Embed Size (px)
Citation preview
Fourth Annual eHealth Developer’s SummitSummary Report
eHealth:Striving for Critical Mass
Fourth Annual
eHealthDevelopers’Summit TM
Presented by:
Copyright © 2004 eHealth Institute™ All rights reserved.
The Fourth Annual eHealth Developers’ Summit™ and the preparationof this report were made possible by grants from the followingorganizations and corporate contributors:
5.0 SponsorCalifornia HealthCare Foundation (www.chcf.org)
4.0 SponsorsW.K. Kellogg Foundation (www.wkkf.org)Markle Foundation (www.markle.org)
3.0 SponsorDivision of Cancer Control and Population Sciences, National CancerInstitute (http://dccps.nci.nih.gov/hcirb/)
2.0 SponsorHealth e-Technologies Initiative (www.hetinitiative.org)
1.0 SponsorKaiser Permanente (www.kp.org)
3.0 Corporate ContributorPurdue Pharma L.P. (www.pharma.com)
1.0 Corporate ContributorsMedical Directions, Inc. (www.md-inc.com)
Disclaimer:The views and ideas expressed in this report reflect those of variousindividuals at the Summit and are not necessarily those of the authorsor the Summit attendees as a whole. Any mention of specificorganizations, trade names, and products in this report is forinformational purposes only and does not imply endorsement orsupport for these organizations and/or products.
Suggested Citation:Eng TR, Beauchamp N. eHealth: Striving for Critical Mass. Seattle,Washington: eHealth Institute, May 2004.
Comments and feedback about this report should be directed to TomEng at: [email protected].
This entire report and additional information about the eHealthDevelopers’ Summit are available at: www.ehealthinstitute.org/summit/.
The eHealth Institute (www.ehealthinstitute.org) is a private, charitable501(c)(3) nonprofit organization that explores ways to use emergingtechnologies, especially the Internet, to improve the health and wellbeing of all people, including the underserved.
eHealth:Striving for Critical Mass
Prepared by
Thomas R. Eng, PresidentNatasha Beauchamp, Consultant
eHealth InstituteMay 2004
Summary Report of
The Fourth Annual eHealth Developers’ SummitNovember 5–7, 2003San Diego, CA

Acknowledgments
First and foremost, the authors thank the speakers, moderators, teamleaders, and other participants of the Fourth Annual eHealthDevelopers’ Summit who were the generators of the ideas in thisreport. We also thank the following colleagues who reviewed andprovided valuable feedback about the contents: Darrell Atkin, TheLaunch Pad; Gwendolyn Doebbert, California Department of HealthServices; Kerry Evers, Pro-Change Behavior Systems, Inc.; HankFanberg, CHRISTUS Health; Verle Harrop, National ResearchCouncil, Canada; Avery Hudson, Memorial Sloan-Kettering CancerCenter; Tom Lee, California HealthCare Foundation; and Madhu Nair,Ansya Enterprise Solutions Inc. In addition, Betsy Hudson providedpublishing assistance in preparing this report.
The success of the Summit was largely attributable to the work of thePlanning and Advisory Committees. The Planning Committeemembers included: David Ahern, Health e-Technologies Initiative;Darrell Atkin, The Launch Pad; Rick Botelho, University of Rochester;Connie Dresser, National Cancer Institute; Kerry Evers, Pro-ChangeBehavior Systems, Inc.; John Harris, Medical Directions, Inc.; LindaHarris, National Cancer Institute; Stephanie Karsten, Humanitas, Inc.;Marc Larsen, Overlake Hospital Medical Center; Tom Lee, CaliforniaHealthCare Foundation; Denise Runde, FAACT; David Ryan,University of Toronto.
The Advisory Committee members included: Peter Basch, MedStarHealth; Gary Kreps, National Cancer Institute; Kevin Patrick,University of California, San Diego; Barbara Rapchak, Leap of FaithTechnologies, Inc.; Andrew Robinson, Patient2Patient, Inc.; David P.Ross, Victor E. Speas Foundation; Steve Solomon, Centers for DiseaseControl and Prevention; Gale Wilson-Steele, MedSeek.
This report and the Summit would not have been possible without thefunding provided by the Summit sponsors. We extend special thanksto David Ahern, Ken Brier, Carol Diamond, Connie Dresser, LindaHarris, John Harris, Sam Karp, Sanjay Koyani, Gary Kreps, Tom Lee,Janice Nall, Ben Reis, Anna-Lisa Silvestre, and Henrie Treadwell, fortheir generous support.
Contents6 Executive Summary
9 Introduction to the Summit
11 The State of eHealth
18 Patient- and Provider-BasedElectronic Health Records and Primary Care
24 eHealth Research and Dissemination
31 Sustaining and Commercializing eHealth
39 Conclusions
42 Appendix A. Organizations Representedat the Summit
44 Appendix B. Summit Awards
6 Summary Report, Fourth Annual eHealth Developers’ Summit
Executive Summary
The focus of many eHealth activities in publichealth revolves around enhancing healthsurveillance and communication. Variousinitiatives of the Centers for Disease Control andPrevention illustrate the movement towardadoption of standards and secureinteroperability across multiple public healthjurisdictions. Pharmaceutical companies, bothconsumers and suppliers of eHealth, remain amajor sponsor of online content but aremethodical in responding to market forces andare very selective in supporting eHealth projects.
Consumer use of online health information isnow the norm and many consumers look uphealth information for other people. Anestimated 82 million consumers used onlinehealth information in 2003, but their “zone ofinfluence” reached more than 135 million peopleas many users searched on behalf of others. Two-thirds of core users report using the Web beforeconsulting physicians or other resources.
Patient/consumer- and provider-basedelectronic health records were major topics ofdiscussion at the Summit. Both personal healthrecord (PHR) and electronic medical record(EMR) products have great potential to improvehealth care quality and reduce costs andmedical errors. Attributes that should beconsidered in evaluating a PHR product includeproduct/device portability, data collectionmethods, storage capacity, data security, anddata transfer capabilities. Most Summitparticipants agreed that the biggest barrier to
This report summarizes the discussions at theFourth Annual eHealth Developers’ Summit,held November 5–7, 2003, in San Diego,California. More than 135 eHealth leaders froma range of disciplines, including health care andmedicine, business, public health, andcomputer science and technology participated.Participants represented more than 120organizations, including commercial eHealthcompanies, health care organizations, academicinstitutions, government agencies, technologycorporations, pharmaceutical and medicaldevice companies, nonprofit organizations,foundations, and investors.
The past year may have marked a turning pointfor eHealth in that a “critical mass” of adoptersseems to have crystallized. Health IT has beenembraced by many prominent U.S. politicalleaders and independent organizations as amajor solution for disjointed health care andpublic health systems.
Hospital and health plans, in particular, havedramatically increased their use of eHealthsolutions in the last few years. And some ofthose using eHealth products for administrativesupport functions have seen substantial savings.eHealth adoption by health care providers is alsoincreasing as more health care institutions aremigrating to eHealth solutions. Onlinecontinuing medical education (CME) is a rapidgrowth sector with nearly half of all physiciansfulfilling their continuing education require-ments online.

eHealth: Striving for Critical Mass 7
adoption of the PHR is the lack of a clear valueproposition.
Current EMR products are not yet sufficientlycompelling for primary care practices and donot meet the needs of primary care physicians.In the real world of primary care, reducingmedical errors and providing better quality careoften are not sufficient reasons or incentives tojustify use of EMRs. Four top issues that EMRdevelopers should address for primary carepractices are affordability, compatibility,interoperability, and data stewardship. Summitparticipants cited lack of reimbursement andlack of tools that are integrated into theworkflow as the major barriers to widespreaduse of EMRs.
Recent Web-based PHRs that interface with theindividual’s health plan and Web-based EMRsthat provide shared provider-patient access areblurring the boundaries of these products, andadditional hybrid EMR/PHR systems are likelyin the near future. Given the wide spectrum ofeHealth technology options available in themarketplace, government regulations orrequirements supported by a consortium ofpayors will probably be needed to realizeinteroperability.
Research has demonstrated that a range ofpeople can successfully use many eHealthproducts. In some cases, users actually preferelectronic modes of communication over face-to-face interactions. Many behavioral eHealthprograms are rooted in social cognitive theory,and seek to improve user confidence (self-efficacy) in implementing behavioral changes.
Developers of eHealth products for diversegroups should consider the special health risks ofthese populations, and take steps to enhance thecultural appropriateness and usability of theirproducts. Developers should be aware that mostpeople of color live above the poverty line andthat they represent a growing market opportunity.Seventy percent of Summit participants believed
that there is a substantial market for eHealthproducts for the underserved.
The time lapse between research results andtheir implementation in product developmentcan be long. Win-win arrangements betweenacademic researchers and commercial companieswith common target audiences may help speeddissemination and infusion of research findingsinto marketable products.
Among developers at the Summit, the mostimportant attributes of a commerciallysuccessful eHealth product were demonstratedcost savings, user satisfaction, and positivehealth status outcomes. Among funders andpurchasers of eHealth products, demonstratedcost savings and positive health outcomes weremost important.
Aligning funding sources with the stage of theeHealth business is critical. Angel investors areappropriate when companies are past the ideastage and need capital to create a prototype andprepare for launch. Corporate funding, on theother hand, is often pursued as a way to attainmarket position. From a deal evaluationperspective, the value of product simplicity, easeof implementation, and convenience should notbe underestimated. Angel investors are typicallyattracted to ideas that use existing technology ina new or creative way, are well-defined, andmeet a proven market need. Those that mimiccurrent procedures and require minimal changeon the part of end users are preferred over thosethat have major barriers to user adoption.
In pursuing strategic corporate relationships,developers need to be clear about the benefits ofaligning with a large corporation because theallure of highly visible co-branding may not besufficient justification. It is important toarticulate specifically what the large corporationcontributes—beyond name recognition—thatwill make a mutually strategic relationship.eHealth products that “complete” a corporation’soffering are a particularly strong proposition.
8 Summary Report, Fourth Annual eHealth Developers’ Summit
Several major needs and gaps were evident as aresult of discussions at the Summit:
Without considerably more public andprivate funding and incentives for eHealthadoption, the benefits of eHealth will notlikely be realized beyond large health careorganizations. Further national progress onthis front requires continued leadership andfunding.
More relevant and compelling eHealthproducts for medium and small group healthcare practices are needed.
Additional experimentation is needed todevelop products and business models thatproduce a tangible benefit to both consumersand the usual direct payors of eHealthproducts, such as health care organizationsand employers.
Proactive efforts are essential in addressinginteroperability, privacy and security, andother issues related to the increasing varietyof personal health monitoring andcommunication devices being deployedoutside traditional health care settings.
Public and private funders of programs andservices for underserved populations shouldconsider collaborating with eHealthdevelopers to generate new models and toolsto address longstanding disparities that havebeen resistant to traditional approaches.
eHealth: Striving for Critical Mass 9
Which of the following best describes your primary discipline?
6%
10%
14%
19%
23%
29%
Other
Public health
Basic sciences/research
Business
Computer science/technology
Healthcare/medicine
Disc
iplin
e
Percentage
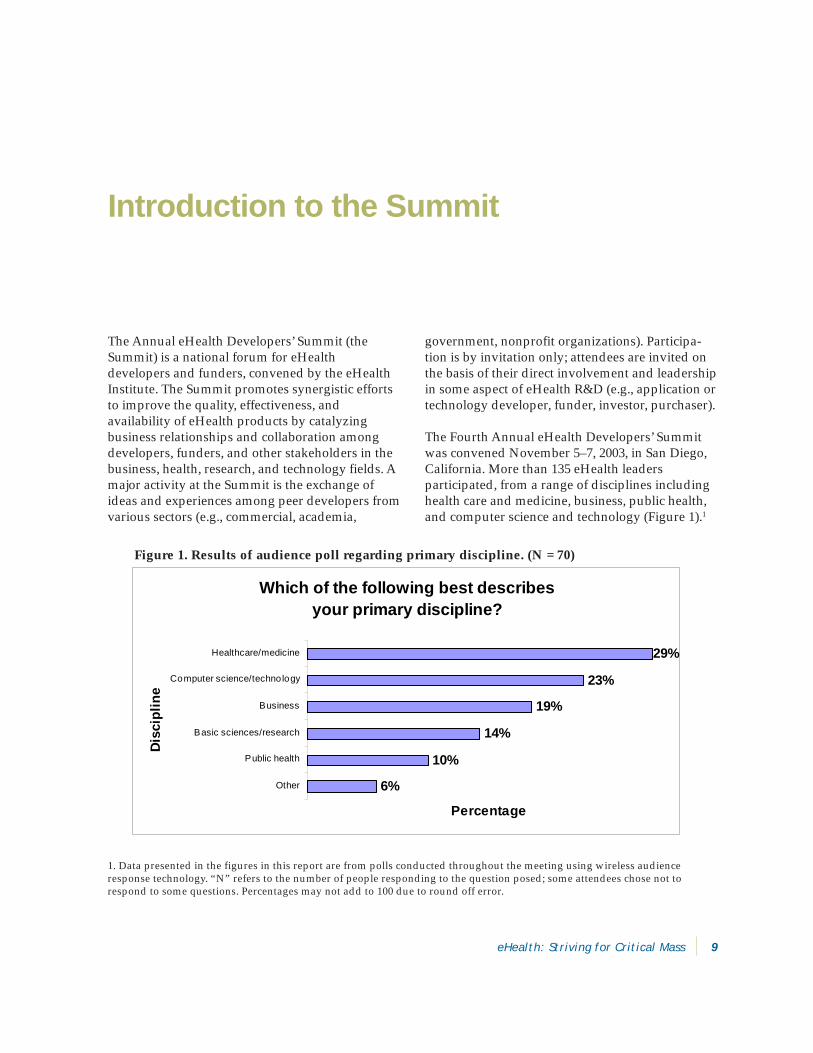
Figure 1. Results of audience poll regarding primary discipline. (N = 70)
government, nonprofit organizations). Participa-tion is by invitation only; attendees are invited onthe basis of their direct involvement and leadershipin some aspect of eHealth R&D (e.g., application ortechnology developer, funder, investor, purchaser).
The Fourth Annual eHealth Developers’ Summitwas convened November 5–7, 2003, in San Diego,California. More than 135 eHealth leadersparticipated, from a range of disciplines includinghealth care and medicine, business, public health,and computer science and technology (Figure 1).1
The Annual eHealth Developers’ Summit (theSummit) is a national forum for eHealthdevelopers and funders, convened by the eHealthInstitute. The Summit promotes synergistic effortsto improve the quality, effectiveness, andavailability of eHealth products by catalyzingbusiness relationships and collaboration amongdevelopers, funders, and other stakeholders in thebusiness, health, research, and technology fields. Amajor activity at the Summit is the exchange ofideas and experiences among peer developers fromvarious sectors (e.g., commercial, academia,
Introduction to the Summit
1. Data presented in the figures in this report are from polls conducted throughout the meeting using wireless audienceresponse technology. “N” refers to the number of people responding to the question posed; some attendees chose not torespond to some questions. Percentages may not add to 100 due to round off error.
10 Summary Report, Fourth Annual eHealth Developers’ Summit
Which best describes your primary organizational affiliation?
3%5%
6%7%
10%14%
23%32%
None o f the above
Large IT/tech. corporation
Pharmaceutical/device company
Health care company
Nonprofit o rganization
Government agency
Academic institution
eHealth/tech. small business
Aff
iliat
ion
Percentage
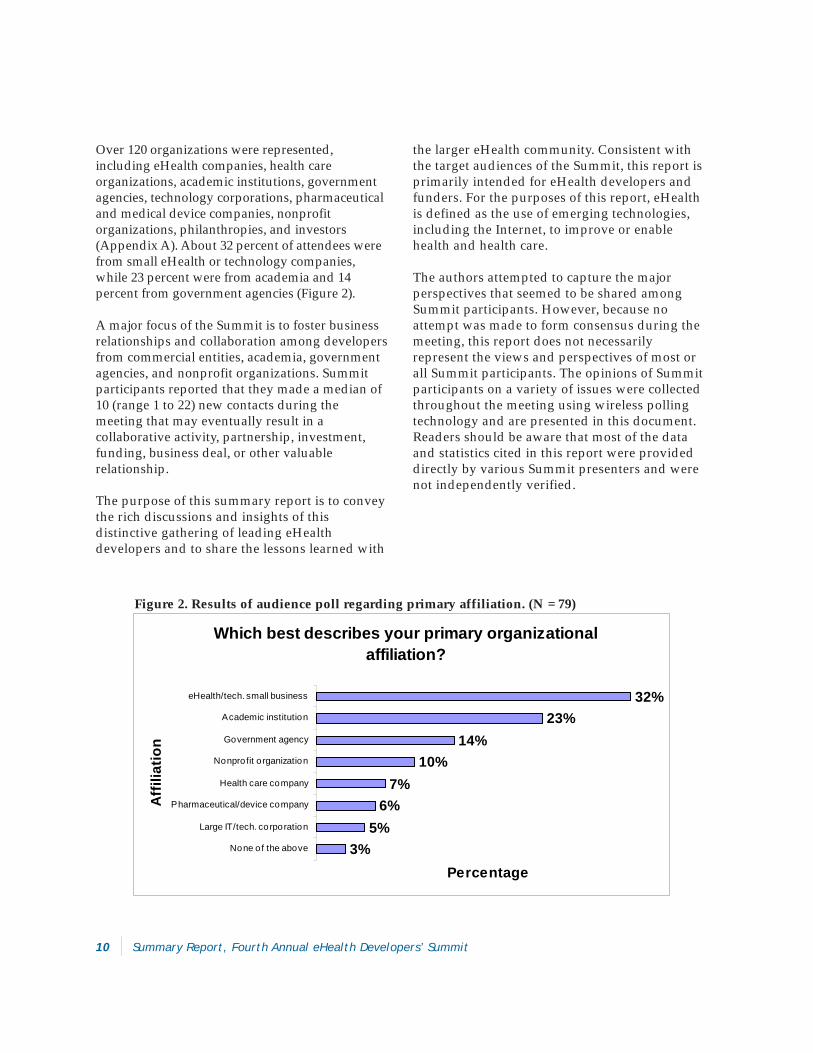
Figure 2. Results of audience poll regarding primary affiliation. (N = 79)
Over 120 organizations were represented,including eHealth companies, health careorganizations, academic institutions, governmentagencies, technology corporations, pharmaceuticaland medical device companies, nonprofitorganizations, philanthropies, and investors(Appendix A). About 32 percent of attendees werefrom small eHealth or technology companies,while 23 percent were from academia and 14percent from government agencies (Figure 2).
A major focus of the Summit is to foster businessrelationships and collaboration among developersfrom commercial entities, academia, governmentagencies, and nonprofit organizations. Summitparticipants reported that they made a median of10 (range 1 to 22) new contacts during themeeting that may eventually result in acollaborative activity, partnership, investment,funding, business deal, or other valuablerelationship.
The purpose of this summary report is to conveythe rich discussions and insights of thisdistinctive gathering of leading eHealthdevelopers and to share the lessons learned with
the larger eHealth community. Consistent withthe target audiences of the Summit, this report isprimarily intended for eHealth developers andfunders. For the purposes of this report, eHealthis defined as the use of emerging technologies,including the Internet, to improve or enablehealth and health care.
The authors attempted to capture the majorperspectives that seemed to be shared amongSummit participants. However, because noattempt was made to form consensus during themeeting, this report does not necessarilyrepresent the views and perspectives of most orall Summit participants. The opinions of Summitparticipants on a variety of issues were collectedthroughout the meeting using wireless pollingtechnology and are presented in this document.Readers should be aware that most of the dataand statistics cited in this report were provideddirectly by various Summit presenters and werenot independently verified.

eHealth: Striving for Critical Mass 11
The State of eHealth
Take-Home Messages
The year 2003 may have marked a turningpoint for eHealth in that a “critical mass” ofadopters seems to have crystallized. HealthIT has been popularized as prominent U.S.political leaders and independentorganizations have embraced nationaleHealth adoption for improving health careand public health systems.
Hospital and health plans have dramaticallyincreased their use of eHealth solutions inthe last few years. Some of those usingeHealth products for administrative supporthave seen substantial savings.
eHealth adoption in primary care settingslags behind its implementation in hospitalsand academic health centers. Summitparticipants cited lack of reimbursement andlack of tools that are integrated into theworkflow as the major barriers towidespread adoption of eHealth inprimary care.
Many consumers use the Web to look uphealth information for other people. This“zone of influence” reached more than 135million people even though “only” 82million consumers used the Internet forhealth information in 2003. Two-thirds ofcore users report using the Web beforeconsulting physicians or other resources.
Online CME is a rapid growth sector withnearly half of all physicians fulfilling theircontinuing education requirements online.
Pharmaceutical companies, both consumersand suppliers of eHealth, remain a majorsponsor of online content but are methodicalin responding to market forces and are veryselective in supporting eHealth projects.
The focus of many eHealth activities inpublic health revolves around enhancinghealth surveillance and communication.Initiatives by the Centers for Disease Controland Prevention illustrate the movementtoward adoption of standards and secureinteroperability across multiple jurisdictions.
Transforming Health Care
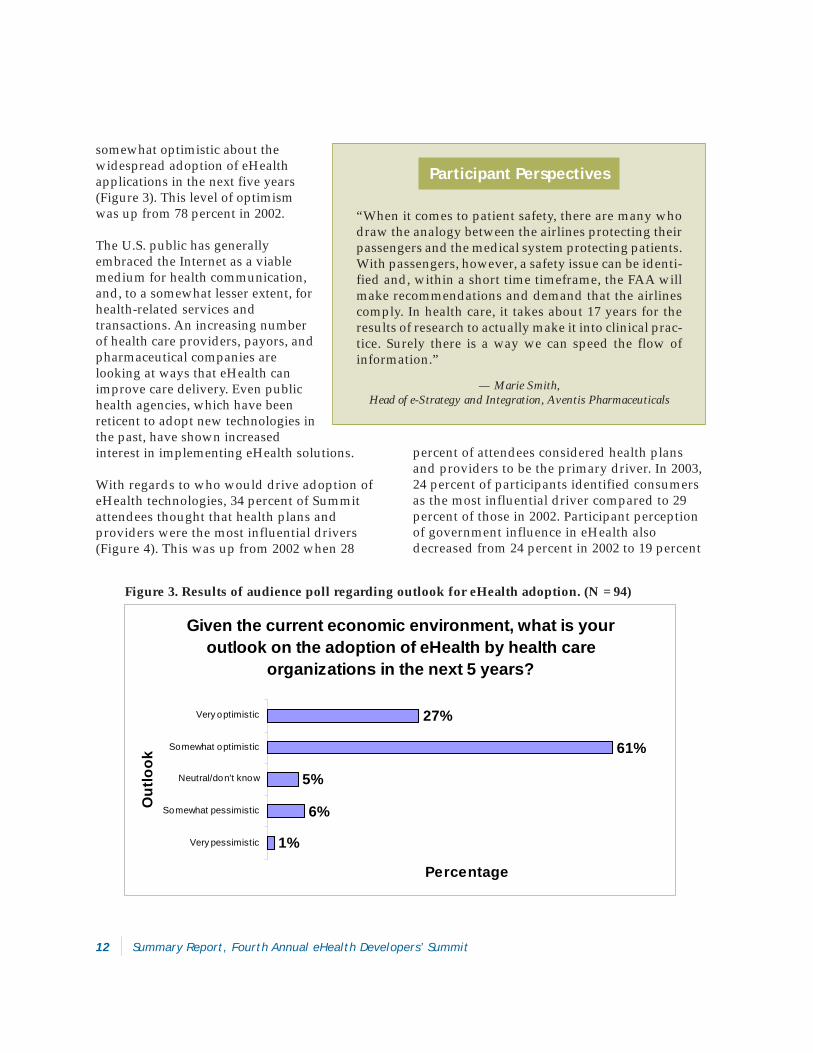
Health care in the United States has been slow toembrace the benefits of eHealth, but this appearsto be changing. Several Summit presentersbelieved that 2003 marked a turning point foreHealth in that a “critical mass” of interestedadopters has coalesced. Within the last year ortwo, several prominent U.S. political leaders andindependent organizations have embraced rapidnational adoption of eHealth as a means toenhance health care and public health systems,especially for improving quality of care andpatient safety. In 2003, 88 percent of Summitattendees stated they were optimistic or
12 Summary Report, Fourth Annual eHealth Developers’ Summit
somewhat optimistic about thewidespread adoption of eHealthapplications in the next five years(Figure 3). This level of optimismwas up from 78 percent in 2002.
The U.S. public has generallyembraced the Internet as a viablemedium for health communication,and, to a somewhat lesser extent, forhealth-related services andtransactions. An increasing numberof health care providers, payors, andpharmaceutical companies arelooking at ways that eHealth canimprove care delivery. Even publichealth agencies, which have beenreticent to adopt new technologies inthe past, have shown increasedinterest in implementing eHealth solutions.
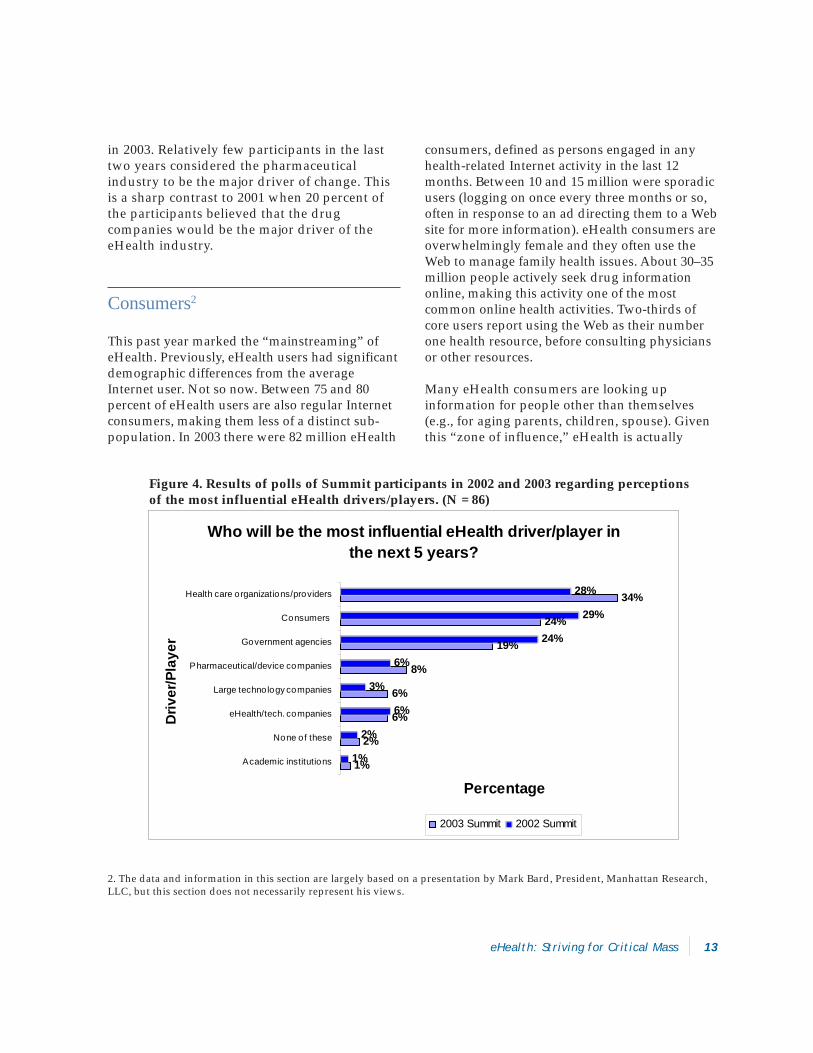
With regards to who would drive adoption ofeHealth technologies, 34 percent of Summitattendees thought that health plans andproviders were the most influential drivers(Figure 4). This was up from 2002 when 28
percent of attendees considered health plansand providers to be the primary driver. In 2003,24 percent of participants identified consumersas the most influential driver compared to 29percent of those in 2002. Participant perceptionof government influence in eHealth alsodecreased from 24 percent in 2002 to 19 percent
Given the current economic environment, what is your outlook on the adoption of eHealth by health care
organizations in the next 5 years?
1%
6%
5%
61%
27%
Very pessimistic
Somewhat pessimistic
Neutral/don't know
Somewhat optimistic
Very optimistic
Out
look
Percentage
Figure 3. Results of audience poll regarding outlook for eHealth adoption. (N = 94)
Participant Perspectives
“When it comes to patient safety, there are many whodraw the analogy between the airlines protecting theirpassengers and the medical system protecting patients.With passengers, however, a safety issue can be identi-fied and, within a short time timeframe, the FAA willmake recommendations and demand that the airlinescomply. In health care, it takes about 17 years for theresults of research to actually make it into clinical prac-tice. Surely there is a way we can speed the flow ofinformation.”
— Marie Smith,Head of e-Strategy and Integration, Aventis Pharmaceuticals
eHealth: Striving for Critical Mass 13
in 2003. Relatively few participants in the lasttwo years considered the pharmaceuticalindustry to be the major driver of change. Thisis a sharp contrast to 2001 when 20 percent ofthe participants believed that the drugcompanies would be the major driver of theeHealth industry.
Consumers2
This past year marked the “mainstreaming” ofeHealth. Previously, eHealth users had significantdemographic differences from the averageInternet user. Not so now. Between 75 and 80percent of eHealth users are also regular Internetconsumers, making them less of a distinct sub-population. In 2003 there were 82 million eHealth
consumers, defined as persons engaged in anyhealth-related Internet activity in the last 12months. Between 10 and 15 million were sporadicusers (logging on once every three months or so,often in response to an ad directing them to a Website for more information). eHealth consumers areoverwhelmingly female and they often use theWeb to manage family health issues. About 30–35million people actively seek drug informationonline, making this activity one of the mostcommon online health activities. Two-thirds ofcore users report using the Web as their numberone health resource, before consulting physiciansor other resources.
Many eHealth consumers are looking upinformation for people other than themselves(e.g., for aging parents, children, spouse). Giventhis “zone of influence,” eHealth is actually
Who will be the most influential eHealth driver/player in the next 5 years?
1%
2%
6%
6%
8%
19%
24%
34%
1%
2%
6%
3%
6%
24%
29%
28%
Academic institutions
None of these
eHealth/tech. companies
Large technology companies
Pharmaceutical/device companies
Government agencies
Consumers
Health care organizations/providers
Driv
er/P
laye
r
Percentage
2003 Summit 2002 Summit
Figure 4. Results of polls of Summit participants in 2002 and 2003 regarding perceptionsof the most influential eHealth drivers/players. (N = 86)
2. The data and information in this section are largely based on a presentation by Mark Bard, President, Manhattan Research,LLC, but this section does not necessarily represent his views.

14 Summary Report, Fourth Annual eHealth Developers’ Summit
touching far more than the 82 million directconsumers who are logging on. Once these otherbeneficiaries are included, eHealth appears to beimpacting more than 135 million people—upfrom 120 million in 2002.
Online patient education and marketing isespecially popular with pharmaceuticalcompanies that are shifting from a passive to amore active or “push” consumer educationstrategy. Applications that help consumerscompare prices of products and services, assistpatients in comparing treatment options,facilitate online transactions with health plans,and help patients to manage chronic conditionsare in high demand.
Developers should be aware that there may be amismatch of the user-purchaser paradigm formany consumer-oriented eHealth products.That is, although consumers may directlybenefit through improved convenience and carequality, they may not be willing to directly payfor access to these resources. A commonchallenge faced by many developers is todevelop a business model that demonstrates atangible benefit (e.g., reduced costs andutilization) to the direct payors of eHealthproducts, who are typically health careorganizations and employers.
Health Care Providers and Organizations3
Physicians still lag in their adoption of eHealthapplications, but acceptance is improving.Physicians typically use the Web to investigatedrug launches and learn more about the latestresearch or clinical guidelines. More than half ofproviders now use the Internet for patienteducation, typically referring patients to sitessuch as Medline and WebMD.
Although 41 percent of all physicians own aPDA, far fewer have integrated eHealth intoclinical practice. Of those who use their PDA inpractice, most use them to look up clinicalguidelines or drug information.
Almost half of all physicians use the Web forCME. Although the competition is becomingintense, developers interested in the health careprovider market might consider online CMEofferings. This product niche is experiencingrapid growth as online CME has become aconvenient and relatively low cost mechanism foraddressing licensure and certification require-ments. Other potential areas of opportunity foreHealth developers mentioned by somepresenters include advanced global healthapplications, e-detailing, and e-prescribing.
In recent years eHealth adoption among healthplans has increased dramatically. In the past thefocus was on simply presenting informationelectronically. More recently, however, manyhealth plans have enabled beneficiaries toconduct online transactions, such as choosingplan options, switching primary providers,scheduling appointments and—in some cases—participating in online clinical consultations. Useof the Internet for administrative functions, suchas claims transactions, formulary and providernetwork access, and reference support for callcenters, has provided substantial savings.eHealth adoption in primary care settings lagsbehind its implementation in hospitals andacademic health centers. This is especially truefor small private practices, which still largelyrely on paper-based medical charts, manualscheduling, and prescription pads. Summitparticipants cited lack of reimbursement andlack of tools that are integrated into theworkflow as the major obstacles to eHealthadoption in primary care settings (Figure 5).
3. The data and information in this section are largely based on a presentation by Mark Bard, President, Manhattan Research,LLC, but this section does not necessarily represent his views.

eHealth: Striving for Critical Mass 15
Pharmaceutical Companies4
Many pharmaceutical companies are consumersof eHealth products (e.g., drug discovery andmanufacturing support software) and developersand funders of products (e.g., online CME,disease management, and patient educationproducts).
Pharmaceutical companies are typicallymethodical in their decision-making and, thus,sometimes cautious to act. It is unusual to seethem diving into an eHealth project without along decision-making process. Large drugcompanies are often wary about eHealthinitiatives because they have been perceived inrecent years by some to have hidden agendas.Only 2 to 3 percent of the proposals they receiveactually get funded. And only projects thatdirectly support the goals of the company andtheir product line are selected.
An example of one company’s eHealth prioritiesincluded e-prescribing, evidence-basedmedicine, mobile health care, and diseasemanagement programs. Some pharmaceuticalcompanies, however, are unsure about themotivations behind the e-prescribing movement,including when Congress considered e-prescribing as part of the new Medicarelegislation. In the area of mobile health care,pharmaceutical companies are likely to besupportive of initiatives that give cliniciansaccess to medical outcome information at thepoint of care. Outcome-based diseasemanagement programs are also of interest.
One presenter provided three basic characteris-tics of eHealth projects that pharmaceuticalcompanies look for in funding decisions:
The project must promote patient safety,limit medical errors, or improve quality ofhealth care.
What is the single biggest barrier to eHealth adoption and implementation in primary health care settings?
2%
6%
8%
9%
37%
39%
Lack of provider technology skills
Other
Provider resistance to technology
Lack of time among clinicians
Lack of too ls integrated into clinical workflow
Lack of reimbursement
Bar
rier
Percentage
Figure 5. Results of audience poll regarding barriers to eHealth adoption in primary care
4. The data and information in this section are largely based on a presentation by Stephen Labkoff, Director of BusinessTechnology, Pfizer Global Pharmaceuticals, but this section does not necessarily represent his views.

16 Summary Report, Fourth Annual eHealth Developers’ Summit
The project must not limitprovider choices.
The project cannot bedeceptive and have hiddenmotives.
Some Summit participantsbelieved that pharmaceuticalcompanies tend to supporteHealth applications that arefocused on “wealthy well”populations. For example, thereare numerous online and offlineadvertising and educationalcampaigns to inform patientsabout prescription medicationsand to encourage brand namerequests.
Public Health5
The focus of this year’s discussion about publichealth applications of eHealth technologycentered on improving public health surveillanceand communication. Public health agencies arealready playing a key role in national defense,but many changes are needed to maximize theircontributions. Current needs include facilitatingautomated data reporting by clinical caresettings to public health agencies, and improvingdata exchange and interoperability among publichealth IT systems.
The recent anthrax bioterrorism incidentspropelled the need for technological enhancementof surveillance and communication systems.During this crisis, most communication had to beconducted over the phone because of technologyinteroperability issues. This overwhelmed theland-line phone system and many public health
workers resorted to cell phones. Some wirelessconversations were intercepted by reporters,resulting in nearly instantaneous broadcast ofdevelopments to the public, which may not havebeen sufficiently vetted.
Learning from past experience, the Centers forDisease Control and Prevention (CDC)established the new PHIN (Public HealthInformation Network). The purpose of PHIN isto promote the universal adoption of standardsthat increase technology interoperability. Ratherthan create new systems, the CDC hopes toleverage what already exists so that multiplejurisdictions (e.g., fire, law enforcement, privatelabs, and public health departments) can all sendand receive messages quickly and securely.Health Level Seven (HL7) messaging and otherdata standards are being promoted by PHIN.The HL7 reference information model, withextensions to support both routine public healthefforts and bioterrorism programs, has beenproposed. PHIN is incorporating Web services,
Working Models
Stephen Labkoff, Director of Business Technology at PfizerGlobal Pharmaceuticals, discussed their successful ven-ture with the State of Florida. A subsidiary, Pfizer HealthSolutions, contracted with the Florida state governmentto improve health outcomes with conditions such as dia-betes, congestive heart failure (CHF), asthma, and heartdisease. With this program, Pfizer reported reducing hos-pitalizations among CHF patients by 15–20 percent. Theircare management application saved the state an estimated$15.9 million in the first year, and they are on target foreven greater projected savings. Several other states areinquiring about using the system with their chronicallyill populations.
5. The data and information in this section are largely based on a presentation by Barry Rhodes, Associate Director ofPublic Health Systems Development, Centers for Disease Control and Prevention, but this section does not necessarilyrepresent his views.
eHealth: Striving for Critical Mass 17
service oriented architectures, and alphatransports. Several software initiatives havearisen from the PHIN, including the NationalElectronic Disease Surveillance System, thePHIN messaging system, and the Health AlertNetwork.
To further promote the adoption of standards,state governments are being provided with up toone billion dollars each, much of it for ITupgrades. To obtain funding, however, statesmust use PHIN standards and include HIPAAcompliant security measures, such as digitalsignatures and encryption technology.Validation, verification systems, management,and conformance testing to proveinteroperability, are also required.
18 Summary Report, Fourth Annual eHealth Developers’ Summit
Patient- and Provider-Based ElectronicHealth Records and Primary Care
Recent Web-based PHRs that interface withthe individual’s health plan and Web-basedEMRs that provide shared provider-patientaccess are blurring the boundaries of theseproducts, and additional hybrid EMR/PHRsystems are likely in the near future.
The personal health record (PHR) is premisedon allowing the consumer or patient tomaintain and update their health data. Thisapproach is consistent with recent trendstoward self-care, increased consumerresponsibility for health care, and the long-termshift toward a patient-centered health caresystem. Provider-based systems, such as theelectronic medical record (EMR), are predicatedon the health care provider having primaryresponsibility for maintenance and currency ofthe electronic record. EMRs typically focus onsupporting clinical practice and administrativeprocesses for providers and their organizations,whereas PHRs often promote greaterparticipation in and responsibility for healthcare recordkeeping among consumers. BothPHR and EMR products have great potential toimprove health care quality and reduce costsand medical errors. Summit presentersdescribed the pros and cons of several optionsfor patient- and provider-based electronichealth records.
Take-Home Messages
Attributes that should be considered inevaluating a personal health record (PHR)product include product/deviceportability, data collection methods,storage capacity, data security, and datatransfer capabilities.
Most Summit participants agreed that thebiggest barrier to user adoption of PHRs isthe lack of a clear value proposition.
Current electronic medical records (EMRs)are not yet sufficiently compelling forprimary care practices and do not meet theneeds of primary care physicians. In the realworld of primary care, reducing medicalerrors and providing better quality careoften are not sufficient reasons or incentivesto justify use of EMRs.
Four top issues that EMR developers shouldaddress for primary care practices areaffordability, compatibility, interoperability,and data stewardship.
Given the wide spectrum of eHealthtechnology options available in themarketplace, government regulations orrequirements supported by a consortium ofpayors will probably be needed to realizeinteroperability.

eHealth: Striving for Critical Mass 19
The Personal Health Record6
Few people use the same health care providerthroughout their lifetime. The need forportability of health records from provider toprovider may be an argument for individuals,rather than providers, to maintain their records.The recent HIPAA regulations support theconcept of consumers controlling access to theirpersonal information. Some PHR advocatesbelieve that the PHR concept promotes greaterhealth literacy and increased patient participa-tion in health care decisions. Payors and planadministrators could use Web-based PHRs toprovide a link to their administrative systemsand to promote better health decision makingamong beneficiaries. Similarly, employers couldemploy Web-based systems to provide access toutilization and decision support tools, facilitatecomparison shopping for services andproducts, and help employees manage healthbenefits, such as reimbursement or medicalsavings accounts.
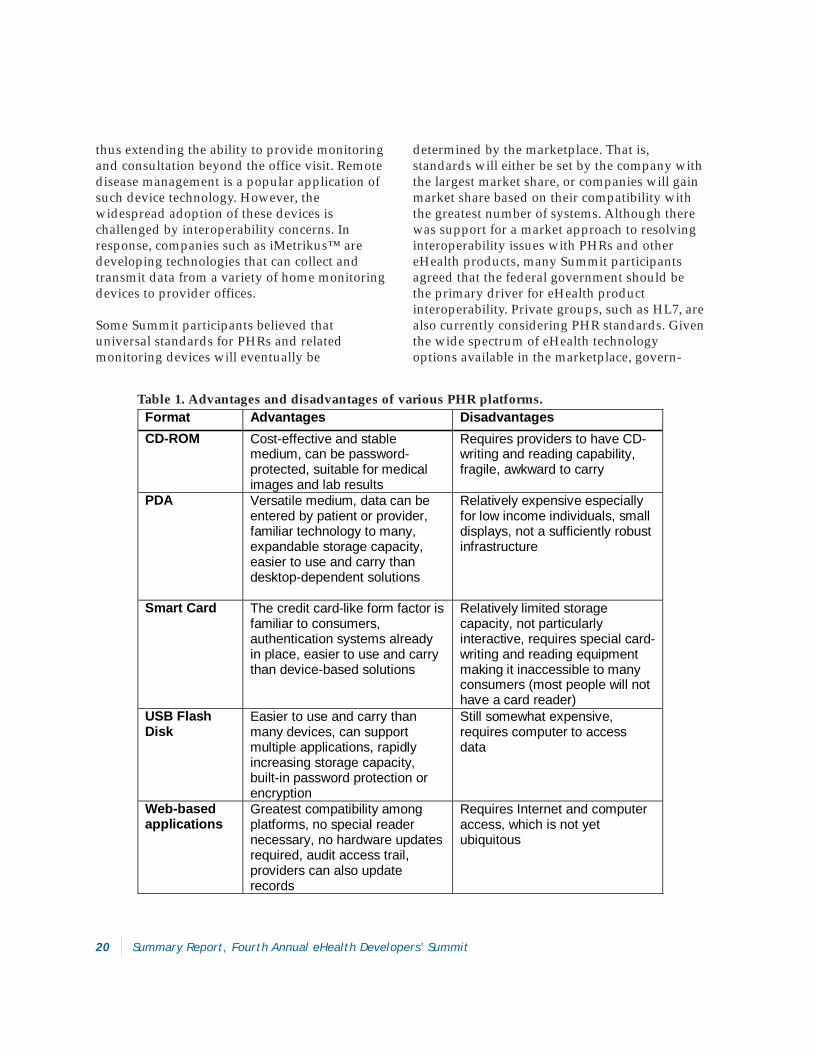
Current PHR products either use compact datastorage solutions or Web-based technology toimprove portability of the individual’s record.The advantages and disadvantages of severalcurrent PHR platforms, including CD-ROMs,PDAs, Smart Cards, USB Flash Disks, and Web-based applications, were explored at the Summit(Table 1).
Several issues to consider in evaluating a PHRproduct include:
Is the product/device easily portable?
How is health data entered and updated?
What is the storage capacity of the device?
How secure is the stored data?
How is the data transferred to providers?
Web-based PHR products may have anadvantage over other formats for robustfunctionality and interactivity. For example,WebMD’s Health Manager™ helps individualsidentify individual health risks and sendsinformation about adverse drug interactions orallergy issues, news articles regarding thepatient’s health concerns, and announcements ofnew relevant clinical trials.
Regardless of the form factor, PHR productshave generic disadvantages. By definition, theyrely on individuals, who vary greatly intechnical ability and level of engagement, tomaintain and update their record in a timelymanner. For example, the homeless and migrantpopulations often have complicated medicalconditions requiring extensive record keeping,but they typically have limited ability andresources for maintaining electronic records.There are also major concerns regarding dataintegrity and accuracy of patient-based systemsthat allow individuals to input or modify data.In the case of some non-Web-based products,there are also issues of hardware and softwarecompatibility. Additionally, more universalreliance upon PHRs would require building incontingencies for situations where people lose orforget to carry their device to a medicalappointment, or the device is inaccessible at thetime of a medical emergency.
The growing variety of PHR form factorsmentioned above illustrates the emergence ofapplications and devices that support thecollection, transfer, and storage of health datafrom homes and non-health care settings. Theseemerging devices are often used to transmit datafrom patients to providers in a secure manner,
6. The data and information in this section are largely based on presentations by Wendy Angst, CEO, Capmed Corporation;Phillip Marshall, Director of Products, WellMed/WebMD; and Matt Sanders, CEO, iMetrikus, but this section does notnecessarily represent their views.
20 Summary Report, Fourth Annual eHealth Developers’ Summit
thus extending the ability to provide monitoringand consultation beyond the office visit. Remotedisease management is a popular application ofsuch device technology. However, thewidespread adoption of these devices ischallenged by interoperability concerns. Inresponse, companies such as iMetrikus™ aredeveloping technologies that can collect andtransmit data from a variety of home monitoringdevices to provider offices.
Some Summit participants believed thatuniversal standards for PHRs and relatedmonitoring devices will eventually be
determined by the marketplace. That is,standards will either be set by the company withthe largest market share, or companies will gainmarket share based on their compatibility withthe greatest number of systems. Although therewas support for a market approach to resolvinginteroperability issues with PHRs and othereHealth products, many Summit participantsagreed that the federal government should bethe primary driver for eHealth productinteroperability. Private groups, such as HL7, arealso currently considering PHR standards. Giventhe wide spectrum of eHealth technologyoptions available in the marketplace, govern-
Format Advantages Disadvantages CD-ROM Cost-effective and stable
medium, can be password-protected, suitable for medical images and lab results
Requires providers to have CD-writing and reading capability, fragile, awkward to carry
PDA Versatile medium, data can be entered by patient or provider, familiar technology to many, expandable storage capacity, easier to use and carry than desktop-dependent solutions
Relatively expensive especially for low income individuals, small displays, not a sufficiently robust infrastructure
Smart Card The credit card-like form factor is familiar to consumers, authentication systems already in place, easier to use and carry than device-based solutions
Relatively limited storage capacity, not particularly interactive, requires special card-writing and reading equipment making it inaccessible to many consumers (most people will not have a card reader)
USB Flash Disk
Easier to use and carry than many devices, can support multiple applications, rapidly increasing storage capacity, built-in password protection or encryption
Still somewhat expensive, requires computer to access data
Web-based applications
Greatest compatibility among platforms, no special reader necessary, no hardware updates required, audit access trail, providers can also update records
Requires Internet and computer access, which is not yet ubiquitous
Table 1. Advantages and disadvantages of various PHR platforms.
eHealth: Striving for Critical Mass 21
ment regulations or requirements supported by aconsortium of payors will probably be neededbefore interoperability becomes reality.
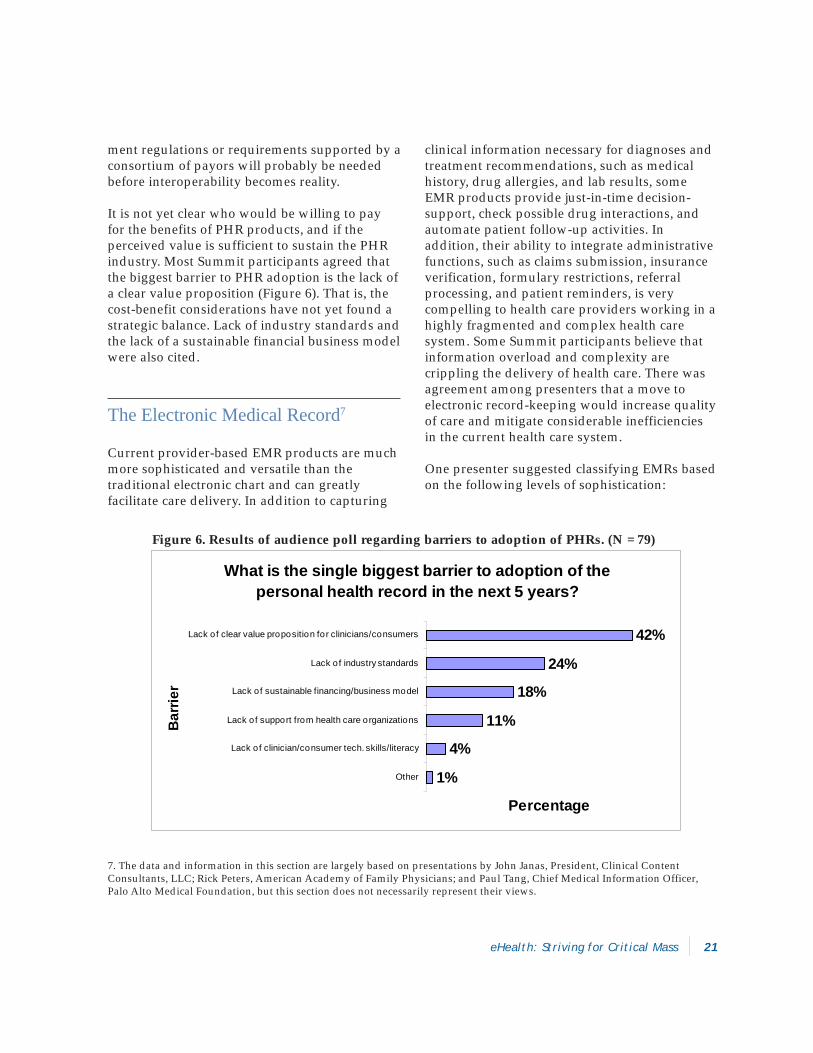
It is not yet clear who would be willing to payfor the benefits of PHR products, and if theperceived value is sufficient to sustain the PHRindustry. Most Summit participants agreed thatthe biggest barrier to PHR adoption is the lack ofa clear value proposition (Figure 6). That is, thecost-benefit considerations have not yet found astrategic balance. Lack of industry standards andthe lack of a sustainable financial business modelwere also cited.
The Electronic Medical Record7
Current provider-based EMR products are muchmore sophisticated and versatile than thetraditional electronic chart and can greatlyfacilitate care delivery. In addition to capturing
clinical information necessary for diagnoses andtreatment recommendations, such as medicalhistory, drug allergies, and lab results, someEMR products provide just-in-time decision-support, check possible drug interactions, andautomate patient follow-up activities. Inaddition, their ability to integrate administrativefunctions, such as claims submission, insuranceverification, formulary restrictions, referralprocessing, and patient reminders, is verycompelling to health care providers working in ahighly fragmented and complex health caresystem. Some Summit participants believe thatinformation overload and complexity arecrippling the delivery of health care. There wasagreement among presenters that a move toelectronic record-keeping would increase qualityof care and mitigate considerable inefficienciesin the current health care system.
One presenter suggested classifying EMRs basedon the following levels of sophistication:
What is the single biggest barrier to adoption of the personal health record in the next 5 years?
1%
4%
11%
18%
24%
42%
Other
Lack of clinician/consumer tech. skills/literacy
Lack of support from health care organizations
Lack of sustainable financing/business model
Lack of industry standards
Lack of clear value proposition for clinicians/consumers
Bar
rier
Percentage
Figure 6. Results of audience poll regarding barriers to adoption of PHRs. (N = 79)
7. The data and information in this section are largely based on presentations by John Janas, President, Clinical ContentConsultants, LLC; Rick Peters, American Academy of Family Physicians; and Paul Tang, Chief Medical Information Officer,Palo Alto Medical Foundation, but this section does not necessarily represent their views.

22 Summary Report, Fourth Annual eHealth Developers’ Summit
• First generation: Collector ofinformation
• Second generation: Documentor• Third generation: Helper• Fourth generation: Colleague• Fifth generation: Mentor
Most EMRs are currently at the“Helper” level, integrating clinicaldata with common administrativetasks, such as billing. Moreinteractive systems mayautomatically route prescriptions,lab tests, and other orders. Thesetypes of EMRs are typically usedby hospitals and managed careorganizations (MCOs), and areengineered to address the needs oflarger facilities and medical groupsrather than primary care practices.The most sophisticated versions,such as the “Mentor” generation,are not yet available. Summitpresenters cautioned that althoughadvanced features are alluring,successful EMR implementations often focus onproviding interactive support to clinicians, andautomating clerical functions while offering thelatest expert clinical support.
The benefits of EMR systems have not beensufficiently compelling for most primary carepractices to implement them. In the real world ofprimary care, reducing medical errors andproviding better quality care often are notsufficient reasons or incentives to justify theexpense of office EMRs. Such systems need todirectly reduce the cost of delivering care orgreatly improve processes by reducing time spenton paperwork, by increasing reimbursements, orby increasing the time physicians can spend withpatients. In addition, those who directly benefitfrom improved quality—patients and payors—are often not those who bear the direct expense ofinstalling and maintaining an EMR. To improvethe likelihood of administrator support for EMRadoption, it is helpful to show how an EMR can
reduce administrative costs and/or improveclinical work flow and efficiency. EMR productsthat begin to incorporate the capabilities of the“Colleague” generation will begin to offer a morecompelling return on investment.
Rick Peters of the American Academy of FamilyPractice presented a study which showed thatcurrent EMRs did not meet the needs of primarycare physicians. The study identified four topissues that developers should address:affordability, compatibility, interoperability, anddata stewardship. Most primary care physiciansfelt that about $173/month was a reasonableexpenditure for an EMR system. They expectedthat a system purchased for this amount wouldinclude authorization, e-prescribing, lab orders,hospital connectivity, patient instructions, patientaccess, and physician referrals as standardfeatures. In order to make a product purchasingdecision, physicians need to have an exit strategyin case a particular brand doesn’t fit their needs.
Working Models
Paul Tang, Chief Medical Officer at the Palo Alto Medi-cal Foundation (PMF), described a study that revealedthat patients usually missed 68 percent of the items thephysician felt were the focus or most important parts ofthe office visit. This problem led PMF to explore howphysicians and patients could share a medical record asa common point of reference. PMF Online presents eachpatient with a personal Web page with secure physician-patient messaging, links to PMF-approved educationalWeb sites, a list of the patient’s prescriptions with onlinerenewal, and access to lab results. Ninety percent of thephysicians who have used PMF Online are satisfied, with70 percent agreeing that it is more efficient than the tele-phone. And patients have not abused their electronicaccess to the physician. Paul noted that the ability ofphysicians and patients to use the same record has beena critical success factor. Online lab results and prescrip-tion renewals have been its most popular features.

eHealth: Striving for Critical Mass 23
Thus, interoperability and ease of data transfer toanother EMR product are necessary. Studyrespondents also placed scheduling ofappointments, handling prescription renewals,and processing new prescriptions, high on theirpriority feature list. Tracking clinic notes andcapturing charges were actually low priorities.
In many situations, patients have had to sign aspecific consent to initiate a cumbersomeauthentication process and release informationover HIPAA compliant systems. Given thepotentially large number of EMR and otheronline systems that require authentication (e.g.,in the banking industry), a national authentica-tion system would make such systems easier to
implement. Consumers would only have to gothrough the consent/authentication process onceto conduct subsequent secure and confidentialonline transactions.
Although current satisfaction levels with thesystem are very high, initial physician resistancewas an issue. The fact that the PMF systemallowed for better monitoring of care deliveryand problems with responsiveness of somephysicians became immediately obvious. Thesystem facilitates implementation of practicestandards, but there were physicians whoperceived this as somewhat intrusive. Use ofPMF Online is now required of physicians in themedical group.
Summit presenters believed thatmajor practice innovations maybe possible with widespreadEMR adoption. By facilitatingreferrals and sharing ofconsultation notes, there wouldbe enhanced communicationacross practice groups. Byproviding access to practice-wide and community/population data, decision-support rules could be based onlocal information and outcomesrather than just on general stateor national data. And moreconvenient and effective patient-provider communication couldresult in better diseasemanagement and preventionand treatment adherence.
Recent Web-based PHRs thatinterface with the individual’shealth plan and Web-basedEMRs that provide sharedprovider-patient access areblurring the boundaries ofthese products, and additionalhybrid EMR/PHR systems arelikely in the near future.
Lessons from the Field
“Patients are more confident in the physician’s treatmentrecommendations when they know the computer is
offering the physician reminders and decision support.”
One physician, who uses an EMR in the exam room, relatedthe story of a patient who was given a prescription and told tocome back in a month or so for follow up. The patient returnedand mentioned no problems with the medication, but her labresults showed no improvement. The physician turned to themonitor, and showed the patient her results and the EMR’s rec-ommendation that her dosage be increased. The medicationwas increased, but the patient’s bloodwork still showed no im-provement when she came back for a second follow-up. Thistime the EMR recommended another increase, but flashed awarning that the highest recommended dosage was reachedand that another medication should prescribed if this dosagedid not work. Upon seeing the warning, the patient said, “Oh,maybe I should start taking the prescription.” It turned out thatshe had heard warnings on television about possible liver dam-age with this medication. Since her brother had died of cirrho-sis, she was understandably cautious and was concerned thather physician might not know of, or be able to monitor the prob-lem well enough. After seeing how the EMR prompted the phy-sician, however, the patient’s confidence was restored and shebegan taking the medication.
24 Summary Report, Fourth Annual eHealth Developers’ Summit
eHealth Research and Dissemination
Take-Home Messages
Many behavioral eHealth products arerooted in social cognitive and other theories,and seek to improve user confidence (self-efficacy) in implementing behavioralchanges.
Research has demonstrated that a range ofpeople can successfully use many eHealthproducts. In some cases, users actually preferelectronic modes of communication overface-to-face interactions. Consumer andprovider satisfaction levels with somepatient-provider communication eHealthproducts have been very high.
Win-win arrangements between academicresearchers and commercial companies withcommon target audiences may help speeddissemination and infusion of researchfindings into marketable products.
Developers of eHealth products for diversegroups should consider the special healthrisks of these populations, and take steps toenhance the cultural appropriateness andusability of their products.
Developers should be aware that mostpeople of color live above the poverty level,and that they represent a growing marketopportunity. Seventy percent of Summitparticipants believed that there is asubstantial market in eHealth products forthe underserved.
eHealth Research8
The Summit featured several eHealth researchstudies that were selected by a review committeeamong dozens that were submitted in responseto a national call for papers.The five studiespresented were selected based on theiroriginality, overall quality, scientific rigor,methodology, design and analysis, potentialimpact on eHealth, and clarity of writing.Although each study examined the effectivenessof specific eHealth products, their resultsprovided insight into the impact of similarapplications.
Two of the studies focused around patienteducation and behavior change, one projectstudied the collection of data from low-incomeindividuals, and the two remaining studies
8. The data and information in this section are largely based on presentations by Beth Bock, Associate Professor, BrownMedical School; Susan Martin Gould, Research Associate, Colorado State University; Huong Nguyen, Assistant Professor,University of Washington; Lee Ritterband, Assistant Professor, University of Virginia; and Eric Zimmerman, SVP Marketing,RelayHealth, but this section does not necessarily represent their views.

eHealth: Striving for Critical Mass 25
examined the impact of applications thatenhanced patient-provider communications.
Huong Nguyen of the University of Washingtondeveloped a Web-based disease self-manage-ment program for persons with chronicobstructive pulmonary disorder (COPD), whichis the second leading cause of disability in theUnited States. Because of respiratory impair-ments, only a fraction of persons with COPD arewell enough to attend standard supportprograms. The intervention Web site offered fourmodules: an education component withstrategies for coping with breathing problems; ahome-based exercise program with self-monitoring, goal setting, and tailoredrecommendations; symptom and remotepulmonary function monitoring; and socialsupport through peer and professional email,bulletin boards, and chat rooms. The researchersused a device to monitor and report respiratoryfunction status over the Internet.
Sixteen patients were studied for a period ofthree months. Their frequency of use rangedfrom 12 to 102 times during the study period.Compared to baseline data collected beforeexposure to the intervention, there was asignificant change in several importantbehavioral health factors. For example, therewere large effect sizes in the intervention’sability to improve patient management ofbreathing and activities of daily living (e.g.,eating, bathing, and dressing).
Using the construct of social cognitive learning,there was also a large effect size in patients’ self-efficacy to manage their breathing problems.Moderate effect sizes were obtained in the areaof physical role functioning and enduranceexercise, while small effect sizes were noted forgeneral health perception, and perception ofboth online and offline support. The Web sitewas well received by the patients; 88 percentcited that the weekly support chats were helpfuland an equal proportion stated that the programimproved information access. Among those who
had participated in a face-to-face support groupin the past, 57 percent said they preferred theonline format.
Lee Ritterband of the University of Virginia presentedthe study of a multimedia education Web sitedesigned to address the problem of pediatricencopresis, which is the tendency to resist goingto the bathroom due to a traumatic or painfulbowel movement in the past, and often results inmessy and embarrassing accidents. Thissyndrome affects about 1.5 to 7.5 percent of thepediatric population. The Web-based interventionconsisted of modules for both children andparents, including content about anatomy,medication and treatment, behavioral educationabout proper defecation techniques, and exercisesto improve muscle strength and control.
Twenty-four families participated in thismultisite study. The program provided tailoredinformation drawing from a total of 27 modulesbased on an initial survey assessment. Theaverage age of each child was 8.5 years and mostof the children had been dealing with thisproblem for more than a year and a half. Thedesign involved a control trial with a pre- andpost-intervention assessment. Those in thetreatment group were given a computer in theirhome for a week so they could access the Website between physician visits. Those in thecontrol group received their usual andcustomary care with a primary care physician.
After a week’s exposure to the program, childrenin the treatment group showed marked—but notstatistically significant—improvement. Thetreatment patients improved from an initialaverage of six accidents a week to about oneevery two weeks. The control group began witheight accidents a week and did not exhibit anynotable change. Additionally, the treatmentgroup had a 150 percent increase in the numberof bowel movements that occurred in the toilet,whereas, only 16 percent of the control groupdemonstrated any progress in this area. Thetreatment group also demonstrated increased

26 Summary Report, Fourth Annual eHealth Developers’ Summit
bathroom use with and without parentalprompting. Both children and parents appearedto enjoy the program.
Susan Martin Gould of Colorado State Universitypresented the study of a bilingual multimediaprogram that simplified dietary assessment oflow income people applying for food assistance.The goal was to automate the procedure in orderto save staff time and to compare the computer-based program with face-to-face assessments.The application was designed to be easy tounderstand, use minimal text, not requirekeyboard use, and allow users to accuratelyestimate the size of food portions.
Eighty-two people were studied. Mostparticipants were low income persons; 16percent were Spanish speakers and 90 percentwere female. A two-period crossoverdesign with repeated measures wasused. The in-person and automatedassessments matched within 50calories of each other, with someexceptions. Fifty-four percent ofstudy participants indicated that theypreferred a computer assessmentover an in-person interview. Theautomated assessment wascompleted by users about twominutes more quickly than aninterview conducted by a person.
Beth Bock of Brown Medical Schoolpresented the study of a program tofacilitate smoking cessationcounseling by pharmacists. Onlyabout 2 percent of smokers whowant to quit will succeed on theirown. Success rates are much higherif smokers receive social supportand use nicotine replacementtherapies. Based on social cognitivetheory and stage of change models,this intervention was designed toassist pharmacists to implement the“five A’s” of smoking cessation
counseling recommended by the Public HealthService: Ask, Advise, Assess, Assist, andArrange follow-up. The program was designedfor use by persons with low income and/or lowliteracy. Available in kiosk or desktop PCformat, patients at the pharmacy complete asurvey regarding current smoking patterns,previous quit attempts, readiness to change,triggers and social support, and medicalcontraindications for nicotine replacementtherapy. The program then provides pre-written, tailored responses to the patient with arecommendation to talk to the pharmacist. Thepharmacist receives a summary printout withtalking points to facilitate a three- to five-minute counseling session with the patient.
A feasibility trial was conducted with 50smokers with an average age of 45 years. More
Lessons from the Field
“Delineate between your businessand academic activities.”
Edward Ratner described his experience starting up aneHealth business while also working at the Universityof Minnesota. His first piece of advice is to start with agood idea based on something you need for yourself.Then, find a graduate student who is smarter than youto help out. Because of university regulations, Ed wasvery careful to delineate between his business and hisacademic activities. He had to go to considerable ex-pense clarifying his intellectual property rights for theproduct he was developing through his small business.Completing this task early on is extremely importanteven though it cost him tens of thousands of dollars toestablish his company and protect his intellectual prop-erty. In addition, Ed suggested finding a customer tounderwrite R&D by getting them to pay for a versionmade specifically for them. Even if the product is cus-tomized for their needs, the product can be adapted tofit the developer’s vision and subsequently modifiedfor other customers.

eHealth: Striving for Critical Mass 27
than half had no previous computerexperience. Participants used thecomputer program, had a counselingsession with the pharmacist, receivedtheir nicotine replacement therapymedication, and scheduled a one-month follow-up visit. Ninety-fourpercent of participants set a quit dateduring their use of the program. Of the92 percent who returned for their one-month follow-up, 35 percent hadstopped smoking. All of the patientssaid that the program was easy to useand 74 percent said that it was helpfulin motivating them to quit. Thepharmacists rated the program ashighly successful.
Eric Zimmerman of RelayHealth presented astudy on using a secure messaging system toenhance patient-provider communication.Ninety percent of patient-provider interactionsoccur over the phone, typically a veryinefficient mode of communication. Twenty tosixty percent of patient-provider interactions donot require a visit. A group of payors and large,self-insured employers supported this study todetermine if secure messaging integrated withclinical workflow could cut costs andutilization, while maintaining patientsatisfaction. Designed around the metaphor of a“Webvisit,” the program enabled patients torequest medication renewals, view lab results,and ask questions.
A total of 282 primary care physicians wererecruited into the study. In all, 2345 patients whoused the secure messaging system and 3382controls, matched on demographics, healthcharacteristics, and Internet access, were studied.Of those who used the system, 45 percent hadfewer office visits and half appeared to take offless time from work to attend to medicalproblems. Ninety-five percent said the “Webvisit”was more convenient than traditional modes ofcommunication, and that they felt the quality ofcare received was comparable. Three out of four
physicians wanted to continue using the systemeven after the study was over; more than half saidthat for a non-urgent need, they would prefer a“Webvisit.” However, there was a substantial gapbetween what patients were willing to pay ($5–$7) versus what physicians wanted to be paid($31–$35) for an email communication. The studyalso showed that patient access to physicians viaemail did not result in increased utilization andhigher costs. In fact, utilization rates went downin the treatment group, and fears that physicianswould be flooded with patient emails wereunfounded.
eHealth Research into Practice
eHealth research studies can inform thedevelopment and deployment of eHealthinitiatives. Two major questions raised by theresearch presentations are:
How can research findings be quicklyintegrated into eHealth products andstrategies for the real world?
How can eHealth products better meet theneeds of diverse populations?
It typically takes about 17 years for academic
Participant Perspectives
“Academics are very accomplished at systematicallyevaluating what does and does not work, but theydo not necessarily understand customer need. Thebusiness world, however, is very attuned to the cus-tomer. We can create faster, more effective change ifwe bring these two worlds together.”
— David Ahern,National Program Director,
Health e-Technologies Initiative

28 Summary Report, Fourth Annual eHealth Developers’ Summit
research results to become commonclinical practice. This is clearly notacceptable for technology-relatedproducts. Many presenters indicated thatcollaboration with business was criticalto speeding up the diffusion process.
It was suggested that win-winarrangements between academicresearchers and commercial companieswith common target audiences mayhelp speed dissemination. Somepresenters recommended establishingan early partnership. For example, oneresearcher started by conducting one-on-one interviews with key commercialdecision-makers during the develop-ment phase. The possible disadvantage of thisapproach, however, is that it can lead to earlycustomization of the product and, thus, the endproduct may have a very narrow focus andbecome very labor intensive. A major incentivefor businesses to collaborate with academicresearchers is the credibility that academicinstitutions can bring to a relationship. Anothersuggestion was for researchers to attend tradeconferences, or to publish in non-academicjournals, such as those for health decision-makers or IT professionals, as a way to increasethe rate of diffusion.
There are other tensions that can arise inacademic-business partnerships. Academicresearch questions may differ from those thatare central to a business study. Somecommercial companies may not be as interestedin using validated instruments, or in rigoroussampling of the study population. Andresearchers will need to be cognizant ofpotential conflicts of interest in working withcommercial companies.
eHealth for Diverse Audiences9
The Summit convened discussions about howeHealth products can better address the needsand requirements of diverse populations,including the uninsured and underserved (e.g.,minorities, low-income populations, and peoplewith limited proficiency in English).
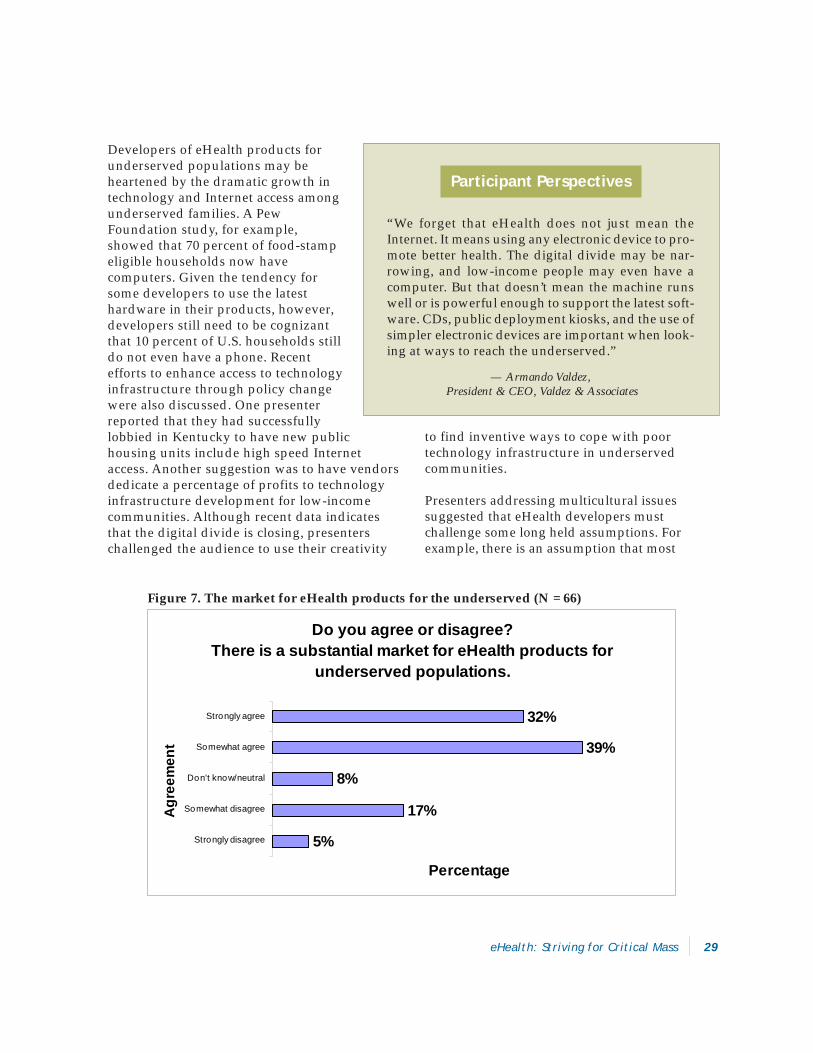
One central question is whether there is a viablemarket for products oriented to these groups. Inan audience poll, 71 percent of Summitparticipants believed that there is a substantialmarket for eHealth products for the underserved(Figure 7). In some cases, the end user will not bethe purchaser of the product, but their use maybe subsidized by payors and other entities (e.g.,government agencies and hospitals) that alreadypay significant sums of money to addressproblems that have been exacerbated from lackof access to care and other factors. The challengewill be to convince such payors to invest inproducts that may prevent expensive problemsat a later time horizon.
Participant Perspectives
“There is a natural tension that just does exist in thesebusiness-academic collaborations. For instance, thebusiness world wants to announce evaluation resultsimmediately and leverage them to commercial ad-vantage. Academics, however, prefer to wait for pub-lication in a peer-reviewed journal, which can take avery long time (12–18 months).”
— Eric Zimmerman,Senior Vice President of Marketing,
RelayHealth Corporation
9. The data and information in the underserved are largely based on presentations by Henrie Treadwell, Senior Social Scientist,National Center for Primary Care, Morehouse School of Medicine; Armando Valdez, President, Valdez and Associates; FaraiChideya, Special Editor, the Beehive, One Economy Corp., but this section does not necessarily represent their views.
eHealth: Striving for Critical Mass 29
Developers of eHealth products forunderserved populations may beheartened by the dramatic growth intechnology and Internet access amongunderserved families. A PewFoundation study, for example,showed that 70 percent of food-stampeligible households now havecomputers. Given the tendency forsome developers to use the latesthardware in their products, however,developers still need to be cognizantthat 10 percent of U.S. households stilldo not even have a phone. Recentefforts to enhance access to technologyinfrastructure through policy changewere also discussed. One presenterreported that they had successfullylobbied in Kentucky to have new publichousing units include high speed Internetaccess. Another suggestion was to have vendorsdedicate a percentage of profits to technologyinfrastructure development for low-incomecommunities. Although recent data indicatesthat the digital divide is closing, presenterschallenged the audience to use their creativity
to find inventive ways to cope with poortechnology infrastructure in underservedcommunities.
Presenters addressing multicultural issuessuggested that eHealth developers mustchallenge some long held assumptions. Forexample, there is an assumption that most
Participant Perspectives
“We forget that eHealth does not just mean theInternet. It means using any electronic device to pro-mote better health. The digital divide may be nar-rowing, and low-income people may even have acomputer. But that doesn’t mean the machine runswell or is powerful enough to support the latest soft-ware. CDs, public deployment kiosks, and the use ofsimpler electronic devices are important when look-ing at ways to reach the underserved.”
— Armando Valdez, President & CEO, Valdez & Associates
Do you agree or disagree? There is a substantial market for eHealth products for
underserved populations.
5%
17%
8%
39%
32%
Strongly disagree
Somewhat disagree
Don't know/neutral
Somewhat agree
Strongly agree
Agr
eem
ent
Percentage
Figure 7. The market for eHealth products for the underserved (N = 66)

30 Summary Report, Fourth Annual eHealth Developers’ Summit
people of color are poor. In fact, the number ofpeople of color who are not poor exceeds thosewho are—three-fourths of African Americans donot live in poverty. Four of five Latinos and 90percent of Asian Pacific Islanders are notimpoverished. Developers focusing onthe “minority market” in general maywish to remind potential corporatefunders about these data and marketopportunities.
Presenters agreed that eHealthdevelopers of products for diversegroups should consider theseguidelines to enhance culturalappropriateness and usability:
Make content available in multiplelanguages.
Target content for a sixth gradereading level or less.
Use sound and graphics(multimedia) instead of text, whilebeing cognizant of hardware andconnectivity requirements for theend user.
Focus on practical, action-oriented, and locally relevantcontent.
Display faces of people from awide range of ethnic backgrounds.
It was also suggested that productsgeared for specific cultural audiencesshould pay attention to health risksparticular to that population. Forexample, diabetes is the leading causeof death among Hispanics. AfricanAmericans are a third more likely todie of cancer than are their Caucasiancounterparts. Korean Americans havefive times the rate of stomach canceras the average population, andVietnamese American women have
the highest incidence of cervical cancer in thenation. These health disparities may present someinteresting eHealth market opportunities.
Working Models
James Rattleff and I-Hung Li of AR Designs describedtheir project in a depressed, rural area in Illinois wherethere are no gas lines and many people do not havecars. Even though there is no cell phone access in thiscommunity, with government funding, AR Designswas able to license technology from NASA that allowsthem to create a box that sits on top of a television anduses voice over IP (VoIP) technology to connect resi-dents with the one physician who serves the area. ARDesigns is hoping to apply this technology in othercommunities that lack basic infrastructure to extendhealth care services, such as monitoring EKGs.
Participant Perspectives
“At a commencement address, Ted Turner was askedto speak about the formula for his success. He saidthat you need to build something based on your vi-sion of how things will be 10–15 years from now.When we look at this in the context of ethnic minori-ties, we have to ask ourselves, will they be the minor-ity, and, will they be poor? Even if your goal is simplyto make money, reflecting on this question makes usthink about whether culturally sensitive programs arejust the issue of people of color, or those helping theunderserved. It may be that cultural competence isan issue that is relevant to all of us, not just those whoare currently in the mainstream.”
— Henrie Treadwell,Director of Kellogg Programs,
National Center for Primary Care

eHealth: Striving for Critical Mass 31
Sustaining and Commercializing eHealth
Take-Home Messages
Commercial eHealth developers should lookfor a funding source that is appropriate fortheir stage of business.
The value of product simplicity, ease ofimplementation, and convenience should notbe underestimated. Angel investors aretypically attracted to ideas that use existingtechnology in a new or creative way, arewell-defined, and have a proven marketneed. Those that mimic current proceduresand require minimal change on the part ofend users are preferred.
Developers need to be very clear about thebenefits of aligning with a large corporation.The allure of highly visible co-branding maynot be sufficient justification. It is importantto articulate specifically what the largecorporation contributes—beyond namerecognition—that will make a mutuallystrategic relationship.
Avoid products that require “cross-silo”cooperation among corporate units. Aproduct that “completes” a corporation’soffering is a particularly strong proposition.
Nearly half of Summit participants fromlarge corporations that received solicitationsfor funding or alliances from small eHealthbusinesses felt that the small business
wanted too much money or control given theproposed arrangement.
Forty-one percent of small businessrepresentatives at the Summit who hadsought funding or alliances with a largecorporation felt that the corporation movedtoo slowly and 33 percent believed that thecorporation was too risk averse.
Among developers at the Summit, the mostimportant attributes of a commerciallysuccessful eHealth product were demon-strated cost savings, user satisfaction, andpositive health status outcomes. Amongfunders and purchasers of eHealth products,demonstrated cost savings, positive healthoutcomes, and a low/reasonable price weremost important.
This year’s discussions about commercializingeHealth focused on small eHealth companies,angel investors, and relationships with largecorporations. There was minimal discussionabout venture capitalists as a source for eHealthfunding given that many of them are stillrecovering from failed eHealth ventures severalyears ago.
As a small business grows it typically goesthrough several stages of development, eachwith its own appropriate source of funding. Onepresenter summed up this evolution in thefollowing manner:

32 Summary Report, Fourth Annual eHealth Developers’ Summit
• Stage 0, “Passion”: Sweat funding• Stage 1, “Idea”: Sweat funding and friends
and family• Stage 2, “Product Prototype”: Angels• Stage 3, “Customers”: Venture capitalists• Stage 4, “Position”: Corporate funding
Commercial eHealth developers should look for afunding source that is appropriate for the stage ofthe business. For example, it probably would notbe appropriate to approach a large corporation forfunding if the product is not yet completed and hasnot yet cultivated a customer base. Corporatefunding is often pursued as a way to attain marketposition. Angel investors, on the other hand, wouldbe most appropriate when companies are past theidea stage and need capital to create a prototypeand prepare for launch.
In the early stages of product development,developers should consider the federal SmallBusiness Innovation Research (SBIR) program,which supports innovative technology R&D inareas of interest to the federal government. Muchof the SBIR funding for eHealth products comesfrom the NIH agencies. SBIR funding cansupport product development and evaluation ofthe product’s effectiveness, but it does notsupport the commercialization process. FromStage 2 forward, funding sources will be focusedon the return on investment. Developers willneed to provide investors with a requestedfunding amount and well-researched projectionsacross a timeline that is appropriate to theinvestor. Large corporations, for example, mayonly be willing to consider propositions in the $2million to $20 million range.
Angel Financing10
Angel investors are wealthy and financiallysophisticated individuals who provide seed and
start-up capital to high-risk, high-growth ventures.An angel investor typically enters the scene when aproduct idea is ready for prototyping and usuallyafter friends and family have invested funds. Angelinvestors are often successful entrepreneurs whoenjoy the start-up process. They are likely to bringmentoring and strategic contacts in addition tofinancial assistance. Motivations for angel investorsto become involved in a deal clearly include areturn on investment, but angel investors also tendto enjoy the excitement and learning of start-upcompanies. It is not uncommon for angel investorsto band together into networks and invest as agroup. Each one may contribute a modest amount(e.g., $25,000), but in aggregate they can offer asubstantial sum. Angel investors provide smallerscale investments than venture capitalists.
Jack Florio, Vice President of the San DiegoTech Coast Angels, described their process fordeal selection. Approximately one-third ofapplicants submitting a plan for funding willreceive an invitation to make a full presenta-tion to the group. Of these, half (one of sixapplicants) will be asked to host a site visit,and half of these (one of 12 applicants) willactually receive funding. The most significantcriteria for selection by an angel investor willlikely be the experience of the venture’smanagement team. Do the principals have abackground in the market? What other
Participant Perspectives
”Out of every 10 projects that are fundedby angel investors, 1 will tend to pay sig-nificant returns, 3 will do okay, and 6 willnot make it at all.”
— Jack Florio,Vice President, San Diego Tech Coast Angels
10. The data and information in this section are largely based on a presentation by Jack J. Florio, Vice President, San Diego TechCoast Angels, but this section does not necessarily represent his views.

eHealth: Striving for Critical Mass 33
enterprises have they been involved with, andhave they delivered before?
In terms of the product idea, the importance ofsimplicity, ease of implementation, andconvenience should not be underestimated.Angel investors are typically attracted to ideasthat use existing technology in a new or creativeway, are well-defined, and have a proven marketneed. Those that mimic current procedures andrequire minimal change on the part of end usersare preferred. A truly innovative concept mayonly be acceptable if there arefew individuals who need to beinvolved in its deployment. Betatesting data showing thatproduct end users will have onlyminimal problems implementingthe innovation are helpful.
In addition to the managementteam and the simplicity of an idea,angel investors are generallylooking for products with highgrowth potential, and asustainable competitive advantage.Funded projects tend to have well-articulated yet flexible strategieswith a valuation suitable for therisk profile. Angel investors alsotend to look for projects withmultiple exit strategies. An IPOoffering, acquisition by a largercompany, or spin off into a newventure are some of the acceptablepossibilities.
One common barrier for eHealthproducts is that the developermay have only identified onepossible beneficiary for theproduct. Successful venturestend to benefit more than onedepartment in the customer base(e.g., physicians and the billingdepartment). Although this maymean a more complicated sale, it
also tends to spread the likelihood of an internalchampion. Often the strongest proponent for thepurchase of a product comes from an unex-pected sector in the customer’s business.
Developers need to be able to demonstrate gainsthat can be monetized. eHealth developers areoften excited because of the good their productswill deliver. While this is good for society, theyhave neglected the business truth that someoneneeds to be able to translate that benefit intomoney saved or money earned.
Lessons from the Field
“Beta testing is essential!”
Stephen Porter, Instructor of Pediatrics in the HealthInformatics program of Children’s Hospital of Boston, wantedto develop an eHealth solution to collect accurate medica-tion history among asthmatic children presenting to the emer-gency room. His population included parents with limitedEnglish capabilities and low literacy rates. Initially he thoughtthat showing pictures would facilitate accurate identificationof medications. But the sorting functions were too difficultbecause there were far too many medications to present atonce. For example, albuterol alone has 30 generic versions.In addition, parents frequently focused on the color of theonscreen label matching the color on their child’s medicationbottle. Any color variation made their decision difficult.
Steve took an alternate approach after determining thatshowing pictures of medications were not as useful as ini-tially expected. They first asked parents to choose the de-livery method for the medication (e.g., inhaler, liquid,nebulizer, or pills). Instead of showing labels, they foundthat parents could anchor on the name of the drug, but cli-nicians and parents needed a common vocabulary for doses.For example, the word “puff” had different meanings todifferent people. The program had defined terms first andthen asked questions in order to get accurate and credibleanswers. Beta testing and learning to speak to the end userin language they understand was critical.

34 Summary Report, Fourth Annual eHealth Developers’ Summit
Investors typically favor products that havethe potential for add-ons. This characteris-tic allows a product to maximize itsexisting customer base and the product’sshelf life. Add-ons contribute to value asthey allow for the product to be used innew and different contexts, thus expandingversatility and the potential market. Inaddition, the more add-ons, the moredifficult it will be for a customer to switchto another brand or product.
Corporate Funding11
While many angel investors tend toprefer safer investments that representonly incremental changes from existingprocedures, large corporations mayinvest in a smaller company preciselybecause it offers a significant change orinnovation. A small, nimble company offers anopportunity to try new approaches and test thewaters. There is a paradox here, however, as thenimbleness of the smaller company is both anasset and a threat to the larger company. And thesheer size of the big corporation may welloverpower the smaller company’s vision.
Small business developers typically pursue a largecorporation after they already have a product witha customer base and are looking to improve amarket position. But a possible relationship mayhave several stages. One presenter suggested thatdevelopers “date before you marry.” Exchange ofmoney or partnership agreements are not requiredto nurture symbiosis. Potential corporate partnersmight be asked to serve on the advisory board orthey could be hired to consult on a project. Thiswill keep the product on the corporation’s radarscreen while giving the developer a taste of whatit’s like to work with them.
Before establishing relationships with largecorporations, developers should clearly outlinethe benefits to themselves. In some cases, co-branding with a large corporation may carrymore baggage than it’s worth. Don’t underesti-mate the value of a symbiotic relationship wherea product simply adds value or extends theutility of the larger organization’s product.
Lessons from the Field
“Gilt by association.”
According to Adee Feinstein, President ofClinication, Inc., some of the best advice he got wasto put together an advisory board. As a new com-pany, this not only afforded him great advice fromexperienced entrepreneurs, but he also benefitedfrom the “gilt by association” phenomenon. Now,when potential customers ask whom he works with,he can list the 15 impressive individuals and affili-ated companies that make up his Advisory Board.Instead of being the new company on the block withan untested track record, his company is perceivedas a credible player in eHealth.
Participant Perspectives
”If you’re going to travel in the wake of abig ship, you want to be in a PT boat, not arowboat.”
— Mark Leavitt,Vice President of Clinical Initiatives,
GE Medical Systems Information Technologies
11. The data and information in this section are largely based on presentations by Mark Blatt, Manager, Healthcare Strategies, Intel;Mark Leavitt, Vice President of Clinical Initiatives, GE Medical Systems Information Technologies; and Bill Crounse, GlobalHealthcare Industry Manager, Microsoft Corporation, but this section does not necessarily represent their views.
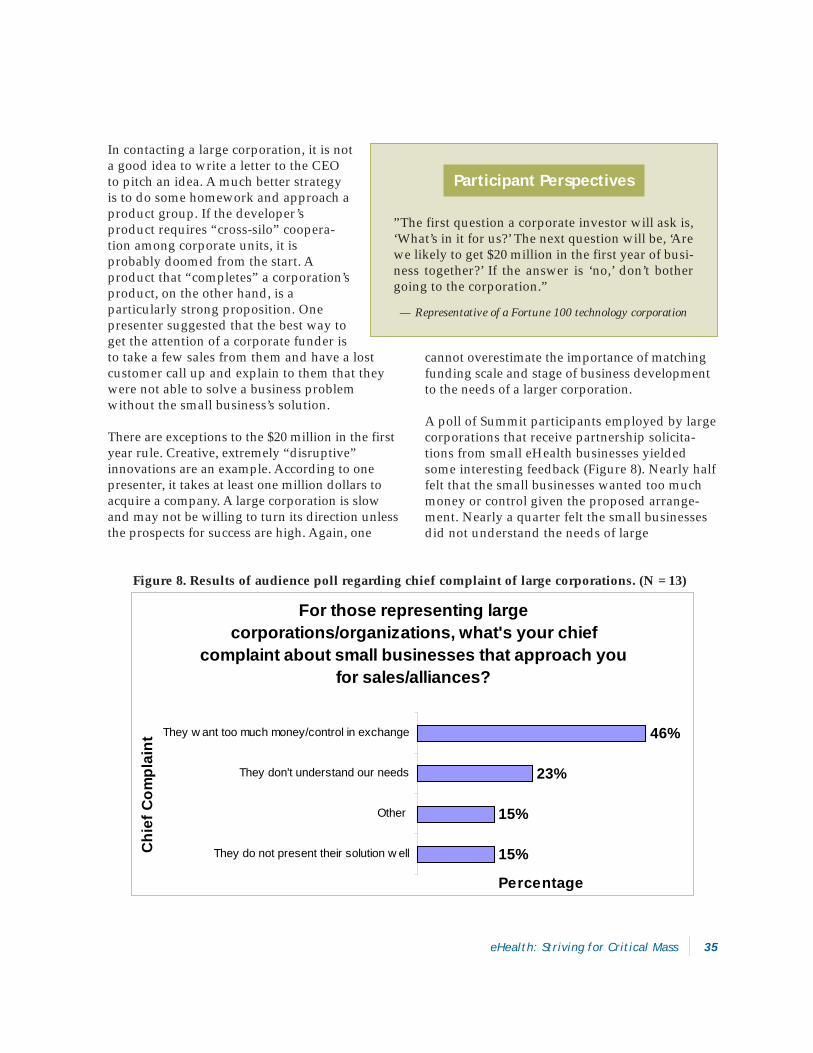
eHealth: Striving for Critical Mass 35
In contacting a large corporation, it is nota good idea to write a letter to the CEOto pitch an idea. A much better strategyis to do some homework and approach aproduct group. If the developer’sproduct requires “cross-silo” coopera-tion among corporate units, it isprobably doomed from the start. Aproduct that “completes” a corporation’sproduct, on the other hand, is aparticularly strong proposition. Onepresenter suggested that the best way toget the attention of a corporate funder isto take a few sales from them and have a lostcustomer call up and explain to them that theywere not able to solve a business problemwithout the small business’s solution.
There are exceptions to the $20 million in the firstyear rule. Creative, extremely “disruptive”innovations are an example. According to onepresenter, it takes at least one million dollars toacquire a company. A large corporation is slowand may not be willing to turn its direction unlessthe prospects for success are high. Again, one
cannot overestimate the importance of matchingfunding scale and stage of business developmentto the needs of a larger corporation.
A poll of Summit participants employed by largecorporations that receive partnership solicita-tions from small eHealth businesses yieldedsome interesting feedback (Figure 8). Nearly halffelt that the small businesses wanted too muchmoney or control given the proposed arrange-ment. Nearly a quarter felt the small businessesdid not understand the needs of large
Figure 8. Results of audience poll regarding chief complaint of large corporations. (N = 13)
For those representing large corporations/organizations, what's your chief
complaint about small businesses that approach you for sales/alliances?
15%
15%
23%
46%
They do not present their solution w ell
Other
They don't understand our needs
They w ant too much money/control in exchange
Chi
ef C
ompl
aint
Percentage
Participant Perspectives
”The first question a corporate investor will ask is,‘What’s in it for us?’ The next question will be, ‘Arewe likely to get $20 million in the first year of busi-ness together?’ If the answer is ‘no,’ don’t bothergoing to the corporation.”
— Representative of a Fortune 100 technology corporation
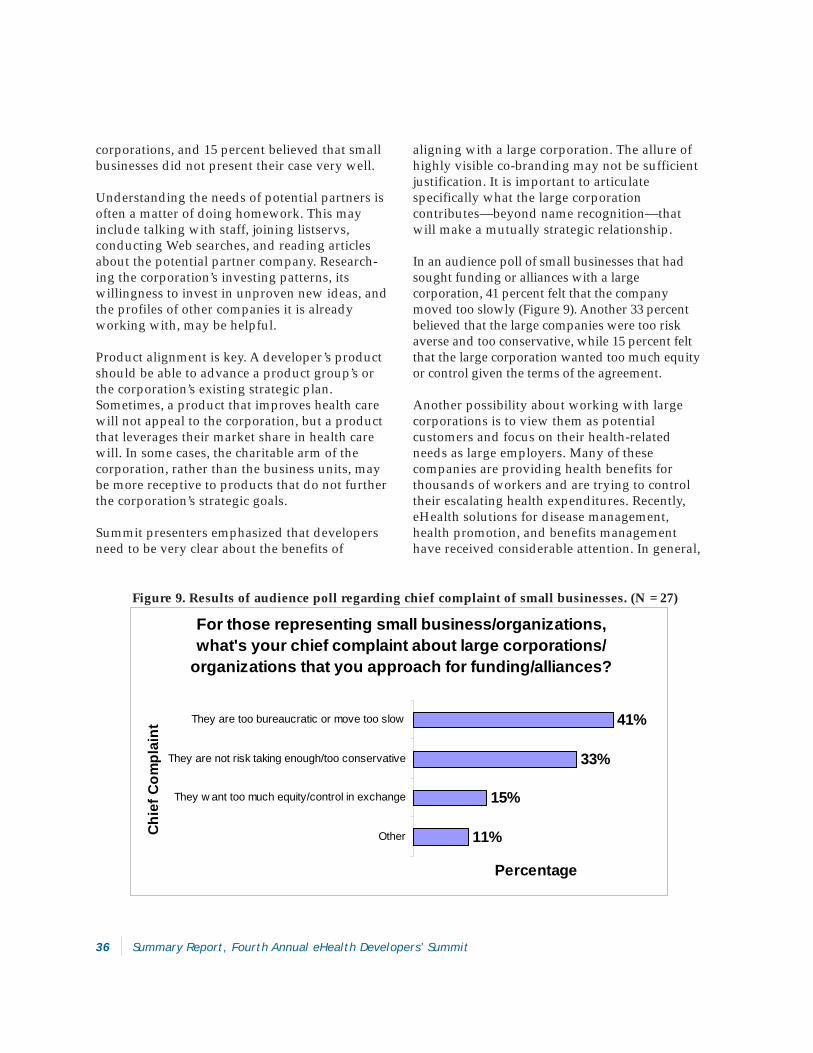
36 Summary Report, Fourth Annual eHealth Developers’ Summit
corporations, and 15 percent believed that smallbusinesses did not present their case very well.
Understanding the needs of potential partners isoften a matter of doing homework. This mayinclude talking with staff, joining listservs,conducting Web searches, and reading articlesabout the potential partner company. Research-ing the corporation’s investing patterns, itswillingness to invest in unproven new ideas, andthe profiles of other companies it is alreadyworking with, may be helpful.
Product alignment is key. A developer’s productshould be able to advance a product group’s orthe corporation’s existing strategic plan.Sometimes, a product that improves health carewill not appeal to the corporation, but a productthat leverages their market share in health carewill. In some cases, the charitable arm of thecorporation, rather than the business units, maybe more receptive to products that do not furtherthe corporation’s strategic goals.
Summit presenters emphasized that developersneed to be very clear about the benefits of
aligning with a large corporation. The allure ofhighly visible co-branding may not be sufficientjustification. It is important to articulatespecifically what the large corporationcontributes—beyond name recognition—thatwill make a mutually strategic relationship.
In an audience poll of small businesses that hadsought funding or alliances with a largecorporation, 41 percent felt that the companymoved too slowly (Figure 9). Another 33 percentbelieved that the large companies were too riskaverse and too conservative, while 15 percent feltthat the large corporation wanted too much equityor control given the terms of the agreement.
Another possibility about working with largecorporations is to view them as potentialcustomers and focus on their health-relatedneeds as large employers. Many of thesecompanies are providing health benefits forthousands of workers and are trying to controltheir escalating health expenditures. Recently,eHealth solutions for disease management,health promotion, and benefits managementhave received considerable attention. In general,
For those representing small business/organizations, what's your chief complaint about large corporations/
organizations that you approach for funding/alliances?
11%
15%
33%
41%
Other
They w ant too much equity/control in exchange
They are not risk taking enough/too conservative
They are too bureaucratic or move too slow
Chi
ef C
ompl
aint
Percentage
Figure 9. Results of audience poll regarding chief complaint of small businesses. (N = 27)
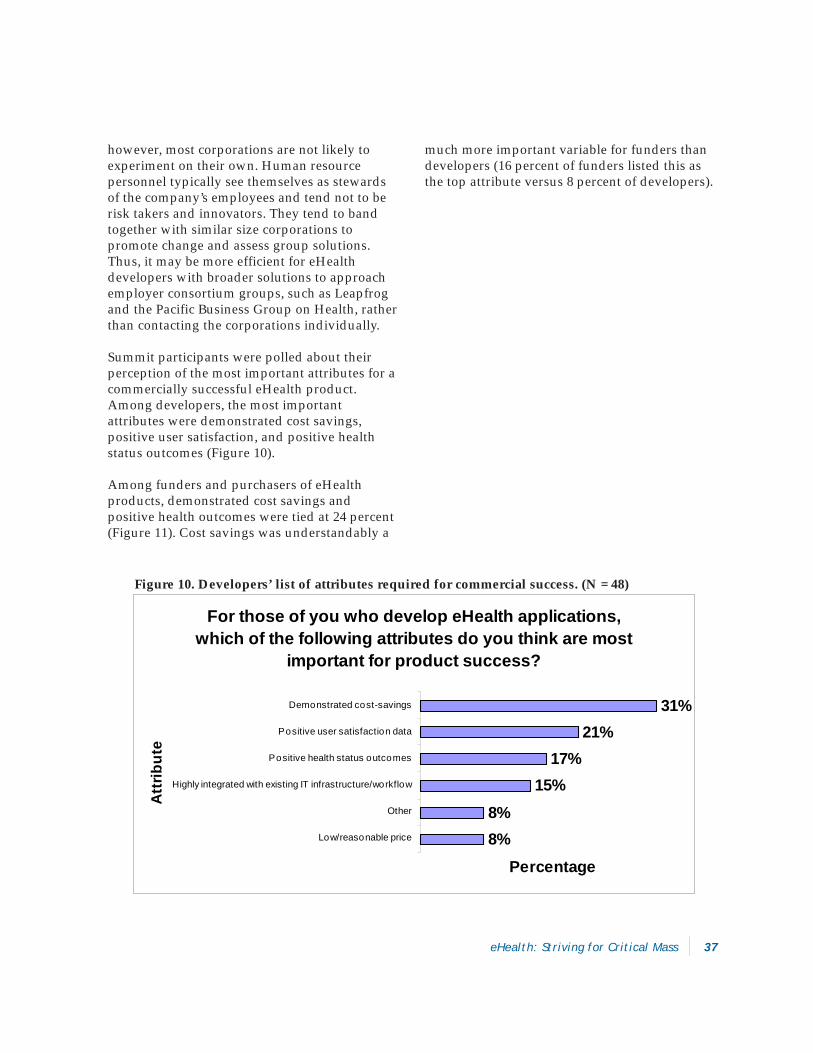
eHealth: Striving for Critical Mass 37
Figure 10. Developers’ list of attributes required for commercial success. (N = 48)
For those of you who develop eHealth applications, which of the following attributes do you think are most
important for product success?
8%8%
15%17%
21%31%
Low/reasonable price
Other
Highly integrated with existing IT infrastructure/workflow
Positive health status outcomes
Positive user satisfaction data
Demonstrated cost-savings
Att
ribut
e
Percentage
however, most corporations are not likely toexperiment on their own. Human resourcepersonnel typically see themselves as stewardsof the company’s employees and tend not to berisk takers and innovators. They tend to bandtogether with similar size corporations topromote change and assess group solutions.Thus, it may be more efficient for eHealthdevelopers with broader solutions to approachemployer consortium groups, such as Leapfrogand the Pacific Business Group on Health, ratherthan contacting the corporations individually.
Summit participants were polled about theirperception of the most important attributes for acommercially successful eHealth product.Among developers, the most importantattributes were demonstrated cost savings,positive user satisfaction, and positive healthstatus outcomes (Figure 10).
Among funders and purchasers of eHealthproducts, demonstrated cost savings andpositive health outcomes were tied at 24 percent(Figure 11). Cost savings was understandably a
much more important variable for funders thandevelopers (16 percent of funders listed this asthe top attribute versus 8 percent of developers).
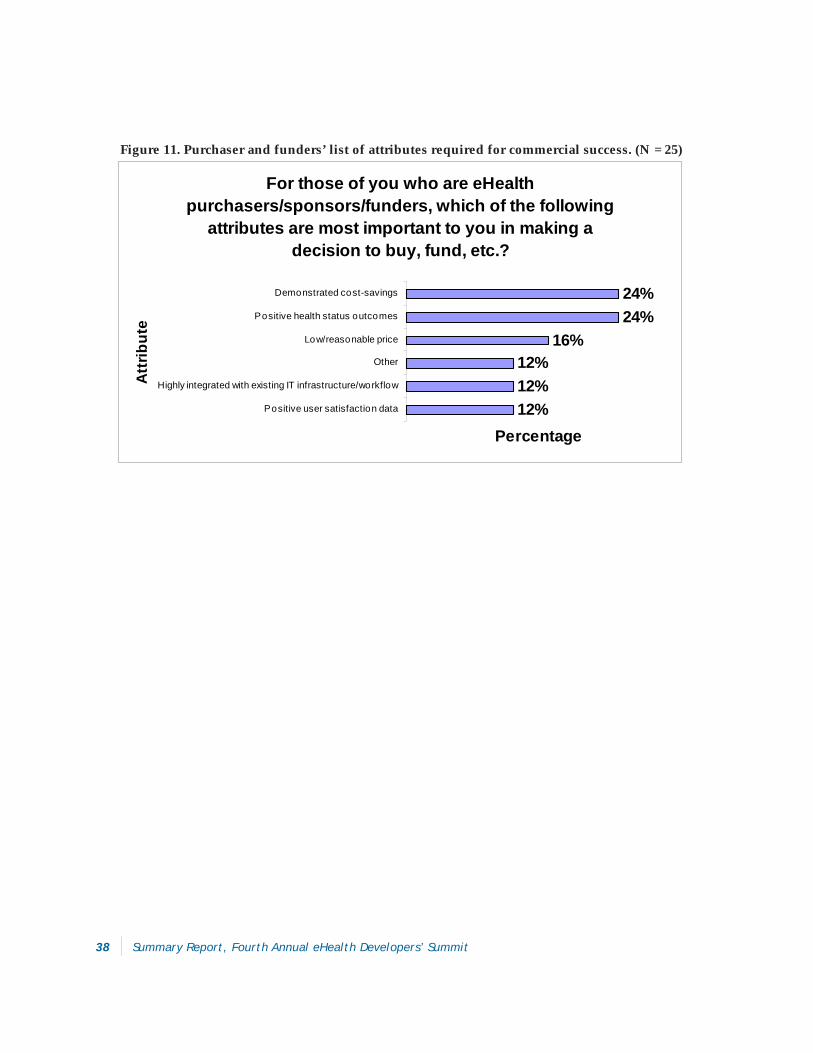
38 Summary Report, Fourth Annual eHealth Developers’ Summit
For those of you who are eHealth purchasers/sponsors/funders, which of the following
attributes are most important to you in making a decision to buy, fund, etc.?
12%12%12%
16%24%24%
Positive user satisfaction data
Highly integrated with existing IT infrastructure/workflow
Other
Low/reasonable price
Positive health status outcomes
Demonstrated cost-savings
Att
ribut
e
Percentage
Figure 11. Purchaser and funders’ list of attributes required for commercial success. (N = 25)
eHealth: Striving for Critical Mass 39
Conclusions
It appears that momentum for eHealth adoptionin health care is coalescing. In the past couple ofyears, calls by prominent political leaders andhealth organizations for national adoption ofeHealth solutions to improve quality of care andto reduce medical errors have been accompaniedby modest federal funding programs. Highlyvisible reports from organizations, such as theInstitute of Medicine, have elevated eHealth/IT asa cornerstone for a national strategy forenhancing quality of care and patient safety.Policymakers have realized that significantimprovements in these areas are not possiblewithout information systems that can accuratelydocument processes of care and outcomes.Without considerably more public and privatefunding and incentives for eHealth adoption,however, the benefits of eHealth will not likely berealized beyond large health care organizations.
In the midst of the “dot-com” era in the late1990s, some eHealth companies—many of whichno longer exist— were touted as instant marketmakers who would create new paradigms inhealth care. It is now clear that the massivehealth care system cannot be turned upsidedown overnight or even over the course of a fewyears. As more health care organizations adopteHealth technologies, they may realize theirinitial goals for the technology, such as improvedefficiencies of care and administrativestreamlining. But, they may also uncoveropportunities to totally revamp ineffective andinefficient care and business practices.Developers should recognize that few
purchasers of eHealth products do so with theintention of implementing entirely new processmodels. Rather, they are typically looking toimprove existing ones.
Large health care organizations, in some caseswith significant pressure and mandates fromlarge employer groups, are quickly adoptingeHealth solutions, as evidenced by recentannouncements of multiyear eHealth/ITinvestments by such organizations. Theperception among many Summit attendees thathealth plans and providers are the mostinfluential drivers of eHealth probably reflectsthe visible leadership of large health careorganizations. Although some organizations arestill on the sidelines, within a few years,investment in eHealth is likely to become aroutine expenditure. In some cases, suchtechnologies will be used as a productdifferentiator to attain and retain planbeneficiaries.
In the short-term, the challenge will bedeveloping and deploying eHealth products formedium and small group practices, whichdeliver the bulk of health care in the UnitedStates. This will not be an easy task as thesetypes of practices are subject to formidablebarriers to IT implementation in general. Summitparticipants cited lack of reimbursement andlack of tools that are integrated into theworkflow as the major obstacles to eHealthadoption in primary care settings. Medium andsmall group practices are less likely than larger

40 Summary Report, Fourth Annual eHealth Developers’ Summit
practices to have sufficient capital to invest in IT,especially when product ROI may be unclear orit is not likely to be realized for many years. Inaddition, they typically do not have access to ITspecialists who can provide independent adviceabout product options. As mentioned previously,issues around product affordability, compatibil-ity, interoperability, and data stewardship, arefront and center. Although selling eHealthproducts to medium and small group practicesmay often be difficult propositions, products thatadequately address the issues above would becompelling to this market segment.
Recent data documenting the widespread androutine use of eHealth resources by consumersconfirm that some eHealth applications havebecome mainstream tools. To date, visibleconsumer demand for health care organizationsand providers to offer eHealth products to theirpatients is not evident. This may be due to publicunfamiliarity with the role of eHealth in carequality or the lack of organized consumeradvocacy groups in this area. In terms of policyinfluence, trade organizations representingeHealth/IT vendors seem to have much morepolitical clout. The longstanding challenge facedby developers of consumer-oriented eHealthproducts is that the end user, who reaps most ofthe benefits, is usually not willing to pay forsuch use. Thus, more experimentation is neededto develop products and business models thatproduce a tangible benefit to both consumersand the usual direct purchasers of eHealthproducts, such as health care organizations andemployers.
Robust mechanisms for electronic health datacapture, storage, and access are paramount forsupport of clinical care and public healthfunctions. The PHR and the EMR are just two ofseveral health data management models. BothPHR and EMR products have great potential toimprove clinical care and public health, but theyalso have inherent disadvantages. Web-basedhybrid EMR/PHR systems are illustrative of themarket movement toward integrated informa-
tion systems that can truly support sharedresponsibility in health decision making.Developers should be cognizant that the likelybenefits of any eHealth product, no matter howobvious to the developer, may not be sufficientlycompelling to health professionals or consumerswho are faced with many daily competingdemands on their time and resources.
Another recent trend is the increasing variety ofpersonal health monitoring and communicationdevices being deployed outside traditionalhealth care settings. These devices have greatpotential to improve care quality and access, but,as with most emerging technologies, theiradoption and impact require overcomingconsumer and provider concerns aboutinteroperability, privacy and security, and otherissues. Proactive efforts to address theseconcerns, especially data standards, are essential.
eHealth applications related to public healthcontinue to focus primarily on diseasesurveillance and national security. eHealthproduct development in public health outside ofthese two areas has been sporadic even thoughsome emerging technologies present compellingopportunities for public health improvement.Most Summit participants believed that there is asubstantial market for eHealth products forunderserved populations. Adoption among thesegroups may not be as difficult as one mightinitially think since research has shown that arange of people can successfully use eHealthtechnology. Products that tackle healthdisparities may present growing eHealth marketopportunities if innovative business models tosupport their use can be crafted. Public andprivate funders of programs and services forunderserved populations should considercollaboration with eHealth developers togenerate new models and tools to addresslongstanding disparities that have been resistantto traditional approaches.
The long lag time from research and discovery tothe incorporation of study findings into product
eHealth: Striving for Critical Mass 41
design and implementation can be animpediment to product success. Collaborationbetween academic institutions and commercialcompanies can help shorten the lag time, butboth parties will need to proactively addresspotential conflicts of interest and intellectualproperty issues.
In the venture capital community, eHealth dealsare still rare; most developers are relying onfriends and family, angels, corporations, andgovernment programs, such as the SBIRprogram, to support product development. Incautious markets, product offerings that aresimple to use and implement, and that haveminimal barriers to widespread adoption arevery compelling opportunities for funders.
Several major needs and gaps were evident as aresult of discussions at the Summit:
Without considerably more public andprivate funding and incentives for eHealthadoption, the benefits of eHealth will notlikely be realized beyond large health careorganizations. Further national progress onthis front requires continued leadership andfunding.
More relevant and compelling eHealthproducts for medium and small group healthcare practices are needed.
Additional experimentation is needed todevelop products and business models thatproduce a tangible benefit to both consumersand the usual direct payors of eHealthproducts, such as health care organizationsand employers.
Proactive efforts are essential in addressinginteroperability, privacy and security, andother issues related to the increasing varietyof personal health monitoring andcommunication devices being deployedoutside traditional health care settings.
Public and private funders of programs andservices for underserved populations shouldconsider collaboration with eHealthdevelopers to generate new models and toolsto address longstanding disparities that havebeen resistant to traditional approaches.
One of the axioms of the eHealth Developers’Summit is that collaborative, transdisciplinary,and multi-sector approaches to productdevelopment and dissemination will result inhigher quality and more effective products. Atthe Summit, participants’ heterogeneousaffiliations and backgrounds help form abackdrop for creative idea generation andexchange. Trans- and multi-disciplinaryapproaches to eHealth product R&D anddissemination are essential as we build criticalmass in implementing these technologies.eHealth developers and funders who aresensitive to the complexity of the health care andpublic health systems—but who can alsochallenge assumptions in creative ways—willlikely find a successful niche.
42 Summary Report, Fourth Annual eHealth Developers’ Summit
Appendix A. Organizations Represented at the FourthAnnual eHealth Developers’ Summit
Health Solutions NetworkHSI Network LLCIDX Systems CorporationiHealth BeatiMetrikus, Inc.Infingo LLCIngham County Health DepartmentIntel CorporationInterMap SystemsInterMed AdvisorsISA GroupKaiser PermanenteLe Coup Digital Innovations, Inc.Leap of Faith Technologies, Inc.LifeMasters Supported SelfCare, Inc.LIFETECHniques, Inc.Management Partners GroupManhattan Research, LLCMarkle FoundationMcCarthy Medical MarketingMedical Directions, Inc.Medicos IncorporatedMedSeekMedSignalsMedStar HealthMicrosoftMorehouse School of MedicineMyDocOnline, Inc.National Cancer InstituteNational Institutes of HealthNational Library of MedicineNational Research Council CanadaNemours Center for Children’s Health MediaNorth Carolina Healthcare Information andCommunications AllianceNortheast HealthOffice of Disease Prevention and HealthPromotionOne EconomyOntoOO Inc.Oregon Center for Applied Science
ACORAlisos InstituteAmerican Academy of Family PhysiciansAmerican Legacy FoundationAnsya Enterprise SolutionsAR DesignsArkansas Children’s HospitalAventisBank of AmericaBaxter Patient Care SystemBeth Israel Deaconess Medical CenterBlue Cross Blue Shield of MassachusettsBock-to-the-Future Inc.Brigham and Women’s HospitalBrown Medical SchoolCalifornia Department of Health ServicesCalifornia HealthCare FoundationCapMed CorporationCenters for Disease Control and PreventionCereplex, Inc.CHI Systems, Inc.Children’s Hospital BostonCHRISTUS HealthClinical Content Consultants, LLCClinication, Inc.Collinge & AssociatesColorado State UniversityComputer Sciences CorporationConsumer Health InteractiveDeschutes Research, Inc.Diagnostic Archives CorporationEastman Kodak CompanyeHealth InternationalElite CareFitSense TechnologyFlorida State UniversityGE Medical Systems Information TechnologiesGeorgia Institute of TechnologyHarvard Medical SchoolHealth e-Technologies InitiativeHealth Hero Network Inc.
eHealth: Striving for Critical Mass 43
Palo Alto Medical FoundationPfizer Global PharmaceuticalsPro-Change Behavior Systems, Inc.Purdue Pharma, L.P.RelayHealthRipple Effects, Inc.Robert Wood Johnson FoundationRoyal Free and University College MedicalSchool at University College, LondonSAICSan Diego State UniversitySan Diego Tech Coast AngelsSiemens Corporate ResearchStanford School of MedicineSusan Levine AssociatesTech Coast AngelsTELUSThe Commonwealth FundThe CORE FoundationThe Launch PadThe NewSof GroupUniversity of Arkansas for Medical SciencesUniversity of California, San DiegoUniversity of California, San FranciscoUniversity of Florida College of MedicineUniversity of MarylandUniversity of Michigan Medical CenterUniversity of MinnesotaUniversity of Nebraska at OmahaUniversity of RochesterUniversity of the Sciences in PhiladelphiaUniversity of Virginia Health SystemUniversity of WashingtonUniversity of Texas MD Anderson Cancer CenterU.S. Department of Health and Human ServicesValdez & AssociatesValley Medical CenterVivoMetrics Inc.Voxiva, Inc.WebMD

44 Summary Report, Fourth Annual eHealth Developers’ Summit
Appendix B. Summit Awards
eHealth Impact Award Nominations Committee
Mark Bard, President, Manhattan Research, LLC
Cynthia Baur, Health Communication andeHealth Advisor, U.S. Department of Health andHuman Services
Steve Downs, Senior Program Officer, RobertWood Johnson Foundation
Thomas Hawkins, Director, eHealth Strategy,Harvard Pilgrim Health Care
Best eHealth Research Paper AwardThe annual Best eHealth Research Paper Award,consisting of a plaque and $1,000, recognizes thebest eHealth-related research conducted withinthe past year. The purpose of the Award is tohighlight and promote the application ofscientific research methods for identifyingeffective eHealth solutions. The Award issponsored by the Health e-TechnologiesInitiative, a national program of the RobertWood Johnson Foundation.
A national call for papers was issued for researchpapers reporting on work completed during theprevious one-year period. Research topicsincluded: 1) application effectiveness; 2) impacton health or health care outcomes; 3) cost-effectiveness, ROI, and sustainable businessmodels; 4) usability, application design, andspecial user populations; and 5) issues ofimportance to eHealth development, adoption,and dissemination.
A review panel selected the top five papers forpresentation at the Summit. Criteria for paper
Award for Application ExcellenceThe purpose of the Award for ApplicationExcellence is to recognize and promote highquality eHealth product development. In 2003,the Award was focused on product impact (the“eHealth Impact Award”). The Awardrecognized the eHealth product (e.g., software,hardware, or device) that has made thegreatest positive impact on health and/orhealth care. The Award, comprised of a plaqueand $1,000, was sponsored by MedicalDirections, Inc.
Nominations for the Award were solicited frompast Summit attendees and invitees and theNominations Committee. The five finalistsselected by the Nominations Committee werepresented to the Summit participants, whoselected the product that they believed had thegreatest impact based on the followingattributes:
The degree and nature of the application/product’s impact on health and/or health care.
The number and characteristics of peopleand/or organizations positively affected.
The nature of the health issue addressed.
The success and sustainability of theapplication/product either throughcommercial or nonprofit channels.
The co-winners of the eHealth Impact Awardwere eProcrates Rx and WebMD Health (tyingwith the same number of votes).

eHealth: Striving for Critical Mass 45
selection included: 1) quality, originality, andtimeliness of the study; 2) scientific rigor of thestudy design, analysis, and interpretation; 3)potential impact of study results to similarapplications and the eHealth sector; and 4)clarity of writing and organization of theabstract. In addition to these evaluation criteria,presenters were judged on the quality and clarityof their presentation, and their ability to answerquestions from the audience.
The five papers selected for presentation at theSummit were:
An Internet Intervention as Adjunctive Therapy forPediatric EncopresisLee M. Ritterband (1); Daniel J. Cox (1); Lynn S.Walker (2); Boris Kovatchev (1); Lela McKnight(3); Kushal Patel (2); Stephen Borowitz (1); JamesSutphen (1). (1) University of Virginia HealthSystem, (2) University of Vanderbilt, (3)University of Miami
Internet-based Support for Dyspnea Self-Management in Patients with COPDHuong Q. Nguyen (1); Virginia Carrieri-Kohlman (1); Sally H. Rankin (2); RobertSlaughter (3), Michael S. Stulbarg (4). (1)Department of Physiological Nursing, School ofNursing, University of California, San Francisco,(2) Department of Family Health Care Nursing,School of Nursing, University of California, SanFrancisco, (3) Office of Research, School ofNursing, University of California, San Francisco,(4) Department of Pulmonary and Critical CareMedicine, School of Medicine, University ofCalifornia, San Francisco
Computer Support for Pharmacy Based SmokingCessationBeth Bock (1); Frederick Bock (1); JamesChristian (2); Kyle Kelly (1). (1) BTTF Inc., (2)PHCC LP
Capturing Food Choice with a Bilingual InteractiveMultimedia Dietary Assessment Tool
Jennifer Anderson; Jamie Zoellner; Susan MartinGould; Department of Food Science & HumanNutrition, Colorado State University
The Webvisit Study: Impact of Online Doctor-PatientCommunication on Satisfaction and Cost of CareEric Zimmerman (1); Jeffrey Rideout (2);Laurence Baker (3). (1) RelayHealth Corporation,(2) Blue Shield of California Foundation, (3)Stanford University
The review panel awarded the “Best eHealthResearch Paper Award” for 2003 to twopresenters: Lee Ritterband, Assistant Professor,Behavioral Medicine, University of VirginiaHealth, and Eric Zimmerman, SVP Marketing,RelayHealth.
Review Panel for Best eHealth ResearchPaper Award David Ahern (Chair), Director, Health e-Technologies Initiative
James Hereford, Executive Director, MedicalInformatics, Group Health Cooperative of PugetSound
Kate Lorig, Director, Stanford Patient EducationResearch Center, Stanford University
Gary Kreps, Chief, Health Communications andInformatics Research Branch, National CancerInstitute
eHealth WIT (Working InnovationTechnology) Teams CompetitionThe eHealth WIT Teams Competition is held eachyear in conjunction with the Summit. The purposeof this competition is to promote collaborationand team problem solving among Summitparticipants from disparate backgrounds andorganizations. During the course of the meeting,small group teams develop an eHealth solution toa problem/opportunity in health or health care.

46 Summary Report, Fourth Annual eHealth Developers’ Summit
The facilitated teams tackled the issue through aseries of small group meetings, and presentedtheir solution to the entire audience and to ajudging panel on the final day of the Summit.
This year’s topic was improving the preventionand management of chronic health conditions.Teams were challenged to develop an eHealthsolution related to one or more chronic healthconditions that do one of the following:
Promote or support the adoption of healthybehaviors among a high risk group.
Support the clinical management of chronicconditions by enhancing patient-providercommunication or improving clinicaldecision making.
Support patient adherence to recommendedtherapies.
Each proposed concept was evaluated by thejudging panel based on innovation, feasibility,sustainability/commercial viability, andpotential impact on health or health care. Thewinning team received a $5,000 grant tosupport team follow-up activities to furtherdevelop the concept.
The judges selected the purple team for theirconcept, “Health Wizard,” as presented by PeterDunbar, Associate Professor, Anesthesiology,University of Washington. The team co-leaderswere Darrell Atkin, President, The Launch Pad;and Royer Cook, President, ISA Group. Theinnovative product envisioned by the winningteam would help address the health maintenanceneeds of the growing elderly population. Thisteam will provide an update on their progress atthe Summit in 2004.
WIT Teams Presentation Judges
Alan Creutz, Associate Partner, ManagementPartners GroupJay Kunin, San Diego Tech Coast Angels
“True Confession” AwardThis award is given to the person who provides themost useful description of what s/he learned fromdealing with a recent business, applicationdevelopment, or research problem. The audiencerecognized Robert Pretlow, President, eHealthInternational, for his presentation on the challengesof working with the medical establishment toaccept his eHealth research findings.
Summit “Renaissance Geek” AwardThis award is given to the Summit attendee whodemonstrates the broadest knowledge acrosstopics, such as art, history, sports, technology,and pop culture. Such knowledge in many areashelps in creative problem solving in eHealthdevelopment and dissemination. The 2004“Renaissance Geek” is Gretchen Oehme(Enterprise Systems Executive - Health CareServices, Information Technology, Blue CrossBlue Shield of Massachusetts), who correctlyanswered the highest number of trivia questionsduring the Summit.
eHealth Prediction 5K/2M FunRun/WalkThis award is given to the individuals who comeclosest to predicting their finishing time over a5K or a 2 mile course.
1st Place - David Ahern, Director, Health e-Technologies Initiative, 9 seconds differencebetween actual and predicted time2nd Place - Shannah Koss, Vice President, HealthSolutions, Voxiva, Inc., 47 seconds difference3rd Place - Houng Nguyen, Assistant Professor,University of Washington, 1 minute and 14seconds difference

Fourth Annual
eHealthDevelopers’Summit TM
www.ehealthinstitute.org