Embed Size (px)
Citation preview
Developing Evidence-based, Pressure-tested Programs for Your Clients 1
Presented by Cedric X. Bryant, Ph.D., FACSM
Chief Science Officer2/3/2018
Getting people moving
Developing Evidence-based, Pressure-tested Programs for Your Clients with Hypertension

Developing Evidence-based, Pressure-tested Programs for Your Clients 2
Discuss new BP guidelines and their implications
Review the pathophysiology and complications of hypertension (HTN)
Describe the treatment options for HTN with a specific focus on effective lifestyle
intervention strategies (weight loss, nutrition, & physical activity)
Provide a brief overview of the pharmacologic treatment options
Discuss behavior-change strategies for driving program success
Ground rules (Questions & Slides)
Presentation ObjectivesPresentation Outline

Developing Evidence-based, Pressure-tested Programs for Your Clients 3
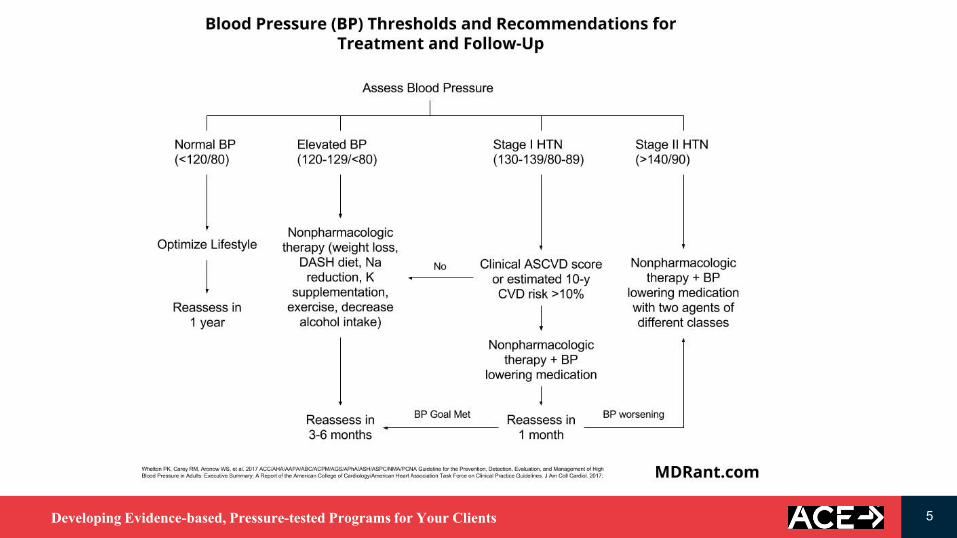
New Categories of BP in Adults*
BP Category SBP DBP
Normal <120 mm Hg and <80 mm Hg
Elevated 120–129 mm
Hg
and <80 mm Hg
Hypertension
Stage 1 130–139 mm
Hg
or 80–89 mm Hg
Stage 2 ≥140 mm Hg or ≥90 mm Hg
*Individuals with SBP and DBP in 2 categories should be
designated to the higher BP category.

Developing Evidence-based, Pressure-tested Programs for Your Clients 4
Prevalence of Hypertension Based on 2 SBP/DBP Thresholds
SBP/DBP ≥130/80 mm Hg or
Self-Reported Antihypertensive
Medication
SBP/DBP ≥140/90 mm Hg or Self-
Reported Antihypertensive
Medication
Overall, crude 46% 32%
Men
(n=4717)
Women
(n=4906)
Men
(n=4717)
Women
(n=4906)
Overall, age-sex
adjusted
48% 43% 31% 32%
Age group, years
20–44 30% 19% 11% 10%
45–54 50% 44% 33% 27%
55–64 70% 63% 53% 52%
65–74 77% 75% 64% 63%
75+ 79% 85% 71% 78%
Race-ethnicity
Non-Hispanic White 47% 41% 31% 30%
Non-Hispanic Black 59% 56% 42% 46%
Non-Hispanic Asian 45% 36% 29% 27%
Hispanic 44% 42% 27% 32%
Developing Evidence-based, Pressure-tested Programs for Your Clients 5
BP Thresholds & Recommendations for Treatment and Follow-
Up (continued on next slide)

Developing Evidence-based, Pressure-tested Programs for Your Clients 6
Basic Pathophysiology of Hypertension

Developing Evidence-based, Pressure-tested Programs for Your Clients 7
The Role of Shear Stress In Atherogenesis
Developing Evidence-based, Pressure-tested Programs for Your Clients 8
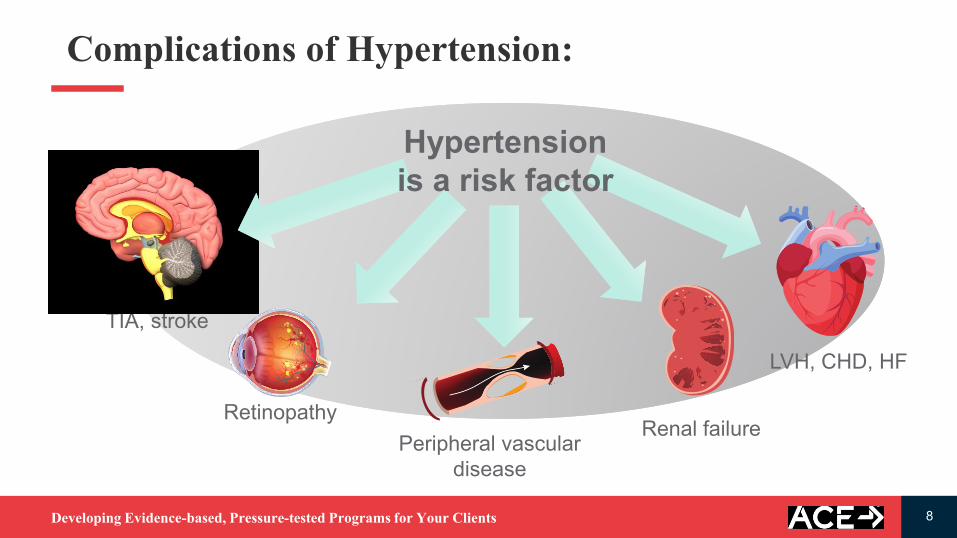
Complications of Hypertension:
TIA, stroke
Retinopathy
Peripheral vascular
disease
Renal failure
LVH, CHD, HF
Hypertension
is a risk factor

Developing Evidence-based, Pressure-tested Programs for Your Clients 9
Impact of a Modest (5 mmHg) Decrease in BP
ReductionOverall Risk Reduction
Stroke (CVA) 14%
Coronary Heart Disease 9%
All Cause Mortality 7%
Developing Evidence-based, Pressure-tested Programs for Your Clients 10
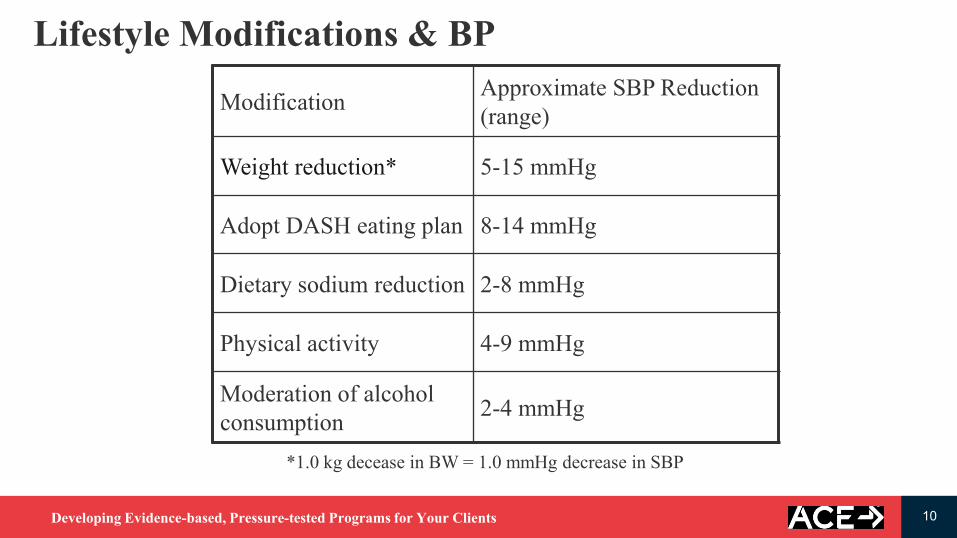
Lifestyle Modifications & BP
ModificationApproximate SBP Reduction
(range)
Weight reduction* 5-15 mmHg
Adopt DASH eating plan 8-14 mmHg
Dietary sodium reduction 2-8 mmHg
Physical activity 4-9 mmHg
Moderation of alcohol
consumption2-4 mmHg
*1.0 kg decease in BW = 1.0 mmHg decrease in SBP

Developing Evidence-based, Pressure-tested Programs for Your Clients 11
Weight Loss
Diet/NutritionPA/Exercise
Lifestyle
Change
Behavior
First Line of Defense: Lifestyle Behavior Change

Developing Evidence-based, Pressure-tested Programs for Your Clients 12
Energy Intake vs Energy Expenditure: No Contest
Large burger 3 540 180
Activity Duration Cost Efficiency
(min) (kcal) (kcal/min)
70% VO2max 60 540 9
40% VO2max 90 540 6
Vs.

Developing Evidence-based, Pressure-tested Programs for Your Clients 13
It’s Simply A Question Of Energy Balance ???

Developing Evidence-based, Pressure-tested Programs for Your Clients 14
Wei
ght
Cha
nge
(kg)
-6
-4
-2
0
2
4
6
8
10
12
14
Women
Increased Physical Activity & BW Change
✓ BW decreases
✓ BW does not change
✓ BW increases
Why variability of responses?

Developing Evidence-based, Pressure-tested Programs for Your Clients 15
Theory: Reduced Daily Energy Expenditure Pattern

Developing Evidence-based, Pressure-tested Programs for Your Clients 16
Washburn et al. Clinical Obesity, Feb 2014
No reductions in non-exercise
activity thermogenesis (NEAT) in
response to prescribed physical
activity/exercise training
✓ 100% of cross-sectional studies
(n=4)
✓ 90% of short-term studies (n=10)
✓ 50% of non-randomized trials
(n=10)
✓ 100% of randomized controlled
trials (n=7)
NEAT Appears To Be Unchanged
Developing Evidence-based, Pressure-tested Programs for Your Clients 17
Theory: Physical Activity and Appetite Control
PA has the potential to adjust appetite control by:
✓ Improving the sensitivity of the physiological satiety signaling system
✓Adjusting macronutrient preferences or food choices
✓Altering the hedonic (pleasurable) response to food
Available research suggests that individuals can be separated in two
groups:
✓Compensators and non-compensators.
✓More studies are needed to further classify individuals who are
compensators vs non-compensators & to identify the mechanisms
responsible for the rates of compensation and its limits.
Developing Evidence-based, Pressure-tested Programs for Your Clients 18
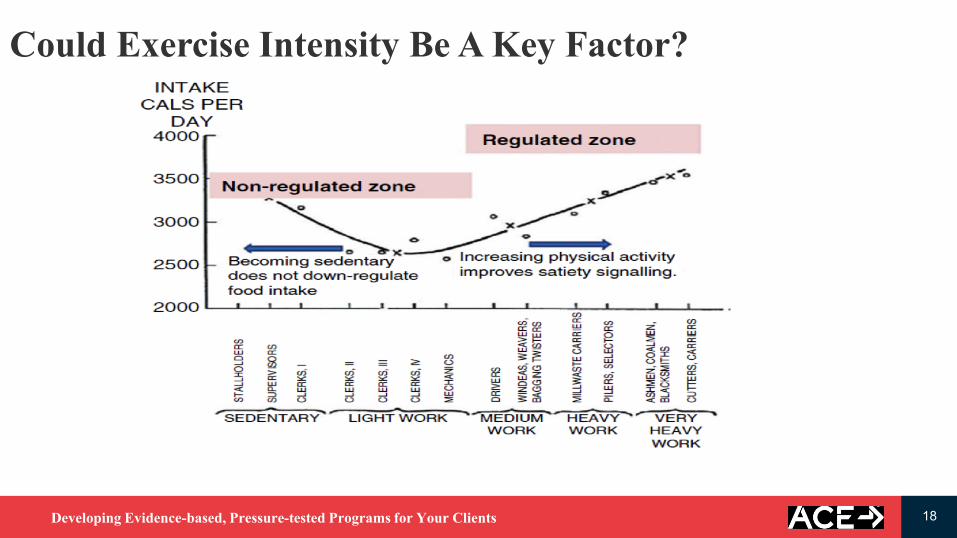
Could Exercise Intensity Be A Key Factor?

Developing Evidence-based, Pressure-tested Programs for Your Clients 19
Don’t Forget The Rest Of The Story: What Would We
Miss If We Choose To Focus On Food Alone?
Improved overall cardiometabolic health
Enhanced weight maintenance
Enhanced mood and psychological outlook
Improved physical functioning
Improved cognitive functioning
Always Think Total Impact!

Developing Evidence-based, Pressure-tested Programs for Your Clients 20
NWCR: Learning from Successful Losers
Slow & steady = long-term success
Eat early, diet late (food = fuel for an active, healthy lifestyle)
Practice mindful eating (Brian Wansink)
Choose a lower-fat (<25% fat) eating plan
Consume foods high in nutrient density (nutrients per calorie of food)
Consume foods low in energy density (calories per weight or volume of food)
Limit alcohol consumption (7 kcal/g)

Developing Evidence-based, Pressure-tested Programs for Your Clients 21
NWCR: Learning from Successful Losers (cont.)
Eat consistently, and maintain the same eating patterns on weekends as on weekdays
Weigh themselves regularly but not obsessively
Get sufficient amounts of sleep
Accumulate about an hour of moderate-intensity physical activity on most days
Combo of weightbearing and non-weightbearing activity is encouraged

Developing Evidence-based, Pressure-tested Programs for Your Clients 22
Regions of Abdominal Fat:
1. Subcutaneous
2. Visceral
A Important Exercise Target: Abdominal Visceral Fat

Developing Evidence-based, Pressure-tested Programs for Your Clients 23
Weight Loss
Diet/NutritionPA/Exercise
Lifestyle
Change
Behavior
First Line of Defense: Lifestyle Behavior Change

Developing Evidence-based, Pressure-tested Programs for Your Clients 24
Exercise professionals should have knowledge of the
following nutrition-related concepts when working with
clients who have HTN:
✓ Dietary Approaches to Stopping Hypertension
(DASH) eating plan
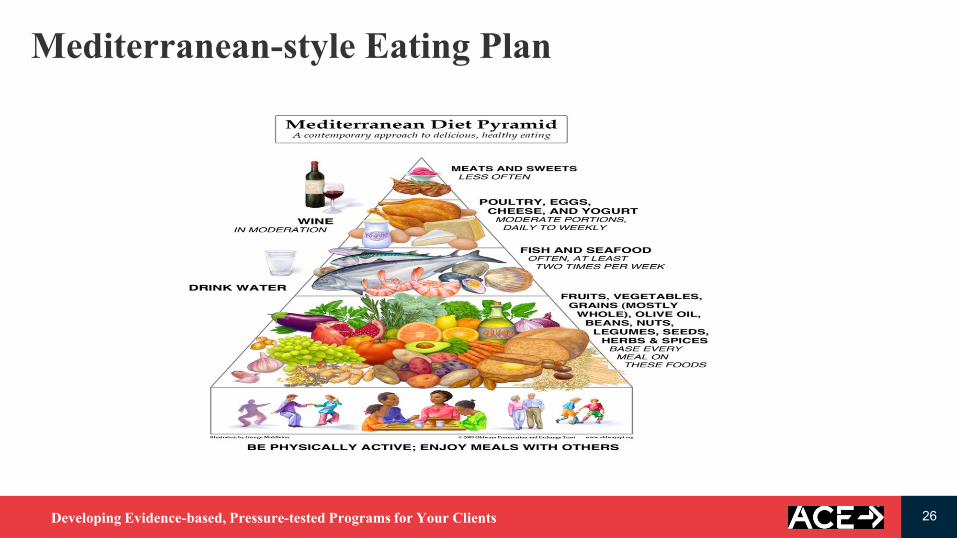
✓ Mediterranean-style eating plan
✓ Diets advocating excessive restriction of certain
macronutrients are likely inadequate and typically are
not adhered to over the long term
HTN: Diet/Nutrition ConsiderationsNutrition Essentials & Hypertension

Developing Evidence-based, Pressure-tested Programs for Your Clients 25
DASH Eating Plan
✓Emphasizes fruits, vegetables,
grains, seafood, poultry, lean
meats, and low-fat diary products
✓Low in saturated fat, cholesterol,
and total fat
✓Reduced red meat, sweets, and
sugary beverages
✓Low in sodium (< 2300 or 1500
mg per day)
✓Rich in magnesium, potassium,
calcium, protein, and fiber
Developing Evidence-based, Pressure-tested Programs for Your Clients 26
Mediterranean-style Eating Plan
Developing Evidence-based, Pressure-tested Programs for Your Clients 27
What the real scoop on sodium?✓Sodium raises BP in some people
(Sodium sensitivity: 25 – 35% of
population)
▪ Older adults
▪ Blacks
▪ Overweight/obesity
✓All individuals with HTN should
limit sodium intake
✓Sodium is found in many foods
in the grocery store (Read food
labels!)
✓Physical activity has been
associated with a reduction in
sodium sensitivity

Developing Evidence-based, Pressure-tested Programs for Your Clients 28
Help Your Clients with Portion Control
Developing Evidence-based, Pressure-tested Programs for Your Clients 29
Nutrition & The Exercise Professional
Don’t be afraid to talk nutrition with your clients (disseminate credible,
evidence-based information:
(www.eatright.org,www.heart.org,www.acefitness.org)
Provide evidence-based information and industry-accepted guidelines
but not individualized or personal recommendations Empower
clients with valid info to make healthy nutrition choices
When discussing nutrition, ask yourself: “Is this within my defined
professional boundaries, expertise and skills?”
Respect scope of practice and refer when needed

Developing Evidence-based, Pressure-tested Programs for Your Clients 30
Weight Loss
Diet/NutritionPA/Exercise
Lifestyle
Change
Behavior
First Line of Defense: Lifestyle Behavior Change

Developing Evidence-based, Pressure-tested Programs for Your Clients 31
Frequency: 4-5 days/week, preferably daily
Intensity: Zone 1 with brief periods in Zone 2—using
ACE 3-Zone Model
Time: 30-60 min/session
Type: Low-impact aerobic exercise supplemented by
an increased NEAT
Cardio Exercise Programming Guidelines (FITT)

Developing Evidence-based, Pressure-tested Programs for Your Clients 32
Post-exercise hypotensive
(PEH) response:
Transient reduction in BP
immediately after PA—typically
5 – 20 mmHg compared to pre-
exercise levels
Why is daily cardio activity the preferred recommendation

Developing Evidence-based, Pressure-tested Programs for Your Clients 33
Frequency: 4-5 days/week, preferably daily
Intensity: Zone 1 with brief periods in Zone 2—using
ACE 3-Zone Model (40 – 70% HRR)
Time: 30-60 min/session
Type: Low-impact aerobic exercise supplemented by
an increased NEAT
Cardio Exercise Programming Guidelines (FITT)

Developing Evidence-based, Pressure-tested Programs for Your Clients 34
During exercise, higher intensities
increase respiratory rates linearly with
the exception of two key deflection
points where significant ventilatory
changes occur:
VT1 - First Ventilatory Threshold -
due to increased CO2 production as
primary fuel utilized changes (fat
carbohydrate); corresponds with initial
accumulation of blood lactate
VT2 - Second Ventilatory Threshold -
associated with a rapid increase in
blood lactate (lactate > 4.0 mmol)
Ventilatory Markers & Exercise Intensity

Developing Evidence-based, Pressure-tested Programs for Your Clients 35
Zone 1 Zone 2 Zone 3
VT1 VT2
VT1 & VT2
Below VT1 VT1 to just below VT2 VT2 and Above
HR HR < VT1 HR > VT1 to HR < VT2 HR > VT2
Talk Test Can talk comfortablyNot sure if talking is
comfortable
Definitely cannot talk
comfortably
RPE Terms
Moderate to Somewhat hard Hard Very hard to Extremely hard
RPE 3 – 4 or 12 – 13 5 – 6 or 14 – 16 7 – 10 or 17 – 20
Cardio Exercise Intensity: ACE 3-Zone Model

Developing Evidence-based, Pressure-tested Programs for Your Clients 36
Frequency: 4-5 days/week, preferably daily
Intensity: Zone 1 with brief periods in Zone 2—using
ACE 3-Zone Model (40 – 70% HRR)
Time: 30-60 min/session
Type: Low-impact aerobic exercise supplemented by
increased NEAT
Cardio Exercise Programming Guidelines (FITT)

Developing Evidence-based, Pressure-tested Programs for Your Clients 37
Make Movement Your Mission: Tips for Increasing NEAT

Developing Evidence-based, Pressure-tested Programs for Your Clients 38
Frequency: 2 days/week, focused on major muscles
Intensity: Think MED until stability, mobility, & proper
movement mechanics are achieved; RPP
Repetitions: Generally, vary inversely with intensity
Sets: One set/multiple sets; experience & preference
Type: Variety of options; experience & preference
Resistance Exercise Programming Guidelines (FIRST)

Developing Evidence-based, Pressure-tested Programs for Your Clients 39
Rate Pressure Product (RPP) = SBP x HR / 100
SBP = Systolic blood pressure
HR = Heart rate
Resistance Exercise & Myocardial Oxygen Demand

Developing Evidence-based, Pressure-tested Programs for Your Clients 40
Relative load (% 1RM)Single-arm curl ( ), single-leg press ( ), and double-leg pressure ( )
RPP
250240230220210200190180170160150140
20 40 60 80
60%
85%
100%
RPP Response to Difference Types of Exercises

Developing Evidence-based, Pressure-tested Programs for Your Clients 41
Frequency: 2-3 days/week, particularly for relative beginners
Intensity: Think MED until stability, mobility, & proper
movement mechanics are achieved; RPP
Repetitions: Generally, vary inversely with intensity
Sets: One set/multiple sets; experience & preference
Type: Variety of options; experience & preference
Resistance Exercise Programming Guidelines (FIRST)

Developing Evidence-based, Pressure-tested Programs for Your Clients 42
Limited body of research with promising results
Lowers BP to a similar degree as steady-state exercise
Other potential benefits have been observed:
✓ Increased nitric oxide response (endothelial function)
✓ Increased pulse wave velocity (arterial stiffness)
Extend warm-up & cool-down periods
Exercise greater caution with poorly controlled, older (>
50 years) or long-standing (> 10 years) HTN clients
regardless of their age
HITT & Hypertension

Developing Evidence-based, Pressure-tested Programs for Your Clients 43
Keep cardio activity below Zone 2 regardless of fitness level
(exception: athlete with approval from medical provider)
Resistance training is important for functional performance
Mind-body activities can be integrated (caution with certain postures)
Understand the effect of meds on exercise responses
Be aware of environmental stressors
Know the signs of a cardiac problem
Special Exercise Considerations & Precautions

Developing Evidence-based, Pressure-tested Programs for Your Clients 44
Does the pain get better or worse with a change in body position?
Is the pain better or worse with respirations?
Is the pain intense, knifelike, or more like a dull ache or pressure?
Is the pain deep or close to the surface?
Is the pain associated with other symptoms like difficulty breathing,
nausea or sweating?
Is the pain diffuse or localized?
Cardiac vs Non-cardiac Chest Pain
If in doubt, treat it as cardiac chest pain

Developing Evidence-based, Pressure-tested Programs for Your Clients 45
Improved BP control
Reduced rate and severity of complications
Reduced dosage of medication required to control BP (Health & Financial +)
Improved CHD risk factor profile
Enhanced mood and psychological status
Improved cognitive health and function
Improved overall quality of life
Exercise & Hypertension: The Benefits

Developing Evidence-based, Pressure-tested Programs for Your Clients 46
Pharmacologic Sites of Action
Diuretics
Aldosterone Ant.
Nitrates
ACE Inhibitors
ARBs
Beta Blockers
Ca+ Channel
Blockers
Alpha 2 Blockers
Vasodilators
Ca+ Channel
Blockers
Alpha 1 Blockers
ACEI
ARB
HeartArteries
Veins
Note: Many of the meds can effect exercise responses; consult physician and/or PDR

Developing Evidence-based, Pressure-tested Programs for Your Clients 47
Help your client to establish effective support systems
Proper goal setting = good initial adherence
✓ Process before performance
✓ Emphasis progression not perfection
Positive experience + empowerment = self-reliance + better long-term
adherence
How a person thinks and feels drives their decision-making and eventually
their actions
Behavior-Change Strategies to Drive Program Success

Developing Evidence-based, Pressure-tested Programs for Your Clients 48
Ultimate Goal = Long-term lifestyle change
40–65% of new exercisers will suffer attrition within 3–6 months, with the
highest risk occurring within the first few weeks.
Identify readiness to change & use motivational interviewing techniques (OARS)
Open-ended questions
Affirmations
Reflective listening
Summarizing
Behavior-Change Strategies to Drive Program Success

Developing Evidence-based, Pressure-tested Programs for Your Clients 49
Optimal Healthcare Is The Ultimate Team Sport

Developing Evidence-based, Pressure-tested Programs for Your Clients 50
✓ Encourage your clients with hypertension to make a firm
commitment to exercise, because even a small amount of
regular exercise (and the subsequent reduction in BP) can
help reduce the long-term consequences of hypertension.
✓ “People won’t care what you know, until they first know
that you care” –John Wooden
Concluding Thoughts
Developing Evidence-based, Pressure-tested Programs for Your Clients 51
Cedric X. Bryant, Ph.D., FACSM
American Council on Exercise
Chief Science Officer
E-mail: [email protected]
Twitter: @drcedricbryant
Website: www.acefitness.org
Thank You!





























