Embed Size (px)
Citation preview

Developing a Baseline – How we know we have achieved what we set out to achieve?
Angela [email protected]
Purpose of the sessionThis session will
• Who and what is PHE?
• Look at what baselines already exist
• Some key national figures
• Open the debate, what are we going to do then
But first, who are we….
2
Public Health EnglandExists to protect and improve the nation's health and wellbeing, and reduce health inequalities. It does this through advocacy, partnerships, world-class science, knowledge and intelligence, and the delivery of specialist public health services. PHE is an operationally autonomous executive agency of the Department of Health.
I am a member of the Thames Valley PHEC. There are three teams within the centre, Health Protection, Healthcare Public Health and Health Improvement. We all work together to achieve the above.
3
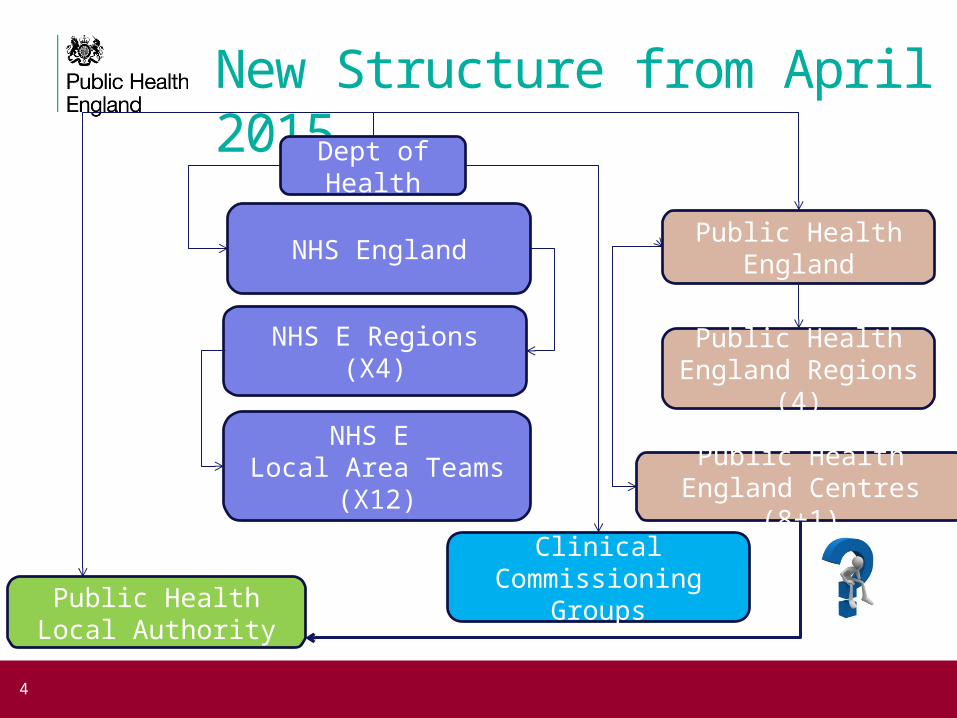
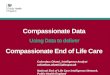
New Structure from April 2015
4
Dept of Health
Public HealthEnglandNHS England
NHS E Regions(X4)
NHS E Local Area Teams
(X12)
Clinical Commissioning
GroupsPublic HealthLocal Authority
Public HealthEngland Regions (4)
Public HealthEngland Centres (8+1)
So who does what….• Dept of Health, small unit that decides policy direction
• NHS England commissions Public Health Services such as bariatric surgery, all primary care services, screening and immunisation services either through areas teams or specialist commissioners
• CCG commission some tier 2 obesity services, in some areas, but also provide clinical direction to primary care
• Local Authorities – 2 types, unitary’s provide all the services in one area, also can influence planning, licensing etc, etc.
5
• Upper tier Local Authorities do not have all the levels of influence but provide public health services and a variety of partnerships dependant on the area
• All Local Authorities must have a JSNA, a Health and Wellbeing Strategy and a Health and Wellbeing board to monitor the strategy
• PHE provides evidence base, support and advice to Local Authorities and to NHS England on what works, cost effectiveness, ROI, translation of NICE Guidance.
6
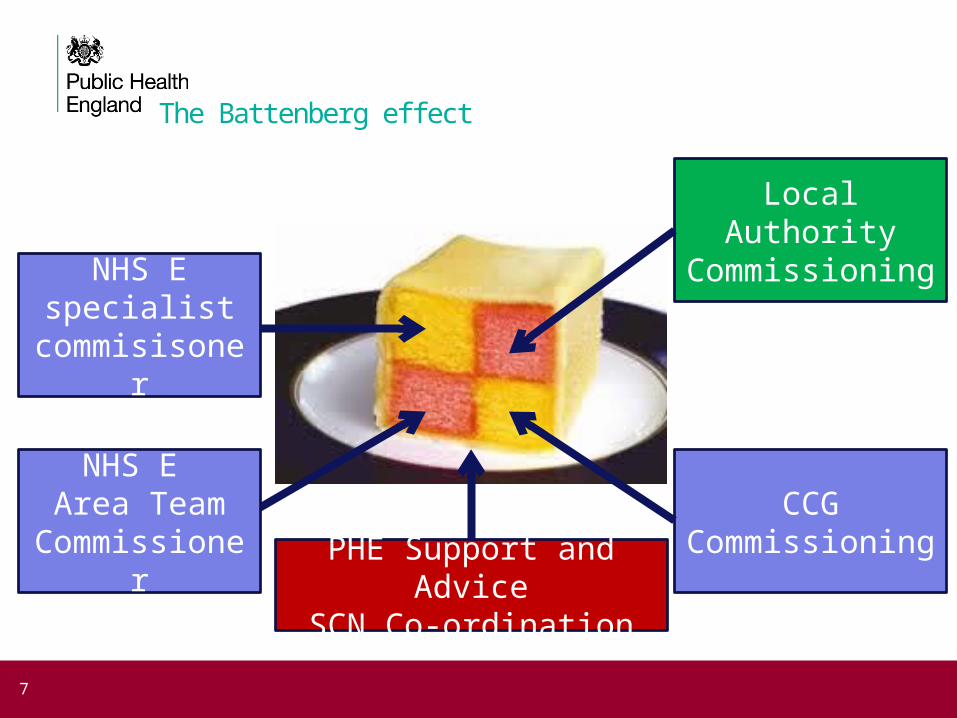
The Battenberg effect
7
NHS E Area Team
Commissioner
NHS E specialist
commisisoner
Local Authority Commissioning
PHE Support and AdviceSCN Co-ordination
CCG Commissioning
What is transition?
Transition is the purposeful, planned movement of adolescents and young
adults with chronic physical and medical conditions from child-centred
to adult-orientated health care systems.”
(Blum et al, 1993) 8
Existing Data and Information…• There are 13,486,095 people aged under 20 in
England, this equates to just over 23% of the total population
• 32 per 10,000 will have a life limiting condition which requires specialist input, that equates to 43,156.
• 577,931live in the Thames Valley (inc MK) that relates to just under 2000 children – approx 100 young people a year transition
9
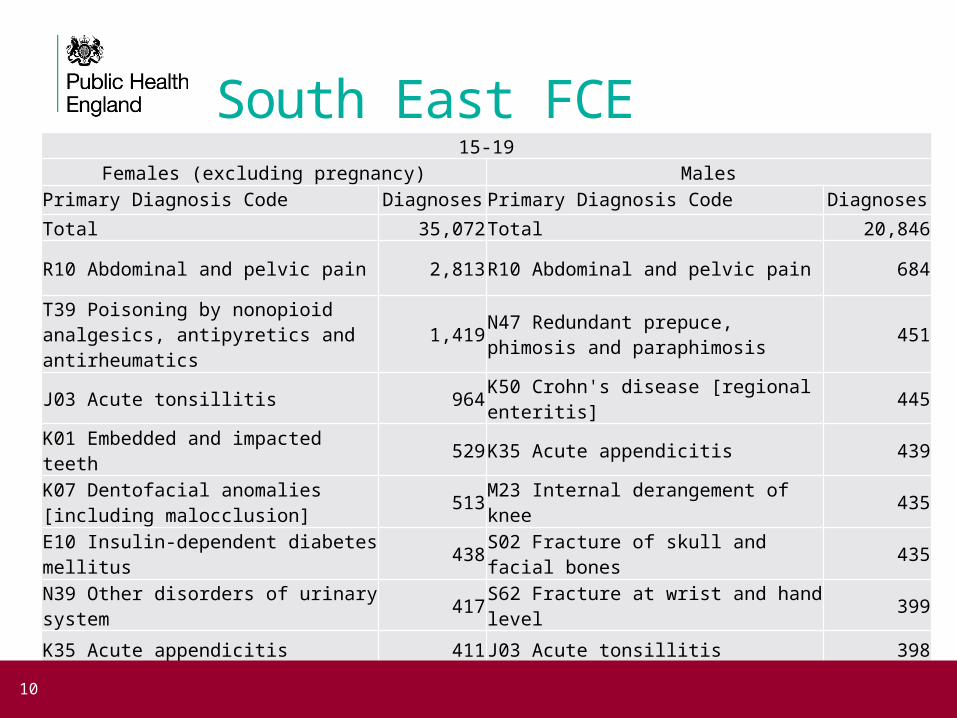
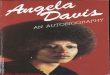
South East FCE15-19
Females (excluding pregnancy) MalesPrimary Diagnosis Code Diagnoses Primary Diagnosis Code Diagnoses
Total 35,072Total 20,846
R10 Abdominal and pelvic pain 2,813R10 Abdominal and pelvic pain 684
T39 Poisoning by nonopioid analgesics, antipyretics and antirheumatics
1,419N47 Redundant prepuce, phimosis and paraphimosis
451
J03 Acute tonsillitis 964K50 Crohn's disease [regional enteritis] 445
K01 Embedded and impacted teeth 529K35 Acute appendicitis 439
K07 Dentofacial anomalies [including malocclusion]
513M23 Internal derangement of knee 435
E10 Insulin-dependent diabetes mellitus 438S02 Fracture of skull and facial bones 435
N39 Other disorders of urinary system 417S62 Fracture at wrist and hand level 399
K35 Acute appendicitis 411J03 Acute tonsillitis 398
K50 Crohn's disease [regional enteritis] 396S82 Fracture of lower leg, including ankle
372
R51 Headache 394K01 Embedded and impacted teeth 350
10

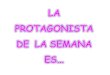
15 -19 year olds excluding pregnancy
11
R10 Abdominal and pelvic painT39 Poisoning by nonopioid analgesics, antipyretics and antirheumatics
J03 Acute tonsillitisK01 Embedded and impacted teeth
K07 Dentofacial anomalies [including malocclusion]K35 Acute appendicitis
K50 Crohn's disease [regional enteritis]E10 Insulin-dependent diabetes mellitus
M23 Internal derangement of kneeR51 Headache
S02 Fracture of skull and facial bonesR69 Unknown and unspecified causes of morbidity
T43 Poisoning by psychotropic drugs, not elsewhere classifiedS82 Fracture of lower leg, including ankle
R07 Pain in throat and chestN39 Other disorders of urinary system
N47 Redundant prepuce, phimosis and paraphimosisA09 Other gastroenteritis and colitis of infectious and unspecified origin
S62 Fracture at wrist and hand levelL05 Pilonidal cyst
2,000 1,500 1,000 500 - 500 1,000 1,500 2,000
b) 15-19 year olds excluding pregnancy related diagnoses for Females
Males
Females

Did not attend rates
12

13
Our Data?• Searched HES Data – outpatient Appointments
Only 23 Episodes recorded… so
• Inpatients episodes2009/10 – 3000 episodes recorded for Thames Valley
2012/13 – 6000+ episodes recorded but not clear why?
Self harm caused by Tobacco increased by 4 fold
• Data not good enough to use therefore
Problem 1
WE HAVE NO RLIABLE DATA
14
What can we do about it?• What data do you collect?
• What data is comparable across the system?
• What are the benchmarks for successful transition?• Reduced admissions
• Controlled condition
• Quantitative versus Qualitative
• Can we run a pilot in one speciality across the network?
• If so, what would work?
15
What and where are the transition points?
• Children's Acute/Secondary care to Adult Acute/Secondary Care
• Children's Social Services to Adult Social Services
• GP care – stays the same? But what is the role of parents?
• School versus Work/college/university
16
17 Angela Baker, Public Health Consultant in Health Improvement