSION
The activity of investigators in studying patients with atopic dermatitis in part reflects an optimism that newer concepts in immunobiology can be utilized to better understand atopic dermatitis pathomechanisms. This enthusiasm, combined with the rapid development of new classes of immunosuppressives, immunomodulators, and light sources, makes it likely that significant strides will be made in the coming decades in the understanding and treatment of atopic dermatitis.
REFERENCES
1. Cooper KD: Mechanisms of atopic dermatitis. In: Norris DA (ed.). Itm"''''e M edlan;sms in C"tan"""s Disease. Marcel Dekker, Inc., New York, 1989, Pp 247-276
2. Hanifin JM, Cooper KD, Roth HL: Atopy and atopic dermatitis. ] Am Acad Dermato/15:703-706,1986
3. Leung DYM, Rhodes AR, Geha RS: Atopic Dermatitis. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg 1M, Austen KF (cds.). Dermatology in Gweral Medicine. McGraw-Hill Book Company, New York, 1987, pp 1385 - 1408
4. Sampson HA: Pathogenesis of eczema. Clin Exp Allergy 20:459 - 467, 1990 5. Larsen FS, Holm NV, Henningsen K: Atopic dermatitis. A genetic-epidemio.
logic study in a population-based twin sample.] Am Acad Dermato/15:487 _ 494,1986
6. Saarinen UM: Transfer of latent atopy by bone marrow transplantation? A case report.] Allergy Clin l",mlll/0174:196-200, 1984
7. Agosti JM, Sprenger JD, Lum LG, et al: Transfer of allergen-specific IgE-mediated hypersensitivity with allogeneic bone marrow transplantation. N Engl] Med 319:1623-1628, 1988
8. Saurat J-H: Eczema in primary immune deficiencies. Clues to the pathogenesis of atopic dermatitis with special reference to the Wiskott Aldrich syndrome. Dermato Venereol (sIIppl) 114:125- 128, 1985
9. Cookson WO, Sharp PA, FauxJA, HopkinJM: Linkage between immunoglobulin E responses underlying asthma and rhinitis and chromosome llq. Lanett 1:1292-1295,1989
to .. Blumenthal M, Marcus-Bagley D, Awdeh Z,Johnson B, Yunis EJ, Alper CA:

VOL. 102, NO. 1 lANUARY 1994
HLA-DR2, [HLA-B7, SC31, DR2], and [HLA-B8, SCOl, DR3] haplotypes dist.inguish subjects with asthma from those with rhinitis only in ra gweed pollen allergy. J 1,,"',,1110/148:411 -4 16, 1992
11. Elliott ST, Hanifin 1M: Delayed cutaneous hypersensitivity and lymphocyte transformation: dissociation in atopic dermatitis. Arch DerlllaloI115:36-39, 1979
12. Rees 1, Friedmann PS, Matthews lNS: Contact sensitivity to dinitrochlorobenzene is impai red in atopic subjects. Arch DwnaroI126:1173- 1175, 1990
13. Uehara M, Sawai T: A longitudinal study of con tact sensitivity in patients with atopic dermatitis. Arch DerlllatoI1 25:366-368, 1989
14. de Groot AC: Thtffrequency of contact allergy in atopic patients with dermatitis. COlllact Derlllalilis 22:273 - 277, 1990
15. Lammintausta K, Kalimo K, Fagerlund VL: Patch test reactions in atopic patients. COlllact Derlllalilis 26:234 - 240, 1992
16. Soter NA: Morphology of atopic eczema. A llergy 9:1 6- 19, 1989 17. Lever R, Turbin M, Sanderson A, MacKie R: Immunophenotyping of the cuta
neous infiltrating and of the mononuclear cell s in the periphera l blood in patients with atopic dermatitis.J b lVcsI Dcrlllato/ 89:4 -7, 1987
18. Vanloost T, Kozel MMA, T ank B, Troost R, Prens EP: Cyclosporine in atopic dermatitis. Modulation in the expression of immunologic markers in lcsional sk in.J Alii Acad DerlllatoI27: 922-928, 1992
19. Zachary CB, Poulter LW, MacDonald OM: Cell-mediated immune responses in atopic dermatitis: the relevance of antigen-presenting cells. Br J Dermatol 113(suppI28}:10 - 16,1 985
20. Bos 10, Hagenaa rs C, Das PK, Krieg SR, Voorn Wl, Kapsenberg ML: Predominance of "memory" T cells (C D4+, CDw29+) over "naive" T cells (CD4 +, CD45R +) in both normal and diseased human skin. A rch Derlllalol Rcs 281:24-30,1989
21. Berg EL, Yoshino T, Rott LS, Robinson MK, W arnock RA, Kishimoto TK,. Picker Ll, Butcher EC: T he cutaneous lymphocyte antigen is a skin lymphocyte homing receptor for the vascular lectin endothelial cell-leukocyte adhesion molecule 1.J Exp Med 174: 1461-1466, 1991
22. Leung DYM, Cotran RS , Pober jS: Expression of an endothelial leukocyte adhesion molecule (ELAM-l) in atopic dermati tis (AD) and elicited late phase allergic skin reactions (LPR) (abstr) . Clill Rcs 38:448A, 1990
23. Grilliths CEM, Voorhees lJ, Nickol off Bl: C haracterization of intercellular adhesion molecule- l and HLA-DR expression in normal and inflamed skin: modulation by recombinant gamma interferon and tumor necrosis factor. J A lii Arad Derlllalo/20:617 -629, 1989
24. Klein LM, Lavker RM, Matis WL, Murphy GF: Degranulation of human mast cells induces an endothelial antigen central to leukocyte ad hesion. Proc Nat! Acad Sci USA 86:8972 - 8976, 1989
25. W alsh Ll, Trinchieri G, W aldorf HA, el al: Human dermal mast cell s contain and release tumor necrosis factor alpha, which induces endothelial leukocyte adhesion molecule 1. Proc NaIl Acad Sci USA 88:4220-4224,1991
26. Groves RW, Ross E, Barker JNWN, Ross lS, Camp RDR, MacDonald OM: Effect of in vivo intcrleukin-l on adhesion molecule expression in normal human skin. J IrIVesl Dermatol 98:384 - 387, 1992
27. Thornhill MH, Haskard DO: IL-4 regulates endothelial cell activation by IL- l , tumor necrosis factor, or IFN-gamma. J [,,11/,,11101145:865-872, 1990
28. Sampson HA, Broadbent KR, Bernhisel-Broadbent J: Spontaneous release of histamine from basophils and histamine-releasing factor in patients with atopic dermatitis and food hypersensitivity [sec comments]. N Ellgi J Med 321:228-232,1989
29. Singer KH, Tuck DT, Sampson HA, Hall RP: Epidermal keratinocytes express the adhesion molecule intercellular ad hesion molecule-I in inflammatory dermatoses.J IlIveSI DerlllatoI92:746-750, 1989
30. Bieber T, Dannenberg B, Ring j , Braun-Falco 0: Keratinocytes inlesional skin of atopic eczema bear HLA-DR, COl a and IgE molecules. Clill Exp Derlllalol 14:35-39, 1989
31. Barker lN , Markey AC, Allen MH, el al: Keratinocyte expression of OKM5 antigen in inflammatory cutaneous disease. BrJ DermaloI120:6 13-618, 1989
32. Rasanen L, Reunala T : Langerhans cell antigen presentation and interleukin-I production in atopic dermatitis. Acta Derm Vellereol Suppl (Slockh) 144:64 - 66, 1989
33. Sticherling M, Bornscheuer E, Schroder J-M, Christophers E: Localization of neutrophil-activating peptide-l / interleukin-8-immunoreactivity in normal and psoriatic skin.J bIVcsl DermaloI 96:26 -30, 1991
34. Vonderheid E: Diagnostic methods for cutaneous T-cell lymphoma. In: Muller SA (cd.). Parapsoriasis. Mayo Foundation , Rochester, 1989, pp 83-94
35. Verga M, Braverman 1M: The usc of immunohistologic analysis in differentiating cutaneous T -cell lymphoma from psoriasis and dermatitis. Arch Derlllalol 127:1503- 1510, 1991
36. Lange-Vejlsgaard G, Ralfkiaer E, Larsen JK, O'Connor N, Thomsen K: Fatal cutaneous T cel l lymphoma in a child with atopic dermatitis. J Am Acad Derlllato/20: 954 - 958, 1989
37. BosJD, van Garderen 10, Krieg SR, Poulter LW : Different in situ distribution patterns of dendritic cells having Langerhans (T6 + ) and interdigitating (RFDI +) cell immunophenotype in psoriasis, atopic dermatitis and other inflammatory dermatoses. J IrIVcsl Dermalol 87:358 - 361, 1986
38. Taylor RS, Baadsgaard 0, Hammerberg C, Cooper KD: Hyperstimulatory COla + CDlb+ CD36+ Langerhanscells arc responsible for increased autologous T lymphocyte reactiviry to lesional epidermal cells of patients with atopic dermatitis.J bll""IIIoI147 :3794-3802, 1991
39. Cooper KD, Meunier L, Ho V, Baadsgaard 0, Lee M-S,' Hansen E, Lisby S, Mehrega n 0 , Allen E, Vejlsgaard GL, Elder JT: Activation of reactive versus malignant T cells in cutaneous T cell lymphoma: role of abnormal antigen
ATOPIC DERMATITIS 135
presenting ce lls and T cell activating molecul es. In: van Vloten W A, Lambert WC (cds.). NA TO ASI Serics Vo lllllle: Basic Mechallisms of Physi%gical alld A berram Lymphoproliferalioll ill Ihe Skill . Plenum Publishing Corporation, New York, 1992
40. Cooper KD, Gonzales-Ramos A, Meunier L, Taylor RS, Lee MS, Hammerberg C: D istinction of dermal Langerhans cells from dcrmalmacrophages by triple color flow cytometric analysis of COla, CD l c, CO ll e, CD llb, FcigGRII and HLA-DR (abstr}.J IrIVCSI DermaloI98:596, 1992
41. Cooper KD: Pathogenesis and pharmacology of atopic dermatitis. In : CzernielewskiJM (cd.). b/Hllllllological alld Pharlllacological Aspect.< oj Alopic alld ComaN Eczema. Pharmacol Skill. K.1rger, Basel, 1991, pp 11 9 - 127
42. Cooper KD, Neises GR, Katz SI: Antigen-presenting OKM5+ mel:mophages appear in human epidermis after ultraviolet radiation. J I,IVcsI Derlllalol 86:363-370,1986
43. Taylor RS, Hammerberg C, C hang L, Cooper KD: Mechanisms of epidermal immunoreactivity in atopic dermatitis (abstr). J IrlVcsI DermaloI94:584, 1990
44. Hauser C, Snapper CM, O hara J, Paul W E, Katz SI: T helper cells grown with hapten-modified cultured Langerhans' cells produce interleukin 4 and stimulate IgE production by B cells. EllrJ Imm'IIIoI19:245-25 1, 1989
45. Rocken M, Muller KM, Saurat J -H, Hauser C: Lectin-mediated induction of IL-4 producing CD4 + T cells. J 1,,"',,(/10/146:577 - 584, 1991
46. Mosmann TR, Cherwinski H, Bond MW , Giedlin MA, Coffman RL: Two types of murine helper T cell clone. I. Definition according to profi les of Iymphokine activities and secreted proteins.] 1111111'11101136:2348 - 2357, 1986
47. Bieber T, Braun-Falco 0: IgE-bearing Langerhans cells arc not specific to atopic eczema but arc found in infl am_matory skin diseases. ] Am A(ad D ermato! 24:658-659, 1991
48. BieberT, Dannenberg B, PrinzJC, Rieber EP, Stolz W , Braun-Falco 0: Occurrence of IgE-bearing epidermal L1ngerh ans cells in atopic eczema: a study of the time course of the lesions and with regard to th e IgE serum leve!. J III vest DermaloI 93:2 15- 219, 1989
49. Wangh B, Rieger A, W anek P, er al: The skin of atopic dermatitis patients harbors heterogenetically different IgE+ cells. In: Czernielewiski J (ed .). Proceedillgs OJI/oe 91h SYlllposillm Oil Adlla ll ccs ill Skill Pharlllacology: Immllllological alld Pharlllacological Aspecls oj A lopic m,d COlllacr Eczellla, 1991
50. Leung DYM, Schneeberger £E, Siraganian RP, Geha RS, Bhan AK: The presence ofIgE on macrophages and dendritic cells infiltrating into th e skin lesion of atopic dermatitis. Clill 1111"1111101 Immwlopalho/42:328-337, 1987
51. Sugiura H, Uehara M, Maeda T: IgE-positive epidermal LangerilallS ce lls in allergic contact dermatitis lesions provoked by DNCB in patienrs with atopic dermatitis. Arch Derlllalol Rcs 282:295-299,1990
52. W angB, Rieger A, Kilgus 0, Ochiai K, Maurer 0, Fodingcr 0, KinetJP, Stingl G: Epidermal Langerhans cells from normal human skin bind monomeric IgE via Fc epsilon RI . J Exp Med 175: 1353 - 1365, 1992
53. BieberT, de la Sa lle H, Wollenberg A, el al: Human epidermal L1ngerhans cells express the high allinity receptor for immunoglobulin E (Fc epsilon RI).] Exp Mcd 175:1285- 1290, 1992
54. Rieger A, W ang B, Kilgus 0 , Ochiai K, Mauercr 0, Fodinger 0, Kinet JP, Stingl G: Fc epsilon RI mediates IgE binding to human epidermal L1ngerhans cell s. J [II VCSI DermaroI 99:30S-32S, 1992
55. Mudde GC, Van Reijsen FC, Boland Gj, De Gast GC, Bruijnzeel PLB, Bruijnzeel-Koomen CAFM: Allergen presentation by epidermal L1ngerhans' cells from patients with atopic dermatitis is mediated by IgE. IlIIlII,lIIology 69:335-341, 1990
56. Fiorentino OF, Bond MW, Mosmann TR: Two types of mouse T helper eel !. IV. Th2 clones secrete a factor that inhibits cytokine production by Th 1 clones. J Exp Med 170:208 1 - 2095, 1989
57. HowardlG, Hale C, Liew FY: Genetically determined susceptibility to Leishmania tropica infection is expressed by hacmatopoietic donor cells in mouse radiation chimaeras. Na,,,,, 288:1 61- 162,1 980
58. Sadick MD, Heinzel FP, Holaday Bj, Pu RT, Dawkins RS, Locksley RM: Cure of murine Icishluanjasis with anti- interleukin 4 monoclonal antibody. Evidence for a T cell-dependent, interferon ga mma-independent mechanism. J ExpMed 171:115 - 127, 1990
59 . Romagnani S: Human THl and TH2 subsets: regulation of d_ifferentiatio l1 and role in protection and immunopathology. 1111 Arch Allergy 1111111,1110198:279-285,1992
60. Barral-Netto M, Barral A, Brownell CE, Skeiky YAW, Ellingsworth LR, Twardzik DR, Reed SG: Tranforming growth factor-beta in Leishmania l infection: a parasite escape mechanism. SciCllu 257:545 - 548, 1992
61. Conrad DH, Ben-Sasson SZ, Le Gros G, Finkelman FD, Paul WE: Infection with Nippostrongylus brasiliensis or injection of anti-I gO antibodies markedly enhances Fe-receptor-mediated interlcukin 4 production by non-B, nonTcclls.J Exp Med 171 :1497- 1508, 1990
62. Cherwinski HM, Schumacher JH , Brown KD, Mosmann TR: Two types of mouse helper T cell clone. III. Further differences in Iymphokine synthesis between Th 1 and Th2 clones revealed by RNA hybridization, functionally monospecific bioassay" and monoclonal antibodies. J Exp Med 166: 1229-1244, 1987
63. Fiorentino OF, Zlotnik A, Vieira p, Mosmann TR, Howard M, Moore KW, O'Garra A: lL- l0 acts on the antigen-presenting cell to inhibit cytokine production by Thl ce lls.] 1""'''1110/146:3444-345 1, 199 1
64. Fiorentino OF, Zlotnik A, Mosmann Tit, el al: IL- iO inhibits cytokine production by activated macrophages.] 1111111'11101147:3815-3822, 1991
65. Lehn M, W eiser WY, Engclhorn S, Gillis S, Remold HG: IL-4 inhibits H202 production and antilcishmanial capacity of human cultured monocytcs mcdiated by IFN-gamma. J 1""'"1110/ 143:3020 - 3024, 1989

136 COOPER
66. Maggi E, Parronchi P, Manetti R, Simonelli C, Piccinni M-P, Rugiu FS, Dc Carli M, Ricci M, Romagnani S: Reciprocal regulatory effects of IFNgamma and IL-4 on the in vitro development of human Th 1 and Th2 clones. ] 1m ,,"wol 148:2142 -2147, 1992
67. Yamamura M, Uyemura K, Deans RJ, W einberg K, Rca TH, Bloom BR, Modlin RL: Defining protective responses to pathogens: cytokine profiles in Leprosy lesions. Sciellce 254:277-279, 1991
68. Vowels BR, Cassin M, Vonderheid EC, Rook AH: Aberrant cytokine production by Sezary syndrome patients: Cytokine secretion pattern resembles murine Th2 cells. ] I'J11est DerlllaloI99:90 -94, 1992
69. Kapsenberg ML, Wierenga EA, Stiekema FEM, e/ al: Thllymphokine production profiles of nickel-specific CD4+ lymphocyte clones from nickcl contact allergic and non-allergic individuals. ] Il1 vesl DermaloI98:59-63 , 1992
70. Livden JK, Nilsen R, Bjerke JR, Matre R: In situ localization of interferons in psoriatic lesions. A rch Dermatol Res 281:392-397,1989
71. Kowalzick L, Weyer U: Psoriasis induced at the injection site of recombinant interferons. Arch Derlllalology 126:1515: 151 6, 1990
72. Nickoloff B, Barker J , Karabin G, el al: Detection of interferon-gamma (IFNgamma) but not tumor necrosis factor (TNF-alpha) mRNA in psotiatic epidermal sheets by polymerase chain reaction (PCR) (abstr.) e lill Res 38:836A, 1990
73. Jujo K, Renz H, AbeJ , Gelfand EW, Leung DY: Decreased interferon gamma and increased interleukin-4 production in atopic dermatitis promotes IgE synthesis. ] A llergy Clill 111111111110190:323 - 331, 1992
74. Reinhold U, Wehrmann W, Kukel S, Kreysel HW: Evidence that defective interfero n-gamma production in atopic dcnnatitis patients is due to intrinsic abnormalities. Clill Exp 11011111110/79:374-379,1990
75. Kim J -W, Chan SC, Henderson WR, el al: Disordered prostaglandin E2 control of cytokine production in atopic dermatitis (abstr).] I11 vesl Derlllalol98:6 1 0, 1992
76. Furue M, Ohtsuki M, Ogata F, Ishibashi Y: Responsiveness to interIeukin 4 and interleukin 2 of peripheral blood mononuclear cells in atopic dermatitis. ] Il1 vest DermatoI96:468 - 472, 1991
77. Renz H,Jujo K, Bradley KL, Domenico J, Gelfand EW, Leung DY: Enhanced IL-4 production and IL-4 receptor expression in atopic dermatitis and their modulation by interferon-gamma. ] Il1vesl DermaloI99:403-408, 1992
78. Maggi E, Biswas P, Del Prete G, el al: Accumulation ofTh-2-like helper T cells in the conjunctiva of patients w ith vernal conjunctivitis. ] ImmutJo! 146:1169-1174,1 991
79. Fischer MA, Black HS: Modification of membrane composition, eicosanoid metabolism, and immunoresponsiveness by dietary omega-3 and omega-6 fatry acid sources, tnodulators of ultraviolet-carcinogenesis. p/JO(oc},em pl,otobioi 54:381 -387, 1991
80. van der Heijden FL, Wierenga EA, BosJD, Kapsenberg ML: High frequency of IL-4 producing CD4 + allergen-specific T lymphocytes in atopic dermatitis lesional skin .] It,vest Dent,aloI 97:389 - 384 , 1991
81. Reinhold U, Goeden B, Kukcl S, Neumann U , Wehrmann W , Kreysel HW: In vitro expanded skin-infiltrating lymphocytes from atopic dermatitis lesions secrete high levels of lL-4 and low levcls of IFN-gamma. ln: Czern.ielewskiJ (cd.) . Proceedillgs oj Ihe 91h Symposi"m Oil Ad"allces ill Ski ll Pharlllacology: [lIIm,,IlO/ogical alld Pharlllacological Aspects oj Alopic alld COll lact Eczema, 1991
82. Ramb-Lindhauer C, Feldmann A, Rotte M, Neumann C: Characterization of grass poll en reactive T-cell lines derived from lesional atopic skin. A rch Dermatol Res 283:71- 76, 1991
83. Mudde GC, Van Reijsen FC, Bruijnzeel-Koomen CAFM: IgE-positive Langerhans cells and TH2 allergen-specific T cells in atopic dermatitis. ] !rlVest Derrllalo199:103S, 1992
84. Bos JD, Wierenga EA, Smitt JHS, van der Heijden FL, Kapsenberg ML: Immune dysregulation in atopic eczema. A rclr Dermalo/128:1509 - 1512, 1992
85. Sager N , Feldmann A, Schill ing G, Kreitsch P, Neumann C: House dust mitespecific T cells in the skin of subjects with atopic dermatitis: frequency and Iymphokine profile in the allergen patch test [see comments]. J Allergy Clin ImmunoI89:801 -810, 1992
86. Van Reijsen FC, Bruijnzeel-Koomen CA, Kalthoff FS, el al: Skin-derived aeroallergen-specific T-cell clones of Th2 phenotype in patients with atopic dermatiris. ] A llergy Clill 1111/11""0190:184 - 193,1992
87. Hanifi n JM, Schneider LC, Leung DYM, Ellis CN, Jaffe HS, Izu AE, Bucalo LR, Hirabayashi SE, Tofte SJ, Cantu-Gonzales G, Milgrom H , Boguniewicz M, Cooper KD: Recombinant interferon gamma therapy for atopic dermatitis.] Alii Acad DerlllaloI 28: 189-197, 1993
88. Klug H, Harnack K: The ultrastructure of interdigitating cells in atopic eczema. Zelll ra lbi A llg Pat/,o/1 35:417 - 423, 1989
89. Czech W, Krutmann J, Schopf E, Kapp A: Serum eosinophil cationic protein (ECP) is a sensitive measure for disease activity in atopic dermatitis. Br J DermatoI1 26:351-355, 1992
90. Colver GB, Symons JA, Duff GW: Soluble interIeukin 2 receptor in atopic eczema. Br Med) 298:1426- 1428, 1989
9 1. Thestrup-Pedersen K, Larsen CS, Kristensen M, Zachariae C: Interleukin-l release from peripheral blood monocytes and soluble interleukin-2 and CD8 receptors in serum from patients with atopic derma.titis. Acta Dum Ve" erco! (StocH) 70:395 - 399, 1990
92. Sowden JM, Powell RJ , Allen BR: Selective activation of circulating CD4 + lymphocytes in severe adult atopic dermatitis. Br] DentraIO/127:228 - 232, 1992
93. Blok B, Taylor RS, Gonzalez A, Simon M, King C, Solomon W , Ellis C,Jaffe H, Cooper KD: Peripheral blood leukocyte subsets in atopic dermatitis: effect of gamma interferon (abstr).] I11 vesl DerlllaloI96:604 , 1991
THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
94. Vestey JP, Howie SE, Norval M, Maingay JP , Neill WA: Severe eczema herpeticum is associated with prolonged depression of cell-mediated immunity to herpes simplex virus. Om Prob! DentraIOI1 8:158-161, 1989
95. Kapp A, K.irnbauer R, Luger TA, SchopfE: Altered production of immuno-modulatin g cytokines in patients with atopic dermatitis. Acta Derlll Vellereol S"ppl (Slocklr) 144:97 -99, 1989
96. Kapp A, Textor A, Krutmann J , Moller A: Immunomodulating cytokines in atopic dermatitis and psoriasis: production of tumour necrosis factor and lymphotoxin by mononuclear cells in vitro. Br] Demralo1122:587 - 592, 1990
97. Kapp A, Neuner P, KrutmannJ , Luger TA, SchopfE: Production of interleukin-2 by Inononuclcar cells in vitro in patients w ith atopic dermatitis and psoriasis. Comparison with serum interleukin-2 receptor levels. Acta Dent' Vellereal (Slocklr) 71:403-406, 1991
98. Chan SC, Audera C, Rocklin R, Hanifin JM: Altered cyclic nucleotide and prostaglandin regulation of T cell cytokine production in atopic dermati tis (abstr).] I11veSI Derlllalo/l00:557, 1993
99. Stevens SR, Griffiths TW, Cooper KD: CD4+ T lymphocytopenia without HIV infection (letter). N Ellgl] Med (in press)
100. Wehrmann W, Reinhold U, Kukel S, Franke N , Uerlich M, Kreysel HW: Selective alterations in natural killer cell subsets in patients with atopic dermatitis. 1111 Arclr A llergy Appl 1111111111101 92:318 - 322, 1990
101. Lesko MJ, Lever RS, Mackie RM, Parrott OM: The effect of topical steroid application on natural ki ller cell activity. Clill Exp Allergy 19:633 -636, 1989
102. Jakob T, Huspith BN, Latchman YE, el al: Depressed lymphocyte transformation and the role of prostaglandins in atopic dermatitis. Clill Exp 111111"'"01 79:380 - 384, 1990
103. Chan SC, Audera C, Rocklin R, el al: Cyclic nucleotide regulation of T cell cytokine production and feedback control in atopic dermatitis (abstr) . Clill R es 41:5A,1993
104. Phipps RP, Stein SH, Roper RL: A new view of prostaglandinE regulation of the immune [esponse. 1111111 ,//101 Today 12:349-352, 1991
105. Hanifin JM: Phosphodiesterase and immune dysfunction in atopic dermatitis. ] Dermatol Sci 1:1-6, 1990
106. Cooper KD, Kang K, Chan SC, Hanifi nJM: Phosphodiesterase inhibition by Ro 20-1724 reduces hyper-lgE synthesis by atopic dermatitis cells in vi tro.] III vest Derlllalol 84:477 - 482, 1985
107. Buckley CC, Ivison C, Poulter LW, Rustin MH: Fc epsilon Rl1 / CD23 receptor djstribution in patch test reactions to aeroallcrgcns in atopic dermatitis. J I11vest DerlllaloI99:184 - 188, 1992
108. Pogh K, Herlin T, Kragballe K: Eicosanoids in skin of patients with atopic dermatitis: prostaglandin E2 and leukotriene B4 arc present in biologically active concentrations. ] A llergy clill [mm,,,,0/ 83:450-455, 1989
109. Polla BS, Ezekowitz RA, Leung DY: Monocytes from patients with atopic dermatitis arc primed for superoxide production. ] A llergy Clill Il/1l11u llol 89:545 -551,1992
110. Li S-H, Chan SC, Toshitani A, Leung DYM, Hani fin JM: Synergistic effects of interIeukin 4 and interferon-gamma on monocyte phosphodiesterase activity. ] I11vesl Dermalol99:65 - 70, 1992
111. Holden CA, Chan SC, Han.ifin JM: Monocyte localization of clevated cAMP phosphodiesterase activity in atopic dermatitis.] 111,'esl DermaloI87:372-376, 1986
11 2. Hanifin JM, Lloyd R, Okubo K, Guerin LL, Fancher L, Chan SC: Relationsh.ip between increased cycl ic AMP-phosphodiesterase activity and abnormal adenylyl cyclase regulation in leukocytes from patients with atopic dermatitis. ] [, ,,,esl DerlllaloI98:100S-105S, 1992
11 3. Heskcl NS, Chan SC, Thiel ML, el al: Elevated umbilical cord blood leukocyte cyclic adenosine monophosphate-phosphodiesterase activity in children with atopic parents.] Am Acad Dent,alol11 :422 - 426, 1984
114. HanifinJM, Chan SC: Characterization of cAMP-phosphodiesterase as a possible laboratory marker of atopic dermatitis. Drug Develop Res 13:123 - 136, 1988
115. Butler JM, Chan SC, Stevens DR, Han.ifin JM: Increased leukocyte histamine release with elevated cyclic AMP-phosphodiesterase activity in atopic dermatitis.] A llergy Clill lrn m ,41101 71:490 - 497, 1983
116. Turner CR, Darowski MJ, Sampson HA, Spannhake EW, Hirshman CA: Dermal mast cell releasabili ty and end organ responsiveness in atopic and nonatopic dogs.] Allergy Clill l"m'"110/83:643 - 648, 1989
117. Ebertz JM, Hirshman CA, Kettelkamp NS, Uno H, Hanifin JM: Substance P - induced histamine release in human cutaneous mast cells.] Il1 vest Dermalol 88:682 -685, 1987
118. Katayama I, Yokozeki H, Nishioka K: Mast-cell-derived mediators induce epidermal cell proliferation: clue for lichenified skin les ion formation in atopic dermatitis. 1111 Arch Allergy 1111111'4110/98:410 -414, 1992
11 9. Sumimoto S, Kawai M, Kasajima Y, Hamamoto T : Increased plasma tumour necrosis factor-alpha concentration in atopic dermatitis. Arch Dis CI,i1d 67:277 -279, 1992
120. Uehara M, Izukura R, Sawai T : Blood eosinophilia in atopic dermatitis. Clill E_"p Dent,alo/15:264-266, 1990
121. Cheng J , Ott N , Peterson E, George T , Gleich GJ, Leiferman KM: Demlal eosinophils in atopic dermatitis undergo cyto lytic degeneration (abstr).] [li Vest Derlllalo1100:545 , 1993
122. Kapp A, Czech W, KrutmannJ , SchopfE: Eosinophil cationic protein in sera of patients with atopic dermatitis. ) A lii Acad Derlllato/ 24:555-558 , 199 1
123. Tsuda S, Kato K, Miyasato M, Sasai Y: Eosinophil involvement in atopic dermatitis as reflected by elevated serum levels of eosinophil cationic protein. ] Derlllalo/19:208 -213, 1992
124. Frings S, Brautigam M, Schopf RE: Blood eosinophils decrease in patients with

VOL. 102, NO.1 JANUARY 1994
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
135.
136.
137.
138.
139.
140.
141.
142.
143.
144.
145.
146.
147.
148.
149.
150.
15 1.
152.
153.
154.
155.
156.
157 .
158.
I?soriasis under cyclosporin A treatment before clinical improvement sets in (abstr) .] Ill vest Derlllatoll00:542, 1993
Agner T : Susceptibility of atopic dermatitis patients to irritant dermatitis caused by sodium lauryl sulphate. Acta Dwn Vellereol (Stockh) 71 :296-300,1 99 1
Schafer L, Kragballe K: Abnormalities in epidermal lipid metabolism in patients with atopic dermatitis.) Ill vest DerlllatoI96: 10 - 15, 1991
Imokawa G, Abe A,Jin K, Higaki Y, Kawashima M, Hidano A: Decreased level of ccram_ides in stratum corneum of atopic dermatitis: an etiologic factor in atopic dry skin?] III vest Derlllatol96:523 - 526, 1991
Wright S, Horrobin D, Manku M: Deficient conversion of linoleic acid.] A m Acad Derlllato/23:533 - 534, 1990
Clark RA, Adinoff AD: The relationship between positive aeroallergen patch test reactions and aeroallergen exacerbations of atopic dermatitis. Clill [111-
111111101 [mllltlllopathoI53:S132-S140, 1989 Keong CH, Kurumaji Y, Miyamoto C, Fukuro S, Kondo S, Nishioka K: Photo
sensitivity in atopic dermatitis: demonstration of abnormal response to UVB.] DerlllatoI1 9:342-347, 1992
H anifin JM, Rajka G: Diagnostic features of atopic dermatitis. Acta Dermatolleller (Stockh) 60(suppl92):44-47, 1980
Rystedt I: W ork-related had eczema in atopics. COlllact Derlllatitis 12:164-171, 1985
Schmunes E, Keil JE: Occupational dermatoses in South Carolina: a descriptive analysis of cost variabl es. ] A lii Acad DerlllatoI9:861-866, 1983
ColloffMJ: Exposure to house dust mites in homes of people with atopic dermatitis. Br) DerlllatoI1 27:322-327 , 1992
Seidenari S, Manzini BM, Danese P, Giannetti A: Positive patch tests to whole mite culture and purified mite extracts in patients with atopic dermatitis, asthma, and rhinitis. AIIII A llergy 69:201 - 206, 1992
va n Voorst Vader PC, Lier JG, W oest TE, Coenraads PJ, Nater JP: Patch tests with house dust mite antigens in atopic dermatitis patients: methodological problems. Acta Derm Vellereol (StocH) 71:301-305, 1991
T anaka V, Anan S, Yoshida H: Immunohistochemical studies in nlite antigcninduced patch test sites in atopic dermatitis. ] Derlllatol Sci 1 :361- 368, 1990
Rokugo M, T agami H , U suba Y, T omita Y: Contact sensitivity to Pityrosporum ovale in patients with atopic dermatitis. Arch Derlllato /126:627 -632, 1990
Kieffer M, Bergbrant 1M, Faergemann J, Jemec GB, Ottevanger V, Skov PS, Svejgaard E: Immune reactions to Pityrosporum ovale in adult patients with atopic and seborrheic dermatitis.] A m Acad Derlllatol 22:739 - 742, 1990
Neuber K, Konig W: Effects of staphylococcus aureus cell wall products (teichoic acid, peptidoglycan) and enterotoxin B on immunoglobulin (lgE, IgA, IgG) synthesis and CD23 expression in patients with atopic dermatitis. ItIllIJII
lIology 75:23 - 28, 1992 Sampson HA, McCaskill CC: Food hypersensitivity and atopic dermatitis: eval
uation of 113 patients.) Pediatr 107:669-675,1985 Sampson HA, Scanlon SM: N atural history of food hyperse nsitivity in children
with atopic dennatitis. ] Pediatr 115:23-27, 1989 Goldenhersh MA: Atopic dermatitis and food hypersensitivity. N Ellgl] Med
322:274, 1990 Agata H, Kondo N, Fukutomi 0, et 01: Interleukin-2 production oflymphocytes
in food sensitive atopic dermatitis. Arch Dis Child 67:280 -284, 1992 Devlin J, David TJ, Stanton RH: Elemental diet for refractory atopic eczema.
Arch Dis Child 66:93-99,1991 Devlin J, David TJ, Stanton RH: Six food diet for childhood atopic dermatitis.
Acta D enll Vellereol (StocH) 71 :20- 24, 1991 GlIstafsson D, Lowhagen T , Andersson K: Risk of developing atopic disease after
early feeding with cows' milk based formula . Arc!' Dis Child 67:1008 - 1010, 1992
Pincelli C, Fantini F, Massimi P, Girolomoni G, Seidenari S, Giannetti A: Ncuropcptides in skin from patients with atopic dermatitis: an itnmunohistochemical study. BrJ DerlllatoI122:745 - 750, 1990
Tobin D , N abarro G, de la Faille HB, van Vloten W A, van der Putte SC, Schuurman HJ: Incteased number of immunoreactive nerve fibers in atopic dermatitis.] Allergy clill 111111111110190:613 -622, 1992
Anand P, Springall DR, Blank MA, Sellu D , PolakJM, Bloom SR: Neuropeptides in skin disease: increased VIP in eczema and psoriasis bur not axillary hyperhidrosis. Br] Derlllato1124:547 - 549, 1991
Pincelli C, Fantini F, Romualdi P, et 01: Skin levels of vasoactive intestinal polypeptide in atopic dermatitis. Arc!' Denllatol Res 283:230 -232,1991
Fantini F, Pincelli C, Romualdi P, et al: Substance P levels arc decreased in lesional skin of atopic dermatitis. Exp Derlllato/1:1 26- 128, 1992
Giannetti A, Girolomoni G: Skin reactivity to neuropeptides in atopic dermatitis. Br] DerlllotoI121 :68 1-688, 1989
Heyer G, Hornstein OP, Handwerker HO: Skin reactions and itch sensation induced by epicutaneous histamine application in atopic dermatitis and controls.) Itlllest DerlllatoI93:492 - 496, 1989
W ahl gren CF, Hagennark 0, Bergstrom R: Patients' perception of itch induced by histamine, compound 48/80 and wool fibers in atopic dermatitis. Acta Denn Vellereol (StacH) 71 :488 -494, 199 1
Schauer E, Aebischer I, Schwarz A, Schwarz T , Krutmann J, Stadl er BM, Luger TA: Proopiomelanocortin derived pcp tides are involved ill the regulation of interferon gamma and IgE (abstr).] Itlllest Derlllotol100:574 , 1993
Hanifin JM: Standardized grading of subjects for clinical research studies in atopic dermatitis: workshop repott. Acta Deml Vellereol SlIppl (Stockll) 144:28-30,1989
SowdenJM, Berth-JonesJ, Ross JS, Motley RJ, Marks R, Finlay AY, Salek MS, Graham-Brown RAC, Allen BR, Camp RDR: Double-blind, controlled,
159.
160.
161.
162.
163. 164.
165.
166.
167.
168.
169.
170.
171.
172.
173.
174.
175.
176.
177.
178.
179.
180.
181.
182.
183.
184.
185.
186.
187.
188.
189.
190.
ATOPIC DERMATITIS 137
crossover smdy of cyclosporin in adults with severe refractory atopic dermatitis. Lallcet 338:137-140,1991
Dahmer FA, Schafer J, Schubert HJ: Quantification of the extent and the severity of atopic dermatitis: the ADASI score (letter). Arch DerlllatoI127:1239- 1240, 199 1
Costa C , Rilliet A, Nicolet M, SauratJH: Scoring atopic detmatitis: the simpler the better? Acta Derlll Vellereol (StocH) 69:41-45, 1989
Rajka G, Langeland T: Grading of the severity of atopic dennatitis. Acta Derlll Veuereol SlIppl (StocH) 144:13-14, 1989
Atherton DJ, Ca rabott F, Glover MT, et 01: The role of psora len chemotherapy (PUV A) in the treatment of severe atopic eczema in adolescence. Br] Derlllatol 118:79 1-795, 1988
Falk ES: UV -light therapies in atopic dermatitis. Photoderlllato/2:241- 246, 1985 Midelfart K, Stenvold SE, Voloden G: Combined UVB and UVA phototherapy
of atopic eczema. Derlllatologica 171:95 -98, 1985 J ekler J, Larko 0: UV A solarium versus UVB phototherapy of atopic dennatitis:
a paired-comparison study. Br) Derlllato/125:569-572, 1991 KrutmannJ, Czech W, Diepgen T , Niedner R, Kapp A, Schopf£: High-dose
UVAI therapy in the treatment of patients with atopic dermatitis.] Alii Acad Derlllato/26:225-230 , 1992
Baadsgaard 0, Lisby S, Wantzin GL, WulfHC, Cooper KD: Rapid recovery of Langerhans cell alloreactivity, without induction of autoreactivity, after in vivo ultraviolet A, but not ultraviolet B exposure of human skin.] [111111111101 142:4213-4218,1989
Baadsgaard 0, WulfHC, Wantzin GL, Cooper KD: UVB and UVC, but not UV A, potently induce the appearance ofT6-DR + antigen-presenting cells in human epidermis. ] I'lIIest Derlllatol 89: 11 3 - 118, 1987
Taylor RS, Cooper KD , HeadingtonJT, et al: Cyclosporine therapy for severe atopic dermatitis.] A lii Acad Derlllato/21:580-583, 1989
MUltro CS, Higgins EM, Marks JM, Daly BM, Friedmann PS, Shuster S: Cyclosporin A in atopic dermatitis: therapeutic response is dissociated from effects on allergic reactions. Br] Derlllato/124:43 - 48, 1991
Ross JS, Camp RD: Cyclosporin A ill atopic dermatitis. Br] Derlllatol122(suppl 36):41-45,1990
de Prost Y, Bodemer C, Teillac D: Randomised double-blind placebo-controlled trial of local cyclosporin in atopic dennatitis. Acta Derlll Vellereol (StacH) 144:136- 138,1989
Dc Rie MA, Meinard.i MM, Bos JD: Lack of efficacy of topical cyclosporin A in atopic dermatitis and . lIergic contact dem13titis. Acta Derm Veuereol (Stock h) 71:452 -454,1991
Cooper KD, Baadsgaard 0, Ellis C N, Duell E, Voorhees JJ: Mechanisms of cyclosporine A inhibirion of antigen-presenting activity in uninvolved and lesional psoriatic epidermis.] Il1vest DerlllatoI94:649 -656, 1990
Taylor RS , B.adsgaard 0, HeadingtOIlJT, Ell is CN, Voorhees JJ, Cooper KD: Epidermal activation of .utoreactive T cells in atopic dermatitis: response to cyclosporine A (abm).] blllest Derlllato190:612, 1988
Boguniewicz M, Jaffe HS, Izu A, Su llivan MJ, York D, Geha RS, Leung DY: Recombinant gaJllma interferon in treatment of patients w ith atopic dermatitis and elevated IgE levels. A lii] Med 88:365-370,1990
Leung DYM, Hirsh RL, Schneider L, Moody C, Taboka R, Li SH, Meyerson LA, Mariam SG, Goldstein G, HanifinJM: Thymopentin therapy teduces the clinical severity of atopic dennatitis.) A llergy e lill 111111111110185:927 - 933, 1990
J{."'g K, Cooper KD: Vanderbark A, Hanifi n JM: Thymopoietill pentapeptide (TP-S) Improves clullcal parameters and lymphocyte subpopulations in atopic dermatitis.] Alii Acad DerlllatoI8:372 -377, 1983
Bjotl1eboe A, Soyland £, Bjorneboe GE, et 01: Effect of n-3 fatty acid supplement to patients with atopic dermatitis. ] Illtem Med SlIpp1225:233 - 236, 1989
Sheehan MP, Atherton DJ: A controlled trial of traditional C hinese medicinal plants in widespread non-exudative atopic eczema. Br] Derlllato/126:179 -184, 1992
Guenther L, Wexler D: Efamol in the treatment of atopic dermatitis (letter). } Alii Acad Derlllatol17:860, 1987
Rasmussen JE: Advances in nondietary management of children with atopic dermatitis. Pedialr DerlllatoI6:210 -215, 1989
Wright S, Burton JL: Oral evening primose seed oil improved atopic eczema. Lallcet 11:1120-1 122, 1982
Glover MT, Atherton DJ: A double-blind con trolled trial of hyposensitization to Dennatophagoides pteronyssinlls in children with atopic eczema. Clill Exp A llergy 22:440-446, 1992
Beck HI, Bjerring P, H arving H: Atopic dermatitis and the indoor climate. The effect from preventive measures. Acta D erlll Vellereol (Stocklt) 69:162- 165, 1989
ColloffMJ, Lever RS, McSharry C: A controlled trial of house dust Illite eradication using natamycin in homes of patients with atopic dermatitis: effect on clinical status and mite populations. Br] Derlllatol121: 199 - 208, 1989
Fukuda H , Imayama S. Okada K: The mite-free room (MFR) for th e management of atopic dermatitis: living in the MFR improved first the itch and then the detl11atitis. A rerugi 40:626-632, 199 1
Kimata H , Igarashi M: Topical cromolyn (disodium cromoglycate) solution in the treatment of young children with atopic dermatitis [sec comments). Clill Exp A llergy 20:281-283, 1990
Berth-Jones J, Graham-Brown RA: Failure of papaverine to reduce pruritus in atopic dermatitis: a double-blind, placebo-controlled cross-over study. Br J Derlllato/1 22:553-557, 1990
Shupack J , Stiller M, Meola T Jr, Orbuch P: Papaverine hydrochloride in the treatment of atopic dermatitis: a double-blind, placebo-controlled crossover c1injcal trial to reassess safety and efficacy. Derlllatologica 183:21 -24, 199 1