Embed Size (px)
Citation preview

RESEARCH ARTICLE Open Access
Developing quality indicators forassessing quality of birth centrecare: a mixed- methods studyInge C. Boesveld1* , Marieke A. A. Hermus2, Hanneke J. de Graaf3, Marit Hitzert3, Karin M. van der Pal-de Bruin2,Raymond G. de Vries4, Arie Franx5 and Therese A. Wiegers6
Abstract
Background: Birth centres are described as settings where women with uncomplicated pregnancies can give birthin a home-like environment assisted by midwives and maternity care assistants. If complications arise or threaten,the woman is referred to a maternity unit of a hospital where an obstetrician will take over responsibility. In the lastdecade, a number of new birth centres have been established in the Netherlands, based on the assumption thatbirth centres provide better quality of care since they offer a better opportunity for more integrated care than theexisting system with independent primary and secondary care providers. At present, there is no evidence forthis assumption. The Dutch Birth Centre Study is designed to present evidence-based recommendations fororganization and functioning of future birth centres in the Netherlands. A necessary first step in this evaluation isthe development of indicators for measuring the quality of the care delivered in birth centres in the Netherlands.The aim of this study is to identify a comprehensive set of structure and process indicators to assess quality of birthcentre care.
Methods: We used mixed methods to develop a set of structure and process quality indicators for evaluating birthcentre care. Beginning with a literature review, we developed an exhaustive list of determinants. We then used aDelphi study to narrow this list, calling on experts to rate the determinants for relevance and feasibility. Amultidisciplinary expert panel of 63 experts, directly or indirectly involved with birth centre care, was invited toparticipate.
Results: A panel of 42 experts completed two Delphi rounds rating determinants of the quality of birth centre carebased on their relevance (to the setting) and feasibility (of use). A set of 30 determinants for structure and processquality indicators was identified to assess the quality of birth centre care in the Netherlands.
Conclusions: We identified 30 determinants for structure and process quality indicators concerning birth centrecare. This set will be validated during the evaluation of birth centres in the Dutch Birth Centre Study.
Keywords: Quality indicators, Birthing centres, Structure and process assessment, Delphi method, The Netherlands
* Correspondence: [email protected] van Es Institute (Netherlands Expert Centre Integrated Primary Care),Wisselweg 33, 1314 CB Almere, Almere, NetherlandsFull list of author information is available at the end of the article
© The Author(s). 2017 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 DOI 10.1186/s12884-017-1439-9

BackgroundInternationally, birth centres are described as settingswhere women with uncomplicated pregnancies can givebirth in a home-like environment. In the Netherlands,women with uncomplicated pregnancies can choosewhere they want to give birth: at home, in a birth centreor in a hospital [1]. At any location, community mid-wives are responsible for care during labour and birth aslong as it stays uncomplicated. When additional medicalassistance is required, the women will receive specialistcare under responsibility of an obstetrician at an obstet-ric unit. Birth care in a birth centre is provided by com-munity midwives, assisted by maternity care assistants.The community midwife accompanies the woman to thecentre when labour has started. A maternity care assist-ant assists the midwife during labour and birth and pro-vides postnatal care to the woman and new-born. Mostbirth centres do not have a permanent staff of midwivesand maternity care assistants. They are only present atthe centre when accompanying a woman in labour.Birth centres have been present in the Netherlands
since the nineteenth century [2], but not until the year2000 did the number of these centres begin to growconsiderably. This appeared to be a reaction to a severeshortage of maternity care providers, especially primarycare midwives and maternity care assistants but also ob-stetric nurses in hospitals. Birth centres were seen as asolution, because they reduce the pressure on hospitalmaternity wards by providing women who do not wantto give birth at home with a safe and home-like alterna-tive. And because birth centres allow midwives tosupervise multiple births simultaneously, they also re-duce the pressure on community midwives. These birthcentres were typically built right next to, or within, thewalls of a hospital. However, most of them disappearedagain when the problem of the shortage of maternitycare providers was alleviated by a dropping birth ratefollowing the millennium baby boom.In recent years perceptions about the safety of the ma-
ternity care system in the Netherlands began to change.An important cause for this was the publication of theEuro-Peristat data, alarming the Netherlands because ofits relatively high perinatal mortality compared to otherEuropean countries [3]. It was suggested that this mightbe related to the strict division between primary and sec-ondary care in the Dutch maternity care system [4–7].The basic feature of this system is that for healthywomen community midwives or general practioners arethe responsible care providers (primary care), and forwomen with pre-existing and emerging pathology obste-tricians are the responsible care providers (secondarycare) [8]. Media attention given to the Euro-Peristat dataand the report from a special committee set up by theMinister of Health (Steering Group “Pregnancy and
Childbirth”) [9] may have attributed to a change in theattitudes and behaviour of Dutch women and their careproviders with an increasing number of women choos-ing, or being referred to, a hospital to give birth [10]: in2000 30.3% of all births took place at home but this fellto 13.1% in 2015 [11]. More and more healthy womenare opting for a hospital birth because they do not feelsafe at home, or are asking for referral to receive treat-ment (i.e. pain medication) that cannot be provided inprimary care [12]. Birth centres can be seen as an oppor-tunity to keep these healthy women away from the clin-ical setting, to provide a safe and home-like alternative,but to be close enough to a hospital to be able to takethem in quickly when referral is warranted. In theirreport, the Steering Group recommended more integra-tion in maternity care, by improved cooperation betweenprimary and secondary care and the introduction ofbirth centres with close links to hospitals. They also rec-ommended further research on the added value of birthcentres [8]. In recent years, following these recommen-dations, a number of new birth centres have beenestablished in the Netherlands, based on the assumptionthat birth centres provide better quality of care – asmeasured by perinatal and maternal outcomes – sincethey offer a better opportunity for more integrated carethan the existing system with independent primary andsecondary care providers [13]. At present, there is noevidence for this assumption because there is no reliableway to measure degree and quality of integration incare provision. The Dutch Birth Centre Study isdesigned to present evidence-based recommendationsfor organization and functioning of future birth cen-tres in the Netherlands, based on careful assessmentof existing birth centres [14]. A necessary first step inthis process is development of indicators for measur-ing the quality of the care delivered in birth centresin the Netherlands.Although formulated in 1990, the definition of quality
of care provided by the Institute of Medicine (IOM) isstill widely accepted: “quality of care is the degree towhich health services for individuals and populationsincrease the likelihood of desired health outcomes andare consistent with current professional knowledge” [15].Usually three dimensions of quality of care are distin-guished: structure (the capacity to provide high qualitycare), process, and outcome [16]. Measures of thesethree dimensions are called indicators. To assess qualityof care, indicators should be developed for the seven do-mains of quality identified by the IOM: effectiveness,safety, timeliness, efficiency, equity, accessibility andpatient-centeredness [17]. Internationally, standards forbirth centres are available and can provide a tool formeasuring the quality of service provided to childbearingfamilies in birth centres [18, 19], but these standards
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 2 of 13

must be adjusted for specific settings of these centres, inour case, the unique maternity care system in theNetherlands. A number of outcome quality indicatorsare available to assess birth centre care (i.e. perinatal andmaternal mortality and morbidity) [20–27], but structureand process indicators, specifically developed for birthcentre care, are scarce.In this article we describe a set of determinants for
structure and process indicators for assessing the qualityof birth centre care and we explain the approach weused to develop this set. We only describe the deve-lopment of determinants for structure and processindicators, because a newly validated Optimality Index(OI-NL2015) and a Composite Adverse Outcome Score(CAOS) were used to evaluate outcomes of birth centrecare [3].
MethodsStudy designIn order to develop a comprehensive set of structureand process quality indicators to evaluate birth centrecare, we used mixed methods. Three phases werefollowed in the development process: 1) identification ofexisting quality indicators in birth care, 2) translatingthese structure and process indicators into determinants,3) determinant selection by Delphi consultation. Thestudy was conducted in the first half of 2013 as part ofthe Dutch Birth Centre Study [3].
1. Identification of existing quality indicators inbirth care
In the first phase of the study, we used various sourcesto find existing quality indicators in birth care. Webegan with an Internet search for documents fromDutch Institutes that had developed quality indicatorsfor maternity care. Documents that described the (devel-opment of ) quality indicators by midwives, obstetriciansand maternity care assistants were obtained. Next, wereviewed international scientific literature about birthcentres in order to identify existing quality indicators.We searched PubMed and the Cochrane Library usingthe Mesh terms: “birthing centres”, “quality indicator”,“health care” and search terms “quality” and “birthcentre”. We used references from these articles to findother relevant articles and documents related to qualityindicators in maternity care.
2. Translating indicators into determinantsIn the second phase we translated the structure andprocess indicators that we had identified into determi-nants (or topics): elements that identify the nature of theindicator. We used a framework based on the sevendomains of quality according to the IOM (effectiveness,safety, timeliness, efficiency, equity, accessibility and
patient-centeredness.) We added an eighth domain,“Law on the Accessibility of Healthcare Facilities”, be-cause of obligations placed on healthcare facilities by thislaw in the Netherlands. The research group used theirexperience to add topics that were missing in the result-ing list. No outcome indicators were included. We thencreated a questionnaire that members of an expert panelcould complete in a minimum amount of time in orderto maximize our response rate.
3. Determinant selection by Delphi consultationWe initiated an online Delphi study with the goal ofobtaining consensus among a group of experts. Theonline Delphi technique is an anonymously structuredapproach, in which information is gathered from a groupof participants through a number of Delphi rounds. Theweb-based anonymous nature of the Delphi techniqueensures that a single individual cannot dominate theconsensus formation. Moreover all participants areequally able to change their opinion in the course of theprocess [28, 29]. Our Delphi study consisted of twoonline questionnaires.
ParticipantsWe selected participants for the expert panel from theResearch Advisory Group of the Dutch Birth CentreStudy [3], participants of former panels of developingindicators for maternity care in the Netherlands, profes-sionals from different disciplines who are working withor in a birth centre with several years of experience,representatives of health insurance companies, policy-makers, clients and advisors in birth care. Of the careproviders, only experts who are actually involved in birth(centre) care were invited and all health care disciplinesrelated to birth (centre) care were represented. We in-cluded professionals in our heterogeneous expert panel:(11 (community and clinical) midwives, 2 general practi-tioners, 5 maternity care assistants, 6 obstetricians, 4paediatricians, 5 obstetrics and gynaecology nurse spe-cialists, 7 managers from birth centres, 5 representativesfrom health insurance companies, 3 representatives fromclients and 15 other experts (i.e. policymakers, advisorsand research experts). We limited the number of partici-pating clients, because their view on quality of birthcentre care is examined in another part of the study [3].
Rating determinants by experts: First Delphi roundIn May 2013, we sent a link to an online questionnaireby e-mail to the expert panel. The experts wereinstructed to rate the determinants on relevance (to thesetting) and feasibility (of use) and, if necessary, tocomment on them. Each determinant was rated on aseven-point Likert scale (1 = not at all relevant/feasible;4 = neutral; 7 = very much relevant/feasible). Finally,
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 3 of 13

experts were encouraged to suggest additional relevantsubjects that should be taken into consideration in theassessment of the quality of birth centre care. All ratingsfrom the first Delphi round were analysed in Excel anddistributions of scores were presented in median scoresfor each determinant. We considered determinants witha median score of ≥6 with agreement to be relevant andfeasible to collect and accepted these immediately.Agreement was defined when 80% or more of the ratingswere within a range of three (i.e. 5–6-7 of 4–5-6).Determinants that scored with a median score of ≤2were rejected. Median scores of >3 and <6 with agree-ment or ≥6 without agreement were discussed again inthe second Delphi round. Furthermore, all the com-ments on determinants from the first round wereanalysed and the descriptions of determinants were re-phrased in cases of ambiguity. All proposed newdeterminants from the first round were categorized in
domains. New determinants were coded and two re-searchers of our research group decided, using a consen-sus method, which determinants should be submitted inthe second round. Items the research group already haddecided to include in the overall study (i.e. professionalexperiences and topics related to integration) were notincluded in the second round.
Rating determinants by experts: Second Delphi roundIn the second Delphi round, the experts were informedabout the median scores on relevance and feasibility ofthe total expert group, their own scores and the com-ments of the respondents regarding determinants forwhich no consensus was reached in the first round. Theywere instructed to re-consider their rating of the deter-minants presented in the first round as well as to rateand comment on the new elements the same way as inthe first round. This was done to allow experts to revise
Fig. 1 Flowchart selection process indicators quality birth centres
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 4 of 13

Table 1 Selected determinants per domain
Determinant Type ofindicator
Rating on: Median scoreLikert scale
Consensus (%) Conclusionround 1
Conclusionround 2
(1–7) (80%consensus)
(80%consensus)
Domain: effectiveness
Written agreements on care aspects(i.e. by hospital care, obstetricians)
Structure Relevance 7 100 Include
Feasible 6 87,5
Structural evaluation of the care providedin the birth centre
Structure Relevance 7 93,7 Include
Feasible 6 83,4
Maternity care assistant present duringlaboura
Process Relevance 6 87,5 Include
Feasible 6,5 79,2
(Integrated) ICT system with hospitaland midwifery practices
Structure Relevanceround 1
6 75 Submit again
Feasible round1
5 54,3
Relevanceround 2
6 90,5 Include
Feasible round2
6 76,2
Domain: safety
Facilities at a birth centre in relation toemergency care (i.e. CPR resuscitation)
Structure Relevance 7 95,9 Include
Feasible 7 97,9
Joint (interdisciplinary) emergency caretraining
Process Relevance 6 95,8 Include
Feasible 6 87,5
Agreements with ambulance service andnearest hospital about urgent referrals
Structure Relevance 7 89,6 Include
Feasible 6 77
Domain: timeliness
Necessary transport time from birthcentre to hospital
Process Relevance 7 100 Include
Feasible 7 96
In case of referral from the birth centredurante partu: required time betweendecision to refer and treatment inhospital
Process Relevance 7 95,9 Include
Feasible 6 81,3
Domain: efficiency
In case of referral from the birth centredurante partu: guaranteed access to thehospital with which agreements weremade
Process Relevance 7 100 Include
Feasible 6 87,6
Distance between birth centre andhospital
Structure Relevance 7 98 Include
Feasible 7 96
Cooperation with (almost) all relevantorganizations in the region (such asmidwifery practices and maternity careassistance organisations)
Process Relevance 6 89,5 Include
Feasible 6 81,3
Protocols on care aspects Structure Relevance 7 87,5 Include
Feasible 6,5 81,3
Participation of birth centre in localmaternity care consultation andcooperation group (VSV)
Process Relevance 7 85,4 Include
Feasible 6 81,3
Indoor connection between birth centreand hospital
Structure Relevance 6 84 Include
Feasible 7 96
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 5 of 13

Table 1 Selected determinants per domain (Continued)
Joint use of an electronic patient record Structure Relevanceround 1
6 87,6 Submit again
Feasibleround 1
6 66,7
Relevanceround 2
6 95,2 Include
Feasibleround 2
6 85,7
System of quality improvement(i.e. accreditation)
Structure Relevanceround 1
6 70,9 Submit again
Feasibleround 1
5 56,3
Relevanceround 2
6 85,7 DecisionResearchgroup: include
Feasibleround 2
5 80,9
Multidisciplinary education as result offormulated points of improvement fromperinatal audit
Process Relevanceround 2
6 90,5 New in round2
Include
Feasibleround 2
6 83,3
Domain: equity
Care pathways formulated with chainpartners
Structure Relevance 6 95,9 Include
Feasible 6 79,2
Birth centre has vision of birth care Structure Relevance 7 91,8 Include
Feasible 6 75
Formal partnership agreement with chainpartners
Structure Relevance 6 83,4 Include
Feasible 7 81,3
Admission agreement for professionalswho use birth care facilities at the birthcentre
Structure Relevanceround 1
6 69,3 Submit again
Feasibleround 1
7 75,5
Relevanceround 2
6 81 Include
Feasibleround 2
7 85,7
Domain: accessibility
24 /7 telephone accessibility birth centre Process Relevance 7 100 Include
Feasible 7 98
Physical access to birthing centre forclients (i.e. parking)
Structure Relevance 7 96 Include
Feasible 6 78
Physical access to birthing centre formidwives and maternity care assistants(e.g. parking)
Structure Relevance 6 92 Include
Feasible 6 80
Domain: patient-centeredness
Facilities at a birth centre in relation topain management (i.e. nitrous oxide)
Structure Relevance 6 100 Include
Feasible 6 83,7
Continuous presence of a healthcareprovider during laboura
Process Relevance 7 98 Include
Feasible 6 81,3
Structural research on client experiences Structure Relevance 7 98 Include
Feasible 6 85,5
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 6 of 13

their opinion of the first round while considering theratings and comments provided by the other membersof the expert panel. The link to the personalized onlinequestionnaire was sent by email 10 days after the firstround. Again, the median scores and the degree ofagreement were calculated. Only scores ≥6 with agree-ment were adopted into the list. Determinants withscores for relevance ≥6 with agreement, but feasibilitybetween 3 and 6 were presented to the research groupfor a final decision.
ResultsFigure 1 shows the total process that led to theselection of structure and process quality indicators ofbirth centres, and the number of determinants(topics) at each step.
Identification of existing quality indicators in birth careTwo hundred fifteen indicators were derived from Dutchsources, 145 from international literature. We eliminatedduplication and excluded all outcome indicators. Indica-tors that clearly do not determine quality of care in abirth centre (because it is clear that this kind of caredoes not occur in birth centres, i.e. caesarean section)were also excluded from this list. Finally 66 structureand process indicators were identified.
Translating indicators into determinantsThese 66 literature-based indicators were divided intoseven themes matching the seven domains of qualityaccording to the United States Institute of Medicine(IOM). The research group added a domain “Law Acces-sibility of Healthcare Facilities”. In these eight domains,22 topics were identified, because several indicators ap-peared to relate to the same topic, albeit with differentwordings. The research group added another 13 topicsthat they missed, based on their experience. After thisprocess, the topics were formulated as 35 determinantsto be included in the first questionnaire for the onlineDelphi panel.
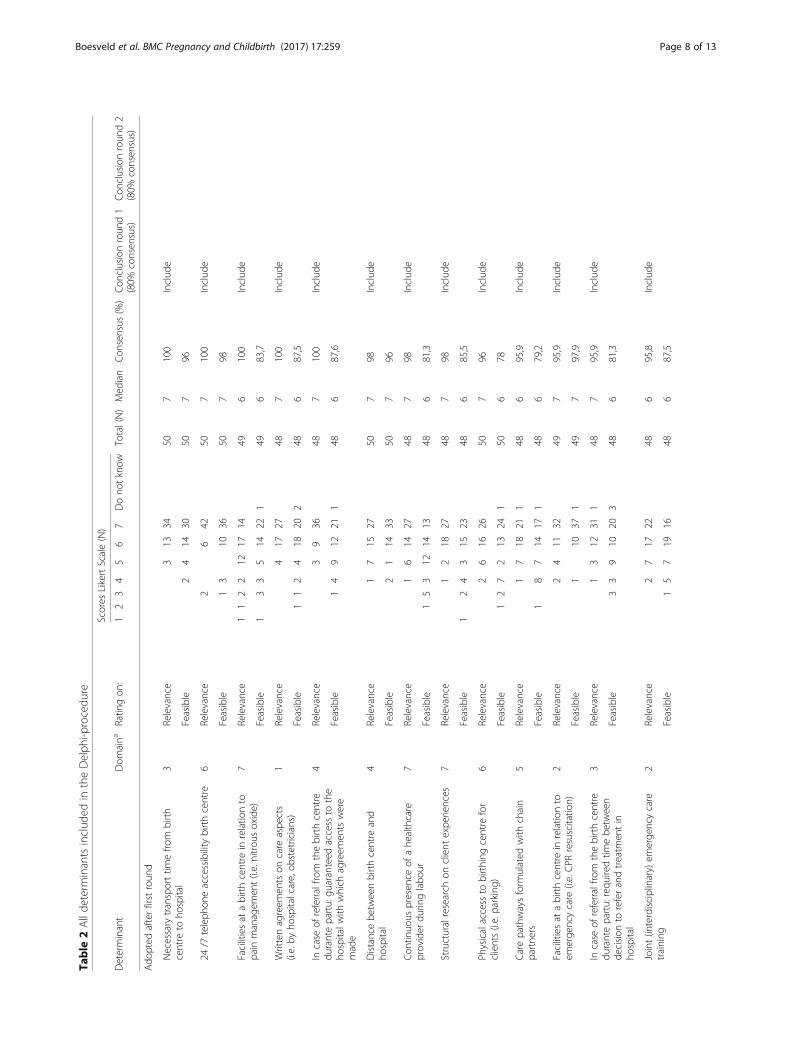
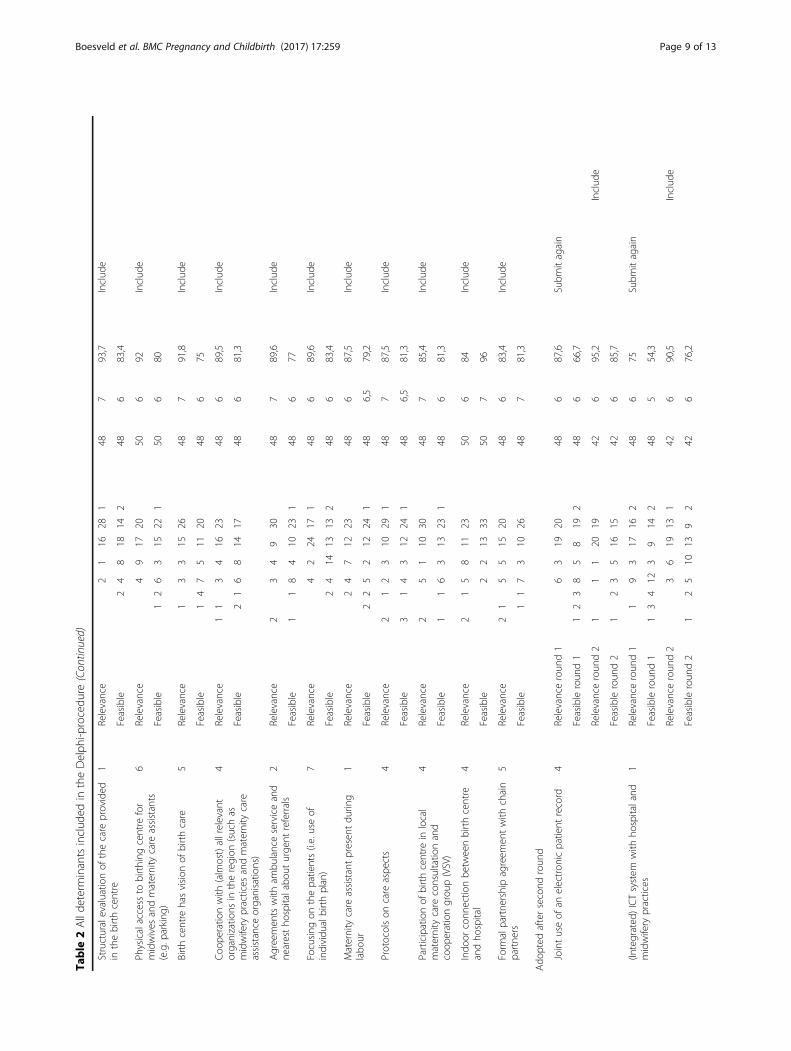
Determinant selection by Delphi consultationThe questionnaire in the first Delphi round was com-pleted by 48 experts (response rate of 76%). 42 of themalso completed the questionnaire in the second round(response rate of 88%). During the first round, 24 of the35 determinants were accepted for inclusion, none wererejected right away, leaving 11 topics without consensus.22 experts mentioned 52 new topics they missed in thequestionnaire. These topics were labelled and catego-rized, after which two researchers of our research groupdecided, based on consensus, that 8 of them would beincluded in the second Delphi round. In the secondround, the 11 topics from the first round on which noconsensus was reached and the 8 new topics were pre-sented to the expert panel. This resulted in the accept-ance of another five determinants and the rejection of13 determinants. One determinant was presented to theresearch group because of low feasibility according tothe experts. The research group accepted this determin-ant, so finally 30 determinants resulted from the Delphiconsultation. Table 1 shows the selected determinantsper IOM quality domain. Table 2 shows all determinantsincluded in the Delphi procedure with the number orrated scores on the Likert Scale.
DiscussionIn this study, part of the Dutch Birth Centre Study, weidentified a set of 30 determinants, to be translated into30 structure and process quality indicators that can beused to assess the quality of birth centre care in theNetherlands. The new developed determinants are de-rived from existing quality indicators in maternity carein the Netherlands (used to measure quality of care bymidwives, obstetricians and maternity care assistants)and indicators derived from international documentsconcerning birth centre care. The experts selected 5determinants that are used by Laws in the research oncharacteristics and practices of birth centres in Australia[20] and 4 determinants derived from Dutch existingquality indicators. They also selected 3 determinantswhich were formulated in a quality framework of birthcentre care, proposed by the Royal Dutch Organization
Table 1 Selected determinants per domain (Continued)
Focusing on the patients(i.e. use individual birth plan)
Process Relevance 6 89,6 Include
Feasible 6 83,4
Participation and representation of clientsin organisation (i.e. in the board)
Structure Relevanceround 2
6 85,7 New in round2
Include
Feasibleround 2
6 78,6
aThese determinants appear similar but are different: ‘Continuous presence of a healthcare provider during labour’ refers to continuous support of labour (notleaving alone the woman in labour). ‘Maternity care assistant present during labour’ refers to the presence of assistance of the midwife during childbirth. In theNetherlands, the midwife attends birth of low risk women, regardless the location (at home, in a birth centre or in a hospital) and is assisted by a maternity careassistant. Sometimes, it happens that the maternity care assistant is too late present at the childbirth to assist the midwife adequately. This determinant refers tothis aspect
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 7 of 13
Table
2Allde
term
inantsinclud
edin
theDelph
i-procedu
re
Scores
LikertScale(N)
Determinant
Dom
aina
Ratin
gon
:1
23
45
67
Dono
tknow
Total(N)
Med
ian
Con
sensus
(%)
Con
clusionroun
d1
(80%
consen
sus)
Con
clusionroun
d2
(80%
consen
sus)
Ado
pted
afterfirstroun
d
Necessary
transporttim
efro
mbirth
centre
toho
spital
3Relevance
313
3450
7100
Includ
e
Feasible
24
1430
507
96
24/7
teleph
oneaccessibility
birthcentre
6Relevance
26
4250
7100
Includ
e
Feasible
13
1036
507
98
Facilitiesat
abirthcentre
inrelatio
nto
pain
managem
ent(i.e.nitrou
soxide)
7Relevance
11
22
1217
1449
6100
Includ
e
Feasible
13
35
1422
149
683,7
Writtenagreem
entson
care
aspe
cts
(i.e.by
hospitalcare,ob
stetricians)
1Relevance
417
2748
7100
Includ
e
Feasible
11
24
1820
248
687,5
Incase
ofreferralfro
mthebirthcentre
durantepartu:gu
aranteed
access
tothe
hospitalw
ithwhich
agreem
entswere
made
4Relevance
39
3648
7100
Includ
e
Feasible
14
912
211
486
87,6
Distancebe
tweenbirthcentre
and
hospital
4Relevance
17
1527
507
98Includ
e
Feasible
21
1433
507
96
Con
tinuo
uspresen
ceof
ahe
althcare
provider
durin
glabo
ur7
Relevance
16
1427
487
98Includ
e
Feasible
15
312
1413
486
81,3
Structuralresearch
onclient
expe
riences
7Relevance
12
1827
487
98Includ
e
Feasible
12
43
1523
486
85,5
Physicalaccess
tobirthing
centre
for
clients(i.e.parking)
6Relevance
26
1626
507
96Includ
e
Feasible
12
72
1324
150
678
Carepathwaysform
ulated
with
chain
partne
rs5
Relevance
17
1821
148
695,9
Includ
e
Feasible
18
714
171
486
79,2
Facilitiesat
abirthcentre
inrelatio
nto
emerge
ncycare
(i.e.CPR
resuscitatio
n)2
Relevance
24
1132
497
95,9
Includ
e
Feasible
110
371
497
97,9
Incase
ofreferralfro
mthebirthcentre
durantepartu:requ
iredtim
ebe
tween
decision
toreferandtreatm
entin
hospital
3Relevance
13
1231
148
795,9
Includ
e
Feasible
33
910
203
486
81,3
Joint(interdisciplinary)em
erge
ncycare
training
2Relevance
27
1722
486
95,8
Includ
e
Feasible
15
719
1648
687,5
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 8 of 13
Table
2Allde
term
inantsinclud
edin
theDelph
i-procedu
re(Con
tinued)
Structuralevaluatio
nof
thecare
provided
inthebirthcentre
1Relevance
21
1628
148
793,7
Includ
e
Feasible
24
818
142
486
83,4
Physicalaccess
tobirthing
centre
for
midwives
andmaternity
care
assistants
(e.g.p
arking
)
6Relevance
49
1720
506
92Includ
e
Feasible
12
63
1522
150
680
Birthcentre
hasvision
ofbirthcare
5Relevance
13
315
2648
791,8
Includ
e
Feasible
14
75
1120
486
75
Coo
peratio
nwith
(alm
ost)allrelevant
organizatio
nsin
theregion
(suchas
midwifery
practices
andmaternity
care
assistance
organisatio
ns)
4Relevance
11
34
1623
486
89,5
Includ
e
Feasible
21
68
1417
486
81,3
Agreemen
tswith
ambu
lanceserviceand
nearestho
spitalabo
uturge
ntreferrals
2Relevance
23
49
3048
789,6
Includ
e
Feasible
11
84
1023
148
677
Focusing
onthepatients(i.e.useof
individu
albirthplan)
7Relevance
42
2417
148
689,6
Includ
e
Feasible
24
1413
132
486
83,4
Maternity
care
assistantpresen
tdu
ring
labo
ur1
Relevance
24
712
2348
687,5
Includ
e
Feasible
22
52
1224
148
6,5
79,2
Protocolson
care
aspe
cts
4Relevance
21
23
1029
148
787,5
Includ
e
Feasible
31
43
1224
148
6,5
81,3
Participationof
birthcentre
inlocal
maternity
care
consultatio
nand
coop
erationgrou
p(VSV)
4Relevance
25
110
3048
785,4
Includ
e
Feasible
11
63
1323
148
681,3
Indo
orconn
ectio
nbe
tweenbirthcentre
andho
spital
4Relevance
21
58
1123
506
84Includ
e
Feasible
22
1333
507
96
Form
alpartne
rshipagreem
entwith
chain
partne
rs5
Relevance
21
55
1520
486
83,4
Includ
e
Feasible
11
73
1026
487
81,3
Ado
pted
aftersecond
roun
d
Jointuseof
anelectron
icpatient
record
4Relevanceroun
d1
63
1920
486
87,6
Subm
itagain
Feasibleroun
d1
12
38
58
192
486
66,7
Relevanceroun
d2
11
120
1942
695,2
Includ
e
Feasibleroun
d2
12
35
1615
426
85,7
(Integrated
)ICTsystem
with
hospitaland
midwifery
practices
1Relevanceroun
d1
19
317
162
486
75Subm
itagain
Feasibleroun
d1
13
412
39
142
485
54,3
Relevanceroun
d2
36
1913
142
690,5
Includ
e
Feasibleroun
d2
12
510
139
242
676,2
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 9 of 13

Table
2Allde
term
inantsinclud
edin
theDelph
i-procedu
re(Con
tinued)
System
ofqu
ality
improvem
ent
(i.e.accred
itatio
n)4
Relevanceroun
d1
110
812
143
486
70,9
Subm
itagain
Feasibleroun
d1
21
17
911
116
485
56,3
Relevanceroun
d2
14
816
121
426
85,7
decision
Research
grou
p:includ
eFeasibleroun
d2
21
315
109
242
580,9
Adm
ission
agreem
entforprofession
als
who
usebirthcare
facilitiesat
thebirth
centre
5Relevanceroun
d1
13
46
1018
749
669,3
Subm
itagain
Feasibleroun
d1
13
38
268
497
75,5
Relevanceroun
d2
11
34
1317
342
681
Includ
e
Feasibleroun
d2
57
291
427
85,7
Multid
isciplinaryed
ucationas
resultof
form
ulated
pointsof
improvem
entfro
mpe
rinatalaudit
4Relevanceroun
d2
13
117
2042
690,5
Includ
e
Feasibleroun
d2
15
316
161
426
83,3
Participationandrepresen
tatio
nof
clients
inorganisatio
n(i.e.in
thebo
ard)
7Relevanceroun
d2
15
1214
1042
685,7
Includ
e
Feasibleroun
d2
17
79
171
426
78,6
Rejected
afterroun
d2
Opp
ortunitiesto
stay
inthebirthcentre
aftergiving
birth
7Relevanceroun
d1
22
415
911
649
571,4
Subm
itagain
Feasibleroun
d1
11
35
613
191
496
77,5
Relevanceroun
d2
24
57
109
542
561,9
Reject
Feasibleroun
d2
34
314
1842
683,3
Legalentity
(i.e.foun
datio
n,association)
8Relevanceroun
d1
22
516
78
45
494
57,2
Subm
itagain
Feasibleroun
d1
11
82
1021
649
667,4
Relevanceroun
d2
33
120
36
24
424
57,1
Reject
Feasibleroun
d2
54
1119
342
680.9
Inde
pend
entsupe
rvisorybo
ard
8Relevanceroun
d1
22
27
613
133
486
66,7
Subm
itagain
Feasibleroun
d1
22
73
1220
248
673
Relevanceroun
d2
11
65
1711
142
678,6
Reject
Feasibleroun
d2
17
217
141
426
78,6
Multid
isciplinarycompo
sitio
nof
the
boardof
thebirthcentre
(e.g.m
idwives,
maternity
care
organizatio
nandho
spital)
4Relevanceroun
d1
31
24
1011
1748
679,1
Subm
itagain
Feasibleroun
d1
11
55
828
487
85,4
Relevanceroun
d2
11
16
518
1042
678,6
Reject
Feasibleroun
d2
32
928
427
92,7
Publicationof
annu
alrepo
rt8
Relevanceroun
d1
21
89
1414
486
77,2
Subm
itagain
Feasibleroun
d1
24
214
252
497
85,5
Relevanceroun
d2
18
714
1242
678,6
Reject
Feasibleroun
d2
67
281
427
83,4
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 10 of 13

Table
2Allde
term
inantsinclud
edin
theDelph
i-procedu
re(Con
tinued)
Num
berof
births
andpo
stpartum
stays
that
occurpe
ryear
inthebirthcentre
4Relevance
22
26
713
1648
675
subm
itagain
Feasible
12
515
2548
793,8
Relevanceroun
d2
21
65
217
426
78,6
Reject
Feasibleroun
d2
18
3342
797,6
Facilitiesat
abirthcentre
inrelatio
nto
stay
(i.e.po
ssibilitiesforfather
tostay
overnigh
t,privateshow
erand/or
toiletin
room
,bath)
7Relevanceroun
d1
24
410
1316
496
79,6
Subm
itagain
Feasibleroun
d1
16
610
2649
785,7
Relevanceroun
d2
14
48
1213
426
78,7
Reject
Feasibleroun
d2
11
48
271
427
92,8
24hpresen
ceof
acaregiverin
birth
centre
(maternity
care
assistantor
midwife)
2Relevanceroun
d2
33
24
413
121
426
69.1
Reject
Feasibleroun
d2
12
12
28
242
427
80,9
Inde
pend
entor
freestand
ingsettingwith
aho
me-like,no
n-clinicalatmosph
ere
6Relevanceroun
d2
41
88
79
542
4,5
54,7
Reject
Feasibleroun
d2
22
56
1413
426
78,6
Detailedbu
sine
ssplan
forthebirthcentre
4Relevanceroun
d2
21
87
156
342
5,5
71,4
Reject
Feasibleroun
d2
14
415
171
426
85,7
Participationof
thebirthcentre
inscientificresearch
1Relevanceroun
d2
13
1014
67
142
571,4
Reject
Feasibleroun
d2
17
812
131
426
78,6
Transfer
from
birthing
room
toa
reside
nceroom
whe
nthemothe
rof
newly-bornchild
wants/can/hasto
stay
a(partof
her)childbe
dpe
riod;
7Relevanceroun
d2
23
114
68
26
424
50Reject
Feasibleroun
d2
11
17
59
126
425,5
50
Staffin
thebirthcentre
mirrorsthe
popu
latio
nthat
(may)usethebirthcentre
7Relevanceroun
d2
93
413
43
24
424
50Reject
Feasibleroun
d2
44
112
310
53
424
38,1
a Descriptio
nof
Dom
ains:
1:Effectiven
ess
2:Safety
3:Timeliness
4:Efficiency
5:Eq
uity
6:Accessibility
7:Pa
tient-cen
teredn
ess
8:Law
onaccessibility
ofhe
alth
care
facilities
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 11 of 13

of Midwives (KNOV). Ten selected determinants areused by different organizations to assess quality of care(e.g. maternity care assistance, emergency care) [30–34].Finally, 7 new determinants were selected by the experts.The final set of indicators will be included in the on-going study to evaluate birth centre care in theNetherlands.
StrengthA strength of the development of this set of determi-nants for indicators is that it is developed in collabor-ation with all parties involved in birth centre care, and isbased on consensus. Therefore it can be expected thatall professionals in the field will accept assessing thequality of birth centre care using this set of indicators.
LimitationsWe are aware that the set of determinants for indicatorswe developed has its limitations. Firstly, to assess care ingeneral, structure, process and outcome indicatorsshould be used. However, because there are already alarge number of quality indicators to assess outcomes ofbirth centre care, this set contains only structure andprocess indicators [35]. The expert panel chose 19 struc-ture and 11 process indicators to asses birth centre care.For the same reason the set we developed does not in-clude indicators of women’s experiences of care, becausethey can be regarded as outcome indicators [36].Thirdly, this set only consists of determinants for indica-tors. The process for developing structure and processquality indicators for birth centres still needs to bedescribed. Also, we do not yet know whether this set ofdeterminants for indicators will be able to differentiatebetween birth centres or not. It has yet to prove itselfin practice: the Dutch National Birth Centre Studywill be the first to use these indicators to assess thequality of care.Finally, although our study was focused on Dutch birth
centres, we expect that this set of determinants forindicators will be applicable in other settings where birthcentres are used.
ConclusionsWe used an online Delphi-method to develop a list ofthirty determinants for structure and process indicatorsto measure quality of birth centre care. We will describethe process for developing quality indicators from thesedeterminants and evaluation of the validity and reliabil-ity of these indicators as part of the Dutch Birth CentreStudy in a later paper. It is important to underscore thatindicators are part of an on-going cycle of qualityimprovement. Indicators should never be static. Changesin evidence or clinical relevance, a consistently highperformance or a low variation in achievement, new
developments and demographic changes in the popu-lation of childbearing women, all may be criteria forremoving an indicator or adding a new one in afuture list of determinants for quality indicators forbirth centre care.
AbbreviationsIOM: Institute of Medicine; KNOV: Royal Dutch Organization of Midwives;ZonMw: the Netherlands Organisation for Health Research and DevelopmentZonMw
AcknowledgementsThe authors gratefully acknowledge the other members of the Project Group‘Birth Centre Study’ for their input in the project. The authors would like tothank the members of the Expert panel for their time and energy spent in thepanel. We are also grateful for the helpful comments of Theo Haitjema andÖmer Aydogan for their useful comments on the draft version of this article.
FundingThis study was funded by ZonMw (the Netherlands Organisation for HealthResearch and Development (ZonMw) in the context of the research programPregnancy and Childbirth, [grant no. 50–50,200–98-102].The authors declare that the funding body had no role in the design of thestudy, collection, analysis and interpretation of data and writing themanuscript.
Availability of data and materialsThe dataset supporting the conclusions of this article is included within thearticle (and its additional file).
Authors’ contributionsAll authors contributed to the design, interpretation of data, drafting andediting of the manuscript. IB collected the data; IB and TW analysed thedata. All authors have read and approved the final manuscript.
Ethics approval and consent to participateDesign and planning of the study were presented to the Medical EthicsCommittee of the UMCU (University Medical Centre Utrecht) who confirmedthat an official ethical approval of this study is not required.
Consent for publicationNot applicable.
Competing interestsThis study was funded by ZonMw (the Netherlands Organisation for HealthResearch and Development (ZonMw) in the context of the research programPregnancy and Childbirth, [grant no. 50–50,200–98-102]. The authors declarethat they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Jan van Es Institute (Netherlands Expert Centre Integrated Primary Care),Wisselweg 33, 1314 CB Almere, Almere, Netherlands. 2Department of ChildHealth, TNO, PO Box 2215 2301, CE Leiden, Leiden, Netherlands.3Department of Obstetrics and Gynaecology, Erasmus University MedicalCentre, PO Box 2014 3000, CA Rotterdam, Rotterdam, Netherlands.4Academie Verloskunde Maastricht/Zuyd University, CAPHRI School for PublicHealth and Primary Care, PO Box 616 6200, MD Maastricht, Maastricht,Netherlands. 5Division Woman and Baby, University Medical Centre Utrecht,PO Box 85500 3508, GA Utrecht, Utrecht, Netherlands. 6NIVEL (NetherlandsInstitute for Health Services Research), PO Box 1568 3500, Utrecht, BN,Netherlands.
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 12 of 13
Received: 26 February 2016 Accepted: 27 July 2017
References1. Wiegers T, de Graaf H, van der Pal K. De opkomst van geboortecentra en
hun rol in de zorg. Tijdschrift voor gezondheidswetenschappen2012. 2012;90(8):475–8.
2. de Graaf JP, Merkus H, Ravelli A, Bonsel G, Steegers E. Short history of Dutchobstetric care and birth centres in particular. In: Perinatal and maternalhealth inequalities: effects of places of residence and delivery. 2013;14
3. Zeitlin J, Mohangoo A, Cuttini M. The European perinatal health report:comparing the health and care of pregnant women and newborn babies inEurope. J Epidemiol Community Health. 2009;63(9):681–2.
4. Evers AC, Brouwers HA, Hukkelhoven CW, Nikkels PG, Boon J, van Egmond-Linden A, et al. Perinatal mortality and severe morbidity in low and high riskterm pregnancies in the Netherlands: prospective cohort study. BMJ.2010;341
5. Tuffnell D. Place of delivery and adverse outcomes. BMJ. 2010;3416. van der Kooy J, Poeran J, de Graaf JP, Birnie E, Denktas S, Steegers EA, et al.
Planned home compared with planned hospital births in the Netherlands:intrapartum and early neonatal death in low-risk pregnancies. ObstetGynecol. 2011;118(5):1037–46.
7. de Jonge A, Baron R, Westerneng M, Twisk J, Hutton EK. Perinatal mortalityrate in the Netherlands compared to other European countries: a secondaryanalysis of euro-PERISTAT data. Midwifery. 2013;29:1011–8.
8. Verloskunde C. Verloskundig Vademecum 2003. College voorZorgverzekeringen: Diemen; 2003.
9. Stuurgroep Zwangerschap en Geboorte. Een goed begin - AdviesStuurgroep zwangerschap en geboorte. Den Haag: 2009.
10. de Vries RG, Paruchuri Y, Lorenz K, Vedam S. Moral science: ethicalargument and the production of knowledge about place of birth.J Clin Ethics. 2013 Fall;24(3):225–38.
11. Nederland SPR. Perinatale Zorg in Nederland 2015. Stichting PerinataleRegistratie Nederland: Utrecht; 2016.
12. Anthony S, Amelink-Verburg M, Jacobusse G, van der Pal-de Bruin, KM. Dethuisbevalling in Nederland 1995-2002. Rapportage over de jaren2001–2002 (Home births in the Netherlands 1995–2002. Report for the years2001-2002). PRN/TNO rapport KvL/JPB 2005;2005.
13. Bonsel GJ, Birnie E, Denktas S, Poeran J, Steegers EAP. Lijnen in dePerinatale Sterfte, Signalementstudie Zwangerschap en Geboorte 2010.Rotterdam:Erasmus MC,2010.
14. Hermus MA, Wiegers TA, Hitzert MF, Boesveld IC, van den Akker-van MarleME, et al. The Dutch birth Centre study: study design of a programmaticevaluation of the effect of birth centre care in the Netherlands.BMC Pregnancy and Childbirth. 2015;15(1):148.
15. Lohr KN, Schroeder SA. A strategy for quality assurance in Medicare. N EnglJ Med. 1990;322(10):707–12.
16. Donabedian A. Explorations in Quality Assessment and Monitoring: Ill.:Health Administration Press; 1980.
17. Institute of Medicine (US). Committee on Quality of Health Care in America.Crossing the quality chasm: A new health system for the 21st century.National Academies Press; 2001.
18. American Association of Birth Centers. Standards for birth centers.Perkiomenville: AABC; 2008.
19. The Royal College of Midwives. Standards for birth Centres in England: astandards document. London: RCM; 2009.
20. Laws PJ, Lim C, Tracy S, Sullivan EA. Characteristics and practices of birthcentres in Australia. Aust N Z J Obstet Gynaecol. 2009;49(3):290–5.
21. Laws PJ, Tracy SK, Sullivan EA. Perinatal outcomes of women intending togive birth in birth centers in Australia. Birth. 2010;37(1):28–36.
22. Stapleton SR, Osborne C, Illuzzi J. Outcomes of care in birth centers:demonstration of a durable model. Journal of Midwifery & Women’s Health.2013;
23. Rooks JP, Weatherby NL, Ernst EK, Stapleton S, Rosen D, Rosenfield A.Outcomes of care in birth centers. The National Birth Center Study.N Engl J Med. 1989;321(26):1804–11.
24. Stewart M, McCandlish R, Henderson J, Brocklehurst P. Review of evidenceabout clinical, psychosocial and economic outcomes for women withstraightforward pregnancies who plan to give birth in a midwife-led birthcentre, and outcomes for their babies. Updated July: Report of a structuredreview of birth centre outcomes; 2005.
25. Waldenstrom U, Nilsson C, Winbladh B. The Stockholm birth centre trial:maternal and infant outcome. BJOG. 1997;104(4):410–8.
26. Byrne JP, Crowther CA, Moss JR. A randomised controlled trial comparingbirthing centre care with delivery suite care in Adelaide, Australia. Aust N ZJ Obstet Gynaecol. 2000;40(3):268–74.
27. Hollowell J, Puddicombe D, Rowe R, Linsell L, Hardy P, Stewart M. TheBirthplace national prospective cohort study: perinatal and maternaloutcomes by planned place of birth. Birthplace in England researchprogramme. Final report part 4: NIHR service delivery and organisationprogramme, 2011 .
28. Keeney S, McKenna H. Hasson F. The Delphi technique in nursing andhealth research: John Wiley & Sons; 2010.
29. Skulmoski GJ, Hartman FT, Krahn J. The Delphi method for graduateresearch. J Inf Technol Educ. 2007;6:1.
30. Kooistra M, Waelput A, Offerhaus P, et al. Kwaliteitsindicatoren voor deeerstelijnsverloskunde. RIVM rapport 260101005. 2009.
31. Zichtbare Zorg Eerstelijnsverloskunde. Zorginhoudelijke indicatorenzichtbare zorg eerstelijnsverloskunde. 2012.
32. Zorginstituut Nederland (2012). Kwaliteitsindicatoren kraamzorg.33. Zorgverzekeraars Nederland (2013). Rapport Kwaliteitsvisie spoedeisende
zorg,34. KNOV. Kwaliteitskader geboortecentra (2010) 2010. Accessed 20 Februar
2013. http://www.knov.nl/werk-en-organisatie/tekstpagina/268/geboortecentra/
35. Wiegers TA, Keirse MJNC, Berghs GAH, van der Zee J. An approach tomeasuring quality of midwifery care. J Clin Epidemiol. 1996;49(3):319–25.
36. van der Kooy J, Valentine NB, Birnie E, Vujkovic M, de Graaf JP, Denktaş,et al. Validity of a questionnaire measuring the world health organizationconcept of health system responsiveness with respect to perinatal servicesin the Dutch obstetric care system. BMC Health Serv Res. 2014;14(1):1.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript atwww.biomedcentral.com/submit
Submit your next manuscript to BioMed Central and we will help you at every step:
Boesveld et al. BMC Pregnancy and Childbirth (2017) 17:259 Page 13 of 13





























