Embed Size (px)
Citation preview

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 122
Designing Framework for Data Warehousing of Patient
Clinical Records using Data Visualization Technique of
Nigeria Medical Records
Dr. Oye, N. D.
Department of Computer Science,
Modibbo Adama University of Technology,
Yola, Adamawa state, Nigeria
Emeje, G.D
Department of Computer Science
Modibbo Adama University of Technology,
Yola, Adamawa state, Nigeria
Abstract:
The availability of timely and accurate data is vital to make informed medical decisions. Today patients data required to make informed medical
decisions are trapped within fragmented and disparate clinical and administrative systems that are not properly integrated or fully utilized. Therefore,
there is a growing need in the healthcare sector to store and organize size-able clinical record of patients to assist the healthcare professionals in
decision making processes. This research is about integrating and organizing disparate clinical record of patients into a Data Warehouse (DW) for data
analysis and mining, which will enable evidence-based decision-making processes. This study uses SQL Server Integration Service (SSIS) for the
extraction transformation and loading (ETL) of patient clinical records from fragmented administrative systems into the DW, Data visualization
technique was used for data presentation while SQL Server Reporting Services and Business Intelligent (BI) tools for designing the output results. This
research will assist medical experts and decision makers in the healthcare industry in planning for the future. This research also provides an architecture
for designing a clinical DW that is not limited to single disease and will operate as a distributed system, Periodic update on a daily basis is possible
because contemporary technologies have narrowed the gap between updates which enable organizations to have a “real time” DW which can be
analyzed using an OLAP Server. In conclusion if this research is deployed it will aid medical decision-making process in the Nigerian medical sector.
Keywords: Clinical records; Data marts; Data Warehousing; Framework; Patient record
1. INTRODUCTION
1.1 Background of the study Knowledgeable decision making in healthcare is vital to
provide timely, precise, and appropriate advice to the right
patient, to reduce the cost of healthcare and to improve the
overall quality of healthcare services. Since medical decisions
are very complex, making choices about medical decision-
making processes, procedures and treatments can be
overwhelming. (Demetriades, Kolodner, & Christopherson,
2005). One of the major challenges of Information
Technology (IT) in Healthcare services is how to integrate
several disparate, standalone clinical information repositories
into a single logical repository to create a distinct version of
fact for all users (Mann, 2005; Zheng et al., 2008; Goldstein et
al., 2007; Shepherd, 2007).
A massive amount of health records, related documents and
medical images generated by clinical diagnostic equipment
are created daily (Zheng, Jin, Zhang, Liu, & Chu, 2008).
Medical records are owned by different hospitals,
departments, doctors, technicians, nurses, and patients. These
valuable data are stored in various medical information
systems such as HIS (Hospital Information System), RIS
(Radiology Information System), PACS (Picture Archiving
and Communications System) in various hospitals,
departments and laboratories being primary locations (Zheng,
Jin, Zhang, Liu, & Chu, 2008). These medical information
systems are distributed and heterogeneous (utilizing various
software and hardware platforms including several
configurations). Such processes and data flows have been
reported by Zheng, Jin, Zhang, Liu, & Chu (2008).All medical
records are located in different hospitals or different
departments of single hospital. Every unit may use different
hardware platforms, different operating systems, different
information management systems, or different network
protocols. Medical data is also in various formats. There are
not only a tremendous volume of imaging files (unstructured
data), but also many medical information such as medical
records, diagnosis reports and cases with different definitions
and structures in information system (structured data), Zheng
et al., (2008).
This causes Clinical Data Stores (CDS) with isolated
information across various hospitals, departments,
laboratories and related administrative processes, which are
time consuming and demanding reliable integration (Sahama,
& Croll, 2007). Data required to make informed medical
decisions are trapped within fragmented, disparate, and
heterogeneous clinical and administrative systems that are not
properly integrated or fully utilized. Ultimately, healthcare
begins to suffer because medical practitioners and healthcare
providers are unable to access and use this information to
perform activities such as diagnostics, prognostics and
treatment optimization to improve patient care (Saliya, 2013).
1.2 Problem Statement
The availability of timely and accurate data is vital to make
informed medical decisions. Every type of healthcare
organization faces a common problem with the considerable
amount of data they have in several systems. Such systems are
unstructured and unorganized, demanding computational time
for data and information integration (Saliya, 2013). Today

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 123
Patient’s data required to make informed medical decisions
are trapped within fragmented and disparate clinical and
administrative systems that are not properly integrated or fully
utilized. The process of synthesizing information from these
multiple heterogeneous data sources is extremely difficult,
time consuming and in some cases impossible. Due to the fast
growing data in the healthcare sector there is need for health
industries to be open towards adoption of extensive healthcare
decision support systems, (Abubakar, Ahmed, Saifullahi,
Bello, Abdulra’uf, Sharifai and Abubakar, 2014). There is a
growing need in the healthcare scenario to store and organize
sizeable clinical data, analyze the data, assist the healthcare
professionals in decision making, and develop data mining
methodologies to mine hidden patterns and discover new
knowledge (Ramani, 2012). Data warehousing integrates
fragmented electronic health records from independent and
heterogeneous clinical data stores (Saliya, 2013) into a single
repository. It is based on these concepts that this study plan to
design a Data Warehousing and Mining Framework that will
organize, extract, and integrate medical records of patients.
1.3 Aim and Objectives of the Study The aim of this study is to design a Data Warehousing and
Mining Framework for clinical records of patients and the
objectives of the study are to:
i. Design a database for the Data Warehouse (DW) Prototype
Model using Dimensional Modeling and Techniques.
ii. Simulate the data warehouse database in order to generate
reports, uncover hidden patterns, and knowledge from the DW
to aid decision making, using the SQL Server 2014, Business
Intelligence (BI) Tools and Microsoft Reporting Services.
iii. Develop a web platform that will integrate the front-end,
middle-end and the back-end using visual studio 2015 as the
development platform. ASP.NET, bootstrap Cascading Style
Sheet (CSS), HTML5 and JavaScript will be used for the
frond end, C# as the middle end programming language and
Microsoft SQL Server Management Studio for the back end
development.
1.4 Significance of the Study
It is clear that advanced clinical data warehousing and mining
information systems will be a driver for quality improvements
of medical care. This ability to integrate data to have valuable
information will result in a competitive advantage, enabling
healthcare organizations to operate more efficiently. The
discovered knowledge in the Human Leaning technique can
be used for community diagnoses or prognosis. It will
eliminate the use of file system and physical conveyance of
files by messengers. It will provide a platform for data mining
operations on patient’s clinical data. This research will
encourage and challenge many government and non-
governmental healthcare providers to opt for data warehouse
and mining investment in order to improve information access
within their organization, bringing the user of their
information system in touch with their data, and providing
cross-function integration of operation systems within the
organizations.
1.5 Definition of Terms
In this section, we have operationally defined some technical
terms that were used in this research.
i. Decision Support System: This refers to the system that uses
data (internal and external) and models, to provide a simple
and easy to use interface, hence, allowing the decision maker
to have control over the decision process.
ii. Prototype: Refers to the replica of the complete system
(“DW prototype framework”) working as if it were real.
iii. Architecture: Is the process that focuses on the formation
of data stores within a DW system, along with the procedure
of how the data flows from the source systems to the
application use by the end users.
iv. Heterogeneous: consisting of or composed of dissimilar
elements or ingredients.
v. Data Mining: The process of sorting through large data sets
to identify patterns and establish relationships to solve
problems through data analysis.
vi. Data Visualization: Technique used in presenting results
obtained in a graphical view for easier understanding and
comprehension.
1.5.1 Data warehouse definition
Inuwa and Garba (2015) define data warehouse as a subject-
oriented, integrated, non-volatile, and time-variant collection
of data in support of management’s decisions.
Subject-oriented: Classical operations systems are organized
around the applications of the company. Each type of
company has its own unique set of subjects.
Integrated: Data is fed from multiple disparate sources into
the data warehouse. As the data is fed it is converted,
reformatted, re-sequenced, summarized, and so forth. The
result is that data once it resides in the data warehouse has a
single physical corporate image.
Non-volatile: Data warehouse data is loaded and accessed,
but it is not updated. Instead, when data in the data warehouse
is loaded, it is loaded in a snapshot, static format. When
subsequent changes occur, a new snapshot record is written.
In doing so a history of data is kept in the data warehouse.
Time-variant: Every unit of data in the data warehouse is
accurate at given moment in time. In some cases, a record is
time stamped. In other cases, a record has a date of
transaction. But in every case, there is some form of time
marking to show the moment in time during which the record
is accurate.’
According to Kimball and Ross as cited by Inuwa and Oye
(2015) DW is the conglomerate of all Data Marts within the
enterprise. Information is always stored in the dimensional
model. Kimball view data warehousing as a constituency of
Data Marts. Data Marts are focused on delivering business
objectives for departments in the organization, and the DW is
a conformed dimension of the Data Marts.
Over the last few years, organizations have increasingly
turned to data warehousing to improve information flow and
decision support. A DW can be a valuable asset in providing
easy access to data for analysis and reporting. Unfortunately,
building and maintaining an effective DW has several
challenges (Güzin, 2007).

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 124
2. LITERATURE REVIEW
2.1.1 Data warehouse modelling
Ballard cited by Inuwa and Oye (2015) gave an assessment of
the evolution of the concept of data warehousing, as it relates
to data modeling for the DW, they defined database
warehouse modeling as the process of building a model for
the data in order to store in the DW. There are two data
modeling techniques that are relevant in a data warehousing
environment and they are:
i. Entity Relationship (ER) Modelling: ER modeling produces
a data model of the specific area of interest, using two basic
concepts: entities and the relationships between those entities.
Detailed ER models also contain attributes, which can be
properties of either the entities or the relationships. The ER
model is an abstraction tool because it can be used to
understand and simplify the ambiguous data relationships in
the business world and complex systems. ER modeling uses
the following concepts: entities, attributes and the
relationships between entities. The ER model can be used to
understand and simplify the ambiguous data relationships in
the business world and complex systems environments.
ii. Dimensional Fact Modeling: Dimensional modeling uses
three basic concepts: Measures, facts, and dimensions,
Dimensional modeling is powerful in representing the
requirements of the business user in the context of database
tables. Measures are numeric values that can be added and
calculated.
2.1.2 Data warehouse modelling techniques
Thomas and Carol cited by Inuwa and Oye (2015) derived the
way a DW or a Data Mart structure in dimensional modelling
can be achieved. Flat schema, Terraced Schema, Star Schema,
Fact Constellation Schema, Galaxy Schema, Snowflake
Schema, Star Cluster Schema, and Star flake Schema.
However there are two basic models that are widely used in
dimensional modeling: Star and Snowflake models.
i. Star Schema: The Star Schema (in Figure 2.1) is a relational
database schema used to hold measures and dimensions in a
Data Mart. The measures are stored in a fact table and the
dimensions are stored in dimension tables. For each Data
Mart, there is only one measure surrounded by the dimension
tables, hence the name star schema. The centre of the star is
formed by the fact table. The fact table has a column or the
measure and the column for each dimension containing the
foreign key for a member of that dimensions. The key for this
table is formed by concatenate all of the foreign key fields.
The primary key for the fact table is usually referred to as
composite key. It contain the measures, hence the name
“Fact”. The dimensions are stored in dimension tables. The
dimension table has a column for the unique identifier of a
member of the dimension, usually an integer of a short
character value. It has another column for a description.
(Inuwa&Oye, 2015).
ii. Snowflake Schema: Snowflake Schema model is derived
from the star schema and, as can be seen, looks like a snow
flake. The snowflake model is the result of decomposing one
or more of the dimensions, which generally have hierarchies
between themselves. Many-to-one relationships among
members within a dimension table can be defined as a
separate dimension table, forming a hierarchy as can be seen
in Figure 2.2.
Figure 2. 1: Star Schema (Jiawei, 2012)
Figure 2. 2: Snowflake Schema (Jiawei, 2012)
2.1.3 Data mart
A Data Mart is a small DW built to satisfy the needs of a
particular department or business area. The term Data Mart
refers to a sub entity of Data Warehouses containing the data
of the DW for a particular sector of the company (department,
division, service, product line, etc.). The Data Mart is a subset
of the DW that is usually oriented to a specific business line
or team. Whereas a DW combines databases across an entire
enterprise, Data Marts are usually smaller and focus on a
particular subject or department. Some Data Marts are called
Dependent Data Marts and are subsets of larger Data
Warehouses. Gopinath, Damodar, Lenin, Rakesh& Sandeep,
2014, also summarized the types of Data Marts as follows:
2.1.3.1 Independent and dependent data marts
An independent Data Mart is created without the use of a
central DW. This could be desirable for smaller groups within
an organization. A dependent Data Mart allows you to unite
your organization's data in one DW. This gives you the usual
advantages of centralization as can be seen in Figure 2.3.
2.1.3.2 Hybrid Data Marts A hybrid Data Mart allows you to combine input from sources
other than a DW. This could be useful for many situations,
especially when you need Ad-hoc integration, such as after a
new group or product is added to the organization as can be
seen in Figure 2.4:
a). A hybrid Data Mart transform data to combine input from
sources other than a DW.
b). Extracting the data from hybrid Data Mart based on
required conditions.
c). After extracting load into as a departmental Data Marts.

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 125
The Data Mart typically contains a subset of corporate data
that is valuable to a specific business unit, department, or set
of users. This subset consists of historical, summarized, and
possibly detailed data captured from transaction processing
systems (called independent Data Marts), or from an existing
enterprise DW (called dependent Data Marts). It is important
to realize that the functional scope of the Data Mart’s users
defines the Data Mart, not the size of the Data Mart database
(Chuck, Daniel, Amit, Carlos and Stanislav, 2006).
2.1.4 Architecture of the DW
Data contained in a DW holds five types of data: data
currency, existing data, data summarization (lightly and
highly summarized data), and Metadata (Inuwa&Garba 2015).
This traditional data warehousing architecture in Figure 2.5
encompasses the following components (Inuwa&Garba
2015):
i. Data sources as external systems and tools for extracting
data from these sources.
ii. Tools for transforming, which is cleaning and integrating
the data.
iii. Tools for loading the data into the DW.
iv. The DW as central, integrated data store.
v. Data Marts as extracted data subsets from the DW oriented
to specific business lines, departments or analytical
applications.
vi. A metadata repository for storing and managing metadata
vii. Tools to monitor and administer the DW and the
extraction, transformation and loading process.
viii. An OLAP (online analytical processing) engine on top of
the DW and Data Marts to present and serve multi-
dimensional views of the data to analytical tools.
ix. Tools that use data from the DW for analytical applications
and for presenting it to end-users.
This architecture exemplifies the basic idea of physically
extracting and integrating mostly transactional data from
different sources, storing it in a central repository while
providing access to the data in a multi-dimensional structure
optimized for analytical applications. However, the
architecture is rather old and, while this basic idea is still
intact, it is rather unclear and inaccurate about several facts:
Firstly, most modern data warehousing architectures use a
staging or acquisition area between the data sources and the
actual DW. This staging area is part of the Extract, Transform
and Load Process (ETL process). It temporarily stores
extracted data and allows transformations to be done within
the staging area, so source systems are directly decoupled and
no longer strained (Thilini& Hugh, 2010). Secondly, the
interplay between DW and Data Marts in the storage area are
not completely clear.
Figure 2. 3: Traditional Data Warehousing Architecture
(Inuwa&Garba, 2015).
Actually, in practice this is one of the biggest discourses about
data warehousing architecture with two architectural
approaches proposed by Bill Inmon and Ralph Kimball
(Inuwa&Garba, 2015). Inmon places his data warehousing
architecture in a holistic modelling approach of all operational
and analytical databases and information in an organization,
the Corporate Information Factory (CIF). What he calls the
atomic DW is a centralized repository with a normalized, still
transactional and fine-granular data model containing cleaned
and integrated data from several operational sources
(Inuwa&Garba, 2015).Inmon’s approach, also called
enterprise DW architecture by Thilini and Hugh (2010) is
often considered a top-down approach, as it starts with
building the centralized, integrated, enterprise-wide repository
and then deriving Data Marts from it to deliver for
departmental analysis requirements.
However, it is possible to build an integrated repository and
the derived Data Marts incrementally and in an iterative
fashion. Kimball on the other hand proposes a bottom-up
approach which starts with process and application
requirements (Kimball, Reeves & Ross) as cited by Inuwa and
Garba (2015). With this approach, first the Data Marts are
designed based on the organization’s business processes,
where each Data Mart represents data concerning a specific
process. The Data Marts are constructed and filled directly
from the staging area while the transformation takes places
between staging area and Data Marts.
The Data Marts are analysis-oriented and multi-dimensional.
The DW is then just the combination of all Data Marts, where
the single Data Marts are connected and integrated with each
other via the data bus and so-called conformed dimensions
that are Data Marts use, standardized or ‘conformed’
dimension tables (Inuwa&Garba, 2015).
When two Data Marts use the same dimension, they are
connected and can be queried together via that identical
dimension table. The data bus is then a net of Data Marts,
which are connected via conformed dimensions. This
architecture (also called Data Mart bus architecture with
linked dimensional Data Marts by Thilini and Hugh (2010)
therefore forgoes a normalized, enterprise-wide data model
and repository.
In Figure 2.4, there are a number of options for architecting a
Data Mart. For example:
Figure 2. 4: DW Architecture (Inuwa&Garba, 2015)

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 126
i. Data can come directly from one or more of the databases in
the operational systems, with few or no changes to the data in
format or structure. This limits the types and scope of analysis
that can be performed. For example, you can see that in this
option, there may be no interaction with the DW Meta Data.
This can result in data consistency issues.
ii. Data can be extracted from the operational systems and
transformed to provide a cleansed and enhanced set of data to
be loaded into the Data Mart by passing through an ETL
process. Although the data is enhanced, it is not consistent
with, or in sync with, data from the DW.
iii. Bypassing the DW leads to the creation of an independent
Data Mart. It is not consistent, at any level, with the data in
the DW. This is another issue impacting the credibility of
reporting.
iv. Cleansed and transformed operational data flows into the
DW. From there, dependent Data Marts can be created, or
updated. It is a key that updates to the Data Marts are made
during the update cycle of the DW to maintain consistency
between them. This is also a major consideration and design
point, as you move to a real-time environment. At that time, it
is good to revisit the requirements for the Data Mart, to see if
they are still valid.
However, there are also many other data structures that can be
part of the data warehousing environment and used for data
analysis, and they use differing implementation techniques.
Although Data Marts can be of great value, there are also
issues of currency and consistency. This has resulted in recent
initiatives designed to minimize the number of Data Marts in
a company. This is referred to as Data Mart Consolidation
(DMC). Data Mart consolidation may sound simple at first,
but there are many things to consider. A critical requirement,
as with almost any project, is executive sponsorship, because
you will be changing many existing systems on which people
have come to rely, even though the systems may be
inadequate or outmoded. To do this requires serious support
from senior management. They will be able to focus on the
bigger picture and bottom-line benefits, and exercise the
authority that will enable making changes (Chuck et al.,
2006).
2.1.5 Benefits of data warehousing
There are several benefits of data warehousing. The most
important ones are listed as follows (Kimball & Ross, 2002):
i. DW improves access to administrative information for
decision makers.
ii. It can get data quickly and easily perform analysis. One can
work with better information, make decisions based on data.
DW increases productivity of corporate decision-makers.
iii. Data extraction from its original data sources into the
central area resolves the performance problem, which arises
from performing complex analyses on operational data.
iv. Data in the warehouse is stored in specialized form, called
a multidimensional database. This form makes data querying
efficient and fast.
v. A huge amount of data is usually collected in the DW.
Compared with relational databases that are still very popular
today, data in the warehouse does not need to be in
normalized form. In fact, it is usually de-normalized to
support faster data retrieval.
2.1.6 Data warehousing in medical field
Health care organizations require data warehousing solutions
in order to integrate the valuable patient and administrative
data fragmented across multiple information systems within
the organization. As stated by Kerkri cited by Saliya (2013),
at a technical level, information sources are heterogeneous,
autonomous, and have an independent life cycle. Therefore,
cooperation between these systems needs specific solutions.
These solutions must ensure the confidentiality of patient
information. To achieve sufficient medical data share and
integration, it is essential for the medical and health
enterprises to develop an efficient medical information grid
(Zheng et al., 2008).
A medical data warehouse is a repository where healthcare
providers can gain access to medical data gathered in the
patient care process. Extracting medical domain information
to a data warehouse can facilitate efficient storage, enhances
timely analysis and increases the quality of real time decision
making processes. Currently medical data warehouses need to
address the issues of data location, technical platforms, and
data formats; organizational behaviors on processing the data
and culture across the data management population. Today’s
healthcare organizations require not only the quality and
effectiveness of their treatment, but also reduction of waste
and unnecessary costs. By effectively leveraging enterprise
wide data on labour expenditures, supply utilization,
procedures, medications prescribed, and other costs associated
with patient care, healthcare professionals can identify and
correct wasteful practices and unnecessary expenditures
(Sahama & Croll, 2007).
Medical domain has certain unique data requirements such as
high volumes of unstructured data (e.g. digital image files,
voice clips, radiology information, etc.) and data
confidentiality. Data warehousing models should
accommodate these unique needs. According to Pedersen and
Jensen cited by Saliya (2013) the task of integrating data from
several EHR systems is a hard one. This creates the need for a
common standard for EHR data.
According to Kerkri cited by Saliya (2013), the advantages
and disadvantages of data warehousing are given below.
Advantages:
1. Ability to allow existing legacy systems to continue in
operation without any modification
2. Consolidating inconsistent data from various legacy
systems into one coherent set
3. Improving quality of data
4. Allowing users to retrieve necessary data by themselves
Disadvantages:
1. Development cost and time constraints
2.1.7 Cancer data warehouse architecture
Cancer known medically as a malignant neoplasm, is a broad
group of various diseases, all involving unregulated cell
growth. In cancer, cells divide and grow uncontrollably,
forming malignant tumours, and invade nearby parts of the
body. The cancer may also spread to more distant parts of the

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 127
body through the lymphatic system or bloodstream. Not all
tumours are cancerous. Benign tumours do not grow
uncontrollably, do not invade neighbouring tissues, and do not
spread throughout the body. Determining what causes cancer
is complex. Many things are known to increase the risk of
cancer, including tobacco use, certain infections, radiation,
lack of physical activity, poor diet and obesity, and
environmental pollutants. These can directly damage genes or
combine with existing genetic faults within cells to cause the
disease. Approximately five to ten percent of cancers are
entirely hereditary. People with suspected cancer are
investigated with medical tests. These commonly include
blood tests, X-rays, CT scans and endoscopy (Sheta &
Ahmed, 2012).
Figure 2. 5: Cancer DW Architecture (Sheta& Ahmed, 2012)
2.1.8 Influenza disease data warehouse
architecture Influenza, commonly known as the ‘flu’, is an infectious
disease of birds and mammals caused by ribonucleic acid
(RNA) viruses of the family Orthomyxoviridae, the influenza
viruses, (Rajib, 2013). The most common symptoms are
chills, fever, sore throat, muscle pains, headache (often
severe), coughing, weakness/fatigue Irritated, watering eyes,
Reddened eyes, skin (especially face), mouth, throat and nose,
Petechial Rash and general discomfort. Influenza may
produce nausea and vomiting, particularly in children.
Typically, influenza is transmitted through the air by coughs
or sneezes, creating aerosols containing the virus. Influenza
can also be transmitted by direct contact with bird droppings
or nasal secretions, or through contact with contaminated
surfaces. Influenza spreads around the world in seasonal
epidemics, resulting in about three to five million yearly cases
of severe illness and about 250,000 to 500,000 yearly deaths
(Rajib, 2013). People who suspected influenza are
investigated with medical tests. These commonly include
Blood test (white blood cell differential), Chest x-ray,
Auscultation (to detect abnormal breath sounds),
Nasopharyngeal culture.
Figure 2.6 shows the proposed architecture for the health care
data warehouse specific to Influenza disease by Rajib in 2013.
Architecture of Influenza specific health care data warehouse
system builds with Source Data components in the left side
where multiple data that comes from different data source and
transform into the Data Staging area before integrating. The
Data staging component present at the next building block.
Those two blocks is under Data Acquisition Area. In the
middle Data Storage component that manages the data
warehouse data. This component also with Metadata, that also
keep track of the data and also with Data Marts. Last
component of this architecture is Information Delivery
component that shows all the different ways of making the
information from the data warehouse available to the user for
further analysis (Rajib, 2013).
Figure 2. 6: Data Warehouse Architecture for Influenza
Disease (Rajib, 2013)
2.1.9 Cardiac surgery data warehousing model
Cardiac Surgery clinical data can be distributed across various
disparate and heterogeneous clinical and administrative
information systems. This makes accessing data highly time
consuming and error prone .
A data warehouse can be used to integrate the fragmented data
sets. Once the data warehouse is created it should be
populated with data through Extract, Transform and Load
processes. Figure 2.12 shows a graphical overview of cardiac
surgery data warehousing model (Saliya, 2013).
Figure 2. 7: Data Warehousing Model for Integrating
Fragmented Electronic Health Records from Disparate
and Heterogeneous Cardiac Surgery Clinical Data Stores
(Saliya, 2013).
2.1.10 Diabetic data warehousing model
Diabetes is a defect in the body’s ability to convert glucose
(sugar) to energy. Glucose is the main source of fuel for our
body. When food is digested it is changed into fats, protein, or
carbohydrates. Foods that affect blood sugars are called
carbohydrates. Carbohydrates, when digested, change to

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 128
glucose. Examples of some carbohydrates are: bread, rice,
pasta, potatoes, corn, fruit, and milk products. Individuals
with diabetes should eat carbohydrates but must do so in
moderation. Glucose is then transferred to the blood and is
used by the cells for energy. In order for glucose to be
transferred from the blood into the cells, the hormone - insulin
is needed. Insulin is produced by the beta cells in the pancreas
(the organ that produces insulin). In individuals with diabetes,
this process is impaired. Diabetes develops when the pancreas
fails to produce sufficient quantities of insulin, Type 1
diabetes or the insulin produced is defective and cannot move
glucose into the cells and occurs most frequently in children
and young adults, although it can occur at any age. Type 1
diabetes accounts for 5-10% of all diabetes in the United
States. There does appear to be a genetic component to Type 1
diabetes, but the cause has yet to be identified. Type 2
diabetes. Either insulin is not produced in sufficient quantities
or the insulin produced is defective and cannot move the
glucose into the cells, is much more common and accounts for
90-95% of all diabetes. Type 2 diabetes primarily affects
adults, however recently Type 2 has begun developing in
children. There is a strong correlation between Type 2
diabetes, physical inactivity and obesity, (Abubakar et al.,
2014).
Gap Analysis
The research carried out by other researchers, only focus on
building a data warehouse for a particular disease. No single
study exists which adequately covers the integration of
clinical record of patients into a data warehouse for data
analysis and mining that is not specific to a single disease.
There is also no specific research that covers the integration of
medical record of patients using the Nigerian medical records
for analysis and mining using data visualization for decision
making.Therefore this research is designing a framework for
integrating patient clinical records into a single data
warehouse for data analysis and mining using data
visualization technique that is not specific to single disease
using Nigeria medical record.
3. METHODOLOGY The following research method and tools were used in
achieving these research objectives:
System Analysis: UML was used in analysing all the
physical and logical models. OLAP: Online Analytic
processing (Server) was used for processing and analysing
data from the server on a web browser. ETL: Extraction
transformation and loading of data into the data warehouse for
mining and visualization purpose SSIS: Integrating the
operations data with the main data warehouse database.
Visualization Technique: Presentation of mine data
from the data warehouse as visual effects rather than row and
columns. Data are displayed in form of graphs and shapes for
easy interpretation and understanding. Microsoft Visio 2015
as the UML tool, was used in in designing all the logical
models of the proposed system. Aspx, HTML 5 and Bootstrap
CSS were used in designing the GUI and SQL Server
Reporting Services was used in designing the data
visualization, clinical decision support and mining outputs of
the system. The programming language of choice for the
middle end was C# pronounced C-sharp. The database used in
designing the physical models is Microsoft SQL Server 2014,
while, SQL Server 2012 server tools were used for writing the
ETL (Extraction, Transformation and Load) program.
4. RESEARCH RESULTS
System Prototype Development and Validation
The system prototype development is the actual application of
the analysis and design that has been carried out. In this phase
of the study, we have designed the DW (Fact and dimension
tables) prototype, the ETL (Extract, Transform and Load), the
front end (GUI) and the Middle end of the application for the
purpose of this study. Validation process involves the
confirmation by medical system administrators and
personnel’s that an information system (DW prototype) has
been realized appropriately and it is in conformity with the
User’s needs and intended use. Figures 1-7 are available in the
appendix.
FIGURE:1 Shows the architectural design of the Framework
for Data Warehouse and Mining Clinical Records. The
architecture has the followings abilities:
i. Integration of the independent and dependent Data Marts
within the architecture.
ii. It has a multi-tier ETL which are simpler and in different
stages.
iii. It has a standard access points for all medical and non-
medical experts (Using a three tier server).
iv. It has the ability to Mine and analyse records using Data
Visualization
The architecture has a back and frond end system in which so
many activities are carried out. The back end systems
comprise of the operational data source system, data staging
area and the data presentation area. Data are first extracted
from different operational data source systems using ETL and
then stored at the data staging area where it is being processed
as soon as it is captured. The activities of the ETL at the data
staging area include data cleansing and validation, data
integration, data fixing and data entry errors removal,
transforming and refreshing data into a new normalized
standard. As soon as data is cleaned, the transformed data are
loaded and indexed into the data presentation area where the
DW is located. The frontend systems in the other hand
comprise of the main servers (OLAP) and data access tools.
The OLAP server hold the copy of the cleansed clinical
records. The data access tool is the interface where
applications are stored, which allows for data Analysis,
Reporting/Querying and Data mining activities.
FIGURE: 2, is about Creating and loading of the Clinical
DW database
The DW database was created on an MSSQL Server 2014
database, and the data loading was also done through the SSIS
package. Fact and Dimension tables were pushed into the DW
database, Figure 2 shows Physical database of the DW Model
by Star Schema. The DW database is the one that integrates

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 129
the Fact and Dimension tables of patient’s clinical records
into the MSSQL Server 2014 database. It was part of the
MSSQL Server database that we used as the database
repository. The DW database was populated with the correct
data of good quality that we can make use of as the data
repository. Data visualization is all about presenting data in
graphical format rather than rows and columns thereby
making data interpretation easy and is best use by decision
makers to take decisions for organizations.
FIGURE 3, shows some of the Dimension and Fact tables
that were extracted from the source system into the staging
database area. The tables were cleansed and refreshed at this
point and ready for transfer into their respective Data Marts.
Having designed the Fact and Dimension tables and the
extraction of data from the source system, then the researcher
populated the Data Marts with the data that was extracted
earlier from the staging databases. It is now from the Data
Marts that another ETL was performed to transport the data
into the DW database.
System Verification, Reports and Data
Visualization
The best way to verifying the data in the DW is to prepare
queries on these data. In this study, certain reports, data
analysis and data visualization were presented and the purpose
of these reports and analysis is to demonstrate the usefulness
of the DW approach to data presentation and decision making.
Even though these reports and analysis were based on some
random requirements, this set of sample reports and analysis
can be used as a basis for generating more comprehensive sets
by applying complex queries on the data. We have classified
the Analysis, Reports and Data Visualization that we
generated from the DW based on all the analysis on patient
diagnosis and details. Figure 4, illustrates the general system
architecture for this study. It shows how the Source System
database, Servers and the User/administrator system are
connected for possible data visualization and decision making.
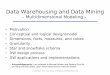
FIGURE: 5, shows data visualization of Malaria patients and
their LGA of residence within the year 2015, 2016 and 2017.
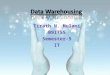
Figure 6, shows data visualization of Tuberculosis patients
and their LGA of residence within the year 2015, 2016 and
2017. Decision makers can use the visualized report to
determine the trend of infection between the various patients
LGA of residence. Proper decision can be taken on how to
curb the rate of infection within the LGA’s with high rate of
illness by setting appropriate infrastructure and medical
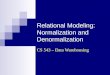
personnel in those LGA. Figure 7, shows a report of patients
diagnosed with typhoid-fever based on their gender, month
and the year of diagnosis.
5. CONCLUSION This research has design and implemented a Clinical DW and
Mining system using data visualization technique within the
context of the healthcare service, to better incorporate
patient records into single systems for simpler and improved
data mining, analysis, reporting and querying. The Clinical
DW we built contains only the data that is required for data
mining, reporting and analysis for the purpose of this study
and it can be updated periodically, such that all the data can
be integrated from different source systems into the central
DW. The system is design to operate as a distributed system.
Periodic update on a daily basis is possible because
contemporary technologies have narrowed the gap between
updates. This can enable organizations to have a “real time”
DW which can be analyzed using an OLAP Server.
The research focused on developing a Framework for DW and
Mining of clinical records of patient, for improve data
analysis and mining using data visualization. The study also
considered the ideologies of data warehousing in the course of
this research and demonstrated how data can be incorporated
from diverse desperate heterogeneous clinical data stores into
a single DW for mining and analysis purpose, to aid
medical practitioners and decision makers in decision making.
The researchers have also been able to develop a web based
data mining, reporting and analysis tool (GUI) where users
can interact with the system to get a speedy and timely
information needed for the clinical decision making and
community diagnosing.
The Framework for DW and Mining of clinical record of
patients was design not to be specific to only a number of
disease but to accept as many diseases as possible without any
limitation. The ideologies that the researchers followed to
develop this system makes it scalable and as such, it can be
adopted for any form of disease, infections analysis and
mining by medical institutions and healthcare providers in
Nigeria. The designed framework can be used by industry
professionals and researcher for implementing data
warehousing system in the medical field, for long time data
analysis and mining. The framework can also be used for
community diagnosing in cases of outbreak of certain disease.
Developing a Framework for DW and Mining of Clinical
records is very essential, particularly for medical decision-
makers, academic researchers, IT professionals and non-
professional. Clinical data mining must not only support
medical professionals and decision makers to understand the
past, but also it strive professionals to work towards new
prospects.

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 130
6. ACKNOWLEDGMENTS We thank the experts who have helped to review this paper.
7. REFERENCES
[1] Abubakar, etal (2014). Building a diabetes data warehouse to support decision making in healthcare industry. IOSR Journal of
Computer Engineering (IOSR-JCE), 16(2), e-ISSN: 2278-0661, p- ISSN: 2278-8727Volume 16, Issue 2, Ver. IX (Mar-Apr.
2014), PP 138-143 www. Retrieved from iosrjournal.org
[2] Chuck, B., Daniel, M. F., Amit, G. C., & Stanislav, V. (2006). Dimensional Modeling: In a DSS Environment. NY 10504-1785
U.S.A.: IBM Corporation, North Castle Drive Armonk
[3] Demetriades, J. E., Kolodner, R. M., & Christopherson, G. A. (2005). Person Centered Health Records. Towards Healthy People.
. Health Informatics Series. USA: Springer. Tavel, P. 2007 Modeling and Simulation Design. AK Peters Ltd.
[4] Goldstein, D., Groen, P. J., Ponkshe, S., & Wine, M. (2007). Medical informatics 20/20: quality and electronic health records
through collaboration, open Solutions, and innovation. Massachusetts, Sudbury, USA: Jones and Bartlett Publishers, Inc.
[5] Gopinath, T., Damodar, N. M., Lenin, Y., Rakesh, S., & Sandeep, M. (2014). Scattered Across Data Mart Troubles Triumph Over
in the course of Data Acquisition through the Decision Support System. International Journal of Computer Technology and
Application, 2(5), 411-419.
[6] Güzin, T. (2007). Developing a Data Warehouse for a University Decision Support System. Atilim University, The Graduate
School of Natural and Applied Sciences.
[7] Ibrahim I., & Oye, N. (2015). Design of a Data Warehouse Model for a University Decision Support System. Information and
Knowledge Management, 5.
[8] Inuwa, I., & Garba, E. (2015). An Improved Data Warehouse Architecture for SPGS, MAUTECH, Yola, Nigeria. West African
Journal of Industrial & Academic Research, 14(1).
[9] Kimball, R. &. (2002). The Data Warehouse Toolkit: The Complete Guide to Dimensional Modelling. In R. Kimball, & M. Ross,
The Data Warehouse Toolkit: The Complete Guide to Dimensional Modelling. New York: John Wiley & Sons, Inc.
[10] Mann, L. (2005). From “silos” to seamless healthcare: bringing hospitals and GPs back together again. Medical Journal of
Australia, 1(182), 34-37. Retrieved from http://www.mja.com.au/public/issues/182_01_030105/man10274_fm.html
[11] Rajib, D. (2013). Health care data warehouse system Architecture for influenza (flu) Diseases. Global Institute of Management &
Technology, Krishnanagar., Department of Computer Science & Engineering, West Bengal, India.
[12] Sahama, T. R., & Croll, P. R. (2007). A data warehouse architecture for clinical data warehousing. First Australasian Workshop
on Health Knowledge Management and Discovery. Retrieved from http://crpit.com/confpapers/CRPITV68Sahama.pdf
[13] Saliya, N. (2013). Data warehousing model for integrating fragmented electronic health records from disparate and
heterogeneous clinical data stores. Queensland University of Technology, School of Electrical Engineering and Computer Science
Faculty of Science and Engineering, Australia.
[14] Shepherd, M. (2007). Challenges in health informatics. 40th Hawaii International Conference on System Sciences.
doi:10.1109/HICSS.2007.123
[15] Sheta, O., &Ahmed, A. N. (2012). Building a Health Care Data Warehouse for Cancer Diseases. International Journal of
Database Management Systems (IJDMS), 4.
[16] Thilini, A., & Hugh, W. (2010). Key organizational factors in Data Warehouse architecture selection. Journal of Decision Support
Systems, 49(2), 200–212.
[17] Zheng, R., Jin, H., Zhang, H., Liu, Y., & Chu, P. (2008). Heterogeneous medical data Share and integration on grid. International
Conference on BioMedical Engineering and Informatics. doi:10.1109/BMEI.2008.185
[18] Zhu, X., & Davidson, I. (2007). Knowledge Discovery and Data Mining: Challenges and Realities. New York: Hershey, New
York.

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 131
APPENDIX
Figure 1: Framework for Data Warehousing and Mining Clinical Records of Patients
Figure 2: Star schema of the designed Framework for Data Warehousing and Mining Clinical Records of
Patients

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 132
Figure 3: ETL for data cleansing and loading of the DW
Figure 4: Showing the structural architecture of the system
User PCs Web
Browser connection
Source SystemStaging Area
(ETL Server)
OLAP Server
Microsoft SQL
2014
Data Warehouse
Database Server
MSSQL Database
2012MSSQL Database
2012
MSSQL Server Reporting
Services 2012

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 133
Figure 5: Malaria output result, based on month and year of diagnosis
Figure 6: Tuberculosis report based on LGA of residence and year of diagnosis

International Journal of Computer Applications Technology and Research
Volume 8–Issue 04, 122-134, 2019, ISSN:-2319–8656
www.ijcat.com 134
Figure 7: Typhoid-Fever report based on gender, month and year of diagnosis