Embed Size (px)
Citation preview

SPECIAL ARTICLE
Developing a Clinical Pathway for SomaticSymptom and Related Disorders in PediatricHospital SettingsPatricia Ibeziako, MD,a Khyati Brahmbhatt, MD,b,c Andrea Chapman, MD,d Claire De Souza, MD,e Lisa Giles, MD,f Shanti Gooden, MD,c Finza Latif, MD,g
Nasuh Malas, MD,h Lisa Namerow, MD,i Ruth Russell, MD,j Petra Steinbuchel, MD,c Maryland Pao, MD,k Sigita Plioplys, MDl
A B S T R A C T Somatic symptom and related disorders (SSRDs) are commonly encountered in pediatric hospitalsettings. There is, however, a lack of standardization of care across institutions for youth with thesedisorders. These patients are diagnostically and psychosocially complex, posing significantchallenges for medical and behavioral health care providers. SSRDs are associated with significanthealth care use, cost to families and hospitals, and risk for iatrogenic interventions and misseddiagnoses. With sponsorship from the American Academy of Child and Adolescent Psychiatry andinput from multidisciplinary stakeholders, we describe the first attempt to develop a clinical pathwayand standardize the care of patients with SSRDs in pediatric hospital settings by a working groupof pediatric consultation-liaison psychiatrists from multiple institutions across North America.The authors of the SSRD clinical pathway outline 5 key steps from admission to discharge andinclude practical, evidence-informed approaches to the assessment and management of childrenand adolescents who are medically hospitalized with SSRDs.
aDepartment of Psychiatry,
Boston Children’s Hospital and
Harvard Medical School, Boston,
Massachusetts; bLangley Porter
Psychiatric Institute,cDepartment of Psychiatry, Weill
Institute for Neurosciences, and
Benioff Children’s Hospital,
University of California, San
Francisco, San Francisco,
California; dDepartment of
Psychiatry, British Columbia
Children’s Hospital and The
University of British Columbia,
Vancouver, Canada; eDepartment
of Psychiatry, The Hospital for
Sick Children and University of
Toronto, Toronto, Canada;fDepartment of Psychiatry and
Behavioral Health, Primary
Children’s Hospital and School of
Medicine, The University of Utah,
Salt Lake City, Utah; gDepartment
of Psychiatry and Behavioral
Sciences, Children’s National
Medical Center and The George
Washington University,
Washington, District of Columbia;hDivision of Child and Adolescent
Psychiatry, Department of
Psychiatry, C.S. Mott Children’s
Hospital, University of Michigan
Hospital Systems, Ann Arbor,
Michigan; iDepartment of
Psychiatry, Connecticut Children’s
Medical Center and Institute of
Living, School of Medicine,
University of Connecticut,
Hartford, Connecticut;jDepartment of Psychiatry,
Montreal Children’s Hospital and
McGill University, Montreal,
Canada; kIntramural Research
Program, National Institute of
Mental Health, National Institutes
of Health, Bethesda, Maryland;
and lDepartment of Child and
Adolescent Psychiatry, Ann and
Robert H. Lurie Children’s
Hospital of Chicago and Feinberg
School of Medicine, Northwestern
University, Chicago, Illinois
www.hospitalpediatrics.orgDOI:https://doi.org/10.1542/hpeds.2018-0205Copyright © 2019 by the American Academy of Pediatrics
Address correspondence to Patricia Ibeziako, MD, Psychiatry Consultation Service, Boston Children’s Hospital, 300 Longwood Ave, Boston,MA 02115. E-mail: [email protected]
HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online, 2154-1671).
FINANCIAL DISCLOSURE: Dr Ibeziako receives grant support from the National Heart, Lung, Blood Institute; the other authors haveindicated they have no financial relationships relevant to this article to disclose.
FUNDING: Funded by the American Academy of Child and Adolescent Psychiatry Abramson Fund.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Drs Ibeziako, Brahmbatt, Chapman, De Souza, Giles, Gooden, Latif, Malas, Namerow, Russell, Steinbuchel, and Plioplys were involved inthe conceptualization and design of the study, developed the clinical pathway, drafted the initial manuscript, and critically reviewed andrevised the manuscript; Dr Pao was involved in the conceptualization and design of the study, provided feedback on the clinical pathway,and critically reviewed and revised the manuscript; and all authors approved the final manuscript as submitted.
HOSPITAL PEDIATRICS Volume 9, Issue 3, March 2019 1
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

Somatization is the process of experiencingemotions as physical symptoms (eg,headaches, stomachaches, nausea, andfatigue) and is a common experience ofchildren and adolescents.1 When thesesymptoms are persistent and markedlyinterfere with functioning, the group ofconditions known as somatic symptomand related disorders (SSRDs) should beconsidered. SSRDs are characterized byimpaired physical symptoms that areinfluenced by psychological factors,although they may co-occur with a medicalcondition, especially when symptoms aresevere enough to warrant hospitalization.2,3
SSRDs in youth are associated withdisruptions to education, peer relationships,recreation, and family functioning and cannegatively affect their developmentaltrajectory.2,4 Families affected by SSRDs tendto distrust emotional or psychologicalexplanations for the symptoms, fear that amedical condition has been missed, andperceive stigma about a mental healthdiagnosis.5 Often this results in late ordeclined mental health treatment,medication overreliance, and familyfrustration.6,7
Primary and specialty pediatric careservices, such as pediatric hospital medicine,neurology, and gastroenterology, are oftenextensively used by children with SSRDs.3,8–11
Children with SSRDs account for 10% to 15%of medical visits in primary care,12,13 andsomatization is the second leading reason forconsultation requests received by child andadolescent psychiatrists in pediatrichospitals.14 Health care professionals oftenfeel unprepared to care for these patientsbecause of insufficient training in thediagnostic and management processes,15 lackof common terminology for the illnessphenomenon, absence of standard treatmentguidelines, and time-consuming nature oftheir care.16 Literature reveals that themanagement of youth with SSRDs isassociated with a high level of provider andfamily frustration and poor treatmentoutcomes despite the often extensive level ofresources used.12,17,18 Other related challengesinclude a heightened risk of iatrogenic injury,prolonged medical hospitalization, diagnosticerrors (involving both medical and mentalhealth diagnoses), increased morbidity, high
health care costs, and high levels of economicand emotional burden to families.
Given these challenges, and the lack ofstandardization of care in the pediatricSSRD population, there is a clear need todevelop evidence-informed, integrated,SSRD care models through the use of aclinical pathway (CP). CPs bridge the gapbetween research findings and dailypractice19 by bringing available evidence tohealth care professionals and outliningessential steps in patient care that can beadapted to the local context.19–24 With CPs,providers aim to reduce practice variationsand improve the efficiency and effectivenessof health care.25 Multiple studies reveal thatCPs improve clinical outcomes26–28 whiledecreasing length of stay and hospitalcosts.29 The use of CPs is increasingworldwide, and they are commonly used inNorth America for medical conditions suchas asthma and diabetes.25–28 There is,however, a lack of published CPs for themanagement of psychiatric disorders inpediatric hospital settings.
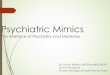
Waynik et al30 describe a model fordeveloping and implementing CPs (Fig 1).Factors that are used to predict thesuccessful development and implementationof CPs include high disease prevalenceand high practice variability,25 which areboth prominent features of pediatricSSRDs.14–16 Although there is some evidenceabout psychotherapeutic interventionswhen addressing SSRD in primary care,7
there are limited published data on bestpractices for SSRD management inpediatric hospitals. In the current article,we describe the process and contentof a CP developed by an expert group ofpediatric consultation-liaison psychiatristsin the United States and Canada to guidethe care of patients with SSRDs in pediatrichospital settings.
METHODS
The SSRD working group used astandardized model for creating a CP.30 Eachof the steps is described below:
1. Identifying the need for a CP: Asdescribed previously, SSRDs areprevalent in the pediatric population,have high medical and psychiatric
comorbidities, and result in considerablehealth care use, with providers havinglittle guidance in or coordination of thecare of patients with SSRDs in pediatrichospitals. A CP was adopted tostandardize fundamental elements ofcare and facilitate best practices.
2. Assembling a team of experts: The SSRDworking group consisted of 12 pediatricconsultation-liaison psychiatrists whohave an established expertise, clinicalexperience, and interest in SSRDevaluation and management in pediatrichospitals. These psychiatrists practice ina wide variety of settings and contextsfrom 8 US states and 3 Canadianprovinces. A pediatrician with expertisein CP development provided guidanceand feedback during the process.
3. Compiling and reviewing existingresearch: The literature on SSRD isevolving. The current evidence base wasreviewed by working group membersand informed the pathway development.Local SSRD pathways and protocols from7 institutions of the participatingworking group members were reviewedto identify common and essentialelements and themes as well asimportant lessons learned fromdeveloping and implementing localpathways, which also informed thecurrent CP.
4. Developing the CP:a. Initial draft: The SSRD working group
held monthly teleconference calls for2 years starting in April 2016. After thefirst few months of review anddiscussion of literature as well aslessons learned from developing andimplementing local pathways, keysteps in the SSRD pathway wereoutlined. Achieving interdisciplinaryconsensus on SSRD evaluation,diagnosis, symptom management, anddischarge planning were consideredto be important aspects of thepathway. The vital role ofcommunicating with families andensuring linkages to outpatient careproviders was highlighted.
b. American Academy of Child andAdolescent Psychiatry (AACAP)
2 IBEZIAKO et al
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

Abramson Fund grant: A full weekendworkshop for the Pathways in ClinicalCare (PaCC) working group, consistingof the SSRD working group and2 other working groups, wassponsored by the AACAP AbramsonFund grant. The initial draft of the CPgenerated by the SSRD working groupwas shared with the whole PaCCworking group for feedback. Thepediatrician with CP expertiseprovided substantive input regardingthe development, content, language,and visual representation of theinformation. Reflections andresponses received during thisworkshop were incorporated into asecond draft of the SSRD CP.
c. Stakeholder feedback: Stakeholderfeedback was obtained from 6 NorthAmerican pediatric clinicalinstitutions. These stakeholders camefrom 12 disciplines involved in thediagnosis and treatment of patientswith SSRDs in the pediatric hospitalsetting. This included providers frompediatric hospital medicine,
adolescent medicine, psychology, childpsychiatry, social work, physical andoccupational therapy, casemanagement, neurology, surgery,nursing, and nursing education. Thestakeholders reviewed the seconddraft of CP materials (flowchart andtext documents) and provided specificfeedback on each section of thepathway. Written transcripts of thestakeholder feedback statementswere systematically analyzed foremerging themes (Table 1). Through aconsensus working group process,each feedback element was reviewed,and modifications were made tofurther strengthen the structure andcontent of the pathway.
d. Final draft: The SSRD CP waspresented at a member servicesforum at the AACAP 2017 annualconference in Washington, District ofColumbia. The feedback generatedfrom the forum participants,composing a diverse nationalaudience, was incorporated into thefinal version of the SSRD CP.
RESULTS
The CP development resulted in the creationof 4 components of an SSRD CP, which willbe described in further detail below:
1. an introduction for the suite of CPdocuments;
2. a flowchart to serve as a graphicillustration of the steps in the approachto caring for youth who are hospitalizedwith SSRDs;
3. a detailed text guide including anarrative explanation of each stepoutlined in the CP with supportingliterature; and
4. sample scripts and handouts tostandardize and aide with communicationwithin the steps of the CP.
CP Introduction
In the introductory document, theauthors describe the need for a hospital-based SSRD CP; outline the potentialclinical, financial, and administrativebenefits of addressing the challengesfaced when caring for this patientpopulation; and provide an overview ofthe proposed CP (see SSRD Pathway:Introduction to the CP for SSRDs inthe Supplemental Information). Theinformation presented in theintroductory document is relevant toboth health care providers andhospital administrators when addressingthe whole range of hospital stakeholdersinvolved in facilitating SSRD CPadoption and implementation at thelocal level.
CP Flowchart
The flowchart serves as a visual referencein which the 5 critical steps of the SSRD CPfrom admission to discharge, includingscreening, evaluation, and management, arehighlighted (Fig 2).
CP Text Guide
In the comprehensive companion textdocument for the SSRD CP, the authorsprovide specific, detailed information foreach step of the pathway; this serves as anexplanatory guide for the graphicflowchart (see SSRDs CP Text: Care ofPediatric Patients With SSRDs in Inpatient
FIGURE 1 Steps in creating a CP, reprinted with permission from Dr Ilana Waynik. AAP, AmericanAcademy of Pediatrics.
HOSPITAL PEDIATRICS Volume 9, Issue 3, March 2019 3
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

Medical and Surgical Units in theSupplemental Information). The SSRD CPtext guide includes pertinent backgroundinformation on somatization and SSRD inyouth; the authors describe howinterdisciplinary inpatient pediatric careteams can implement each step and providerecommendations for screening, integratedmedical and psychiatric evaluation, andmanagement. The guide includes the
existing literature that informed each stepof the pathway.
CP Scripts and Handouts
The scripts and handouts developed as partof the SSRD CP are summarized in Table 2.These materials are used to guide theinterdisciplinary providers on how topresent the SSRD CP approach to patientsand their families, including how tointroduce psychiatry and other consultantsas part of the interdisciplinary team,describe the evaluation process to thepatient and family, and share input frominterdisciplinary findings with families. Inthe handouts, the authors summarizepatient- and/or family-centered facts aboutSSRDs and provide consistent language toanchor providers in the communication ofaspects of SSRD care. Because thesepatients rarely present first to behavioralhealth providers, a goal in using thesescripts is to help increase comfort and skillamong health care providers from variousdisciplines in managing SSRDs and tomitigate the challenges experienced byfamilies in receiving and accepting theSSRD diagnoses.
DISCUSSION
This is the first CP developed by a group ofexpert child psychiatrists, with pediatricstakeholder input, from multiple institutionsin North America to standardize pediatricSSRD care in the inpatient hospital setting.The efforts of the working group resulted ina pathway for SSRDs that meets theoperational definition of CPs on the basis ofthe following 4 criteria: (1) it is a structuredmultidisciplinary plan of care; (2) it is usedto translate guidelines or evidence into localprocesses; (3) it includes details of thesteps in a course of treatment or care in aplan, pathway, algorithm, guideline, orprotocol; and (4) it is developed with theaim to standardize care for a specificpopulation.25
Key Themes in the SSRD CP
The first and second steps of the SSRDCP emphasize the early identification ofsomatization with a process ofsimultaneous physical and mental healthdiagnostic evaluations. Studies reveal thatearly mental health consultation reduces
the length of admissions for pediatricpatients who are medically ill with comorbidmental health diagnoses, including patientswith SSRDs.31 It is critical to ensure thatpatients and families understand theinterdisciplinary nature of evaluation andthe multifactorial nature of SSRDs tonormalize the involvement of mental healthprofessionals.6,11,32 Delayed mental healthinvolvement results in patients and familiesperceiving that their care is being“handed off” to mental health and furtherstigmatizes the condition.10 The presence ofinconsistent physical symptoms and/orpsychosocial stressors, although raising theconcern for possible somatization, isinsufficient to make a diagnosis of SSRD.The importance of an interdisciplinaryevaluation that includes a comprehensiveand judicious medical workup is alsoemphasized to ensure that existing medicalconditions are not overlooked in thecontext of the concerns for somatizationand SSRD evaluation. With the use of theSSRD CP, patient and family expectations areset early in the course of the inpatienthospitalization to align them with the role ofthe interdisciplinary care team. Theseexpectations include interdisciplinaryevaluation and management in whichsymptom reduction (as feasible) is targetedthrough the use of behavioral interventions,rehabilitation therapies, and parent trainingand establishing an interdisciplinaryoutpatient treatment plan.6,33
For the third and fourth steps of theSSRD CP, it is recommended that aninterdisciplinary provider meeting and aninforming family meeting be held once thediagnostic assessment is completed. SSRDcare is often characterized by disjointedevaluations and mixed message delivery topatients and families.7 Ensuring effective,interdisciplinary communication with thefamily has been found to be associatedwith improved treatment adherence,participation in outpatient follow-up,and improved patient outcomes.32 Teammeetings have been shown to be associatedwith high patient and caregiver satisfactionin the pediatric inpatient medicalsetting, particularly for patients withcomorbid medical and mental healthdiagnoses.34 A coordinated approach by
TABLE 1 Stakeholder Feedback
Stakeholder disciplines
Pediatrics and/or pediatric hospital medicine
Adolescent medicine
Psychology
Child psychiatry
Social work
Physical therapy
Occupational therapy
Case management
Neurology
Surgery
Nurses
Nurse educators
Overall feedback
“An important topic, for which a pathway andguide are needed.”
“I think this generally looks very good. I likethe organized, multidisciplinary approach.I’ve shown it to a few other members ofmy team who agree.”
“[I] like the idea of making things consistent.”
“This will be a very helpful document. It is welllaid out and very clear.”
Emergent themes
Streamlining and formatting suggestions forthe flowchart and documents
Clarify timing of psychiatry involvement
Clarify terminology and language
Clarify roles and responsibilities ofinterdisciplinary providers
Goal discordance: medical and psychiatryteams
Clarify communication with patients andfamilies
Clarify communication processes with externalhealth care providers
Provide resources for physicians and otherhealth care providers
Customization of care versus standardization
Anticipated process challenges
Create a new model of care
4 IBEZIAKO et al
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

interdisciplinary providers reaffirms themultifactorial nature of SSRDs, facilitatesa consistent communication strategy,and reduces the likelihood ofmisunderstandings or miscommunicationabout the diagnoses. In the informingmeeting, families are provided with ashared conceptual framework for somaticsymptom development. Providers areallotted an opportunity to educate familiesabout SSRDs and review the diagnostic
formulation by using language that isconsistent with the Diagnostic andStatistical Manual of Mental Disorders, FifthEdition (DSM-5). Involving primary care andother key outpatient providers in theinforming meeting allows for a naturaltransition point in the SSRD care fromcompleting the diagnostic evaluation tofocusing on multidisciplinary managementand disposition planning, includingoutpatient care.7,32 Using terminology that is
consistent, understandable, and based onthe DSM-5 and providing explanationregarding the biopsychosocial model iscritical to effective symptom evaluation andmanagement.7 Therefore, practical scriptsare included in the CP to guide clinicians atall levels of training to effectively discussthe conceptual framework of symptomdevelopment, diagnosis, and treatmentregarding pediatric SSRDs. The scriptsfoster the operationalization of the CP byincluding tools and resources for providersto enact the core steps of the pathway.
Early management and disposition planningare the focus in the fifth and final step of thepathway. The treatment of SSRDs can beinitiated within the hospital setting with thegoal of improving functionality andsuccessfully transitioning to outpatientcare.35 Children with more profound andpervasive functional impairment, with orwithout other comorbid conditions, mayneed more intensive treatments, includingadmission to medical-psychiatric programsor physical rehabilitation units.6 Dispositionplanning is multidisciplinary with a focus onpromoting active engagement with theprimary care provider (PCP), establishingfollow-up care with outpatient mental healthproviders who are familiar with SSRDs,ongoing monitoring by subspecialtypediatric providers as indicated, usingcontinued outpatient rehabilitative servicesif needed, and providing guidance tofamilies and schools.10,32,33,35,36 Scheduled andfrequent follow-up visits with a PCP areimportant to maintain the alliance andinvestment in treatment and provideongoing medical education andreassurance.33
Limitations and Future Directions
The SSRD CP working group primarilyconsisted of experts in child and adolescentconsultation-liaison psychiatry. Providers inother disciplines, including psychology, wereinvolved in the stakeholder feedback butwere not part of the primary workinggroup. Interdisciplinary and patient and/orfamily involvement in the operationalizationof the SSRD CP and care expansionto outpatient settings will be helpfulin capturing a broader perspective onSSRD care.
FIGURE 2 CP for SSRDs.
HOSPITAL PEDIATRICS Volume 9, Issue 3, March 2019 5
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

Compared with other clinical diagnoses inchild and adolescent psychiatry, such asdepression and anxiety, as well as suicide,there is a relative dearth of literature onSSRD evaluation and management,particularly in inpatient pediatric settings.Available evidence supported thedevelopment of this pathway; however,randomized controlled trials for theevaluation and treatment of SSRDs are stilllacking. The working group was faced with adiversity of practices, expectations, systems,and resources that currently exists in SSRDcare throughout the represented geography.This was obviated by sharing currentpractices and resources, developing aconsensus set of principles andfundamental practices, and accounting forthe known limitations in mental healthconsultation and access that often exist inmany parts of North America. Because theSSRD working group relied on expertconsensus and experience to inform theCP and resource development, there ispotential for the introduction of bias in theCP development by relying more on themembers of the group with greaterexperience in SSRD care. For this initialeffort in the standardization of care, theconsensus was developed by usingdiscussions and verbal communicationsamong the working group members;no formal method of consensusgathering, such as the Delphi procedure,was used.
Specific recommendations for inpatientassessment and the management of SSRDshave been made in this CP. We recognizethat the pathway implementation may beinfluenced by resource availability in localhospital settings, including a psychiatryconsultation-liaison service. The diversity ofthe practice locations of the working groupwas intended to mitigate this limitation,and consideration of resource limitations wasa guiding principle in this CP development.The SSRD CP is a flexible guide that allowsfor clinicians to adapt it to local resourcesand realities while preserving the corefeatures, central themes, and principles ofthe CP.
With significant changes in the diagnosticlanguage and criteria of SSRDs within the
TABLE 2 SSRD CP Scripts and Handout
Description
Family introductory handout Your child currently has physical symptoms that are causing greatworry and may leave you with questions and concerns. Yourfamily is attempting to understand your child’s symptoms and getan explanation for why your child continues to have physicalsymptoms. These symptoms are impairing and getting in the wayof your child’s health and success. We understand that yourchild’s illness has been difficult for your child and everyone inyour family.
At this time, your child will be admitted to the hospital for a briefstay to conduct an evaluation with the goals of the following:• understanding your child’s symptoms and their impact onfunctioning;
• providing a diagnosis or diagnoses;• providing an explanation for your child’s symptoms;• providing some symptomatic relief for your child; and• developing a plan for continued care to improve your child’sfunctioning.
Your child’s evaluation will include the following:• a careful review of previous medical records and informationabout your child;
• completion of previous medical records and information aboutyour child;
• completion of any further evaluations as needed; and• working together with a team that may include pediatricians,pediatric
• subspecialists, psychiatry, psychology, social work, physicaltherapy, occupational therapy, speech therapy, and child life.
At the end of your child’s stay, your child will have a completedevaluation, discussion of results, review of diagnoses, andexplanations for symptoms as well as a plan for future symptomcare. Your child’s symptoms may not be gone when your childis ready to leave the hospital. We will work to establish goalsto improve your child’s health and help your child return tonormal activities, including a plan to collaborate with your child’sschool, primary care doctor, and other providers in thecommunity to promote your child’s functioning and improvementon discharge.
Sample script
Introducing psychiatry and otherconsultations to the family
“We are going to review all the tests and treatments you’ve done sofar to determine what has been helpful, what needs to berepeated, and what new tests and consultations are needed. Wesee many children with symptoms similar to what your child hasand have a standard multidisciplinary approach to care thatincludes different consultants from medical specialties, surgicalspecialties, physical and/or occupational therapy, social work,psychiatry and/or psychology, etc. This comprehensive approachwill help us better understand the nature of your child’ssymptoms and the impact on all areas of his or her life andwill also help us develop an effective management plan.”You may include this last sentence here or only in thecontext below.
If family is resistant to psychiatry consultation or asks for moreinformation regarding this, clarify that psychiatry helps with thefollowing:• understanding the child’s symptoms;• assessing the impact of the symptoms on the child and on thefamily; and
• helping the child and family cope with the symptoms and gettheir lives back.
6 IBEZIAKO et al
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

DSM-5, as well as the overlap of a variety of
other clinical and nonclinical termscommonly used when describing symptoms
and presentations of SSRDs, the workinggroup spent a considerable amount of time
clarifying, reviewing, and discussing the useof language and terms. Ultimately, the
decision was made to focus on DSM-5 language for consistency and clarity given
the audience using the SSRD CP. Localpractices and language that is familiar and
well accepted by patients, families, andproviders can be accommodated within the
CP so long as they generally adhere to the
principles and current evidence and theDSM-5. Although the scope of the SSRD CP
was to be focused on the inpatient pediatricsetting, the CP and its associated resources
contain significant language prompts toengage and communicate with providers
within the outpatient setting so as to allowfor a smooth transition of care and cross-
talk between the 2 systems. Because thesepatients often present to emergency
departments, future efforts to addressSSRD care in this setting will also be
important.
Finally, the implementation and efficacy ofthis SSRD CP has not yet been establishedempirically. Future directions for the CPimplementation point toward developingpartnerships with pediatric hospitalists andsubspecialists, hospital administrators,nurses, consultation-liaison psychiatrists,psychologists, and support staff. It isimportant to identify local champions tolead implementation by providing educationand support for the clinical application ofthe pathway. Research studies on thefeasibility and outcomes of the SSRD CP areneeded to investigate if the SSRD CP has thepotential to be used to standardize pediatricSSRD care in hospital settings acrossmedical institutions in North America. Themembers of the North American PaCC SSRDworking group plan to implement the SSRDCP in individual institutions and empiricallystudy the implementation process andanticipated outcomes, includingimprovements in clinical care, cost savings,and the impact of early interdisciplinarycollaboration.
TABLE 2 Continued
Description
Introducing the use of measures “As part of our evaluation, we have some measures for you and yourchild to complete that will help us in our assessment. Thesemeasures take approximately [insert number] minutes to completeand help us standardize our evaluation process while being asthorough as possible. The measures assess [insert examples basedon measures being administered]. Please be assured that completingthese measures is voluntary, and if you do not wish to do so, thiswould not change the care that you receive while in the hospital.”
Informing family meeting “As we said at the beginning of your child’s hospital stay, after completingyour child’s evaluation, we come together as a multidisciplinary teamto discuss what we think is contributing to your child’s symptomsand what we think the treatment should be. We want to give you achance to ask questions and to be sure that you feel comfortableabout our assessment and treatment plan. We understand howdebilitating these symptoms have been and want to take our time tobe sure we address your questions or concerns.”
“We want to share with you a summary of your child’s symptoms,why we consulted with the specialists we did, what diagnoses wewere considering, and what our findings did or did not support.Please tell us along the way if we have any part of the historywrong or if there is anything you do not understand. And pleaselet us know if there is any particular medical condition ordiagnosis that you feel we have not adequately addressed.”
• [Patient name] first presented with:
• Previous workup included:
• Our team performed the following tests and/or evaluations:
• We found the following:
• Given these findings and with the input from our specialists,we think your child’s symptoms are best understood asa:
• In our experience, symptoms due to [insert here] respond bestto the following treatment approach:
Discussing the mind-bodyconnection
“The brain and body are connected and communicate throughnerves, hormones, and chemicals. We call this the mind-bodyconnection. Sometimes it’s hard to understand how the mind-body connection contributes to symptoms, so we want to explainthat. The body automatically sends information to the brain, andat the same time, the brain automatically sends information tothe body to communicate feelings, such as fear and pain.”
“You may have heard of the ‘fight-flight-freeze’ response. When wesense danger, the brain tells the body to stay on alert usingelectrical and chemical signals. The body starts doing things tohelp us survive; for example, lungs breathe faster and shallower,and [the] heart beats faster and harder to get more oxygen tothe brain and muscles. Muscles tense up, getting ready to fightor run. All of these reactions happen quickly and automatically,without us even thinking about it. Later, when the danger is gone,the brain tells the body to calm down, but the experience canleave a physical toll on the body. This is our body’s response tostress, also known as the physiology of stress.”
“Stress can be positive or negative, and although we may notconsider something ‘dangerous’ or stressful, our bodies canexperience the effects of stress through physical symptoms. Inthis way, we can view the physical symptoms as the body tellingus it is feeling distressed or that we are feeling the emotion orstress in our bodies.”
a If an SSRD is being considered or the diagnosis has been made, the attending physician leading themeeting should use the actual diagnosis rather than a symptom or general language (eg, conversionrather than “stress”). Ask psychiatry colleagues present to give their assessment of potentialcontributors that have been determined from the psychiatric evaluation performed. Additionalexplanatory handouts can be used as needed, including the AACAP Facts for Families on SSRD.1
HOSPITAL PEDIATRICS Volume 9, Issue 3, March 2019 7
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

CONCLUSIONS
This CP is the first attempt to develop astandardized approach to SSRD care acrossmultiple pediatric institutions in NorthAmerica. Given the existing gap in guidelinesfor the care of these patients in manyhospitals, this CP will be a helpfulresource for health care providers ofvarious disciplines in the assessmentand management of youth who aremedically hospitalized with SSRD.
Acknowledgments
The PaCC working group of the AACAPPhysically Ill Child Committee assisted in theconceptualization and design of the studyand provided feedback on the CP.The PaCC working group consists of allnamed authors as well as the followingmembers: Khalid Afzal, MD; Sonali Bora,MD; Sophia Hrycko, MD; Lisa Horowitz, PhD,MPH; Willough Jenkins, MD; Kyle Johnson,MD; Julia Kearney, MD; Elizabeth Kowal, MD;Brian Kurtz, MD; Roberto Ortiz-Aguayo,MD; and Gabrielle Silver, MD. We aregrateful to all the stakeholders whoprovided feedback on the CP; Ilana Waynik,MD, for providing guidance in CPdevelopment; Hana Saab, PhD, for helpinganalyze the stakeholder feedback; andQuentin Bernhard, Kathleen Samiy,and Patricia Jutz for their help withformatting the pathway flowchart and textdocuments.
REFERENCES
1. American Academy of Child andAdolescent Psychiatry. Physicalsymptoms of emotional distress:somatic symptom and related disorders.2018. Available at: https://www.aacap.org/AACAP/Families_and_Youth/Facts_for_Families/FFF-Guide/Physical_Symptoms_of_Emotional_Distress-Somatic_Symptoms_and_Related_Disorders.aspx. Accessed August 27,2018
2. American Psychiatric Association.Diagnostic and Statistical Manual ofMental Disorders. 5th ed. Washington,DC: American Psychiatric Publishing;2013
3. Bujoreanu S, Randall E, Thomson K,Ibeziako P. Characteristics of medically
hospitalized pediatric patients withsomatoform diagnoses. Hosp Pediatr.2014;4(5):283–290
4. Thomson K, Randall E, Ibeziako P,Bujoreanu IS. Somatoform disordersand trauma in medically-admittedchildren, adolescents, and young adults:prevalence rates and psychosocialcharacteristics. Psychosomatics. 2014;55(6):630–639
5. Looper KJ, Kirmayer LJ. Perceived stigmain functional somatic syndromes andcomparable medical conditions.J Psychosom Res. 2004;57(4):373–378
6. Ibeziako P, Bujoreanu S. Approach topsychosomatic illness in adolescents.Curr Opin Pediatr. 2011;23(4):384–389
7. Malas N, Ortiz-Aguayo R, Giles L, IbeziakoP. Pediatric somatic symptom disorders.Curr Psychiatry Rep. 2017;19(2):11
8. Geist R, Weinstein M, Walker L, Campo JV.Medically unexplained symptoms inyoung people: the doctor’s dilemma.Paediatr Child Health. 2008;13(6):487–491
9. Lindley KJ, Glaser D, Milla PJ.Consumerism in healthcare can bedetrimental to child health: lessons fromchildren with functional abdominal pain.Arch Dis Child. 2005;90(4):335–337
10. Campo JV, Fritz G. A management modelfor pediatric somatization.Psychosomatics. 2001;42(6):467–476
11. Campo JV. Annual research review:functional somatic symptoms andassociated anxiety anddepression–developmentalpsychopathology in pediatric practice.J Child Psychol Psychiatry. 2012;53(5):575–592
12. Rask CU, Ørnbøl E, Fink PK, SkovgaardAM. Functional somatic symptoms andconsultation patterns in 5- to 7-year-olds. Pediatrics. 2013;132(2). Availableat: www.pediatrics.org/cgi/content/full/132/2/e459
13. Gieteling MJ, Lisman-van Leeuwen Y, vander Wouden JC, Schellevis FG, Berger MY.Childhood nonspecific abdominal pain infamily practice: incidence, associated
factors, and management. Ann Fam Med.2011;9(4):337–343
14. Shaw RJ, Pao M, Holland JE, DeMaso DR.Practice patterns revisited inpediatric psychosomatic medicine.Psychosomatics. 2016;57(6):576–585
15. Miresco MJ, Kirmayer LJ. Thepersistence of mind-brain dualism inpsychiatric reasoning about clinicalscenarios. Am J Psychiatry. 2006;163(5):913–918
16. Wileman L, May C, Chew-Graham CA.Medically unexplained symptoms andthe problem of power in theprimary care consultation: aqualitative study. Fam Pract. 2002;19(2):178–182
17. Dell ML, Campo JV. Somatoformdisorders in children and adolescents.Psychiatr Clin North Am. 2011;34(3):643–660
18. Ring A, Dowrick C, Humphris G, Salmon P.Do patients with unexplained physicalsymptoms pressurise generalpractitioners for somatic treatment? Aqualitative study. BMJ. 2004;328(7447):1057
19. Grimshaw JM, Eccles MP, Lavis JN, Hill SJ,Squires JE. Knowledge translation ofresearch findings. Implement Sci. 2012;7:50
20. Rotter T, Plishka C, Hansia MR, et al. Thedevelopment, implementation andevaluation of clinical pathways forchronic obstructive pulmonarydisease (COPD) in Saskatchewan:protocol for an interrupted timesseries evaluation. BMC Health ServRes. 2017;17(1):782
21. Francke AL, Smit MC, de Veer AJ,Mistiaen P. Factors influencing theimplementation of clinical guidelines forhealth care professionals: a systematicmeta-review. BMC Med Inform DecisMak. 2008;8:38
22. Hakkennes S, Dodd K. Guidelineimplementation in allied healthprofessions: a systematic review of theliterature. Qual Saf Heal Care. 2008;17(4):296–300
23. Kitson A. Knowledge translation andguidelines: a transfer, translation or
8 IBEZIAKO et al
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

transformation process? Int J Evid-BasedHealthc. 2009;7(2):124–139
24. Yana R, Jo RM. Getting guidelines intopractice: a literature review. Nurs Stand.2004;18(50):33–40
25. Lawal AK, Rotter T, Kinsman L, et al. Whatis a clinical pathway? Refinement of anoperational definition to identify clinicalpathway studies for a Cochranesystematic review. BMC Med. 2016;14:35
26. Ban A, Ismail A, Harun R, Abdul RahmanA, Sulung S, Syed Mohamed A. Impact ofclinical pathway on clinical outcomes inthe management of COPD exacerbation.BMC Pulm Med. 2012;12:27
27. Casas A, Troosters T, Garcia-Aymerich J,et al; Members of the CHRONIC Project.Integrated care prevents hospitalisationsfor exacerbations in COPD patients. EurRespir J. 2006;28(1):123–130
28. Rotter T, Kinsman L, James E, et al.Clinical pathways: effects on professionalpractice, patient outcomes, length of stay
and hospital costs. Cochrane DatabaseSyst Rev. 2010;(3):CD006632
29. Kaiser SV, Rodean J, Bekmezian A, et al;Pediatric Research in Inpatient Settings(PRIS) Network. Effectiveness ofpediatric asthma pathways forhospitalized children: a multicenter,national analysis. J Pediatr. 2018;197:165–171.e2
30. Waynik I, Sekaran A. A path to successfulpathway development. Presented atPediatric Hospital Medicine AnnualConference; July 29, 2016; Chicago, IL
31. Bujoreanu S, White MT, Gerber B,Ibeziako P. Effect of timing of psychiatryconsultation on length of pediatrichospitalization and hospital charges.Hosp Pediatr. 2015;5(5):269–275
32. Plioplys S, Asato MR, Bursch B,Salpekar JA, Shaw R, Caplan R.Multidisciplinary management ofpediatric nonepileptic seizures. JAm Acad Child Adolesc Psychiatry.2007;46(11):1491–1495
33. Burton C, Weller D, Marsden W, Worth A,Sharpe M. A primary care symptomsclinic for patients with medicallyunexplained symptoms: pilotrandomised trial. BMJ Open. 2012;2:e000513
34. Kitts RL, Gallagher K, Ibeziako P,Bujoreanu S, Garcia G, Demaso DR.Parent and young adult satisfaction withpsychiatry consultation services in achildren’s hospital. Psychosomatics.2013;54(6):575–584
35. Ibeziako P, Rohan JM, Bujoreanu S, ChoiC, Hanrahan M, Freizinger M. Medicallyhospitalized patients with eatingdisorders and somatoform disorders inpediatrics: what are their similaritiesand differences and how can weimprove their care? Hosp Pediatr. 2016;6(12):730–737
36. Kroenke K. Efficacy of treatment forsomatoform disorders: a review ofrandomized controlled trials. PsychosomMed. 2007;69(9):881–888
HOSPITAL PEDIATRICS Volume 9, Issue 3, March 2019 9
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

originally published online February 19, 2019; Hospital Pediatrics Steinbuchel, Maryland Pao and Sigita Plioplys
Shanti Gooden, Finza Latif, Nasuh Malas, Lisa Namerow, Ruth Russell, Petra Patricia Ibeziako, Khyati Brahmbhatt, Andrea Chapman, Claire De Souza, Lisa Giles,
Pediatric Hospital SettingsDeveloping a Clinical Pathway for Somatic Symptom and Related Disorders in
ServicesUpdated Information &
2018-0205http://hosppeds.aappublications.org/content/early/2019/02/17/hpeds.including high resolution figures, can be found at:
Supplementary Material
2018-0205.DCSupplementalhttp://hosppeds.aappublications.org/content/suppl/2019/02/17/hpeds.Supplementary material can be found at:
References
2018-0205#BIBLhttp://hosppeds.aappublications.org/content/early/2019/02/17/hpeds.This article cites 31 articles, 9 of which you can access for free at:
Subspecialty Collections
psychology_subhttp://www.hosppeds.aappublications.org/cgi/collection/psychiatry_Psychiatry/Psychologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
mlhttp://www.hosppeds.aappublications.org/site/misc/Permissions.xhtin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.hosppeds.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

http://hosppeds.aappublications.org/content/suppl/2019/02/17/hpeds.2018-0205.DCSupplementalData Supplement at:
Print ISSN: 1073-0397. Illinois, 60143. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. published, and trademarked by the American Academy of Pediatrics, 345 Park Avenue, Itasca,publication, it has been published continuously since 1948. Hospital Pediatrics is owned, Hospital Pediatrics is the official journal of the American Academy of Pediatrics. A monthly
by guest on July 8, 2020www.aappublications.org/newsDownloaded from

originally published online February 19, 2019; Hospital Pediatrics Steinbuchel, Maryland Pao and Sigita Plioplys
Shanti Gooden, Finza Latif, Nasuh Malas, Lisa Namerow, Ruth Russell, Petra Patricia Ibeziako, Khyati Brahmbhatt, Andrea Chapman, Claire De Souza, Lisa Giles,
Pediatric Hospital SettingsDeveloping a Clinical Pathway for Somatic Symptom and Related Disorders in
http://hosppeds.aappublications.org/content/early/2019/02/17/hpeds.2018-0205located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 1073-0397. Illinois, 60143. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. published, and trademarked by the American Academy of Pediatrics, 345 Park Avenue, Itasca,publication, it has been published continuously since 1948. Hospital Pediatrics is owned, Hospital Pediatrics is the official journal of the American Academy of Pediatrics. A monthly
by guest on July 8, 2020www.aappublications.org/newsDownloaded from


![[스트레스/대응 기능장애] ThemeGallery PowerTemplatecontents.kocw.net/KOCW/document/2016/chosun/kimhyunlye/1.pdf · 2017. 2. 20. · Somatic Symptom Disorder . 정의 및](https://img.pdfslide.net/doc/110x75/5ffc4fecee9d8d4e5a459b42/eeoe-ee-themegallery-p-2017-2-20-somatic-symptom.jpg)