-
1
Development and Validation of a Gene Signature Classifier for
Consensus Mo-
lecular Subtyping of Colorectal Carcinoma in a CLIA-Certified
Setting
Jeffrey S. Morris1, Rajayalakshmi Luthra2, Yusha Liu3, Dzifa
Duose2, Wonyul Lee4, Neelima Reddy2,
Justin Windham5, Huiqin Chen4, Zhimin Tong2, Baili Zhang2, Wei
Wei6, Manyam Ganiraju7, Bradley
Broom7, Hector Alvarez2, Alicia Mejia2, Omkara Veeranki2, Mark
Routbort2, Van Morris8, Michael J.
Overman8, David Menter8, Riham Katkhuda9, Ignacio I. Wistuba2,
Jennifer S. Davis10, Scott Kopetz8*,
Dipen M. Maru2*
1 Department of Biostatistics, Epidemiology and Informatics,
University of Pennsylvania School of
Medicine
2 Division of Pathology and Laboratory Medicine, The University
of Texas MD Anderson Cancer Cen-
ter
3 Department of Biostatistics, University of Chicago School of
Medicine
4 Department of Biostatistics, The University of Texas MD
Anderson Cancer Center
5 NanoString Technologies Inc.
6 Cleveland Clinic Foundation
7Department of Bioinformatics and Computational Biology, The
University of Texas MD Anderson
Cancer Center
8Department of Gastrointestinal Medical Oncology, The University
of Texas MD Anderson Cancer
Center
9Department of Pathology, University of Chicago Medical
Center
10Department of Epidemiology, The University of Texas MD
Anderson Cancer Center
* Contributed equally as co-senior authors of this article
Corresponding Author:
Dipen Maru, MD
Professor
Departments of Anatomic Pathology and Translational Molecular
Pathology
The University of Texas MD Anderson Cancer Center
Phone: 713 792 2678
Email: [email protected]
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
mailto:[email protected]://clincancerres.aacrjournals.org/
-
2
Abstract:
Purpose: Consensus molecular subtyping (CMS) of colorectal
cancer (CRC) has potential to reshape
the CRC landscape. We developed and validated an assay that is
applicable on formalin fixed paraf-
fin embedded (FFPE) samples of CRC and implemented the assay in
a CLIA-certified laboratory. Ex-
perimental design: We performed an in silico experiment to build
an optimal CMS classifier using a
training set of 1329 samples from 12 studies and validation set
of 1329 samples from 14 studies. We
constructed assay based on Nanostring codesets for the top 472
genes, and performed analyses on
paired flash frozen (FF)/FFPE samples from 175 CRCs to adapt the
classifier to FFPE using a subset
of genes found to be concordant between FF and FFPE, and tested
the classifier`s reproducibility,
repeatability, and validated in a CLIA-certified laboratory. We
assessed prognostic significance of
CMS in 345 patients pooled across 3 clinical trials. Results:
The best classifier was Weighted Sup-
port Vector Machine with high accuracy across platforms and gene
lists (>0.95), and the 472-gene
model outperforming existing classifiers. We constructed subsets
of 99 and 200 genes with high
FF/FFPE concordance, and adapted FFPE-based classifier that had
strong classification accuracy
(>80%) relative to “gold standard” CMS. The classifier was
reproducible to sample type, RNA quality,
and demonstrated poor prognosis for CMS1-3 and good prognosis
for CMS2 in metastatic CRC
(p
-
3
Introduction:
Colorectal cancer (CRC) is the third most common cancer and a
leading cause of cancer death
worldwide. Several papers were published introducing CRC
molecular subtyping systems; each parti-
tioning colorectal cancer into three to six subtypes (1-7). The
translational value of these works were
limited by their relatively small sample sizes and lack of
consensus regarding which of the six subtyp-
ing systems best captured the tumor heterogeneity and had
superior utility as predictive and/or prog-
nostic marker. In this context, Guinney, et al. (8) assembled
the colorectal subtyping consortium
(CRCSC) that sought to identify consensus molecular subtypes
(CMS) by assembling a data base of
gene expression measurements from 4,151 CRC patients from a
collection of 18 international stud-
ies, having each of the six subtyping systems applied to each of
these samples, and then using a
network analysis to identify consensus clusters. The four
consensus subtypes were identified primari-
ly based on the biologic characteristics of colorectal cancer.
However, findings by Guinney, et al. and
subsequent other studies have demonstrated prognostic and
predictive value of CMS in colorectal
cancer (9-17).
In order to fully realize these potential benefits of CMS, it is
necessary to have a robust, reliable sin-
gle sample classifier to discern a CRC patient’s CMS from the
tumor tissue. As part of an internation-
al consortium (8), we previously presented a Random Forest
classifier that included 5973 genes and
a “single sample” classifier based on nearest centroid predictor
applied using 693 genes, built primari-
ly using microarrays designed for use with flash frozen (FF)
samples. Efforts are needed to build a
more parsimonious single sample classifier using fewer genes
that can be reliably run on RNA ex-
tracted from formalin-fixed paraffin embedded (FFPE) samples. In
this paper, we introduce an FFPE-
based CMS classifier using the NanoString platform that has
strong accuracy for predicting the CMS
in CRC samples including those from the CRCSC study. This gene
classifier was discovered and val-
idated in silico by using the CRCSC data sets and subsequently
optimized based on degree of corre-
lation across tissue types; FFPE vs. FF samples and platform
type NanoString vs. Affymetrix. Subse-
quently, we validated this FFPE tissue based gene classifier in
a CLIA-certified molecular diagnostic
laboratory and demonstrate prognostic significance of CMS in
CRC.
Material and Methods:
Development and Validation of CMS Classifier on CRCSC: We
performed in silico development
and validation of the CMS classifier using the samples and
datasets that were part of the “consensus”
set in CRCSC, meaning that they had so-called “gold standard”
CMS status, defined based on
agreement among the six different subtyping systems, against
which we could compare to assess
classification accuracy of our CMS classifier. Details of the
discovery and validation approach, data
sets used, including tissue type, total number of samples, total
number of consensus samples and
preprocessing method are shown in figure-1A, supplementary
table-1 and supplementary methods 1
and 2. Classification Modeling Strategies: The classification
modelling strategies we considered
included Linear Discriminant Analysis (18,19), Quadratic
Discriminant Analysis (20,21), K-Nearest
Neighbor (22,23), Random Forrest (8,24), Rotation Forrest
(25,26), Weighted Support Vector Ma-
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
4
chine (wSVM)(27,28), Distance-Weighted Discrimination
(DWD)(29,30), and Ensemble Methods
comprised of voting schemes across these classifiers
(supplementary methods 3). We split the train-
ing data set of V1 into subsets, containing 332, 332, 332, and
333 samples, respectively, for use in
the four-fold cross validation model building strategy. For each
modeling strategy, we applied the
Quantile Normalization(30) and fit the model to each of the four
¾ subsets, optimizing tuning parame-
ters using nested cross validation, and assessed accuracy for
predicting the gold standard CMS on
the left-out ¼ subset. Tuning parameters that showed the best
accuracy were selected as optimal
parameters for each subset. We summarized the predictive
accuracy of each modeling strategy as a
function of number of genes, allowing us to both assess which
modeling strategy appears to be best
and the minimum number of genes needed for accurate CMS
classification. Choosing the best mod-
eling strategy, we computed the classification accuracy in the
validation data set V2 as well as the
various subsets mentioned above, and summarized results again as
a function of number of genes in
the model. Gene Ranking Strategy: We designed a boosting
procedure based on multi-class Ada-
boost (31) to order the genes (see supplementary methods 4),
which amounts to a forward stage-
wise additive selection in which samples were repeatedly
re-weighted at each step so the next best
gene focused more on samples misclassified on previous steps,
resulting in a list of genes ranked in
descending order of classification importance. By using the same
reduced gene sets for each classifi-
cation method, we were able to gain a straightforward comparison
of which method appears to per-
form better, to find the minimum gene set size yielding good
classification performance, and to fairly
compare the various methods at any desired model size. wSVM
classifier: Our results revealed that
the best performing classifier was the wSVM. The user calls the
wSVM function with an N by P matrix
of expression values for P genes for each of N samples with the
column names as Entrez IDs, and
the function will quantile normalize the data and apply the wSVM
to get class predictions. After pair-
wise coupling, for sample I, we obtain probabilities of each
CMS, ij such that ∑ 𝜋𝑖𝑗 = 14𝑗=1 , with
i=maxj {ij} indicating the highest CMS class probability for
that sample, which we consider a meas-
ure of CMS classification confidence. We have two possible rules
to classify a sample into a CMS
group based on these measures:
1. Most Likely CMS: Classify sample i into the most likely CMS,
{j: ij =max (ij)}, regardless of clas-
sification confidence i.
2. Most Likely CMS with a Confidence Threshold: Classify sample
i into the most likely CMS as
long as the classification confidence i is above some threshold
(e.g. 0.50 or higher), and oth-
erwise consider indeterminate {Choose CMS j: ij =max (ij) if ij
>, otherwise CMS indetermi-
nate}. Indeterminate samples are heterogenous tumors containing
characteristics of multiple
CMS, so could also be called “mixed CMS”, as done for 13% of
total samples by Guinney et al.
(8).
Generation of Gene Signature Classifier in CRC Samples:
Summary of the Approach for Development of NanoString
Classifier: We used a novel strategy
to port the CMS classifier designed for Affymetrix platform on
FF samples over to the NanoS-
tring/FFPE setting that efficiently utilizes the vast
information available to us in the CRCSC data sets
and overcomes inconsistencies in mRNA quality between FF and
FFPE samples (Figure 1-B and
supplementary Figure-1).
Affymetrix 133-2 Plus2.0 and NanoString CodeSets Based Gene
Expression Assays: Flash fro-
zen and FFPE tumor samples from randomly selected 175 patients
including 95 men and 80 women
with stage I-IV colon cancer were included in the first phase of
the study to build a FFPE classifier.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
5
Seventy-two out of 175 samples were included in the CRCSC,
therefore, the “gold standard” CMS based on
Affymetrix expression array was known and only Nanostring assay
was run on RNA extracted from FF and
FFPE tissue samples of these tumors. Additional FF and FFPE
samples from 103 tumors were identified from
our institutional biorepository. The “gold standard” CMS was not
known for these samples, therefore, Affymet-
rix 133-2 Plus2.0 was run on FF samples to identify the CMS as
the “gold standard”. Subsequently, Nanostring
assay was run on RNA extracted from FF and FFPE samples from
these tumors. All samples were derived
from primary colon/rectum resection specimens without
preoperative tumor targeted therapy. The
clinico-pathologic features of the patient population are shown
in Table-1 and supplementary meth-
ods 5. Briefly, tumor areas with higher than 60% tumor
cellularity from the gland forming tumor and
higher than 20% tumor cellularity from signet ring or mucinous
tumor were manually macro-dissected
from FF or FFPE tissue sections to enrich for the demarcated
tumor area. In more than 2/3 samples,
superficial and deep (invasive border) areas of the tumor were
included for the macro dissection.
RNA was extracted using Qiagen’s AllPrep DNA/RNA kits (QIAGEN,
Netherlands) per manufacturer’s
instructions. Each sample was quantitated using the qubit
fluorometer, with yields ranging from .9 g
to 26 g. Each sample was run on the Agilent Bioanalyzer (Agilent
Technologies, Santa Clara, CA) to
determine the RNA Integrity Number (RIN) for the FF samples and
the DV200 value for the FFPE
samples. The FFPE samples included in the development of single
sample classifier had 18% to 79%
of the RNA having greater than 200 intact nucleotides. Gene
expression analysis with Affymetrix 133-
2 Plus2.0 was performed as described previously (supplementary
methods 6). We designed a custom
set of NanoString CodeSets (NanoString Technologies, Seattle,
WA) with 472 signature probes, se-
lected from the top 500 genes from the boosting procedure and 28
reference probes. The NanoS-
tring CodeSets for each gene was chosen to be the genomic region
that was most highly correlated
with the fRMA level-expression summary of the gene by Affymetrix
133-2 Plus2.0 probe set (Affymet-
rix, Santa Clara, CA). The genes with at least 0.70 correlation
between the CodeSets and gene level
summary were included in the customized CodeSets. The 28
reference CodeSets were selected from
the reference CodeSets on the NanoString PanCan array plusR, and
selecting genes with evidence of
no difference in CMS in our preliminary data (32-36). The assay
was performed as per the NanoS-
tring guidelines (supplementary methods 7) with 10 patient
samples, a positive and negative control
on each cartridge. Raw data from the nsolver software was
transferred to the bioinformatics group
where the custom CMS classifier algorithm in the form of R
script was used to determine which sam-
ples belonged to a particular CMS.
Validation at the Research Molecular Diagnostic Laboratory: The
NanoString CodeSets were technically validated by running two
samples with “gold standard” CMS known from the CRCSC data on three
different lots of CodeSets. The old lot of CodeSets and new lot of
CodeSets were run to-gether in the same run and accuracy in
identifying the CMS by these CodeSets was assessed by lin-ear
regression. We tested repeatability of CMS assay across 4 different
runs by same technician in 12 samples, reproducibility with
different technician in 12 samples, and reproducibility with
different input RNA quantity (50-500ng) for 6 samples using the
same CodeSets on the same nCounter used for prior experiments. We
also tested reproducibility of CMS between colonoscopy biopsies and
sur-gically resected primary CRC by running customized CodeSets on
matched biopsies and resection samples, using same CodeSets and
nCounter and laboratory personnel. Assessing Performance of CMS
Classifier Assay in A CLIA Certified Laboratory:
The NanoString assay with top 200 genes (CRC CMS-200) and top 99
genes (CRC CMS-100),was
further validated at our CLIA-certified Molecular Diagnostic
Laboratory (MDL) to apply this assay as
an integral biomarker for a phase II clinical trial
(NCT034365630) assessing safety and efficacy of
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
6
dual TGF-β trap: anti-PD-L1 molecule M7824 (EMD-Serono) in CMS4
subtype CRC. Thirty-five tumor
samples from stage II/III primary colon cancer, previously used
for validation at the research molecu-
lar diagnostic laboratory, were used to validate the assay
across 10 runs for a total of 120 reactions.
All 35 samples were included in the CRCSC study and gold
standard CMS was known for these
samples, and the laboratory technician was blinded from the gold
standard CMS for those samples.
Input for the assay was 250 ng of total RNA extracted from FFPE
tumor tissue with 20% or higher
tumor cellularity. Accuracy, analytical sensitivity, and
analytical specificity were assessed by compar-
ing calls from the MDL CMS panel with “gold standard” CRCSC
Affymetrix calls. Reproducibility was
assessed across original run and at least 3 additional repeat
runs without re-extraction of RNA. Re-
peat runs were also performed with re-extracted RNA and by 2
technicians.
Assessing Performance of CMS Classifier as a Prognostic Marker
in Stage IV Colorectal Can-
cer:
Patients with a CMS determination from the NanoString based gene
expression score were pooled
from three separate sources, including two clinical trials;
NCT03436563 (n=91) and a phase II trial
assessing Trametinib and Durvalumab in microsatellite stable
colorectal cancer (n=19,
NCT03428126) and Assessment of Targeted Therapies Against
Colorectal Cancer (ATTACC,
NCT01196130) Screening Protocol (n=235) (37). The ATTACC samples
and the samples from the
Trametinib/Durvalumab study were characterized by CRC CMS-100
assay at the research molecular
diagnostic laboratory, while samples from patients enrolled in
M7824 clinical trial were characterized
by CRC CMS-200 performed at the CLIA compliant molecular
diagnostic laboratory. Median overall
survival was calculated from date of stage IV diagnosis to death
or date of last follow up, which was
censored. Survival patterns were visualized with Kaplan Meier
survival curves and compared using
the log-rank test. Graphs were generated using IBM SPSS
Statistics 24.
The study was approved by the institutional review board (IRB)
with an informed consent from each
subject or each subject`s guardian for the clinical trial
samples. The work on samples from subjects
not enrolled in the clinical trial was approved by the IRB with
waiver of informed consent. The study
has been conducted as per the ethical guidelines of U.S. common
rule.
Results:
Performance of CRCSC Classifier on CRCSC Data Sets:
We selected the wSVM model as it had the best performance in the
Training Data V1 using 4-fold
cross-validation (Supplementary Figure 2, Supplementary Table 2
and supplementary material 8).
The 4-group classification accuracy of the wSVM model on the
validation data set V2 was 0.955 for
the full model (5973 genes), and still outstanding for models
involving smaller gene numbers, with 4-
group classification accuracies of 0.959, 0.932, and 0.898 for
models with 500, 75, and 20 genes, re-
spectively. The performance of the wSVM classifier for the
out-of-sample subset (V2o), the RNAseq
subset (TCGA), and the Affymetrix subset (V2a) were comparable
to the overall validation perfor-
mance (V2), suggesting the classifier was robust to platform and
has good out-of-sample perfor-
mance, relatively evenly across CMS (Supplementary Tables 3-7,
supplementary material 9). We
chose a wSVM classifier with 472 genes to move forward with
further validation. This classifier yield-
ed an overall 96.3% classification accuracy in the Affymetrix
subset V2a, with accuracies of 0.966,
0.967, 0.932, and 0.971 for CMS1, CMS2, CMS3, and CMS4,
respectively. The CMS structure was
remarkably persistent being highly consistent in training and
validation datasets (heat map in Sup-
plemental Figure-3). Further comparison on our classifier with
classifiers described by Guinney et. al.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
7
is shown in the supplementary Table-8. Performance of 472 gene
CRCSC classifier based on single
Affymetrix probe gene set and the classifier performance by
classification confidence are described in
supplementary material 10 and 11 and supplementary Figure-4.
Supplementary Table-9 shows all of
the misclassified samples along with the corresponding wSVM
class probabilities (ij) for each CMS,
classification confidence (i), and indication of whether this
sample could be considered a “CMS mix-
ture” (i.e. (ij >0.20 for multiple CMS) and if the “gold
standard” was a part of that mixture. From this,
we see that most of the “misclassified samples” had lower
classification confidence i, and many had
evidence of being CMS mixtures, with the “gold standard” CMS
being a component of the mixtures.
Nanostring CRCSC Classifier Optimization Based on Correlation
between FF and FFPE Tumor
Samples:
The sample-specific correlations of FF and FFPE measurements
were very high for most samples
(Figure 2a, Supplementary Table 10A and supplementary material
12), with a small number of sam-
ples with low correlations tending to have poorer RNA quality
for their FF samples (p=0.0077) but not
FFPE (p=0.28, Figures 2B and 2C). A histogram of the
gene-specific correlation of FF and FFPE
measurements for each of the 472 classifier genes is found in
Figure 2D and summarized in supple-
mentary Table 10B. This histogram demonstrates the high level of
variability across genes in terms
of concordance of paired FF/FFPE gene expression measurements,
and the remarkable consistency
of the gene-specific concordances across batches (Supplementary
Figure 5) suggests that this con-
cordance is a consistent characteristic of the gene/probe set
and not a random technical factor. This
motivated us to select a subset of genes showing high FF/FFPE
concordance for use in our FFPE
classifier, choosing the top 100 genes in terms of FF/FFPE
correlation for the CMS-100 classifier and
the top 200 genes for CMS-200.
NanoString FFPE Classifier Performance:
Figure 3 shows the classification accuracy of CMS-100 on FFPE
and FF samples, CMS-472 on FF
samples, and the Affy FF-100 and Affy FF-472 based on the
Affymetrix validation data V2a, with ac-
curacy split out by confidence threshold and proportion of
unclassified samples. The CRC CMS-
100 model applied to FFPE samples had 4-group accuracy of 0.80
with 0.81 for CRCSC samples and
0.78 for non-CRCSC samples. For samples with high confidence
(i>0.80 or 0.90), the performance
was better with 4-group accuracy of 0.86 and 0.89, respectively.
For FF samples, the CMS-100 had
4-group classification accuracy of 0.80, 0.74 for the CRCSC
samples and 0.88 for non-CRCSC sam-
ples, and 4-class accuracy of 0.87 and 0.92 for samples
classified with high confidence i =0.80 or
0.90, respectively (supplementary material 13). These performed
comparably to the CMS-472, the
472 gene classifier on FF samples, and not much worse than
CMS-100 in an idealized non-clinical
setting based on batch-corrected Affymetrix data from the CRCSC
studies.
Supplementary figures 6A and 6B plot the 4-class accuracy vs.
confidence level i for FFPE and FF
samples, demonstrating that samples classified with high
confidence were more likely to be accurate-
ly classified. Supplementary figures 6C and 6D plot the 4-class
accuracy vs. RNA quality, defined by
%200nt (FFPE) or RIN (FF), demonstrating that there is little if
any association of CMS accuracy with
RNA quality, suggesting that the performance of classifier is
robust to RNA quality in this study. One
gene out of the 100 was mistakenly left off an order of the
Nanostring codesets for some of the vali-
dation study, so the corresponding classifier CMS-100 that was
validated has 99 genes. We con-
firmed the performance of the 100 and 99 gene classifier was
concordant.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
8
The CRC CMS-100 assay with 99 genes was 100% reproducible in
predicting a CMS across different
runs (12 samples= 48 runs), between two laboratory personnel (12
samples) and with different RNA
input concentration (n=6). The reproducibility between biopsy
and resection was 91% with 15 of 17
patients had same CMS between matched biopsy and resection
specimens (Supplementary Table-
11). All (12 from left colon and 5 from right colon) biopsy
samples were procured from same tumor as
surgically resected specimens. Tissue sections from RNA were
derived from FFPE blocks that were
generated for the clinical use. The two cases with discrepant
CMS between biopsy and resection
were sporadic CRC without any known predisposing condition or
preoperative tumor targeted thera-
py. To determine impact of tumor location and histopathologic
features on reproducibility of CMS, an-
other pathologist reviewed Hematoxylin & Eosin stained
sections of primary tumor from surgical re-
sections of those included in assessment of inter-run
reproducibility, InterTech reproducibility, repro-
ducibility across different RNA concentration and
reproducibility between biopsy and resection (n=30).
In 19 samples both superficial and deep area of the tumor were
macro dissected, 4 samples had only
superficial and 7 had only deep area of the tumor macro
dissected. Five tumors were poorly differen-
tiated, one with mucinous histology and 25 tumors were
moderately differentiated including one with
mucinous histology. Due to high reproducibility across runs,
technicians and RNA concentration, we
did not observe any difference in CMS call among samples with
different areas of macro dissection or
histologic parameters. We also did not observe significant
difference in probability of a CMS in the
context of histologic parameters. However, two (of 17) samples
that showed discrepancy for CMS be-
tween biopsy and surgical resection had only deep area of the
tumor macro dissected from the resec-
tion specimens. We also did not find histologic features unique
to 7 samples that were discrepant for
the CMS between research laboratory and CLIA certified
laboratory.
Performance of CRC CMS-200 in CLIA-certified Molecular
Diagnostic Laboratory:
On initial run, 32/35 samples were accurately assigned the CMS
as compared to the gold standard
based on “most likely CMS”, i.e. with confidence threshold of
i>0.50. Three misclassified samples,
with 0.50 and 0.57 “most likely CMS” probability on the initial
run had “most likely CMS” probability in
the borderline range (≥0.43 & 0.57 is used, then in all
three samples in all runs had CMS as per the gold
standard, and the assay had 100% analytical sensitivity and
analytical specificity. Inter run reproduci-
bility was assessed from 3 separate extractions from 4 unique
patient samples for a total of 12 cases.
These 12 cases were run across 3 separate NanoString Runs and by
2 technologists. There was
100% concordance for the CMS classification among all 3 runs
with an average standard deviation of
± 0.002 for the “most likely CMS” probability. The inter tech
reproducibility was 100% for the CMS
classification between both technicians with an average standard
deviation of ± 0.002 for the CMS
probability. Intra run reproducibility was assessed among 4
samples run in triplicate on a single
NanoString run. There was 100% concordance for the CMS
classification among all 3 runs with an
average standard deviation of ± 0.012 for the CMS probability.
Comparing CMS reproducibility with
CMS-100 (99 genes) vs. 200 gene assay demonstrated 97%
reproducibility with only 1 of 35 samples
showing discordant CMS. List of CMS100 (99 genes) and CMS200
test and 16 housekeeping genes
is shown in Supplementary Table-12. These reproducibility and
repeatability findings were deemed
up to the level of a CLIA certified assay to determine CMS 4 vs.
other CMS for FFPE tumor samples
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
9
from patients enrolled in the clinical trial targeting patients
with CMS4 colorectal cancer, as described
in the methods.
KRAS-BRAF Mutational Status and Prognostic Relevance of CMS by
the NanoString CMS
Classifier:
To confirm the expected biologic performance of the assay, we
surveyed a set of mCRC patients en-
rolled in clinical trials and ATTACC Protocol (Table-2). Higher
frequency of KRAS mutation was ob-
served with CMS 3 (66%) and CMS 4 (50%) samples. BRAF mutations
were identified only in CMS 1
(50%), CMS 4(8%), and mixed (12%) subtype samples (Figure-4A).
We did not find significant differ-
ence in any of the clinicopathologic and molecular
characteristics between samples that were classi-
fied as mixed vs. those that were classified in to one of CMS.
Using the CMS-100 (99 genes) classifi-
er, we were able to identify significant differences in overall
survival by CMS, consistent with prior
studies (9,14). Specifically, patients with a CMS2 tumor had the
best survival with a median of 46.1
months from stage IV diagnosis (95% CI: 36.6, 58.1), patients
with a CMS1 or CMS3 tumor had the
poorest survival after a stage IV diagnosis with median survival
times of 23.2 (95% CI: 19.3, 59.2) or
21.4 (95% CI: 15.8, 34.6) months, respectively. Patients with a
CMS4 tumor had a survival pattern
that was in between that of CMS2 and CMS1 or CMS3 with a median
survival time of 35.3 months
(95% CI: 32.2, 40.0) (Figure-4B).
Discussion:
Consensus molecular subtyping has great potential to reshape the
landscape of CRC treatment and
contribute to the development of new precision therapeutic
approaches. However, to realize this po-
tential, it is necessary to transform the CMS based on network
analysis of multiple gene expression
datasets into a clinical test requires an assay that is
reproducible across platforms and tissue types,
has high classification accuracy, and is able to generate CMS in
a single sample setting. We
achieved this objective using a three step approach for building
the classifier; in silico testing of vari-
ous classification strategies considering various gene list
sizes on CRCSC data generated on Affy-
metrix platform and determining that wSVM is the optimal system,
a gene reduction exercise to select
genes with best concordance across gene expression profiling
platforms and tissue types to ensure
optimal performance in FFPE samples, updating the wSVM using the
CRCSC training set based on
this reduced number of genes, and then using this classifier on
measurements from the Nanostring
assay on FFPE samples after transforming these values onto the
scale of the Affymetrix data on FF
samples that dominated the CRCSC training set.
Rather than just choosing a classification strategy in an ad hoc
fashion, we used a systematic, rigor-ous strategy to rank the genes
based on their classification value and to compare a large number
of classification strategies for a wide range of model sizes. This
allowed us to find out which strategy performed best, the wSVM, and
to determine how parsimonious a classifier could be without
sacrific-ing substantial classification accuracy. Given that the
classification literature clearly demonstrates that no one
classification strategy is optimal for all data sets, the
consideration of multiple approaches is important when building
classification signatures. Moreover, findings from the Microarray
Quality Con-trol (MAQC) project from FDA has shown that even slight
differences in the statistical analysis led to discrepancies in
biological interpretation (38). High accuracy in predicting CMS by
nearly all statistical
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
10
methods gives credence to the utility of our CMS assay in
accurately classifying a colon cancer in one of the CMS. The wSVM
classifier we built using this strategy applied to training data,
consisting largely of batch-
corrected Affymetrix gene expression measurements from FF
samples, performed exceptionally well
in the CRCSC validation data. Our custom design of CodeSets best
capitulating the signal in our
training data, and our strategy of starting with more genes than
necessary, then narrowing to a subset
with evidence of high FF/FFPE correlation further mitigated the
influence of FFPE on classification
performance. Our quantile normalization strategy was sufficient
to obtain reasonable performance for
small (99 or 200) gene FFPE NanoString classifier. This strategy
allowed us to efficiently utilize our
data resources, using the enormous data on FF samples to train
the classifier and collecting a smaller
set of paired FF/FFPE samples to identify genes with high
FF/FFPE concordance and map the FFPE
NanoString expression values to the scale of the FF Affymetrix
expression values, leading to our
novel strategy for building the classifier. The consistency of
gene-specific FF/FFPE concordance
across batches provides strong support for this strategy.
The high concordance we observed in CMS for CRC samples between
a research molecular testing laboratory and a CLIA-certified
clinical molecular diagnostic laboratory indicate robust
performance of the assay. High inter-laboratory reproducibility is
likely due to similarities in the pre-analytical and analytical
processes between two laboratories. Another reason for our high
inter-laboratory reproduc-ibility is the use of NanoString
n-counter technology that utilizes non-amplified nucleic acids
without any reverse transcription step and is applicable to
multiple samples. Ragulan et. al.(39) demonstrated high
classification accuracy and reproducibility of NanoString based
subtyping-classification between FF and FFPE tissue samples of
colorectal cancer. In spite of significant differences in the CRC
clas-ses and validation approach, this study and our study indicate
that NanoString is a reliable platform to develop and validate gene
expression based signature using FFPE samples of CRC. Guinney et
al. (8) found that approximately 87% of CRC tumors classified
cleanly into a single CMS, but approximately 13% were “mixed CMS”,
not outliers or a fifth subtype but heterogeneous samples
containing characteristics of multiple CMS. We also found similar
proportions of “mixed CMS” sam-ples in our analyses. Clinically,
patients with mixed CMS tumors could be treated multiple ways. One
option would be to include any “mixed CMS” sample with a high
enough probability of CMSx as a po-tential candidate for any
targeted therapy that has been validated as a precision therapeutic
for CMSx (x=1, 2, 3, or 4), which of course would require
prospective validation before clinical application. There is
increasing evidence of the prognostic and predictive utility of
CMS. Lenz et al. (9) using a NanoString based assay in a large
cohort of patients with metastatic or advanced colorectal cancer
enrolled in CALGB/SWOG 80305 phase III clinical trial, demonstrated
that there is significant differ-ence in overall survival by CMS
with median survival of 40 months in CMS2 vs. median survival of 15
months in CMS1. The NanoString assay used for the CALGB/SWOG 80305
and our study differed significantly. Lenz et al. developed a
customized NanoString based genes that were derived from some of
the large data sets with published gold standard CMS labels,
including, The Cancer Genome Atlas and other studies (5,13). Only
genes that are common to these three data sets and those as-sessed
in the CALGB/SWOG 80405 panel are used. While the genes included in
our NanoString based assay were all derived from CRCSC database.
Similar prognostic trends were observed by other groups including
in patients enrolled in FIRE3 study comparing Cetuximab vs.
Bevacizumab with FOLFIRI in metastatic colorectal cancer patients
and by Mooi et. al.(14). As research only clas-sifiers, these
methodologies are not designed for application for individual
patients or suitable for use
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
11
in prospective patient assignment. In contrast, our classifier
as deployed in a clinical lab is suitable for classifying
individual patients with the rigor needed for guiding clinical
management. Our CLIA validated assay has potential of integral,
integrated and exploratory marker. Hypotheses being explored
include focused immunotherapy in CMS1, which represents a subgroup
with evidence of higher immune infiltrates and activated T-cells.
CMS2 represents a group with best overall survival from EGFR
inhibition in retrospective assessment of the CALGB/SWOG 80405
trial, while CMS1 benefited from VEGF inhibition (PMID 31042420).
CMS4 has active stromal signature and an im-mune modulating
strategy has been proposed. For example, in the clinical trial
(NCT034365630) as-sessing safety and efficacy of dual TGF-β trap:
anti-PD-L1 molecule M7824 (EMD-Serono), CMS as-say was used as an
intergral biomarker to select patients with CMS4. Expanded efforts
in this trial or other ongoing trials can be done looking to
identify other CMS where efficacy of either M7824 or other drug can
be assessed based on its mechanism of action and CMS biology. As an
integrated assay, all patients can be prospectively tested to
identify CMS. The interim analysis then looks at all comers, and if
negative, then looks at CMS specific subgroups, with plan to
continue the second half of the randomized study. Finally as an
exploratory biomarker, a retrospective analysis can be done with
the high quality CLIA assay to look for a CMS signal but also to
minimize the risk of inconsistent assays when designing the follow
up study. To support the goal of dissemination of a robust CMS
classifier for retrospective or prospective utilization, the
NanoString CodeSets and supporting bioinformatics information can
be found at http://qcsrlshinypro.mdanderson.edu/CMSclia/.
Unavailability of matched samples prevented us from assessing CMS
accuracy between primary and
metastatic tissues in our study. Fontana E et.al (40) using
publically available data from Khambata-
Ford dataset (41), demonstrated no significant difference in CMS
distribution between localized vs.
metastatic disease. The impact of sample site on CMS
classification is necessary to determine host
organ influence and metastasis associated evolution of gene
expression in CRC.
In summary, we have developed, validated and demonstrated
prognostic utility of a CRC-CMS assay
using FFPE samples. This CLIA validated assay provides a
foundation to expand its utility to assess
prognosis in a standard of care setting and explore the assay as
a predictor of response to therapy in
clinical trials.
Acknowledgments: This work is funded by National Cancer
Institute through Assay Validation For
High Quality Markers For NCI-Supported Clinical Trials
(UH2CA207101) and MD Anderson Cancer
Center SPORE in Gastrointestinal Cancer (P50 CA221707). Part of
this research was performed in
MD Anderson’s Core facilities which is supported in part by the
National Institutes of Health through
Cancer Center Support Grant CA016672. Part of the validation
work in the clinical lab was funded as
part of a clinical trial (NCT03436563) funded by EMD-Serono. We
thank Kim-Anh Vu in MD Anderson’s Department of Anatomic Pathology
for helping with the figures.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://qcsrlshinypro.mdanderson.edu/CMSclia/http://projectreporter.nih.gov/project_info_description.cfm?aid=9427630http://clincancerres.aacrjournals.org/
-
12
References:
1. Cancer Genome Atlas N. Comprehensive molecular
characterization of human colon and rectal cancer. Nature
2012;487(7407):330-7 doi 10.1038/nature11252.
2. Perez-Villamil B, Romera-Lopez A, Hernandez-Prieto S,
Lopez-Campos G, Calles A, Lopez-Asenjo JA, et al. Colon cancer
molecular subtypes identified by expression profiling and
associated to stroma, mucinous type and different clinical
behavior. BMC Cancer 2012;12:260 doi 10.1186/1471-2407-12-260.
3. Schlicker A, Beran G, Chresta CM, McWalter G, Pritchard A,
Weston S, et al. Subtypes of primary colorectal tumors correlate
with response to targeted treatment in colorectal cell lines. BMC
Med Genomics 2012;5:66 doi 10.1186/1755-8794-5-66.
4. Sadanandam A, Lyssiotis CA, Homicsko K, Collisson EA, Gibb
WJ, Wullschleger S, et al. A colorectal cancer classification
system that associates cellular phenotype and responses to therapy.
Nat Med 2013;19(5):619-25 doi 10.1038/nm.3175.
5. Marisa L, de Reynies A, Duval A, Selves J, Gaub MP, Vescovo
L, et al. Gene expression classification of colon cancer into
molecular subtypes: characterization, validation, and prognostic
value. PLoS Med 2013;10(5):e1001453 doi
10.1371/journal.pmed.1001453.
6. De Sousa EMF, Wang X, Jansen M, Fessler E, Trinh A, de Rooij
LP, et al. Poor-prognosis colon cancer is defined by a molecularly
distinct subtype and develops from serrated precursor lesions. Nat
Med 2013;19(5):614-8 doi 10.1038/nm.3174.
7. Budinska E, Popovici V, Tejpar S, D'Ario G, Lapique N, Sikora
KO, et al. Gene expression patterns unveil a new level of molecular
heterogeneity in colorectal cancer. J Pathol 2013;231(1):63-76 doi
10.1002/path.4212.
8. Guinney J, Dienstmann R, Wang X, de Reynies A, Schlicker A,
Soneson C, et al. The consensus molecular subtypes of colorectal
cancer. Nat Med 2015;21(11):1350-6 doi 10.1038/nm.3967.
9. Lenz HJ, Ou FS, Venook AP, Hochster HS, Niedzwiecki D,
Goldberg RM, et al. Impact of Consensus Molecular Subtype on
Survival in Patients With Metastatic Colorectal Cancer: Results
From CALGB/SWOG 80405 (Alliance). Journal of clinical oncology :
official journal of the American Society of Clinical Oncology
2019;37(22):1876-85 doi 10.1200/JCO.18.02258.
10. Kwon Y, Park M, Jang M, Yun S, Kim WK, Kim S, et al.
Prognosis of stage III colorectal carcinomas with FOLFOX adjuvant
chemotherapy can be predicted by molecular subtype. Oncotarget
2017;8(24):39367-81 doi 10.18632/oncotarget.17023.
11. Song N, Pogue-Geile KL, Gavin PG, Yothers G, Kim SR, Johnson
NL, et al. Clinical Outcome From Oxaliplatin Treatment in Stage
II/III Colon Cancer According to Intrinsic Subtypes: Secondary
Analysis of NSABP C-07/NRG Oncology Randomized Clinical Trial. JAMA
oncology 2016;2(9):1162-9 doi 10.1001/jamaoncol.2016.2314.
12. Stintzing S WP, Lenz HJ et al. Consensus molecular subgroups
(CMS)of colorectal cancer (CRC) and first-line efficacy of FOLFIRI
plus cetuximab or bevasizumab in the FIRE3 (AIO KRK-0306) trial. .
JCO 2017;35(Suppl 15):3510.
13. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken
JH, Aderka D, et al. ESMO consensus guidelines for the management
of patients with metastatic colorectal cancer. Annals of oncology :
official journal of the European Society for Medical Oncology
2016;27(8):1386-422 doi 10.1093/annonc/mdw235.
14. Mooi JK, Wirapati P, Asher R, Lee CK, Savas P, Price TJ, et
al. The prognostic impact of consensus molecular subtypes (CMS) and
its predictive effects for bevacizumab benefit in metastatic
colorectal cancer: molecular analysis of the AGITG MAX clinical
trial. Annals of oncology : official journal of the European
Society for Medical Oncology 2018;29(11):2240-6 doi
10.1093/annonc/mdy410.
15. Becht E, de Reynies A, Giraldo NA, Pilati C, Buttard B,
Lacroix L, et al. Immune and Stromal Classification of Colorectal
Cancer Is Associated with Molecular Subtypes and Relevant for
Precision Immunotherapy. Clinical cancer research : an official
journal of the American Association for Cancer Research
2016;22(16):4057-66 doi 10.1158/1078-0432.CCR-15-2879.
16. Lal N, White BS, Goussous G, Pickles O, Mason MJ, Beggs AD,
et al. KRAS Mutation and Consensus Molecular Subtypes 2 and 3 Are
Independently Associated with Reduced Immune Infiltration and
Reactivity in Colorectal Cancer. Clinical cancer research : an
official journal of the American Association for Cancer Research
2018;24(1):224-33 doi 10.1158/1078-0432.CCR-17-1090.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
13
17. Okita A, Takahashi S, Ouchi K, Inoue M, Watanabe M, Endo M,
et al. Consensus molecular subtypes classification of colorectal
cancer as a predictive factor for chemotherapeutic efficacy against
metastatic colorectal cancer. Oncotarget 2018;9(27):18698-711 doi
10.18632/oncotarget.24617.
18. Huang D, Quan Y, He M, Zhou B. Comparison of linear
discriminant analysis methods for the classification of cancer
based on gene expression data. J Exp Clin Cancer Res 2009;28:149
doi 10.1186/1756-9966-28-149.
19. Guo Y, Hastie T, Tibshirani R. Regularized linear
discriminant analysis and its application in microarrays.
Biostatistics 2007;8(1):86-100 doi
10.1093/biostatistics/kxj035.
20. Arevalillo JM, Navarro H. A new method for identifying
bivariate differential expression in high dimensional microarray
data using quadratic discriminant analysis. BMC Bioinformatics
2011;12 Suppl 12:S6 doi 10.1186/1471-2105-12-S12-S6.
21. Hastie T, Tibshirani R. Efficient quadratic regularization
for expression arrays. Biostatistics 2004;5(3):329-40 doi
10.1093/biostatistics/5.3.329.
22. Ayyad SM, Saleh AI, Labib LM. Gene expression cancer
classification using modified K-Nearest Neighbors technique.
Biosystems 2019;176:41-51 doi 10.1016/j.biosystems.2018.12.009.
23. Kumar MA, Ewoldt RH, Zukoski CF. Intrinsic nonlinearities in
the mechanics of hard sphere suspensions. Soft Matter
2016;12(36):7655-62 doi 10.1039/c6sm01310d.
24. Huynh-Thu VA, Geurts P. Unsupervised Gene Network Inference
with Decision Trees and Random Forests. Methods Mol Biol
2019;1883:195-215 doi 10.1007/978-1-4939-8882-2_8.
25. Stiglic G, Rodriguez JJ, Kokol P. Rotation of random forests
for genomic and proteomic classification problems. Adv Exp Med Biol
2011;696:211-21 doi 10.1007/978-1-4419-7046-6_21.
26. Rodriguez JJ, Kuncheva LI, Alonso CJ. Rotation forest: A new
classifier ensemble method. IEEE Trans Pattern Anal Mach Intell
2006;28(10):1619-30 doi 10.1109/TPAMI.2006.211.
27. Chan WH, Mohamad MS, Deris S, Zaki N, Kasim S, Omatu S, et
al. Identification of informative genes and pathways using an
improved penalized support vector machine with a weighting scheme.
Comput Biol Med 2016;77:102-15 doi
10.1016/j.compbiomed.2016.08.004.
28. Abdi MJ, Hosseini SM, Rezghi M. A novel weighted support
vector machine based on particle swarm optimization for gene
selection and tumor classification. Comput Math Methods Med
2012;2012:320698 doi 10.1155/2012/320698.
29. Huang H, Lu X, Liu Y, Haaland P, Marron JS. R/DWD:
distance-weighted discrimination for classification, visualization
and batch adjustment. Bioinformatics 2012;28(8):1182-3 doi
10.1093/bioinformatics/bts096.
30. Franks JM, Cai G, Whitfield ML. Feature specific quantile
normalization enables cross-platform classification of molecular
subtypes using gene expression data. Bioinformatics
2018;34(11):1868-74 doi 10.1093/bioinformatics/bty026.
31. Ji Zhu HZ, Saharon Rosset and Trevor Hastie. Multi-class
AdaBoost. 2009. 349-60 p. 32. Chen DT, Davis-Yadley AH, Huang PY,
Husain K, Centeno BA, Permuth-Wey J, et al. Prognostic
Fifteen-Gene Signature for Early Stage Pancreatic Ductal
Adenocarcinoma. PLoS One 2015;10(8):e0133562 doi
10.1371/journal.pone.0133562.
33. Ligibel JA, Cirrincione CT, Liu M, Citron M, Ingle JN,
Gradishar W, et al. Body Mass Index, PAM50 Subtype, and Outcomes in
Node-Positive Breast Cancer: CALGB 9741 (Alliance). J Natl Cancer
Inst 2015;107(9) doi 10.1093/jnci/djv179.
34. Prat A, Galvan P, Jimenez B, Buckingham W, Jeiranian HA,
Schaper C, et al. Prediction of Response to Neoadjuvant
Chemotherapy Using Core Needle Biopsy Samples with the Prosigna
Assay. Clinical cancer research : an official journal of the
American Association for Cancer Research 2016;22(3):560-6 doi
10.1158/1078-0432.CCR-15-0630.
35. Veldman-Jones MH, Lai Z, Wappett M, Harbron CG, Barrett JC,
Harrington EA, et al. Reproducible, Quantitative, and Flexible
Molecular Subtyping of Clinical DLBCL Samples Using the NanoString
nCounter System. Clinical cancer research : an official journal of
the American Association for Cancer Research 2015;21(10):2367-78
doi 10.1158/1078-0432.CCR-14-0357.
36. Wallden B, Storhoff J, Nielsen T, Dowidar N, Schaper C,
Ferree S, et al. Development and verification of the PAM50-based
Prosigna breast cancer gene signature assay. BMC Med Genomics
2015;8:54 doi 10.1186/s12920-015-0129-6.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
14
37. Overman MJ, Morris V, Kee B, Fogelman D, Xiao L, Eng C, et
al. Utility of a molecular prescreening program in advanced
colorectal cancer for enrollment on biomarker-selected clinical
trials. Annals of oncology : official journal of the European
Society for Medical Oncology 2016;27(6):1068-74 doi
10.1093/annonc/mdw073.
38. Goodsaid FM, Amur S, Aubrecht J, Burczynski ME, Carl K,
Catalano J, et al. Voluntary exploratory data submissions to the US
FDA and the EMA: experience and impact. Nature reviews Drug
discovery 2010;9(6):435-45 doi 10.1038/nrd3116.
39. Ragulan C, Eason K, Fontana E, Nyamundanda G, Tarazona N,
Patil Y, et al. Analytical Validation of Multiplex Biomarker Assay
to Stratify Colorectal Cancer into Molecular Subtypes. Scientific
reports 2019;9(1):7665 doi 10.1038/s41598-019-43492-0.
40. Fontana E, Eason K, Cervantes A, Salazar R, Sadanandam A.
Context matters-consensus molecular subtypes of colorectal cancer
as biomarkers for clinical trials. Annals of oncology : official
journal of the European Society for Medical Oncology
2019;30(4):520-7 doi 10.1093/annonc/mdz052.
41. Khambata-Ford S, Garrett CR, Meropol NJ, Basik M, Harbison
CT, Wu S, et al. Expression of epiregulin and amphiregulin and
K-ras mutation status predict disease control in metastatic
colorectal cancer patients treated with cetuximab. Journal of
clinical oncology : official journal of the American Society of
Clinical Oncology 2007;25(22):3230-7 doi
10.1200/JCO.2006.10.5437.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
15
Table-1: Clinicopathologic features of patients and samples
included in the assay development and validation in the research
molecular diagnostic laboratory
Characteristics
n
Age 50 years 136
Gender Male 95 Female 80
Tumor location Right colon 75 Left and sigmoid colon 92 Rectum 5
Multiple primary tumors 3
pT stage pT1 0 pT2 16 pT3 133 pT4 18 pT4a 3 pT4b 1
pN stage pN0 76 pN1 55 pN1a 2 pN1b 5 pN1c 0 pN2 27 pN2a 4 pN2b 2
pN3 0 pNX 4
pM stage pM0 165 pM1 5 pMX 5
Grade Low (well or moderately differentiated) 145 High (poorly
differentiated) 30
Time between date of surgery and gene expression analysis
< 5years 20
5-10 years 95 >10 years 60
Samples Matched flash frozen and formalin fixed paraffin
embedded
149
Only formalin fixed paraffin embedded 12 Only flash frozen 4
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
16
Table-2: Patient characteristics of the cohorts utilized to
correlate CMS and overall survival
N = 345
Mean Age at Initial Diagnosis (SD) 50.9 (11.5)
Mean Age at Stage IV Diagnosis (SD) 51.5 (11.5)
Sex
Male 187 (54.2) Female 158 (45.8)
Race/Ethnicity
Non-Hispanic (NH) White 258 (74.8) NH African American 32 (9.3)
Hispanic 27 (7.8) NH Asian 22 (6.4) Other/Unknown 6 (1.7)
Stage at Initial Diagnosis
I 5 (1.4) II 24 (7.0) III 110 (31.9) IV 204 (59.1) NA 2
(0.6)
KRAS mutation status
wild type 107 (31.0) canonical mutation 147 (42.6) NA 91
(26.4)
NRAS mutation status
wild type 236 (68.4) canonical mutation 17 (4.9) non-canonical
mutation 1 (0.3) NA 91 (26.4)
BRAF mutation status
wild type 229 (66.4) v600 20 (5.8) other mutation 5 (1.4) NA 91
(26.4)
MSI status
MSS 177 (51.3) NA 168 (48.7)
Consensus Molecular Subtype
1, Immune 12 (3.5) 2, Canonical 117 (33.9) 3, Metabolic 21 (6.1)
4, Mesenchymal 161 (46.7) Mixed 34 (9.9)
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
17
Figure Legends:
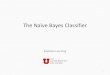
Figure-1: Flowchart showing approach development and validation
of CMS classifier on colorectal cancer sub-
typing consortium (CRCSC) (1A) and development of NanoString
classifier on colorectal cancer samples.
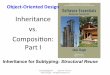
Figure 2: Sample-wise and Gene-wise correlation of paired
FF/FFPE Samples: Figure- 2A: Histogram of sam-
ple-wise Spearman correlation of paired FF/FFPE values across
all 472 CMS genes on Nanostring assay, with
threshold of 0.75 marked with red vertical line. Figure-2B and
2C: Association of sample-wise FF/FFPE with
RNA Quality: Scatterplot of gene-specific Spearman correlation
of FF/FFPE vs. RNA quality of FF samples
(2B, based on RIN) and FFPE samples (2C, based on % with 200nt).
Figure-2D: Histogram of gene-wise
Spearman correlation of paired FF/FFPE values based on samples
with sample-wise correlation > 0.75, with
thresholds to determine the top 100 and top 200 genes indicated
by red and blue vertical lines, respectively.
Figure-3: Bar chart and table showing 4-class accuracy of CMS
classifiers, along with number (proportion) of
samples classified to each CMS. We assess accuracy for
classifier with top 100 genes in terms of FF/FFPE
correlation for FFPE and FF, computed based on Nanostring
measurements for FFPE and FF in current study
(Nano FFPE-100, Nano FF-100) and based on Affymetrix
measurements for FF in the Affy CRCSC validation
data set (V2a, Affy FF-100), and for the full 472 gene
classifier applied to FF samples run on Nanostring plat-
form for current study (Nano FF-472) and FF samples run on
Affymetrix in the Affymetrix CRCSC validation
data set (Affy FF-472). Performance is summarized overall and
for subsets of samples with high classification
confidence (⍺>0.50, 0.80 or 0.90).
Figure-4: Distribution of KRAS and BRAF mutations across CMS
(4A) and correlation of CMS with overall sur-
vival (4B) in stage IV colorectal cancer.
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
CRCSC databases (n=18)
Agilent Datasets excluded
CRCSC databases (n=14)
V1: Discovery set
(n=1329 samples from 12 studies)V2: Validation
set (n=1329
samples from
14 studies)• Apply four-fold cross validation
model building for each
classification model
• Apply quantile normalization
Test accuracy of classification model
Predictive accuracy of each model as function
of number of genes
• Gene ranking strategy based on its
classification from 5973 to 5 genes
• Compare the classification model with same
gene list
V2a:
Validation
subset with
data on
Affymetrix
U133Plus2.0
(n=929
samples )
V2ap:
Validation
subset with
Affymetrix
U133Plus2.0
arrays fRMA
probe-level
data (n=929
samples)
Validation
subset with
TCGA RNAseq
data (n=189
samples)
V2o: Out of
sample
validation
subset
containing
GSE2109 and
GSE17536
(n=383
samples)
Test accuracy of each model and gene ranking
strategy on validation cohorts
Select the best performing model with least
number of genes - Weighted Vector Support
Machine Model
Further
optimization &
tuning of the
parameters
ValidationDiscovery
• Obtain best possible accuracy by
tuning parameters with each model
• Apply multiclass Adaboost to rank
genes for each model
Figure 1A
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
Sample wise correlation (ρ) between NanoString flash
frozen (FF) value and NanoString formalin fixed paraffin
embedded (FFPE) value across 472 genes (n=175
samples)
Samples with ρ≥0.75 (n=142 samples)
Gene-wise correlation (r) between FF value & FFPE to
identify sets of genes with top 100 (CMS100) and top
200 (CMS200) correlations
Train new model on reduced gene sets (CMS100/CMS200)
on CRCSC V1 and obtain new wSVM classifier Ψ100 and
Ψ200Determine accuracy using Affymetrix data on CRCSC V2
Pick gene set (100 or 200 genes)
NanoString expression for each
FFPE sample for the chosen
gene set (n=158)
Quantile normalized expression
on NanoString FFPE sample for
the chosen gene set
Compute probability of each CMS pj• Most likely CMS: Choose CMS
j with
highest pjOR
• Apply confidence threshold:
Choose CMS j with highest pj if
greater than confidence threshold α,
otherwise classify as “Mixed CMS”
• Quantile normalized to the scale of
Affymetrix value of matched FF
sample for the chosen gene set
Apply Ψ to NanoString data normalized
to the scale of Affymetrix data
CMS for each sample
Figure 1B
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
Figure 2F
req
ue
ncy
Fre
qu
en
cy
Sa
mp
le-w
ise
FF
/FF
FP
E
co
rre
latio
n
Sa
mp
le-w
ise
FF
/FF
FP
E
co
rre
latio
n
Sample-wise FF/FFPE correlation
Gene-wise FF/FFPE correlation
top 100 genes
top 100 genes
FF RIN
FFPE %200nt
p-value=0.0077
p-value=0.280
00.3
0.4
0.5
0.6
0.7
0.8
0.9
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0.2 0.4 0.6 0.8 1.0
0.2 0.4 0.6 0.80.0
2 4 6 8 10
20
40
60
80
0
20
20 30 50 70
40
40
60
60
80
80
100
120
140
A B
C D
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
CMS1 CMS2 CMS3 CMS4 Unclassified
No threshold 0.80 38 (0.24) 88 (0.56) 9 (0.06) 23 (0.15) 0
α>0.50 0.81 36 (0.23) 85 (0.54) 8 (0.05) 22 (0.14) 5
(0.03)
α>0.80 0.86 29 (0.19) 65 (0.42) 8 (0.05) 11 (0.07) 43
(0.28)
α>0.90 0.90 25 (0.16) 51 (0.33) 7 (0.04) 7 (0.04) 66
(0.42)
CMS1 CMS2 CMS3 CMS4 Unclassified
No threshold 0.80 34 (0.22) 72 (0.47) 31 (0.20) 16 (0.10) 0
α>0.50 0.82 34 (0.22) 71 (0.46) 28 (0.18) 19 (0.12) 4
(0.03)
α>0.80 0.87 29 (0.19) 64 (0.42) 19 (0.13) 9 (0.06) 30
(0.20)
α>0.90 0.92 20 (0.13) 51 (0.34) 16 (0.11) 5 (0.03) 59
(0.39)
CMS1 CMS2 CMS3 CMS4 Unclassified
No threshold 0.81 40 (0.26) 64 (0.42) 20 (0.13) 29 (0.19) 0
α>0.50 0.82 38 (0.25) 60 (0.40) 19 (0.13) 27 (0.18) 7
(0.05)
α>0.80 0.85 34 (0.22) 51 (0.33) 16 (0.10) 23 (0.15) 29
(0.19)
α>0.90 0.88 30 (0.20) 42 (0.28) 12 (0.08) 20 (0.13) 48
(0.32)
CMS1 CMS2 CMS3 CMS4 Unclassified
No threshold 0.89 222 (0.17) 597 (0.45) 176 (0.13) 334 (0.25)
0
α>0.50 0.9 218 (0.16) 590 (0.44) 172 (0.13) 329 (0.25) 20
(0.02)
α>0.80 0.96 162 (0.12) 479 (0.36) 120 (0.09) 247 (0.19) 320
(0.24)
α>0.90 0.98 131 (0.10) 418 (0.31) 103 (0.08) 199 (0.15) 478
(0.36)
CMS1 CMS2 CMS3 CMS4 Unclassified
No threshold 0.95 232 (0.18) 572 (0.43) 173 (0.13) 352 (0.27)
0
α>0.50 0.95 231 (0.17) 569 (0.43) 170 (0.13) 348 (0.26) 11
(0.01)
α>0.80 0.98 190 (0.14) 530 (0.40) 146 (0.11) 313 (0.24) 150
(0.11)
α>0.90 0.99 169 (0.13) 498 (0.38) 123 (0.09) 288 (0.22) 251
(0.19)
Nano FF-1004-class
accuracy
4-class accuracy
4-class accuracy
4-class accuracy
4-class accuracy
Distribution of predicted CMS
Nano FFPE-100Distribution of predicted CMS
Affy FF-472*Distribution of predicted CMS
Nano FF-472Distribution of predicted CMS
Affy FF-100*Distribution of predicted CMS
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Nano FFPE-100 Nano FF-100 Nano FF-472 Affy FF-100 Affy
FF-472
4-Group Accuracy Assessment of the CMS Classifier
No threshold
Fo
ur
Gro
up
-Accu
racy
α>0.50 α>0.80 α>0.90
Figure 3
A
B
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/
-
1.00
0.50
0
1.00
0.50
0
Pro
po
rtio
n
NA
NA
p
-
Published OnlineFirst October 27, 2020.Clin Cancer Res Jeffrey S
Morris, Rajyalakshmi Luthra, Yusha Liu, et al. CLIA-Certified
SettingConsensus Molecular Subtyping of Colorectal Carcinoma in a
Development and Validation of a Gene Signature Classifier for
Updated version
10.1158/1078-0432.CCR-20-2403doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2020/10/27/1078-0432.CCR-20-2403.DC1
Access the most recent supplemental material at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and
accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
Subscriptions
Reprints and
[email protected] at
To order reprints of this article or to subscribe to the
journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take
you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2020/10/27/1078-0432.CCR-20-2403To
request permission to re-use all or part of this article, use this
link
on July 5, 2021. © 2020 American Association for Cancer
Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on October 27, 2020; DOI:
10.1158/1078-0432.CCR-20-2403
http://clincancerres.aacrjournals.org/lookup/doi/10.1158/1078-0432.CCR-20-2403http://clincancerres.aacrjournals.org/content/suppl/2020/10/27/1078-0432.CCR-20-2403.DC1http://clincancerres.aacrjournals.org/cgi/alertsmailto:[email protected]://clincancerres.aacrjournals.org/content/early/2020/10/27/1078-0432.CCR-20-2403http://clincancerres.aacrjournals.org/
Article FileFigure-1AFigure-1BFigure-2Figure-3Figure-4