Embed Size (px)
Citation preview

Vol. 117 No. 5 May 2014
Developing a protocol for gastrostomy tube insertion in patientsdiagnosed with head and neck cancerSyed F. Habib, Suhail Ahmed, Rachel Skelly, Kavita Bhatt, Bhaveshree Patel, Derek Lowe, Julian Tuson, andSimon N. RogersAintree University Hospital, Liverpool, United Kingdom
Selecting patients with head and neck cancer requiring a pretreatment gastrostomy feeding tube is not
straightforward. The nutritional status and functional deficits associated with the cancer, its treatment, and the long-term side
effects predicate the need for gastrostomy tube placement. However, gastrostomy tubes are not without morbidity and are an
added burden to the patient. The aim of this retrospective case series review was to evaluate the clinical characteristics of
newly diagnosed patients with head and neck cancer treated with curative intent having gastrostomy placement, with
the intent of developing a protocol to help with the timely selection of patients for pretreatment gastrostomy insertion.
A gastrostomy tube was placed in 32%. A regression model identified 5 independent predictors (P < .001) to predict
gastrostomy tube placement: overall clinical stage, tumor site, clinical T stage, patient age, and clinical N stage. A protocol to
help the multidisciplinary team to decide whether a pretreatment gastrostomy tube should be placed is suggested. (Oral Surg
Oral Med Oral Pathol Oral Radiol 2014;117:551-559)
Statement of Clinical Relevance
The incidence of head and neck (H&N) cancer is risingin England.1 There is evidence of improved survival2
but also recognition of the late effects of treatment andits effect on function and health-related quality of life(HRQOL).3 Treatment of H&N cancer is associatedwith significant morbidity and malnutrition due toswallowing difficulties.4-10 A subgroup of patients willrequire dietary supplementation to meet nutritional re-quirements. The gastrostomy tube is a well-establishedmethod of providing nutrition in patients who are unableto maintain nutritional requirements via the oral route.Feeding gastrostomy tubes can be inserted percutane-ously under direct vision using an endoscope (known aspercutaneous endoscopic gastrostomy [PEG]), underradiologic guidance (called radiologically inserted gas-trostomy [RIG]), or using a conventional open or lapa-roscopic surgical approach. PEG is the most commonlyemployed technique, owing to fewer complications.11 Asignificant number of these tubes are placed prophylac-tically (i.e., before the start of treatment in anticipation ofswallowing difficulties faced during or after treatment).The length of time during which patients are dependenton gastrostomy tubes ranges up to 7.1 months, with amedian of 21 weeks.12,13 A cross-sectional study byCheng et al.14 that included 98 patients reported that theprevalence of gastrostomy tube was 30% at 1 month and8% at 3 years. The percentage of patients with long-termdependence on gastrostomy feeding varies across studiesaccording to subgroups and can be as high as 41% at 12
Aintree University Hospital.Received for publication May 27, 2013; returned for revision Dec 1,2013; accepted for publication Dec 30, 2013.� 2014 Elsevier Inc. All rights reserved.2212-4403/$ - see front matterhttp://dx.doi.org/10.1016/j.oooo.2013.12.412
months and 17% at 48 months in patients undergoingintense chemoradiotherapy.15
The role of nutritional supplementation via tubefeeding is well established in patients undergoingtreatment of H&N cancer, especially if their treatmentplan includes the use of chemoradiation.16,17 This canbe achieved with nasogastric or gastrostomy tubes.There is a consensus for using a gastrostomy tube ifnutritional supplementation is likely to last more than 4weeks.18 But it is not clear whether the gastrostomytubes should be prophylactic (i.e., placement before thestart of treatment) or reactive (i.e., placement if patientsdevelop swallowing dysfunction during the course oftreatment). Various single-center retrospective analysesand case note reviews have described benefits of pro-phylactic gastrostomy tubes and recommended theiruse in all patients undergoing chemoradiotherapy,19-21
whereas others have argued against such practice be-cause it leads to long-term dependence on tube feedingin addition to other complications.17,22-24 A retrospec-tive study determined that a significant number of pa-tients (47%) never used their PEG or used it for lessthan 2 weeks, although the results need to be viewedwith caution because usage data were not available forone-third of patients.25 In addition, gastrostomy feeding
A retrospective analysis of gastrostomy tube inser-tion in patients with head and neck cancer wasperformed with a view to developing a protocol.Statistically significant factors form the basis of thesuggested protocol. Gastrostomy usage, complica-tions, and quality of life are reported.
551

Table I. Characteristics of patients having prophylacticand reactive gastrostomy tubes
ProphylacticGT (N ¼ 224)
ReactiveGT (N ¼ 65) P*
GenderMale 72% (162) 91% (59) .001
Age (y) .10<55 33% (74) 32% (21)55-69 41% (92) 29% (19)70þ 26% (58) 38% (25)
Primary treatmentSurgery and RT 40% (90) 52% (34) <.001Surgery alone 18% (41) 37% (24)Chemo/RT alone 42% (93) 11% (7)
Free flap (if surgery)No free flap 35% (46) 54% (35) .005Soft 46% (60) 23% (15)Composite 19% (25) 12% (8)
T stageT3/T4 62% (137/222) 35% (23/65) .02
N stageN1þ 43% (97/223) 45% (29/65) .89
Overall clinical stage3-4 83% (186) 72% (47) .08
Tumor locationOral 26% (59) 35% (23) .005Pharyngeal 50% (113) 31% (20)Laryngeal 12% (27) 26% (17)Other H&N 11% (25) 8% (5)
SpecialtyMFU 46% (102) 43% (28) .78ENT 54% (122) 57% (37)
Year diagnosed2005-2006 41% (92) 34% (22) .182007-2008 37% (82) 32% (21)2009 22% (50) 34% (22)
GT, gastrostomy tube;MFU, Aintree Maxillo Facial Unit; ENT, AintreeEar Nose & Throat Department; RT, radiotherapy;H&N, head and neck.*Fisher exact test for gender and specialty; otherwise, c2 test.
ORAL AND MAXILLOFACIAL SURGERY OOOO
552 Habib et al. May 2014
does not improve survival and is associated with poorerquality of life (QOL).26-28 One retrospective analysisconcluded that clinical judgment appears to be suffi-cient for deciding which patients will benefit fromprophylactic tube placement.29 In another review ofpractice in cases where PEG tubes were not placedprophylactically, 18% of patients without recurrentdisease at 6 months and 6% of those without recurrentdisease at 1 year were dependent on PEG tubes.30
Recently published guidelines suggest intensive patientfollow-up and prophylactic feeding tube insertionshould be seriously considered for individuals initiallypresenting with 1 or more of the following symptoms:significant weight loss (more than 5% in 1 month or morethan 10% in 6 months), body mass index (BMI) below18.5, dysphagia, anorexia, dehydration, pain, or anyother symptom that interferes with the ability to eat.31
A comprehensive review of multiple studies and asystematic review of available evidence concluded thatcurrent evidence is insufficient to make a definitiverecommendation for prophylactic gastrostomy tubeinsertions and that further studies are necessary todetermine the effect of such practices on tumor controland patient survival. Such studies are also necessary toassess the effect of timing of PEG insertion on thelong-term outcomes of PEG tube dependence andeating ability.32,33 A web-based survey at a tertiaryreferral center in England concluded that there is nonational consensus on which patients to recommendfor gastrostomy and that consideration should be givento the development of clinical decision-making modelsin an attempt to systematize the decision-makingprocess.34 Hence, the aim of this case note review wasto evaluate what proportion of newly diagnosed pa-tients with H&N cancer treated with curative intent atAintree University Hospital had gastrostomy place-ment over a period of 5 years between 2005 and 2009.We have analyzed the proportion and duration ofprophylactic gastrostomy tubes that were used forfeeding after initiation of treatment or that continued tobe used at discharge from the hospital after surgery.We also aimed to report the clinical characteristics,timing, and complications, with the purpose ofinforming discussions on the development of a pro-tocol to help with the timely selection of patients forprophylactic gastrostomy tube insertion.
METHODSA retrospective case series review of 947 patientstreated for primary H&N squamous cell carcinomabetween 2005 and 2009 at University Hospital Aintreewas performed. Patients with cutaneous and salivarygland malignancy, those treated with palliative intent,and those living overseas were excluded. Mortalitystatus was tracked via the Office for National Statistics.
Clinical data from the H&N cancer database at the timeof primary cancer treatment were supplemented withdietetic and archive records. Patient weight (kg), BMI,albumin (g/L), PEG or RIG placement, and dietitianinput were recorded. Questions about feeding tubesformed part of the annual postal survey of H&N cancersurvivors in 2012. It included questions regardingfeeding tubes ever placed, tubes currently in situ, thetiming of removal, and the frequency of use to sup-plement food/nutrition. We recorded the immediate andlate complications associated with gastrostomy tubeinsertion.
The University of Washington Quality of LifeQuestionnaire (UWQOL) version 4 is well estab-lished.35 For this study, the UWQOL was analyzed interms of its 2 subscale composite scores, “physicalfunction” and “social-emotional function,” and a single6-point “overall” QOL measure. Physical function isthe simple average of the swallowing, chewing, speech,

Table II. Gastrostomy tubes and nutritional data from 526 dietary assessments
Tube use Weight (kg), median (IQR), n BMI, median (IQR), n Albumin (g/L), median (IQR), n
Gastrostomy tube 70 (59-82), n ¼ 225 24 (21-28), n ¼ 168 40 (34-43), n ¼ 184No gastrostomy tube 72 (60-85), n ¼ 280 26 (22-29), n ¼ 215 35 (30-41), n ¼ 213
Mann-Whitney test P ¼ .09 P ¼ .004 P < .001How was tube used (if known):
Tube used 70 (61-80), n ¼ 81 24 (21-27), n ¼ 65 39 (34-42), n ¼ 65Tube not used 66 (63-82), n ¼ 29 23 (21-27), n ¼ 21 39 (34-43), n ¼ 23Mann-Whitney test P ¼ .98 P ¼ .99 P ¼ .76
Not known 70 (58-84), n ¼ 115 24 (21-29), n ¼ 82 40 (34-43), n ¼ 96
IQR, interquartile range; BMI, body mass index.
OOOO ORIGINAL ARTICLE
Volume 117, Number 5 Habib et al. 553
saliva, taste, and appearance domain scores, and social-emotional function is the simple average of the activity,recreation, pain, mood, anxiety, and shoulder domains.In earlier work, we combined domain scores withdomain importance to define cutoff levels beyondwhich patients could be regarded as having a “signifi-cant problem.”36,37 In regard to the single-item overallQOL scale, patients were asked to consider not onlyphysical and mental health but also other factors, suchas family, friends, spirituality, or personal leisure ac-tivities important to their enjoyment of life.
Association of patient and clinical factors withinsertion of gastrostomy tubes and type of tube (pro-phylactic or reactive) was tested using the Fisher exacttest or the c2 test as appropriate. Association of weight,BMI, and albumin level with gastrostomy tube insertionand use was tested using the Mann-Whitney test. TheMann-Whitney test was also used to test associationwith overall QOL and the subscale scores of theUWQOL, and the Fisher exact test was used with sig-nificant problems in each UWQOL domain. Binarylogistic regression was used to model the selectionprocess, which leads to some patients being exposed togastrostomy tubes and others not so. Predicted proba-bilities from the final model provided the basis of theprotocol to help in the multidisciplinary team decisionon whether a gastrostomy tube should be placed.Kaplan-Meier estimates of survival were performed foroverall survival. Missing data are reflected by changesin denominator. IBM SPSS, version 19, was used for allanalyses.
After submission to the local Clinical GovernanceDepartment, the study was confirmed as meeting thecriteria for service evaluation and audit.
RESULTSA total of 947 patients were identified, with mean ageof 63 years (standard deviation, 11 years), and 70%(659) were men. Primary diagnosis was made betweenJanuary 1, 2005, and December 31, 2009, with 510from the Maxillo Facial Unit and 437 from the EarNose & Throat Department. Tumor site was identifiedas oral for 44% (412) (in the oral cavity), pharyngeal for
26% (242), laryngeal for 22% (210), and other H&Ncancer locations for 9% (83). Clinical T stage wasadvanced T3-4 for 33% (309 of 934); N was positivefor 34% (320 of 942); and overall clinical grade wasadvanced stage 3-4 for 51% (483 of 943). Primarytreatment was surgery alone for 44% (415), surgerywith adjuvant radiotherapy for 31% (292), and che-moradiotherapy or radiotherapy alone for 25% (240).Of those treated with surgery, 36% (256 of 707) hadfree flaps (178 soft, 78 composite). Kaplan-Meier esti-mates for all-causes survival were 84% (standard error[SE], 1%) at 12 months, 73% (SE, 1%) at 24 months,and 56% (SE, 2%) at 60 months.
A gastrostomy feeding tube was placed within 4months of diagnosis or surgical procedure in 32% (299of 947). Of these, 7 had both PEG and RIG, 12 hadRIG only, and 280 had PEG only. The median timefrom primary diagnosis to insertion of a tube was 25days (interquartile range [IQR], 14-43 days) (n ¼284); from primary surgery, 3 days before (IQR, 9days before to 14 days after surgery [n ¼ 184]), with22% (65 of 289) being done after treatment started. Ofthe 299 with a tube inserted, data about whether theywere used or not were known for 130: for 78% (101)they were used, and in 22% they were not used. Of the101 users, the nature of use was known for 91: 62%(56) were tube dependent and 38% (35) were supple-mentary. Duration of using the tube was known for 86:22% (19; 2 of these until death), under 3 months; 19%(16; 2 until death), 3 to 5 months; 24% (21; 9 untildeath), 6 to 11 months; and 35% (30), 12 months ormore.
Patients having reactive insertions were differentfrom those having prophylactic insertions (Table I) inregard to gender (relatively more men), age group(more elderly), primary treatment (more with surgerywithout free flaps), T stage (more early T1/T2 tumors),and tumor site (more laryngeal, less pharyngeal). Dataabout use were known for 86 of the 224 having pro-phylactic tubes, with 69% of tubes (59 of 86) beingused, 61% of users (33 of 54) being tube dependent,39% (21 of 54) of tubes being supplementary, and59% of tubes (29 of 49) being used for at least 6

Table III. Gastrostomy tubes and HRQOL asmeasured by the UWQOL
Gastrostomy tube
PNo (392)* Yes (163)*
% Overall QOLOutstanding 4% (14) 5% (8)Very good 32% (121) 26% (41)Good 35% (132) 29% (46) .05y
Fair 23% (87) 26% (42)Poor 6% (24) 11% (18)Very Poor 1% (4) 3% (4)Poor or very poor 7% (28/382) 14% (22/159) .02
UWQOL Physical subscale90-100 38% (149) 10% (17)80-89 16% (64) 6% (9)70-79 12% (47) 17% (28)60-69 15% (59) 16% (26)50-59 11% (44) 25% (41)<50 6% (25) 25% (41)Median (IQR) 82 (64-95),
n ¼ 38859 (49-74),n ¼ 162
<.001y
UWQOL Social-emotional subscale90-100 30% (116) 22% (36)80-89 21% (80) 13% (21)70-79 19% (75) 18% (29)60-69 11% (42) 16% (26)50-59 10% (40) 9% (14)<50 9% (35) 22% (36)Median (IQR) 82 (65-91),
n ¼ 38870 (53-88),n ¼ 162
<.001y
UWQOLz % “significant problem”
Appearance 8% (32/390) 13% (21/163) 0.11Swallowing 6% (25/391) 30% (48/161) <.001Chewing 6% (22/382) 20% (32/158) <.001Speech 6% (23/382) 16% (25/161) .001Taste 8% (32/385) 22% (35/157) <.001Saliva 19% (73/377) 40% (63/157) <.001Pain 14% (54/381) 25% (40/161) .004Activity 12% (48/387) 17% (27/159) .17Recreation 6% (24/381) 15% (24/160) .002Shoulder 9% (34/374) 11% (17/158) .63Mood 14% (52/383) 20% (33/163) .05Anxiety 14% (56/392) 23% (37/162) .02
HRQOL, health-related quality of life; UWQOL, University ofWashington Quality of Life Questionnaire; IQR, interquartile range.*N with UWQOL records if alive at 9 months; some item de-nominators were lower, because not all UWQOL returns werecomplete.yMann-Whitney test for overall QOL and subscale scores; otherwise,Fisher exact test.zSignificant problem trigger criteria as follows:Pain, appearance, activity, recreation, mood (scores of 0 or 25 or 50and important).Swallowing, speech, anxiety (scores of 0 or 30).Shoulder, taste, saliva (scores of 0 or 30 and important).Chewing (score of 0).
ORAL AND MAXILLOFACIAL SURGERY OOOO
554 Habib et al. May 2014
months. Corresponding data for reactive tubes wereknown for 43 of the 65, with 95% (41 of 43) beingused, 64% (23 of 36) of these being tube dependent,36% (13 of 36) supplementary, with 61% (22 of 36)used for at least 6 months.
In the 2012 survey of H&N cancer survivors, 28%(82 of 290) of this 2005-2009 cohort said that eitherthey had a feeding tube currently in place (n ¼ 11) or ithad been removed (n ¼ 71). For 44 patients, the medianduration of tube use was 6 months (IQR, 3-15 months).When asked about how much the tube was used tosupplement their food/nutrition, 15% (11) said “never,”11% (8) said “a little,” 26% (19) said “a lot,” and 48%(35) said “all the time.” For the 7 having both PEG andRIG, the gap between insertions was known for 4, withRIG being inserted 0 (same day), 3, 6, and 15 days afterinsertion of PEG.
Dietary assessment data within 4 months of diagnosisor surgical procedure were available for 78% (233 of299) of those with tubes and for 45% (293 of 648) ofthose without tubes. For these 526 assessments, weightwas known for 505, BMI for 383, and albumin for 397.There were significant differences seen in regard toBMI and albumin (Table II). Overall for this group withdietary assessments, 44% (233 of 526) had gastrostomytubes. In regard to weight, the percentage was 48%(57 of 118) for those under 60 kg, 48% (53 of 111)for those 60 to 69 kg, 43% (51 of 119) for those 70 to79 kg, and 40% (63 of 156) for 80 kg and heavier.Regarding BMI, the percentage was 50% (23 of 46) for<20, 50% (72 of 143) for 20 to 24, 40% (50 of 125) for25 to 29, and 33% (23 of 69) for 30 or above. Finallywith albumin, the percentage was 32% (25 of 77) for<30 g/L, 32% (24 of 74) for 30 to 34 g/L, 51% (40 of79) for 35 to 39 g/L, and 57% (95 of 167) for 40 g/Land above. The results were further stratified (seeTable II) for those with gastrostomy tubes into thosewho had used them and those who did not. Dataavailability was limited about usage (130 of 299 withtubes overall), and there were no notable differencesin weight, BMI, or albumin by whether tubes were usedor not.
Kaplan-Meier estimates for all-causes survival forthose having tubes were 82% (SE, 2%) at 12 months,65% (SE, 3%) at 24 months, and 45% (SE, 3%) at 60months; for those without, 85% (SE, 1%) at 12 months,76% (SE, 2%) at 24 months, and 61% (SE, 2%) at 60months (log-rank test; c2 ¼ 18.1; P < .001). In regardto HRQOL outcome, all patient UWQOL records be-tween 9 and 60 months were considered, with the re-cord closest to 24 months chosen for the analysis. Themedian time for the records analyzed was 24 months(IQR, 20-28 months) for both groups (gastrostomy tubeand no gastrostomy tube). If we factor in survival to 9months, then UWQOL records were available after 9
months for 64% (gastrostomy tube, 163 patients) and68% (no gastrostomy tube, 392 patients) of those aliveat 9 months. Those with tubes had worse HRQOL ataround 2 years after treatment, most notably in physicalfunctioning (Table III).

Table IV. Clinical factors and gastrostomy tubeinsertion
Patients (n) Gastrostomy tube P*
All patients 947 32% (299)GenderMale 659 35% (228) .002Female 288 25% (71)
Age (y)<55 233 43% (100) <.00155-69 453 34% (156)70þ 261 16% (43)
Primary treatmentSurgery and RT 292 43% (125) <.001Surgery alone 415 17% (70)Chemo/RT alone 240 43% (104)
Free flap (if surgery)No free flap 451 19% (85) <.001Soft 178 43% (77)Composite 78 42% (33)
T stageTis, T1 331 8% (27) <.001T2 294 36% (105)T3 72 49% (35)T4 237 55% (130)
N stageN0 622 19% (120) <.001N1 111 46% (51)N2-3 209 61% (127)
Overall clinical stage0-1 264 3% (9)2 196 26% (51)3 108 34% (37) <.0014 370 55% (202)
Tumor locationOral 412 20% (83) <.001Pharyngeal 242 58% (140)Laryngeal 210 21% (45)Other H&N 83 37% (31)
SpecialtyMFU 510 26% (134) <.001ENT 437 38% (165)
Year diagnosed2005 144 40% (58)2006 163 37% (60)2007 183 33% (60) .0022008 221 22% (48)2009 236 31% (73)
Tis, tumor in situ; H&N, head and neck;MFU, Aintree Maxillo FacialUnit; ENT, Aintree Ear Nose & Throat Department; RT, radiotherapy.*Fisher exact test for gender and specialty; otherwise, c2 test.
OOOO ORIGINAL ARTICLE
Volume 117, Number 5 Habib et al. 555
Placement of a gastrostomy tube was associated withseveral clinical and patient factors (Table IV). Alogistic regression analysis was performed to model theselection process, which leads to some patients beingexposed to gastrostomy tubes and others not so. Thecharacteristics of Table IV were considered jointlyin the regression model to predict gastrostomy tubeplacement, and 5 independent predictors were identi-fied at P < .001 in stepwise regression, these beingoverall clinical stage, tumor site, clinical T stage, pa-tient age group, and clinical N stage. A compositevariable for staging was created, as shown in Table V,and the regression was rerun, with 3 independent pre-dictors identified (the composite staging variable, tu-mor site, and age group). Predicted results performedwell against actual results by tumor staging and site(see Table V). The Nagelkerke pseudo-R2 statistic forthis predictor model was 0.40 excluding age group,increasing to 0.42 with age group. Predicted proba-bilities from the final model involving tumor staging,tumor site, and age were calculated and are given inTable VI for reference and potentially for use in afuture treatment protocol. For example, based on thehistorical data, the model computes a 65% chance ofa gastrostomy tube placement for a patient aged <55years with a T4N1 tumor of the oral cavity; 58% ifaged 55 to 69 years; and 36% if aged 70 or older.
Two patients had major procedure-related compli-cations (0.7%). On both occasions, the complicationswere identified immediately. One patient had splenicinjury during the procedure and required emergencysurgery; the second patient had intra-abdominal hema-toma due to laceration of the gastric wall, which wasmanaged conservatively and resolved spontaneouslywith good outcome. Ten patients (3.3%) had unplannedadmissions within 30 days of their procedure. Fourpatients were admitted within 7 days (1.3%). Reasonsfor readmission included displaced or blocked gastro-stomy tube (n ¼ 2) (0.7%), disease progression (n ¼ 2)(0.7%), gastrostomy site infection (n ¼ 3) (1.0%), andaspiration pneumonia secondary to alcohol excess(n ¼ 1) (0.3%). There have been no cases of tumorimplantation to date. Late displacement of the gastro-stomy tube (>30 days after insertion) was common(n ¼ 20) (6.7%). Most were replaced at the bedside.
DISCUSSIONThere is a clear rationale for gastrostomy tube place-ment in patients with H&N cancer; however, the mostappropriate means to select patients in an evidence-based protocol for prophylactic feeding tube placementseems controversial. The purpose of this study was toinvestigate which patients were having gastrostomytubes inserted as part of their primary treatment and touse this knowledge to inform the development of a
protocol. Data from this study need to be viewed withcaution, because they reflect one unit’s experience asdistilled from a retrospective case note review. Thesample does not represent the totality of new patientsdiscussed at the multidisciplinary team level. Also,there has been a change in treatment strategies at theUnit, with a higher proportion of patients havingtransoral laser or chemotherapy, and these 2 treatmentswere not adequately represented in the sample. We havenot used dysphagia at presentation or consistency of
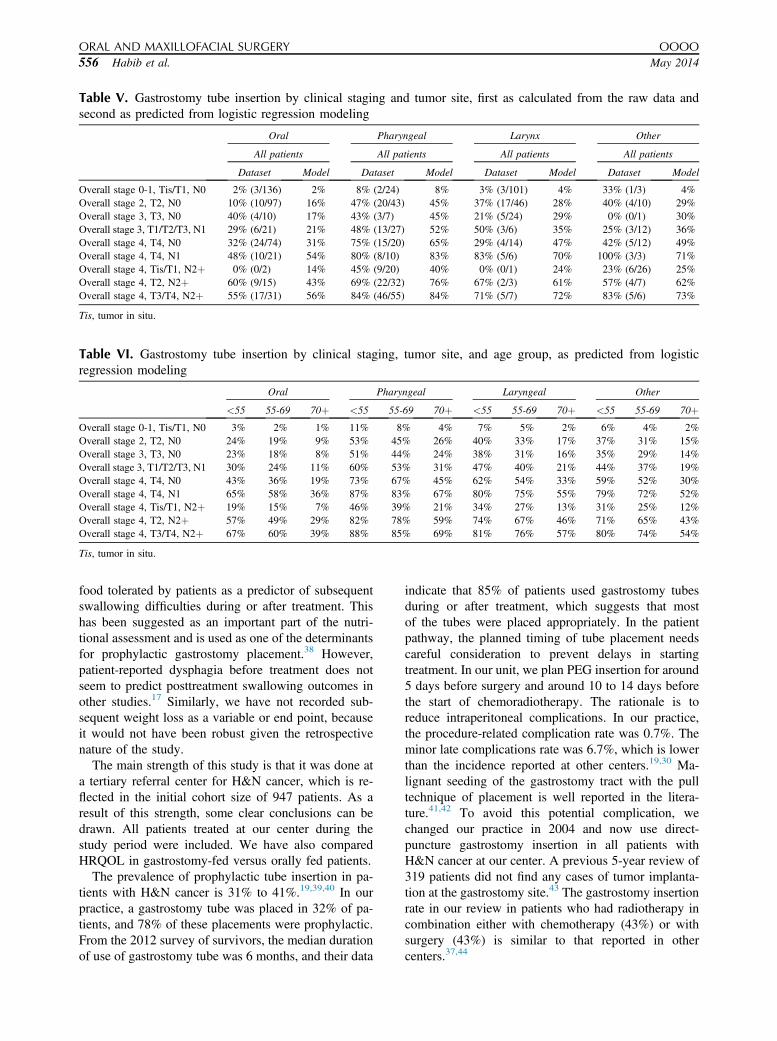
Table V. Gastrostomy tube insertion by clinical staging and tumor site, first as calculated from the raw data andsecond as predicted from logistic regression modeling
Oral Pharyngeal Larynx Other
All patients All patients All patients All patients
Dataset Model Dataset Model Dataset Model Dataset Model
Overall stage 0-1, Tis/T1, N0 2% (3/136) 2% 8% (2/24) 8% 3% (3/101) 4% 33% (1/3) 4%Overall stage 2, T2, N0 10% (10/97) 16% 47% (20/43) 45% 37% (17/46) 28% 40% (4/10) 29%Overall stage 3, T3, N0 40% (4/10) 17% 43% (3/7) 45% 21% (5/24) 29% 0% (0/1) 30%Overall stage 3, T1/T2/T3, N1 29% (6/21) 21% 48% (13/27) 52% 50% (3/6) 35% 25% (3/12) 36%Overall stage 4, T4, N0 32% (24/74) 31% 75% (15/20) 65% 29% (4/14) 47% 42% (5/12) 49%Overall stage 4, T4, N1 48% (10/21) 54% 80% (8/10) 83% 83% (5/6) 70% 100% (3/3) 71%Overall stage 4, Tis/T1, N2þ 0% (0/2) 14% 45% (9/20) 40% 0% (0/1) 24% 23% (6/26) 25%Overall stage 4, T2, N2þ 60% (9/15) 43% 69% (22/32) 76% 67% (2/3) 61% 57% (4/7) 62%Overall stage 4, T3/T4, N2þ 55% (17/31) 56% 84% (46/55) 84% 71% (5/7) 72% 83% (5/6) 73%
Tis, tumor in situ.
Table VI. Gastrostomy tube insertion by clinical staging, tumor site, and age group, as predicted from logisticregression modeling
Oral Pharyngeal Laryngeal Other
<55 55-69 70þ <55 55-69 70þ <55 55-69 70þ <55 55-69 70þOverall stage 0-1, Tis/T1, N0 3% 2% 1% 11% 8% 4% 7% 5% 2% 6% 4% 2%Overall stage 2, T2, N0 24% 19% 9% 53% 45% 26% 40% 33% 17% 37% 31% 15%Overall stage 3, T3, N0 23% 18% 8% 51% 44% 24% 38% 31% 16% 35% 29% 14%Overall stage 3, T1/T2/T3, N1 30% 24% 11% 60% 53% 31% 47% 40% 21% 44% 37% 19%Overall stage 4, T4, N0 43% 36% 19% 73% 67% 45% 62% 54% 33% 59% 52% 30%Overall stage 4, T4, N1 65% 58% 36% 87% 83% 67% 80% 75% 55% 79% 72% 52%Overall stage 4, Tis/T1, N2þ 19% 15% 7% 46% 39% 21% 34% 27% 13% 31% 25% 12%Overall stage 4, T2, N2þ 57% 49% 29% 82% 78% 59% 74% 67% 46% 71% 65% 43%Overall stage 4, T3/T4, N2þ 67% 60% 39% 88% 85% 69% 81% 76% 57% 80% 74% 54%
Tis, tumor in situ.
ORAL AND MAXILLOFACIAL SURGERY OOOO
556 Habib et al. May 2014
food tolerated by patients as a predictor of subsequentswallowing difficulties during or after treatment. Thishas been suggested as an important part of the nutri-tional assessment and is used as one of the determinantsfor prophylactic gastrostomy placement.38 However,patient-reported dysphagia before treatment does notseem to predict posttreatment swallowing outcomes inother studies.17 Similarly, we have not recorded sub-sequent weight loss as a variable or end point, becauseit would not have been robust given the retrospectivenature of the study.
The main strength of this study is that it was done ata tertiary referral center for H&N cancer, which is re-flected in the initial cohort size of 947 patients. As aresult of this strength, some clear conclusions can bedrawn. All patients treated at our center during thestudy period were included. We have also comparedHRQOL in gastrostomy-fed versus orally fed patients.
The prevalence of prophylactic tube insertion in pa-tients with H&N cancer is 31% to 41%.19,39,40 In ourpractice, a gastrostomy tube was placed in 32% of pa-tients, and 78% of these placements were prophylactic.From the 2012 survey of survivors, the median durationof use of gastrostomy tube was 6 months, and their data
indicate that 85% of patients used gastrostomy tubesduring or after treatment, which suggests that mostof the tubes were placed appropriately. In the patientpathway, the planned timing of tube placement needscareful consideration to prevent delays in startingtreatment. In our unit, we plan PEG insertion for around5 days before surgery and around 10 to 14 days beforethe start of chemoradiotherapy. The rationale is toreduce intraperitoneal complications. In our practice,the procedure-related complication rate was 0.7%. Theminor late complications rate was 6.7%, which is lowerthan the incidence reported at other centers.19,30 Ma-lignant seeding of the gastrostomy tract with the pulltechnique of placement is well reported in the litera-ture.41,42 To avoid this potential complication, wechanged our practice in 2004 and now use direct-puncture gastrostomy insertion in all patients withH&N cancer at our center. A previous 5-year review of319 patients did not find any cases of tumor implanta-tion at the gastrostomy site.43 The gastrostomy insertionrate in our review in patients who had radiotherapy incombination either with chemotherapy (43%) or withsurgery (43%) is similar to that reported in othercenters.37,44

OOOO ORIGINAL ARTICLE
Volume 117, Number 5 Habib et al. 557
Pretreatment weight loss has been described as thestrongest predictor of survival in patients with H&Ncancer.45 We recorded weight, BMI, and albumin atpresentation in anticipation of indicating the degreeof malnutrition and learning whether it showed differ-ences in the physician’s choice of patients for prophy-lactic PEG. There was a differential loss of nutritionalinformation according to the use of a gastrostomy tube,which could compromise any comparisons made. Theavailable results do not suggest that these variableshave much clinical relevance, despite differences inBMI and albumin reaching statistical significance.
Among the well-established factors associated withthe requirement of nutritional support during treatmentof H&N cancer are tumor location, T stage, N stage,chemoradiotherapy, and type of surgery.46-50 Our studyfound these factors to be statistically significant de-terminants and predictors of gastrostomy insertion. Thecombination of these factors is known to cause long-term swallowing dysfunction, necessitating ongoingnutritional support.15,51-53 Based on our findings, wesuggest a protocol that will act as a guideline for con-sidering nutritional management of patients with H&Ncancer who are being treated with curative intent. Thelogistic regression analysis strongly supports the in-clusion of stage, site, and age as independent predictors.Interestingly, treatment modality, inherently a strongpredictor did not come through as an independentpredictor. This is of minimal concern while developinga protocol, because treatment is strongly related to,and included within, stage and site. Focusing on stage,site, and age means that it is possible to adopt a moreflexible approach. Our protocol allows individualjudgments to be made in terms of patient selection,rather than having a dogmatic strategy of offering agastrostomy tube to all patients having chemotherapy.Another aspect for consideration is patient difficulty inswallowing at presentation (dysphagia), and again,rather than include it as a patient-reported indicator in aprotocol, we suggest that dysphagia is also reflectedwithin stage and site. Age does appear to be an inde-pendent predictor, and this is really pertinent, becausethe oldest elderly patients are going to be less able totolerate aggressive treatments, such as free flaps orchemotherapy. The protocol as highlighted in Table VIcan form the basis on which discussions are held aboutthe relative importance of other factors. For example,T4N2, oral, age 55 to 69 has a figure of 60%, whichindicates historically that just over half of such patientshad a tube placed. Other information, such as BMI,weight loss, excessive alcohol use, comorbidity, andpatient preference, could either increase or decrease thelikelihood of placement. If one preferred to run a pro-tocol based on staging and site without age, then themodel values from Table V would provide the figures
for guidance. There are other protocols in existence,such as the KAREN scoring system,54 and although thisincludes the American Society of Anesthesiologistsphysical status class, alcohol consumption, and numberof regular medications, our protocol is probably basedon stronger predictors, whereby these other issues helpinform decision making on an individual-patient basis.
CONCLUSIONOur data indicate key predictors of gastrostomy place-ment. At Aintree hospitals, we now recommend thatpatients should be strongly considered for a gastro-stomy if their likelihood of placement is estimated toexceed 50%. A prospective audit is planned to allowrefinement of this protocol.
We thank members of the Aintree Head and Neck OncologyGroup for their advice during the preparation of this articleand for allowing the reporting of patients under their care. Wethank the Clinical Audit Department for their help in case noteretrieval.
REFERENCES1. Price G, Roche M, Wight R, Crowther R; Oxford Cancer Intel-
ligence Unit; NCIN Head and Neck Cancers Site Specific ClinicalReference Group. Profile of head and neck cancers in England:secular and geographical trends in the incidence, mortality andsurvival of laryngeal and oropharyngeal cancers. London,England: Solutions for Public Health; 2010.
2. Rogers SN, Brown JS, Woolgar JA, et al. Survival followingprimary surgery for oral cancer. Oral Oncol. 2009;45:201-211.
3. Rogers SN, Humphris G, Lowe D, et al. The impact of surgery fororal cancer on quality of life as measured by the Medical Out-comes Short Form 36. Oral Oncol. 1998;34:171-179.
4. Hillman RE, Walsh MJ, Wolf GT, Fisher SG, Hong WK. Func-tional outcomes following treatment for advanced laryngeal can-cer. Ann Otol Rhinol Laryngol. 1998;107:2-27.
5. Murry T, Madasu R, Martin A, Robbins KT. Acute and chronicchanges in swallowing and quality of life following intra-arterialchemoradiation for organ preservation in patients with advancedhead and neck cancer. Head Neck. 1998;20:31-37.
6. Newman LA, Vieira F, Schwiezer V, et al. Eating and weightchanges following chemoradiation therapy for advanced headand neck cancer. Arch Otolaryngol Head Neck Surg. 1998;124:589-592.
7. Lazarus CL, Logemann JA, Pauloski BR, et al. Swallowing dis-orders in HNC patients treated with radiotherapy and adjuvantchemotherapy. Laryngoscope. 1996;106:1157-1166.
8. Dejanger E, Goethals P. Deglutition disorder as a late sequel ofradiotherapy for a pharyngeal tumor. Am J Gastroenterol.1994;90:493-495.
9. Kotz T, Abraham S, Beitler J, Wadler S, Smith RV. Pharyngealtransport dysfunction consequent to an organ-sparing protocol.Arch Otolaryngol Head Neck Surg. 1999;125:410-413.
10. Mittal BB, Pauloski BR, Haraf DJ, et al. Swallowing dysfunc-tiondpreventative and rehabilitation strategies in patients withhead and neck cancers treated with surgery, radiotherapy, andchemotherapy: a critical review. Int J Radiat Oncol Biol Phys.2003;57:1219-1230.
11. Rustom IK, Jebreel A, Tayyab M, England RJ, Stafford ND.Percutaneous endoscopic, radiological and surgical gastrostomy

ORAL AND MAXILLOFACIAL SURGERY OOOO
558 Habib et al. May 2014
tubes: a comparison in head and neck cancer patients. J LaryngolOtol. 2006;120:463-466.
12. Abitbol A, Abdei-Wahab M, Harvey M, et al. Phase II study oftolerance and efficacy of hyperfractionated radiation therapy and5-fluorouracil, cisplatin, and paclitaxel (taxol) and amifostine(ethyol) in head and neck squamous cell carcinomas: a-3 protocol.Am J Clin Oncol. 2005;28:449-455.
13. Goguen LA, Posner MR, Norris CM, et al. Dysphagia aftersequential chemoradiation therapy for advanced head and neckcancer. Otolaryngol Head Neck Surg. 2006;134:916-922.
14. Cheng SS, Terrell JE, Bradford CR, et al. Variables associatedwith feeding tube placement in head and neck cancer. ArchOtolaryngol Head Neck Surg. 2006;132:655-661.
15. Garden AS, Harris J, Trotti A, et al. Long-term results ofconcomitant boost radiation plus concurrent cisplatin for advancedhead and neck carcinomas: a phase II trial of the Radiation TherapyOncology Group (RTOG 99-14). Int J Radiat Oncol Biol Phys.2008;71:1351-1355.
16. Lees J. Nasogastric and percutaneous endoscopic gastrostomyfeeding in head and neck cancer patients receiving radiotherapytreatment at a regional oncology unit: a two year study. Eur JCancer Care (Engl). 1997;6:45-49.
17. Hutcheson KA, Barringer DA, Rosenthal DI, May AH,Roberts DB, Lewin JS. Swallowing outcomes after radiotherapyfor laryngeal carcinoma. Arch Otolaryngol Head Neck Surg.2008;134:178-183.
18. National Institute for Clinical Excellence. Nutritional support inadults: oral nutrition support, enteral tube feeding and parenteralnutrition. London, England: National Institute for ClinicalExcellence; February 2006.
19. Raykher A, Correa L, Russo L, et al. The role of pre-treatmentpercutaneous endoscopic gastrostomy in facilitating therapy ofhead and neck cancer and optimizing the body mass index of theobese patient. JPEN J Parenter Enteral Nutr. 2009;33:404-410.
20. Nguyen NP, North D, Smith HJ, et al. Safety and effectiveness ofprophylactic gastrostomy tubes for head and neck cancer patientsundergoing chemoradiation. Surg Oncol. 2006;15:199-203.
21. Beaver ME, Matheny KE, Roberts DB, Myers JN. Predictors ofweight loss during radiation therapy. Otolaryngol Head NeckSurg. 2001;125:645-648.
22. Corry J, Poon W, McPhee N, et al. Prospective study of percu-taneous endoscopic gastrostomy tubes versus nasogastric tubesfor enteral feeding in patients with head and neck cancer under-going (chemo)radiation. Head Neck. 2009;31:867-876.
23. Mekhail TM, Adelstein DJ, Rybicki LA, Larto MA, Saxton JP,Lavertu P. Enteral nutrition during the treatment of head and neckcarcinoma: is a percutaneous endoscopic gastrostomy tube pref-erable to a nasogastric tube? Cancer. 2001;91:1785-1790.
24. Paleri V, Patterson J. Use of gastrostomy in head and neck cancer:a systematic review to identify areas for future research. ClinOtolaryngol. 2010;35:177-189.
25. Madhoun MF, Blankenship MM, Blankenship DM, Krempl GA,Tierney WM. Prophylactic PEG placement in head and neckcancer: how many feeding tubes are unused (and unnecessary)?World J Gastroenterol. 2011;17:1004-1008.
26. Roberge C, Tran M, Massoud C, et al. Quality of life and homeenteral tube feeding: a French prospective study in patients withhead and neck or oesophageal cancer. Br J Cancer. 2000;82:263-269.
27. Ringash J, Lockwood G, O’Sullivan B, et al. Hyperfractionated,accelerated radiotherapy for locally advanced head and neckcancer: quality of life in a prospective phase I/II trial. RadiotherOncol. 2008;87:181-187.
28. Rogers SN, Thomson R, O’Toole P, Lowe D. Patients experiencewith long-term percutaneous endoscopic gastrostomy feeding
following primary surgery for oral and oropharyngeal cancer.Oral Oncol. 2007;43:499-507.
29. Ahmed KA, Samant S, Vieira F. Gastrostomy tubes in patientswith advanced head and neck cancer. Laryngoscope. 2005;115:44-47.
30. McLaughlin BT, Gokhale AS, Shuai Y, et al. Management ofpatients treated with chemoradiotherapy for head and neck cancerwithout prophylactic feeding tubes: the University of Pittsburghexperience. Laryngoscope. 2010;120:71-75.
31. Orphanidou C, Biggs K, Johnston ME, et al. Prophylactic feedingtubes for patients with locally advanced head-and-neck cancerundergoing combined chemotherapy and radiotherapydsystematicreview and recommendations for clinical practice. Curr Oncol.2011;18:e191-e201.
32. Locher JL, Bonner JA, Carroll WR, et al. Prophylactic percuta-neous endoscopic gastrostomy tube placement in treatment of headand neck cancer: a comprehensive review and call for evidence-based medicine. JPEN J Parenter Enteral Nutr. 2011;35:365.
33. Nugent B, Lewis S, O’Sullivan JM. Enteral feeding methods fornutritional management in patients with head and neck cancersbeing treated with radiotherapy and/or chemotherapy. CochraneDatabase Syst Rev. 2010;CD007904.
34. Moor JW, Patterson J, Kelly C, Paleri V. Prophylactic gastro-stomy before chemoradiation in advanced head and neck cancer:a multi-professional web-based survey to identify current practiceand to analyse decision making. Clin Oncol (R Coll Radiol).2010;22:192-198.
35. Laraway DC, Rogers SN. A structured review of journal articlesreporting outcomes using the University of Washington Qualityof Life Scale. Br J Oral Maxillofac Surg. 2012;50:122-131.
36. Rogers SN, Lowe D, Yueh B, Weymuller EA. The physicalfunction and social-emotional function subscales of the Univer-sity of Washington Quality of Life Questionnaire. Arch Otolar-yngol Head Neck Surg. 2010;136:352-357.
37. Rogers SN, Lowe D. Screening for dysfunction to promotemultidisciplinary intervention by using the University of Wash-ington Quality of Life Questionnaire. Arch Otolaryngol HeadNeck Surg. 2009;135:369-375.
38. Jack DR, Dawson FR, Reilly JE, Shoaib T. Guideline for pro-phylactic feeding tube insertion in patients undergoing resectionof head and neck cancers. J Plast Reconstr Aesthet Surg. 2012;65:610-615.
39. Mangar S, Slevin N, Mais K, Sykes A. Evaluating predictivefactors for determining enteral nutrition in patients receivingradical radiotherapy for head and neck cancer: a retrospectivereview. Radiother Oncol. 2006;78:152-158.
40. Lee JH, Machtay M, Unger LD, et al. Prophylactic gastrostomytubes in patients undergoing intensive irradiation for cancer of thehead and neck. Arch Otolaryngol Head Neck Surg. 1998;124:871-875.
41. Adelson RT, Ducic Y. Metastatic head and neck carcinoma to apercutaneous endoscopic gastrostomy site. Head Neck. 2005;27:339-343.
42. Volkmer K, Meyer T, Sailer M, Fein M. Metastasis of anesophageal carcinoma at a PEG sitedcase report and review ofthe literature. Zentralbl Chir. 2009;134:481-485.
43. Ahmed S, Bowering K, Polavarapu N, Nicholson R, Thomas P,Sturgess R. PEXACT: analysis of 319 procedures performed atthe Digestive Diseases Unit, University Hospital Aintree. Gut.2010;59:A143.
44. Rabinovitch R, Grant B, Berkey BA, et al. Impact of nutritionalsupport on treatment outcome in patients with locally advancedhead and neck squamous cell cancer treated with definitiveradiotherapy: a secondary analysis of RTOG trial 90-03. HeadNeck. 2006;28:287-296.

OOOO ORIGINAL ARTICLE
Volume 117, Number 5 Habib et al. 559
45. Mick R, Vokes EE, Weichselbaum RR, Panje WR. Prognostic fac-tors in advanced head and neck cancer patients undergoing multi-modality therapy. Otolaryngol Head Neck Surg. 1991;105:62-73.
46. Gardine RL, Kokal WA, Beatty JD, et al. Predicting the need forprolonged enteral supplementation in the patient with head andneck cancer. Am J Surg. 1988;156:63-65.
47. Ishiki H, Onozawa Y, Kojima T, et al. Nutrition support for headand neck squamous cell carcinoma patients treated with chemo-radiotherapy: how often and how long? ISRN Oncol. 2012;2012:274739.
48. Anwander T, Berge S, Appel T, et al. Percutaneous endoscopicgastrostomy for long-term feeding of patients with oropharyngealtumors. Nutr Cancer. 2004;50:40-45.
49. Thiel HJ, Fietkau R, Sauer R. Malnutrition and the role ofnutritional support for radiation therapy patients. Recent ResultsCancer Res. 1988;108:205-226.
50. Schweinfurth JM, Boger GN, Feustel PJ. Preoperative riskassessment for gastrostomy tube placement in head and neckcancer patients. Head Neck. 2001;23:376-382.
51. Nguyen NP, Moltz CC, Frank C, et al. Dysphagia followingchemoradiation for locally advanced head and neck cancer. AnnOncol. 2004;15:383-388.
52. Murphy BA, Gilbert J. Dysphagia in head and neck cancer pa-tients treated with radiation: assessment, sequelae, and rehabili-tation. Semin Radiat Oncol. 2009;19:35-42.
53. Caudell JJ, Schaner PE, Meredith RF, et al. Factors associatedwith long-term dysphagia after definitive radiotherapy for locallyadvanced head-and-neck cancer. Int J Radiat Oncol Biol Phys.2009;73:410-415.
54. Eley KA, Shah R, Bond SE, Watt-Smith SR. A review ofpostoperative feeding in patients undergoing resection andreconstruction for oral malignancy and presentation of a pre-operative scoring system. Br J Oral Maxillofac Surg. 2012;50:601-605.
Reprint requests:
Simon N. Rogers, FDSRCS, FRCS, MDConsultant in Oral & Maxillofacial SurgeryRegional Head and Neck DepartmentAintree University HospitalLiverpool L9 7ALUnited [email protected]





























